Welcome - 2021 Benefit Plans Overview - Florida Gateway College
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Welcome
2021 Benefit Plans
Overview
Florida Gateway’s
Plan Choices
MEDICAL – Health Insurance Plan Options
• Florida Blue BlueOptions PPO 03559
• Florida Blue BlueOptions PPO 03769
• Florida Blue BlueCare HMO 58
2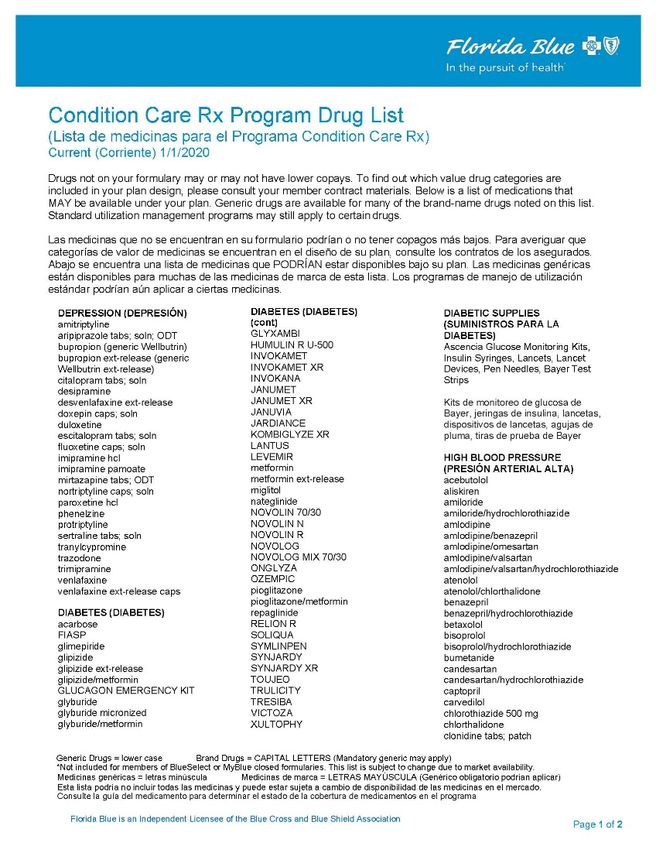
Overview of Health Plans
BlueOptions PPO 03766 BlueOptions PPO 03769
Monthly Premium Monthly Premium
Preventative Services Preventative Services
(Adult & Child) (Adult & Child)
$0 copay $0 copay
Office Visits
PPO 03559 PPO 03769
Family $40 $40 Any services received at doctors
Physician/PCP office will apply to copay.
Specialist $60 $60
Teledoc $10 $10 When you need care now
On vacation, on a business trip, or
away from home
Lab Lab is paid at 100% by using
In-Network – $0 $0 Quest. You can make
Quest appointments online!!!
Out of Network CYD + 30% CYD + 40% www.questdiagnostics.com
Out-of-Network CYD + 30% CYD + 40% Anything other than Blue Options
is Out of Network. Using
Traditional doctors will protect you
from balance billing.
CYD = Calendar Year Deductible
4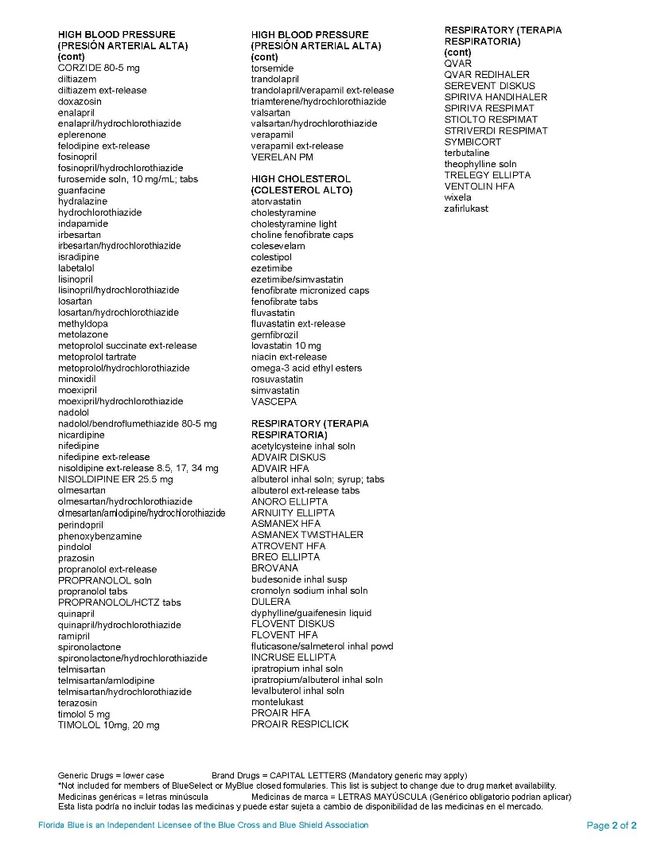
Preventative Health
PPO PPO
Plan Plan
03559 03769
Adult Wellness Includes: $0 $0 See 2020 Clinical Preventive
• Annual physical Care Guidelines. See slides
• Mammogram 22-23.
• PSA Exam
Colonoscopy $0 $0 The U.S. Preventive Services
• Adult Wellness Benefit Talk to Task Force (USPSTF)
• One routine your doctor recommends screening for
colonoscopy (age 50+ about colorectal cancer (CRC) using
paid in full of allowed which a colonoscopy, in adults,
amount) screening beginning at age 50 years and
• Colaguard- noninvasive method is continuing until age 75 years.
option for colon cancer right for The risks and benefits of these
screening you. screening methods vary.
5
Hospital Services – Inpatient
PPO Plan 03559 PPO Plan 03769
Inpatient Facility To determine Option
Copay Option 1 / Option 2 Option 1 / Option 2 levels or
In-Network $9,000 / $1,650 $1,250 / $2,250 participation, go to
Out of Network the Online Provider
$2,500 DED + 40% Directory
www.floridablue.com
Provider Services Any services
while Inpatient received by a
In Network DED + 20% DED + 20% Provider while in the
Out of Network hospital.
INN DED + 20% INN DED + 20%
Option 1 facility / Option 2 facility (teaching or specialized hospital)
6
Hospital Services – Outpatient
PPO Plan PPO Plan B
03559 03769
Option 1 / Option 2 Option 1 / Option 2
Outpatient To determine Option levels or
In-Network $250/$350 CYD + 20%/ CYD + participation, go to the Online
20% Provider Directory
Hospital
Out of Network www.floridablue.com
DED + 30% DED + 40%
Provider Services Any services received by a
while Outpatient Provider
In Network DED + 20%/ $40 / $60
Specialist DED + 20% Copay
Out of Network DED + 30% DED + 40%
7Deductible & Coinsurance
PPO Plan PPO Plan
03559 03769
Calendar Year Deductible $700/$2,100 $800/$2,400 Applies to services such
as Provider Services in
Coinsurance Hospital, Independent
Diagnostic Testing
In Network 20% 20% Facility, Durable Medical
Out of Network 40% 30% Equipment, Prosthetics &
Orthotics and Ambulance
Services
8Out of Pocket Maximum
PPO Plan Plan PPO
03559 03769
In Network and Out The maximum a
of Network members pays out of
(Combined) pocket in a benefit year.
Per Person/Family $7,000/$14,000 All of the following is
$7,000/$14,000 applied to Max Out of
Pocket: Copays,
Calendar Year Deductible
and Coinsurance
Lifetime maximums are no longer in effect due to
Health Care Rform
9Overview of Health Products
BlueCare HMO
Plan
58
Preventative Services
(Adult & Child)
$0 copayOffice Visits
HMO 58
Family Physician / PCP $40 Any services received at doctors
office will apply to copay.
Specialist $60
Teledoc $10 When you need care now
On vacation, on a business trip, or
away from home.
Lab Lab is paid at 100% by using
In Network – Quest $0 Quest. You can make
Out of Network Not Covered appointments online!!!
www.questdiagnostics.com
Out-of-Network Not Covered Anything other than BlueOptions is
Out of Network. Using Traditional
doctors will protect you from
balance billing.
11Preventative Health
HMO 58
Adult Wellness Includes: $0 See 2020 Clinical Preventive
• Annual physical Care Guidelines. See slides 22-
• Mammogram 23.
• PSA Exam
Colonoscopy $0 The U.S. Preventive Services
• Adult Wellness Benefit. Task Force (USPSTF)
One routine recommends screening for
colonoscopy (age 50+ colorectal cancer (CRC) using a
paid in full of allowed colonoscopy, in adults, beginning
amount) at age 50 years and continuing
Cologuard until age 75 years. The risks and
benefits of these screening
A noninvasive option for methods vary.
colon cancer screening
12Hospital Services – Inpatient
HMO 58
Inpatient Facility Copay To determine Option
In-Network $350 per day up to a levels or participation, go
maximum of $1,750 per to the Online Provider
admission Directory
www.floridablue.com
Out of Network Not Covered
Provider Services while Any services received by
Inpatient a Provider while in the
In-Network $0 hospital.
Out of Network Not Covered
Option 1 facility / Option 2 facility (teaching or specialized hospital)
13Hospital Services – Outpatient
HMO 58
Outpatient To determine Option
In-Network Hospital $750 levels or participation,
go to the Online
Provider Directory
Out of Network Not Covered www.floridablue.com
Provider Services while Any services received
Outpatient by a Provider
In-Network $40 / $60 Copay
Out of Network Not Covered
14Deductible & Coinsurance
HMO 58
Calendar Year Deductible N/A Applies to services such as
Provider Services in Hospital,
Coinsurance Independent Diagnostic
Testing Facility, Durable
In Network 80% / 20% Medical Equipment,
Out of Network Not Covered Prosthetics & Orthotics and
Ambulance Services
15Out of Pocket Maximum
HMO 58
In Network and Out of The maximum a members
Network (Combined) pays out of pocket in a benefit
Per Person/Family $6,000 / $12,000 year. All of the following is
applied to Max Out of Pocket:
Copays, Calendar Year
Deductible and Coinsurance
16Pharmacy
Retail – In-Network Mail order
Plans (30 day supply) (90 day supply)
PPO 03769 $15 - generic $30/$90/$130
$45 - preferred brand Specialty drugs are cost share and not
PO 03559 available through mail order
HMO 58 $65 - non-preferred brand
The use of specialty mediations is a
$250 - Monthly Member Out of major factor in drug trends across the
Pocket Maximum per specialty industry.
prescription applies
If a Brand Name Rx is purchased when a Generic Rx is available and the Physician has
not indicated that a Brand Name Rx is medically necessary, member will be required to
pay the difference between the cost of the Brand Name and Generic Rx in addition to
the Rx copay. Pharmacy expenses apply to out-of-pocket maximums.
17Pharmacy
Florida Blue Rx – Condition Care Value Drug Benefit
Waived Copay for Generic and Preferred Brand.
Drugs Classes as applicable for the following:
• Depression
• Diabetes Supply (including Insulin)
• High Blood Pressure
• High Cholesterol
• Respiratory
• Smoking Cessation
The most current listing can be found as a link within the
Medicare Guide when you log into your account online.
18Condition Care Rx Program
1920
21
Register for Teledoc today!
There is No cost to
register!
It only takes a few
minutes.
Do it today before you
don’t feel well.
You can down load the
app to your phone too.
22Member Care Programs
Better You 24/7 Nurse Care Condition Care
from Blue Advice Line Consultant Management Coordination
Team (CCT)
888-476-2227 Catherine Muroski
800-477-3736 877-789-2583 FCSRMC Case Manager
ext.54837
(407) 833-7873
• Benefit catherine.muroski@bcbsfl.com
• Better You • Symptom
from Blue Optimization • Case
Support
• Core Chronic Management
• Lifestyle • Care Referrals • Rare Chronic • Transition of
• Behavioral
Coaching Health • Oncology care
• Social and • Transplants • Pediatric
Coaching
• Behavioral Community • High Risk • Hospice
Risk Resources • Maternity • PCMH/ACO
• Decision
Screening • Prenatal and and much
Support
much more more
Well At Risk Acute/Chronic
23You can also read

















































