Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Review for Medical and Pharmacological Sciences 2023; 27: 333-351
Intermittent fasting in type 2 diabetes: from
fundamental science to clinical applications
L. CHEN1, F.-Y. TIAN1, X.-H. HU2, J.-W. WU1, W.-D. XU1, Q. HUANG3
1
First School of Clinical Medicine, 2Fourth School of Clinical Medicine, Zhejiang Chinese Medical
University, Hangzhou, Zhejiang, China
3
Department of Endocrinology, First Affiliated Hospital of Zhejiang Chinese Medicine University.
Hangzhou, China
Lan Chen, Fengyuan Tian and Xinhao Hu share first authorship
Abstract. – Type 2 diabetes mellitus (T2DM) diabetes in people aged 20-79 years is estimated
is a huge challenge for global public health sys- at 10.5% (536.6 million) in 2021, rising to 12.2%
tems. Currently, healthcare policies advocate (783.2 million) by 20453. However, current T2DM
the prevention of the onset and progression of medications without lifestyle interventions lack
T2DM by improving individual lifestyles. The in-
creasing benefits of intermittent fasting (IF) as a comprehensiveness in glycemic control4. In light
dietary intervention have been elucidated. How- of the limitations of available antidiabetic agents,
ever, the beneficial effects of IF in T2DM re- alternative treatments are highly recommended.
main inconclusive. We demonstrated the phys- In recent years, the dietary intervention has be-
iological mechanisms underlying the positive come a hot topic of research.
effects of IF in T2DM. IF could trigger metabol- Intermittent fasting (IF) is a dietary pattern
ic transformation to improve systemic metabo- involving energy restriction and time-restricted
lism and induce tissue-specific metabolic adap-
tations through alterations in the gut microbio-
fasting5. Alternative invention of energy intake
ta, adipose tissue remodeling, correction of cir- offers better compliance than continuous energy
cadian rhythm disturbances, and increased au- restriction (CER)6. Studies5,7,8 in animals and hu-
tophagy in peripheral tissues. The efficacy and mans have shown that IF has a modulating func-
safety of IF regimens in clinical applications car- tion in a variety of chronic diseases, including
ry a risk of hypoglycemia and require monitoring obesity, diabetes, cardiovascular disease, multiple
of blood glucose and timely adjustment of med- sclerosis, neurodegenerative diseases of the brain,
ications. However, there is limited evidence of a and cancer.
positive effect of IF in weight loss and improve-
ment of glycemic variables. Overall, IF serves
In addition to a simple calorie restriction (CR),
as a promising therapeutic target for T2DM and IF has unique and specific properties, which
needs to be established by a large randomized could trigger systemic metabolic improvements
controlled trial. through metabolic transformation and induce
tissue-specific metabolic adaptations including
Key Words: changes in the gut microbiome, adipose tissue
Intermittent fasting (IF), Type 2 diabetes mellitus remodeling, correction of circadian rhythm dis-
(T2DM), Metabolic transformation, Gut microbiota,
turbances, and increased autophagy in peripheral
Adipose tissue, Circadian biology, Autophagy.
tissues. This review briefly elucidates the posi-
tive effects of IF on T2DM in these five aspects.
Furthermore, IF may encourage weight reduction
Introduction to avoid different diabetes risk factors, including
lower fasting glucose and fasting insulin and
The incidence and prevalence of type 2 diabe- improved insulin sensitivity9. Here, we summa-
tes mellitus (T2DM) continue to rise globally1. rized the benefits of IF regimens and explored the
T2DM is characterized by hyperglycemia due efficacy and side effects of IF in prediabetes and
to insulin resistance (IR) or insufficient insu- T2DM. We intended to provide several sugges-
lin secretion2. International Diabetes Federation tions for future research and clinical applications
(IDF) estimates that the global prevalence of of IF.
Corresponding Author: Qi Huang, MD; e-mail: 19843012@zcmu.edu.cn 333L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
Types of Intermittent Fasting nificantly higher blood ketone levels, especially
β-hydroxybutyric acid18. Elevated β-hydroxybu-
There are various models of intermittent fast- tyrate further raises increased autophagy and
ing and three of them have been widely used reduces oxidative stress (Figure 1)19. On the oth-
in clinical practice: alternate daytime fasting er hand, IF-induced metabolic transformation
(ADF), IF 5:2 (two days of fasting per week), and also mediates significant alterations in several
time-restricted eating (TRE)10. metabolic pathways. These include a decrease
ADF consists of a feeding day and a fasting in rapamycin (mTOR) activity and stimula-
day11. Individuals can consume food and beverag- tion of AMP-activated protein kinase (AMPK)
es without restriction during feeding days and no (Figure 1)20. Reduced glucose and amino acid
caloric intake during fasting days. Modified ADF levels during fasting lead to reduced mTOR
involves individuals consuming typically 20- pathway activity, and inhibition of mTOR ac-
25% (500-800 kcal) of their energy requirement tivity decreases protein synthesis and stimu-
during fasting days12. The IF 5:2 comprises two lates increased autophagy and mitochondrial
stages embodying two fasting days (500-1,000 synthesis21. Fasting affects bioenergetic sensors,
kcal per day) and five other days of free feeding13. especially AMPK, which is activated to pro-
The two restriction days can be consecutive or mote increased autophagy, thereby eliminating
nonconsecutive. TRE has a time requirement for damaged proteins and organelles from the body
the diet, i.e., limiting eating to a specific number and improving mitochondrial function 20. These
of hours per day (usually 4 to 8 hours) and ab- changes can promote metabolic homeostasis and
staining from water or zero-calorie beverages for play a role in maintaining glucose homeostasis
the rest of the day14. and improving insulin sensitivity19.
Other forms of fasting are less common, such
as B2 and 4:3 IF. In the B2 program, the regime
consists of two meals per day, with breakfast Gut Microbiota
from 6 am to 10 am and lunch from 12 pm to
4 pm15. 4:3 IF is similar to IF 5:2, except for an The composition of the gut microbiota is re-
extra day of fasting per week16. modeled in response to changes in individual
dietary habits and nutritional status22. IF leads
to altered cellular responses, shifting cells from
Physiological Mechanisms Associated glucose-dependent to using ketone body carbon
with Intermittent Fasting (KBC), thereby suppressing inflammation and
altering the gut microbiota23,24. Gut microbiota
The potential mechanisms for improving dominates host health and the pathogenesis of
T2DM through IF are complex and can be broad- metabolic diseases such as obesity and diabe-
ly summarized as follows: metabolic transforma- tes25-30. The mechanism regulates systemic me-
tion, alterations in the gut microbiota, adipose tabolism by improving inflammation and reduc-
tissue remodeling, improved circadian rhythms, ing intestinal permeability31.
and increased autophagy. These alterations can The earliest epidemiology of obesity and
induce tissue-specific metabolic adaptations that T2DM-related inflammation dates back to the
allow for remission or even cure of T2DM. We 1960s32,33. Many studies34,35 on T2DM and obe-
summarize the limited evidence and describe sity have demonstrated a rise in circulating in-
these alterations in detail from animal experi- flammatory markers. Low-grade inflammation
ments as well as molecular mechanisms. is a vital determinant of obesity and diabetes36.
Inflammatory mediators such as tumor necrosis
factor-alpha (TNF-α) and interleukin-1β (IL-1β)
Metabolic Transformation undermine insulin sensitivity and poor glucose
tolerance and mediate IR37-40. Related studies41
In the fasting state, triglycerides (TG) are have shown that obesity and diabetes share an
converted to fatty acids and glycerol through important common feature, namely, an increased
lipodieresis. The liver then converts fatty acids proportion of the thick-walled phylum/mycobac-
to ketone bodies, which provide energy to tis- terial phylum. A high-fat diet (HFD) can induce
sues in various parts of the body17. Animals and changes in the gut microbiota by promoting the
humans using fasting or IF protocols had sig- development of Gram-negative bacteria, which
334Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
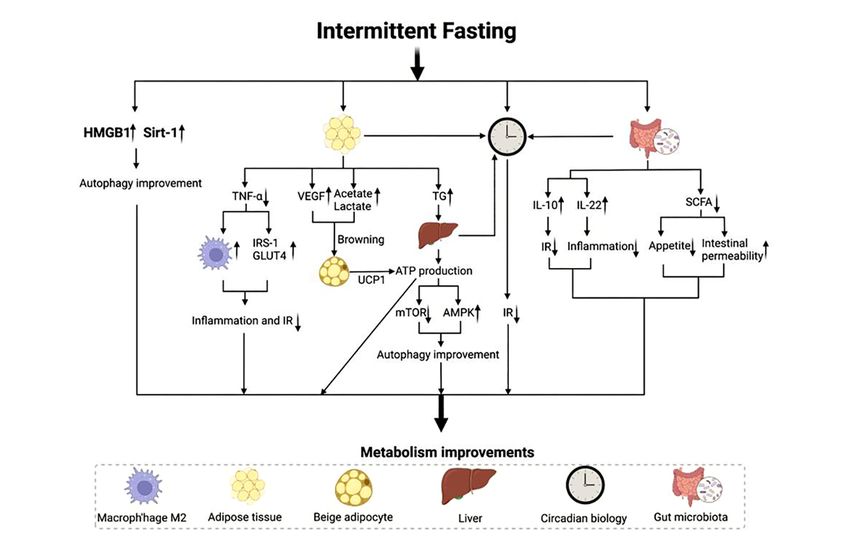
Figure 1. Physiological mechanisms associated with intermittent fasting. Brown to the beige coloration of AT adipose tissue
due to elevated acetate and lactate and VEGF cycling. Beige adiposity increases the expression of UCP1, which leads to
improved metabolism by promoting the oxidative metabolism of glucose and fat coupled to ATP synthesis. At the same time, a
decrease in TNF-α promoted an increase in IRS-1 and GLUT4 and the polarization of macrophage M2. These changes improve
insulin resistance and AT inflammation, resulting in improved metabolism. On the other hand, TG increases due to IF, and TG
is broken down into ketone bodies in the liver. Ketone bodies increase autophagy in the organism through a decrease in mTOR
activity and activation of AMPK. Elevated HMGB and Sirt-1 similarly increase autophagy. Increased autophagy further
improves metabolism. IF alters the composition of the gut microbiota, thereby increasing the levels of IL-10, IL-11 and SCFA.
IL-10 and IL-22 balance the body’s metabolism by improving IR and inflammation, respectively. SCFA, on the other hand,
improves body metabolism by reducing appetite and intestinal permeability. Finally, AT, gut microbiota and liver influence
the local peripheral clock and regulate the circadian system together with the central clock, thus reducing IR and correcting
metabolic disturbances. IF: intermittent fasting; HMGB: high mobility group box 1; Sirt-1: sirtuin-1; TNF-α: tumor necrosis
factor-alpha; IRS-1: insulin receptor substrate 1; GLUT4: glucose transporter protein type 4; VEGF: vascular endothelial
growth factor; TG: triglycerides; ATP: adenosine triphosphate; mTOR: rapamycin; AMPK: AMP-activated protein kinase; IR:
insulin resistance; SCFA: short-chain fatty acid; UCP1: uncoupling protein 1; IL: interleukin.
leads to lipopolysaccharide (LPS) production to by Lactobacillus paracasei and Faecalibacterium
trigger systemic inflammation42. Furthermore, prausnitzii can inhibit the activity of nuclear fac-
changes in the gut microbiota brought on by IF tor-κB (NF-κB)52,53.
may lessen T2DM’s inflammatory symptoms43-45. On the other hand, IF treatment significantly
For example, interleukin-10 (IL-10) induced by increased the levels of the thick-walled phylum
Roseburia guts, Bacteroides fragilis, Akkerman- while reducing most other phyla and elevating
sia muciniphila, Lactobacillus Plantarum, and short-chain fatty acids (SCFAs) production, com-
Lactobacillus casei improves glucose metabolism pared to ad libitum-fed control animals54. SCFAs
and prevents aging-related IR (Figure 1)46-48. En- are the product of gut microbiota fermentation
terobacteriaceae can restore insulin sensitivity of indigestible foods55. The key factor in mu-
and induce transforming growth factor-β (TGF-β) cin production (increased mucin expression) and
to suppress intestinal inflammation by increasing tight junction integrity preservation, SCFAs are
interleukin-22 (IL-22) production (Figure 1)49- crucial for limiting increasing intestinal permea-
51
. The anti-inflammatory molecules produced bility (Figure 1). A distinctive feature of T2DM is
335L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
the increase in intestinal permeability that leads the adipose vascular endothelial growth factor
to the transfer of LPS and microbial metabolites (VEGF) cycle and thus increased WAT browning
into the bloodstream, which in turn causes IR (Figure 1). Li et al73 demonstrated that IF induces
and metabolic endotoxemia56,57. Entering circu- inguinal WAT by altering the abundance of intes-
lating LPS interacts with LPS-binding proteins tinal microbiota and promoting the production of
and membrane-bound cluster of differentiation 14 acetate and lactate. The specific mechanism by
(CD14) receptors. Their complexes interact with which IF induces adipose browning needs to be
toll-like receptor 4 (TLR4) to influence inflam- further investigated.
matory signals and insulin signaling pathways58. IF ameliorates inflammation in adipose tissue,
Meanwhile, SCFAs can control energy intake and some studies79 have shown that IF reduces
through the gut-brain axis59. The gut-derived sa- pro-inflammatory markers (e.g., macrophages,
tiety hormones glucagon-like peptide-1 (GLP-1) IL-1, IL-6, TNF-α, etc.) in subcutaneous white
and peptide YY (PYY) are mainly secreted by adipose tissue (sWAT) of diet-induced obese
enteroendocrine L cells, with the highest density (DOI) mice. AT inflammation mediated by ad-
in the ileal and colonic epithelium60-63. SCFAs are ipose macrophages and their secreted TNF-α
a major stimulator of GLP-1 production by endo- is shown in Figure 180,81. There is evidence that
crine L cells64. GLP-1 regulates appetite through TNF-α can inhibit the activity of peroxisome
its effects on opioid melanocortinogen (POMC) proliferator-activated receptor-γ (PPARγ) through
and neuropeptide Y (NPY) neurons in the arcuate multiple pathways82. The classical pathway blocks
nucleus of satiety (ARC) and is known to inhibit the binding of PPARγ to its downstream response
gastric emptying and gastric acid secretion (Fig- elements by activating the NF-κB pathway83.
ure 1)65-67. Thus, there is also a link between GLP- HFD-fed mice treated with PPARγ agonists dis-
1 and reduced hunger during IF68. play higher insulin sensitivity and an increase in
Overall, IF-mediated changes in gut microbio- the anti-inflammatory phenotype of M2 macro-
ta alleviate inflammation and maintain intestinal phages84. In addition, circulating free fatty acid
permeability in T2DM. To improve the efficacy (FFA) levels were increased due to the inhibition
of IF in T2DM, further robust preclinical and of PPARγ downstream signaling85. And FFA can
clinical studies are needed to standardize the op- promote the polarization of pro-inflammatory
timal regimen for IF. phenotype M1 macrophages86. TNF-α knockout
mice avert HFD-induced IR and show lower FFA
levels87. In addition, TNF-α significantly down-
Adipose Tissue regulates insulin receptor substrate 1 (IRS-1)
and glucose transporter protein type 4 (GLUT4)
IF can positively affect T2DM by remodeling expression and inhibits AMPK activity (Figure
adipose tissue (AT), mainly by the browning of 1)88,89. Activated AMPK induces polarization of
white adipose tissue (WAT), increasing thermo- M2 macrophages and inhibits IR (Figure 1)86,88,90.
genesis of brown adipose tissue, and reducing in- Moreover, IF improves insulin sensitivity by
flammation (Figure 1)69-71. We briefly describe the decreasing inflammatory collagen IV expression
improvement of AT browning and inflammation. in visceral white adipose tissue (vWAT)91. Thus,
It was found that IF-induced WAT browning to further elucidate the specific mechanisms of IF
and beiging increased adipogenic thermogenesis and adipose tissue remodeling numerous preclini-
and improved HFD-induced obesity and meta- cal and clinical studies are needed.
bolic dysfunction72-75. AT browning and beiging
increase the expression of uncoupling protein 1
(UCP1), which improves insulin sensitivity by Circadian Biology
promoting the oxidative metabolism of glucose
and fat by uncoupling with adenosine triphos- TRE can increase insulin sensitivity and pos-
phate (ATP) synthesis, resulting in heat produc- itively affect systemic metabolic disorders by
tion and energy expenditure (Figure 1)76,77. IF-in- altering the frequency of eating, correcting cir-
duced browning appears to be largely unrelated cadian rhythm disturbances, and altering the ex-
to the classical differentiation stimuli β-adrener- pression of biological clock genes. The circadian
gic receptor (β-AR) and fibroblast growth factor biological system consists of a central brain clock
21 (FGF21)78. Kim et al72 found IF mice promote in the supraoptic nucleus of the hypothalamus
selective activation of adipose macrophages via and various peripheral tissue clocks (e.g., similar
336Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
clock oscillators found in peripheral tissues such ders by regulating circadian rhythms needs to be
as the liver)92. The circadian system plays an im- demonstrated by additional studies.
portant role in metabolic and energetic physiolog-
ical changes through behavioral interventions93,94.
Light information and feeding time (Zeitgebers) Improved Autophagy
are the main temporal cues92. According to the
circadian rhythm disruption hypothesis, synchro- Autophagy, a process of self-degradation and
nization of feeding with the endogenous clock cleanup by organisms, has been demonstrated to
can promote the homeostasis of the clock sys- play a critical role in T2DM112,113. The recovery
tem95. Conversely, it can lead to misalignment function of autophagy may be severely compro-
of temporal species rhythms, causing circadian mised in mice on an HFD by IR and T2DM114,115.
rhythm disruption and promoting IR and T2DM IF has been proven to restore autophagy, attenuate
development96. the effects of metabolic diseases such as T2DM on
Several clinical trials97-99 have confirmed that autophagy, and maintain cellular rejuvenation116.
human glucose tolerance is higher in the morning Similarly, autophagy suppression reduces the in-
than in the evening. Dysregulation of circadian terventional impact of IF117. In a recent study118,
rhythms leads to a reduction in glucose tolerance the light chain 3 (LC3)-II/LC3-1 ratio was higher
in humans100. Shift workers have an increased risk in mice that followed a 4-month fasting inter-
of developing type 2 diabetes mellitus (T2DM) vention, suggesting enhanced autophagy. On the
compared to people with normal sleep schedules101. other hand, IF stimulates sirtuin-1 (Sirt-1) activity
The circadian rhythm of glucose tolerance in hu- and enhances autophagy and serum high mobil-
mans is mediated primarily through the circadian ity group box 1 (HMGB1) levels119. The role of
rhythm of systemic insulin sensitivity. The cen- HMGB1 and Sirt-1 in the regulation of autopha-
tral clock plays a major role in systemic insulin gy has been demonstrated120 in animals and cell
sensitivity through the hypothalamic connection lines (Figure 1). Autophagy is essential for normal
between sleep/wake and food intake102. The local β-cell function and survival, and regulation of au-
peripheral clock further finetunes systemic insulin tophagy, rather than excessive autophagy, may be
sensitivity via the gut clock103, muscle clock104, a possible mechanism to explain the beneficial ef-
adipose tissue clock105, liver clock106, and pancre- fects of IF on β-cell function. However, the under-
atic clock (Figure 1)107. Among these, appropriate lying molecular mechanisms remain unclear121-123.
management of eating behavior, a crucial compo- IF can result in the remission of β-cell function
nent of rhythmic behavior, might enhance IR to in T2DM124 and might improve metabolism by
some amount (Figure1)108. Significant changes in increasing autophagy in humans (Figure 1)125,126.
peripheral clock gene expression levels in skeletal
muscle and subcutaneous adipose tissue (SAT) are
observed in obese women12. A 5-week randomized Human Intervention Studies
crossover-controlled trial109 of 12 patients with
prediabetes found that TRE (6-h feeding period) IF is a planned dietary intervention with inten-
improved insulin sensitivity and β-cell respon- tionally prolonged fasting. The focus of research
siveness compared to 12-h feeding. Consistent on IF is weight loss. We briefly review some
with this finding, after four days of TRE (6-h trials conducted in recent years in obese patients
TRE from 8 am to 2 pm) in 11 obese patients, it (without prediabetes and T2DM) using the three
was reported110 that TRE lowered fasting glucose main IF regimens (ADF, IF 5:2 and TRE) (Table
and insulin, reduced 24-hour glucose fluctuations, I). In addition, we summarize the results of stud-
altered biological clock gene expression, and may ies with different IF regimens in patients with
also increase autophagy and have anti-aging ef- abnormal glucose metabolism conditions (i.e.,
fects in humans. Notably, however, Lundell et prediabetes and T2DM) (Table II).
al111 reported that TRE improved lipid and amino
acid rhythmicity but did not interfere with the Results of Studies Using the IF Protocols
expression of the core clock. It is undeniable that in Obese Patients (Without Prediabetes
time-restricted fasting has a positive impact on hu- and T2DM)
man metabolism, which requires further research The vast majority of IF outcomes reported
in more clinical applications. However, the precise in randomized trials of obese patients are pri-
mechanism by which IF improves metabolic disor- marily weight loss and improved body composi-
337L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
Table I. Trials of IF in obese patients.
Participants Trial Intervention Body Energy Fat Blood LDL HDL TG Fasting Fasting HOME- HbA1c Inflammation Ref.
weeks groups weight intake mass pressure glucose insulin IR
N = 31, men and 8 ADF (500-kcal fast ↓b ↓ 25% ↓b NT ∅ ∅ ∅ ∅ ∅ ∅ NT ∅ CRP 127
women, with day)
overweight and
Exercise (endurance) ∅ ∅ ↓b NT ∅ ∅ ∅ ↓b ∅ ∅ NT ∅ CRP
without T1DM
or T2DM. ADF with exercise ↓ b
↓ 20% ↓b
NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ CRP
Control (ad libitum ∅ ∅ ∅ NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ CRP
intake, no exercise)
N = 31, men and 12 ADF (600-kcal fast ↓a ↓ 35% ↓a ∅ SBP ∅ ↓a ∅ ∅ ∅ ∅ ∅ NT 128
women, with day)
overweight and ↓ DBPa
without T1DM
or T2DM.
N= 37, men and 8 ADF (3 nonconsec- ↓b ↓ 30% ∅ NT NT NT NT ∅ ↓b ↓b NT NT 12
women, with utive days per week
overweight and 30% energy require-
without T1DM ments 100% energy
or T2DM. intake on feasting
day)
ADF (3 nonconsec- ∅ ∅ ∅ NT NT NT NT ∅ ∅ ∅ NT NT
utive days per week
30% energy require-
ments 145% energy
intake on feasting
day)
N = 112, men 46 5:2: Fast day (500 ↓b ↓ 25% ↓b ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT ↓ sCD40Lb 13
and women, with kcal)
overweight and ∅ IL-6
with MS. Feast day (ad libi-
tum) ∅ TNF-α
Control (ad libitum) ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT ∅ sCD40Lb
∅ IL-6
∅ TNF-α
Continued
338Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
Table I (Continued). Trials of IF in obese patients.
Participants Trial Intervention Body Energy Fat Blood LDL HDL TG Fasting Fasting HOME- HbA1c Inflammation Ref.
weeks groups weight intake mass pressure glucose insulin IR
N = 250, men 52 5:2: Fast day (wom- ∅ ↓ 26% ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ CRP 129
and women, en 500 kcal, men
overweight and 600 kcal)
without T1DM
or T2DM. Feast day (ad libi-
tum)
Mediterranean ∅ ↓ 20% ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ↓b ∅ CRP
Paleo ∅ ↓ 20% ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ CRP
N = 121, wom- 52 5:2: Fast day (500 ↓a
↓ 34% ∅ NT NT NT NT ∅ ∅ ∅ ∅ NT 130
en only, with kcal)
overweight and
without T1DM Feast day (ad libi-
or T2DM. tum)
Calorie restriction ↓a ↓ 25% ∅ NT NT NT NT ∅ ∅ ∅ ∅ NT
(1,500 kcal per day)
N = 58, men and 8 4-h TRE (3-7 pm) ↓b ↓ 30% ↓b ∅ ∅ ∅ ∅ ∅ ↓b ↓b ∅ ∅ IL-6 131
women, with
overweight and ∅ TNF-α
without T1DM 6-h TRE (1-7 pm) ↓b
↓ 30% ↓b
∅ ∅ ∅ ∅ ∅ ↓b
↓b
∅ ∅ IL-6
or T2DM.
∅ TNF-α
Control (no meal ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ IL-6
timing restrictions)
∅ TNF-α
N = 58, men and 12 8-h TRE (12-8 pm) ∅ NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT 132
women, with
overweight and Control (no meal ∅ NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT
without T1DM timing restrictions)
or T2DM.
N = 19, men and 12 10-h TRE (self-se- ↓a ↓ 10% ↓a ↓ SBPa ↓a ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ CRP 133
women, over- lect)
weight with MS. ↓ DBPa
N = 20, men and 12 8-h TRE (self-select) ↓b NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT 134
women, with
Control (no meal ∅ NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT
overweight and
timing restrictions)
without T1DM
or T2DM.
a
p < 0.05, significantly different from baseline (within-group effect). bp < 0.05, significantly different from the control or calorie-restricted group (between-group effect). When the control group is
present, only significant changes versus control are reported. ∅, nonsignificant change; ADF, alternate-day fasting; CRP, C-reactive protein; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c;
HOMA-IR, homeostatic model assessment of insulin resistance; IL, interleukin; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; MS, metabolic syndrome;
NT, not tested (parameter not measured); ND, data not disclosed; SBP, systolic blood pressure; sCD40L, soluble CD40 ligand; TG, triglyceride; TNF, tumor necrosis factor; TRE, time-restricted
eating; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; ↓, decrease in the indicated parameter; ↑, increase in the indicated parameter.
339L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
Table II. Trials of IF in prediabetes and T2DM patients.
Participants Trial Intervention groups Body Energy Fat Blood LDL HDL TG Fasting Fasting HOME-IR HbA1c Inflammation Ref.
weeks weight intake mass pressure glucose insulin
N = 8, men only, 5 6-h TRE (8 am-2 pm) ∅ ∅ NT ↓ SBPb ∅ ∅ ↑b ∅ ↓b ↓b NT ∅ CRP 109
overweight with ↓ DBPb ∅ IL-6
prediabetes.
Control (12-h eating ∅ ∅ NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT ∅ CRP
window) ∅ IL-6
N = 26, men 12 5:2: Fast day (women 600 ↓a ↓ 24% ↓a NT ∅ ∅ ∅ ∅ ∅ NT ↓a ∅ TNF-α 151
and women, kcal, men 650 kcal) ∅ IL-6
overweight with Feast day (ad libitum)
prediabetes.
5:2: Fast day (women 600 ↓a ↓ 25% ↓a NT ∅ ∅ ∅ ∅ ∅ NT ↓a ∅ TNF-α
kcal, men 650 kcal) ∅ IL-6
Feast day (ad libitum)
Lacticaseibacillus rham-
nosus probiotic
N = 97, men 52 5:2: Fast day (500 kcal) ↓a NT ↓a NT ↓a ↓a ↓a ↓a ↓a NT ↓a NT 152
and women, Feast day (ad libitum)
with overweight
and
T2DM.
CR (1,500 kcal/day) ↓a NT ↓a NT ↓a ↓a ↓a ↓a ↓a NT ↓a NT
N = 51, men 12 5:2: Fast day (400-600 ↓ a
NT ↓ a
NT NT NT NT NT NT NT ↓ a
NT 153
and women, kcal)
with overweight Feast day (ad libitum)
and T2DM.
CR (1,200-1,500 kcal/ ↓a NT ↓a NT NT NT NT NT NT NT ↓a NT
day)
Continued
340Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
Table II (Continued). Trials of IF in prediabetes and T2DM patients.
Participants Trial Intervention groups Body Energy Fat Blood LDL HDL TG Fasting Fasting HOME-IR HbA1c Inflammation Ref.
weeks weight intake mass pressure glucose insulin
N = 37, men 12 5:2: Consecutive Fast day ↓a ↓ ND ∅ ∅ ∅ ∅ ∅ ↓a NT NT ↓a NT 154
and women, (500-600 kcal)
with T2DM. Feast day (ad libitum)
5:2: Non-consecutive ↓a ↓ ND ∅ ∅ ↑b ∅ ∅ ↓a NT NT ↓a NT
Fast day (500-600 kcal)
Feast day (ad libitum)
n = 37, men and 2 4-6-h TRE (8 am-2 pm) ↓a ↓ 18% NT ∅ NT NT NT ND ND ∅ NT ∅ CRP 155
women, with
T2DM.
n = 32, men and 1 Buchinger (300 kcal/day ↓b NT NT ↓ SBPb ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT 156
women, with Anal- liquid diet) ↓ DBPb
MS and T2DM. ysis Followed by advice for
after 4 the Mediterranean diet
months
Control (advice about the ∅ NT NT ∅ ∅ ∅ ∅ ∅ ∅ ∅ ∅ NT
Mediterranean diet)
n = 54, men and 12 B2 (500 kcal/day 2 meals ↓b NT NT NT ∅ ∅ ∅ ↓b ∅ NT ∅ NT 15
women, with per day, breakfast and
overweight and lunch only)
T2DM.
A6 (500 kcal/day 6 meals ∅ NT NT NT ∅ ∅ ∅ ∅ ∅ NT ∅ NT
per day)
n = 51, men 12 IER (1,400-1,700 kcal/ ∅ NT ∅ NT ∅ ∅ ∅ NT NT NT ∅ NT 16
only, with day)
overweight and
T2DM.
PPM (1,400-1,700 kcal/ ∅ NT ∅ NT ∅ ∅ ∅ NT NT NT ∅ NT
day)
a
p < 0.05, significantly different from baseline (within-group effect). bp < 0.05, significantly different from the control or calorie-restricted group (between-group effect). When the control group is
present, only significant changes versus control are reported. ∅, nonsignificant change; ADF, alternate-day fasting; CRP, C-reactive protein; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c;
HOMA-IR, homeostatic model assessment of insulin resistance; IER, intermittent energy restriction; IL, interleukin; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein choles-
terol; MS, Metabolic Syndrome; NT, not tested (parameter not measured); ND, data not disclosed; PPM, proportioned meals; SBP, systolic blood pressure; SSM, self-selected meals; TG, triglyceride;
TNF, tumor necrosis factor; TRE, time-restricted eating; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; ↓, decrease in the indicated parameter; ↑, increase in the indicated parameter.
341L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang tion12,13,127-134. Compared to TRE131-134, ADF12,127,128 factors, such as lowering blood pressure, con- and IF 5:213,129,130 have more clinically significant trolling blood lipids, decreasing inflammation, weight loss effects, suggesting that TRE is safe and reducing oxidative stress13,129,133. and well-tolerated. It is relatively easy to accept In conclusion, IF protocols have a positive effect in elderly or frail patients and there are no weight on obesity. Educational activities and follow-up for restrictions135. IF failed to help subjects retain a patients to maintain an IF diet are necessary. leaner mass compared to CER130. However, several studies136-138 that combined TRE with resistance Results of Studies Using the IF Protocols training found an increase in fat-free mass (FFM), in Prediabetes Patients an increase in skeletal muscle, and an improvement The use of IF procedures in individuals with in muscle performance along with weight loss. prediabetes have been positively impacted by re- Perhaps this is a direction for future research. The cent research. To date, two studies109,151 have evalu- main reason for weight loss in the subjects is a ated the impact of IF regimens on individuals with reduction in energy intake. No retaliatory eating prediabetes. Sutton et al109 conducted a 5-week was placed while receiving IF therapy, and all IF trial of TFR (6-h TRE from 8 am to 2 pm) in 8 treatments lowered calorie consumption by more prediabetic male subjects. The results found that than 10%13. According to research139, IF 5:2 had a the subjects decreased fasting insulin and blood high protein, moderate fat, low carbohydrate, and pressure, improved insulin sensitivity and β-cell low fiber consumption composition in terms of diet responsiveness, and reduced oxidative stress in quality. The quality of the diet was consistent with the absence of weight loss, explaining that IF has what subjects needed during the weight-loss period. benefits which are independent of weight loss. Overall, IF is a beneficial way of weight loss. Tay et al151 obtained similar positive results with As part of the IF trials, blood glucose mea- a 12-week dietary intervention of IF 5:2 (fasting surements are frequently evaluated. Fasting glu- 2 days per week, 600 kcal per day) in 33 subjects cose usually remains constant during ADF, IF with obesity and prediabetes. Subjects had reduced 5:2, and TRE. In normoglycemic subjects, cir- energy intake, weight loss, less waist circumfer- culating glucose levels are maintained at steady ence, and lower HbaA1c. Subjects complied very levels, and fasting insulin levels are reduced well in both trials. However, there was no signif- from baseline in several trials12,128,130,131,140,141. In icant decrease in fasting glucose, which may be contrast to those whose baseline insulin lev- related to the short duration of trials. Additionally, els were within the normal range, this impact these two trials109,151 lack awareness of fluctuations was seen more often in people with increased without glucose monitoring during IF. baseline insulin levels (>13 uIU/ml)131. Elevated fasting insulin levels are a diagnostic criterion Results of Studies Using the IF Protocols for IR142, suggesting that IF has a better impact in T2DM Patients on reducing fasting insulin in insulin-resistant Positive outcomes with IF regimens in T2DM patients, which may be related to the metabolic patients have been documented15,16,152-156. The most transformation mechanism17. The effect of IF used IF regime for T2DM is IF 5:2. A 52-week IF on insulin sensitivity varies widely, with some 5:2 trial of 137 patients with both obesity and studies showing improvement12,130,131,141, but most T2DM yielded positive results152. Post-interven- had no effect43,128,132,134,139, 143-145. Some studies tion studies153 showed that weight loss reduced have reported that prolonged fasting leads to HbA1c levels and improved fasting glucose and impaired insulin response146,147, while others lipid levels, which was consistent with the con- have shown that IF140 has a good facilitative tinuous energy restriction (CER) group. The re- function on insulin sensitivity148,149. In animal sults are coherent with the prior trial using IF studies150, IF has been found to improve islet 5:2. Both trials152,153, also performed a medication pancreatic β-cell quality by increasing β-cell effectiveness score (MES), which decreased over progenitor cell neurogenin 3 (Ngn3) expression time indicating that IF would be beneficial for and promoting β-cell neogenesis. It requires T2DM patients in the decrease of the dose of dia- more in-depth research in more trials. In those betes medications. Additionally, subjects showed without T2DM, the majority of investigations on better adherence in the IF group than in the CER glycosylated hemoglobin (HbA1c) have shown group152. At the end of the 52-week intervention, no change128,131,132,134. Additionally, IF is advanta- Carter et al157 conducted a 12-month follow-up geous for lowering other metabolic disease risk intervention and found that subjects had a 0.3% 342
Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
increase in HbA1c levels from the preinterven- glycemic parameters and partial reductions in
tion baseline and a 33% weight recovery from medication intake. IF could improve patient mo-
pre-intervention baseline, suggesting that sus- tivation and compliance and reduce medication
tained intervention and dietary support are need- side effects. As no severe hypoglycemic events
ed to maintain positive outcomes. Corley et al154 and other adverse events have been reported, IF
conducted a 12-week trial of IF 5:2 (continuous or can be considered a relatively safe dietary inter-
noncontinuous fasting) in 37 patients with T2DM vention for T2DM patients.
and obesity. The results showed a reduction in
overall energy intake, weight loss, lower levels of
fasting glucose and HbA1c, and improved quality Safety of Intermittent Fasting
of life in the subjects. Meanwhile, no difference
in outcomes between continuous or discontinu- The safety of intermittent fasting has been ques-
ous fasting is observed. There was a two-fold in- tioned. Therefore, we tried to find little evidence
crease in the risk of hypoglycemic events during for the adverse effects of IF regimens. Fasting is
fasting, but no serious hypoglycemic events oc- barely elite with any long-term gastrointestinal
curred. Therefore, IF 5:2 is feasible to comply adverse effects such as abdominal pain, diarrhea,
with compliance in patients with T2DM, espe- nausea, vomiting, or halitosis131. A reduction in
cially in patients who are diet-controlled and not energy intake was observed without binge eating
taking sulfonylureas and insulin. and other eating disorder symptoms. Psychological
Additionally, the interventions for IF are var- disorders such as depressive mood or manic mood
ied. Subjects with T2DM who fasted 18-20 hours are not observed yet160,161. Moreover, there is no
per day for 2 weeks of metformin intervention clear evidence11,145 of clinically meaningful effects
experienced weight loss and reduced fasting and on thyroid hormones or reproductive hormones.
postprandial glucose levels155. Postprandial glu- Common adverse effects of IF are gout, muscle
cose variability, a major marker of glycemic wasting, and the risk of hypoglycemia. Prolonged
control, was also reduced158. Fifty-four patients fasting inhibits uric acid excretion, which leads to
with T2DM underwent a 12-week intervention a rapid increase in serum uric acid162. IF usually
comparing A6 (three large and three small meals leads to a decrease in overall energy intake and a
per day) vs. B2 (breakfast and lunch) regimen deficit in overall protein intake, which may lead
with the same daily energy restriction in both to muscle atrophy163. However, other studies136-138
groups. Eating only breakfast and lunch favors have combined exercise with IF and achieved
weight loss, liver fat content, fasting glucose, successful FFM maintenance. IF can avoid hy-
C-peptide, glucagon levels, and oral glucose in- poglycemic events in normoglycemic subjects,
sulin sensitivity (OGIS). These regimens improve with the main risk being in patients with T2DM.
insulin sensitivity and β-cell function. Mean- Despite the reduced dose of diabetes medications,
while, the frequency and timing of eating are fasting increases the incidence of hypoglycemia.
as important as energy restrictions. After four Therefore, T2DM patients require close physician
months of the Buchinger diet plan intervention monitoring during intermittent fasting.
(300 kcal per day via liquid intake only, followed In conclusion, IF is a safe dietary intervention
by gradual reintroduction of solid food), subjects option and requires robust coordination with the
showed weight loss, lower HbA1c levels, lower clinician. However, the safety of intermittent
blood pressure, and improved quality of life156. fasting remains inconclusive attributed to the
The results of the 12-week 4:3 IF (1,000 kcal per lack of large randomized controlled trials to test
day for 4 consecutive days per week, with the the long-term efficacy and side effects of IF in
remaining 3 days eating ad libitum) were similar patients with well-defined conditions such as
to the above results, reducing triglyceride levels. metabolic syndrome or mood disorders.
It is worth noting that none of the above dietary
interventions reported severe adverse effects.
In conclusion, IF, in any form, leads to signifi- Clinical Implementation
cant weight loss and reduction in the whole body Considerations for Patients with T2DM
and visceral fat15,16,152-156, and both weight and
visceral fat gain are associated with an increased The clinical implementation of IF in patients
risk of T2DM159. Since IF intervention, patients with T2DM requires appropriate medical man-
with T2DM have experienced improvements in agement. Regular glucose monitoring in the
343L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
fasting state, two hours before and after each
Funding
meal and at bedtime on day 7 is recommended. If This paper is funded by Zhejiang Traditional Chinese Med-
necessary, anti-diabetic medications are reduced icine Science and Technology Plan (ZZYJ-WTRW-2018-01,
according to physician recommendations to avoid 2020ZZ009) and the national key research and development
fasting hypoglycemia, such as sulfonamides and plan “Active Health and Aging Technology Response” key
insulin139,164. The IF intervention should be suspend- project (2018YFC200200).
ed immediately when a severe hypoglycemic event
occurs. Because of the potential for excessive fluid
intake (e.g., water and tea) on fasting days, diuretics
and SGLT-2 medications may need to be reduced or References
discontinued to reduce the risk of dehydration and
hypotension. The specific medication regimen also 1) Chatterjee S, Khunti K, Davies MJ. Type 2 diabe-
relies on the clinical experience of the endocrinolo- tes. Lancet 2017; 389: 2239-2251.
gist due to the lack of clinical data. Physicians are 2) Ghislain J, Poitout V. Targeting lipid GPCRs to
treat type 2 diabetes mellitus-progress and chal-
advised to work individually with patients on a one- lenges. Nat Rev Endocrinol 2021; 17: 162-175.
to-one basis 24/7 to minimize the risk of hypogly-
3) Sun H, Saeedi P, Karuranga S, Pinkepank M,
cemia. Patients are also advised not to adjust their Ogurtsova K, Duncan BB, Stein C, Basit A, Chan
medications privately without physician advice164. JCN, Mbanya JC, Pavkov ME, Ramachanda-
ran A, Wild SH, James S, Herman WH, Zhang P,
Bommer C, Kuo S, Boyko EJ, Magliano DJ. IDF
Conclusions Diabetes Atlas: Global, regional and country-level
diabetes prevalence estimates for 2021 and pro-
jections for 2045. Diabetes Res Clin Pract 2022;
According to a growing amount of research, IF 183: 109119.
provides a wide variety of health advantages. Nu- 4) Siehler J, Blöchinger AK, Meier M, Lickert H. En-
merous studies have shown that the benefits of IF on gineering islets from stem cells for advanced ther-
glucose homeostasis in T2DM patients and healthy apies of diabetes. Nat Rev Drug Discov 2021; 20:
individuals should be further investigated. Almost 920-940.
all kinds of IF exhibited a weight-reduction impact 5) Clifton KK, Ma CX, Fontana L, Peterson LL. Inter-
in all population study participants. And in patients mittent fasting in the prevention and treatment of
cancer. CA Cancer J Clin 2021; 71: 527-546.
with dysglycemia and obesity, IF showed the ability
6) Barnosky AR, Hoddy KK, Unterman TG, Varady
and potential to lower fasting insulin, HbA1c concen- KA. Intermittent fasting vs daily calorie restriction
trations, and insulin sensitivity index. The specific for type 2 diabetes prevention: a review of human
mechanisms are mainly through metabolic trans- findings. Transl Res 2014; 164: 302-311.
formation to improve systemic metabolism and in- 7) Varady KA, Cienfuegos S, Ezpeleta M, Gabel
duce tissue-specific metabolic adaptations, including K. Clinical application of intermittent fasting for
changes in the gut microbiota, remodeling of adipose weight loss: progress and future directions. Nat
tissue, correction of circadian rhythm disturbances, Rev Endocrinol 2022; 18: 309-321.
and increased autophagy in peripheral tissues. IF as a 8) Morales-Suarez-Varela M, Collado Sánchez E,
Peraita-Costa I, Llopis-Morales A, Soriano JM.
nutritional modifier has a few adverse effects mainly Intermittent Fasting and the Possible Benefits in
involving the risk of gout, muscle wasting, and hypo- Obesity, Diabetes, and Multiple Sclerosis: A Sys-
glycemia. In conclusion, IF might act as a safe dietary tematic Review of Randomized Clinical Trials.
therapeutic target. However, it remains unclear which Nutrients 2021; 13: 3179.
diets (ADF, IF 5:2, or TRE) are the best regimen. 9) Hamman RF, Wing RR, Edelstein SL, Lachin JM,
Fortunately, the positive findings so far highlight the Bray GA, Delahanty L, Hoskin M, Kriska AM,
direction of future research. Mayer-Davis EJ, Pi-Sunyer X, Regensteiner J,
Venditti B, Wylie-Rosett J. Effect of weight loss
with lifestyle intervention on risk of diabetes. Dia-
Conflict of Interest betes Care 2006; 29: 2102-2107.
The Authors declare that they have no conflict of interests. 10) Varady KA, Cienfuegos S, Ezpeleta M, Gabel K.
Cardiometabolic Benefits of Intermittent Fasting.
Annu Rev Nutr 2021; 41: 333-361.
Availability of Data and Materials 11) Stekovic S, Hofer SJ, Tripolt N, Aon MA, Royer P,
The experimental data used to support the findings of this Pein L, Stadler JT, Pendl T, Prietl B, Url J, Schro-
study are available from the corresponding author upon re- eder S, Tadic J, Eisenberg T, Magnes C, Stumpe
quest. M, Zuegner E, Bordag N, Riedl R, Schmidt A,
344Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
Kolesnik E, Verheyen N, Springer A, Madl T, Sin- S, Bhapkar M, Martin CK, Gilhooly CH, Hollo-
ner F, de Cabo R, Kroemer G, Obermayer-Pi- szy JO, Hadley EC, Roberts SB. A 2-Year Ran-
etsch B, Dengjel J, Sourij H, Pieber TR, Madeo domized Controlled Trial of Human Caloric Re-
F. Alternate Day Fasting Improves Physiological striction: Feasibility and Effects on Predictors of
and Molecular Markers of Aging in Healthy, Non- Health Span and Longevity. J Gerontol A Biol Sci
obese Humans. Cell Metab 2019; 30: 462-476.e6. Med Sci 2015; 70: 1097-1104.
12) Zhao L, Hutchison AT, Wittert GA, Thompson CH, 23) Chung H, Chou W, Sears DD, Patterson RE,
Lange K, Liu B, Heilbronn LK. Intermittent Fasting Webster NJG, Ellies LG. Time-restricted feeding
Does Not Uniformly Impact Genes Involved in Cir- improves insulin resistance and hepatic steato-
cadian Regulation in Women with Obesity. Obesi- sis in a mouse model of postmenopausal obesity.
ty (Silver Spring) 2020; 28: S63-S67. Metabolism 2016; 65: 1743-1754.
13) Guo Y, Luo S, Ye Y, Yin S, Fan J, Xia M. Intermit- 24) de Cabo R, Mattson MP. Effects of Intermittent
tent Fasting Improves Cardiometabolic Risk Fac- Fasting on Health, Aging, and Disease. N Engl J
tors and Alters Gut Microbiota in Metabolic Syn- Med 2019; 381: 2541-2551.
drome Patients. J Clin Endocrinol Metab 2021; 25) Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V,
106: 64-79. Mardis ER, Gordon JI. An obesity-associated gut
14) de Oliveira Maranhão Pureza IR, da Silva Ju- microbiome with increased capacity for energy
nior AE, Silva Praxedes DR, Lessa Vasconce- harvest. Nature 2006; 444: 1027-1031.
los LG, de Lima Macena M, Vieira de Melo IS, 26) Ridaura VK, Faith JJ, Rey FE, Cheng J, Duncan
de Menezes Toledo Florêncio TM, Bueno NB. Ef- AE, Kau AL, Griffin NW, Lombard V, Henrissat B,
fects of time-restricted feeding on body weight, Bain JR, Muehlbauer MJ, Ilkayeva O, Semenkov-
body composition and vital signs in low-income ich CF, Funai K, Hayashi DK, Lyle BJ, Martini MC,
women with obesity: A 12-month randomized clin- Ursell LK, Clemente JC, Van Treuren W, Walters
ical trial. Clin Nutr 2021; 40: 759-766. WA, Knight R, Newgard CB, Heath AC, Gordon
15) Kahleova H, Belinova L, Malinska H, Oliyarnyk JI. Gut microbiota from twins discordant for obe-
O, Trnovska J, Skop V, Kazdova L, Dezortova M, sity modulate metabolism in mice. Science 2013;
Hajek M, Tura A, Hill M, Pelikanova T. Eating two 341: 1241214.
larger meals a day (breakfast and lunch) is more 27) Turnbaugh PJ, Hamady M, Yatsunenko T, Can-
effective than six smaller meals in a reduced-en- tarel BL, Duncan A, Ley RE, Sogin ML, Jones
ergy regimen for patients with type 2 diabetes: a WJ, Roe BA, Affourtit JP, Egholm M, Henrissat B,
randomised crossover study. Diabetologia 2014; Heath AC, Knight R, Gordon JI. A core gut micro-
57: 1552-1560. biome in obese and lean twins. Nature 2009; 457:
16) Ash S, Reeves MM, Yeo S, Morrison G, Carey D, 480-484.
Capra S. Effect of intensive dietetic interventions 28) Wen L, Ley RE, Volchkov PY, Stranges PB, Ava-
on weight and glycaemic control in overweight nesyan L, Stonebraker AC, Hu C, Wong FS, Szot
men with Type II diabetes: a randomised trial. Int GL, Bluestone JA, Gordon JI, Chervonsky AV. In-
J Obes Relat Metab Disord 2003; 27: 797-802. nate immunity and intestinal microbiota in the de-
17) Anton SD, Moehl K, Donahoo WT, Marosi K, velopment of Type 1 diabetes. Nature 2008; 455:
Lee SA, Mainous AG, Leeuwenburgh C, Mattson 1109-1113.
MP. Flipping the Metabolic Switch: Understanding 29) Qin J, Li Y, Cai Z, Li S, Zhu J, Zhang F, Liang S,
and Applying the Health Benefits of Fasting. Obe- Zhang W, Guan Y, Shen D, Peng Y, Zhang D, Jie
sity (Silver Spring) 2018; 26: 254-268. Z, Wu W, Qin Y, Xue W, Li J, Han L, Lu D, Wu P,
18) Sleiman SF, Henry J, Al-Haddad R, El Hayek L, Dai Y, Sun X, Li Z, Tang A, Zhong S, Li X, Chen
Abou Haidar E, Stringer T, Ulja D, Karuppagound- W, Xu R, Wang M, Feng Q, Gong M, Yu J, Zhang
er SS, Holson EB, Ratan RR, Ninan I, Chao MV. Y, Zhang M, Hansen T, Sanchez G, Raes J, Fal-
Exercise promotes the expression of brain de- ony G, Okuda S, Almeida M, LeChatelier E, Re-
rived neurotrophic factor (BDNF) through the ac- nault P, Pons N, Batto JM, Zhang Z, Chen H,
tion of the ketone body β-hydroxybutyrate. Elife Yang R, Zheng W, Li S, Yang H, Wang J, Ehrlich
2016; 5: e15092. SD, Nielsen R, Pedersen O, Kristiansen K, Wang
J. A metagenome-wide association study of gut
19) Finkel T. The metabolic regulation of aging. Nat microbiota in type 2 diabetes. Nature 2012; 490:
Med 2015; 21: 1416-1423. 55-60.
20) Hardie DG. AMPK: positive and negative regula- 30) Karlsson FH, Tremaroli V, Nookaew I, Bergström
tion, and its role in whole-body energy homeosta- G, Behre CJ, Fagerberg B, Nielsen J, Bäckhed F.
sis. Curr Opin Cell Biol 2015; 33: 1-7. Gut metagenome in European women with nor-
21) Dall KB, Færgeman NJ. Metabolic regulation of mal, impaired and diabetic glucose control. Na-
lifespan from a C. elegans perspective. Genes ture 2013; 498: 99-103.
Nutr 2019; 14: 25. 31) Tremaroli V, Bäckhed F. Functional interactions
22) Ravussin E, Redman LM, Rochon J, Das SK, between the gut microbiota and host metabolism.
Fontana L, Kraus WE, Romashkan S, Williamson Nature 2012; 489: 242-249.
DA, Meydani SN, Villareal DT, Smith SR, Stein 32) Ogston D, McAndrew GM. FIBRINOLYSIS IN
RI, Scott TM, Stewart TM, Saltzman E, Klein OBESITY. Lancet 1964; 2: 1205-1207.
345L. Chen, F.-Y. Tian, X.-H. Hu, J.-W. Wu, W.-D. Xu, Q. Huang
33) Grace CS, Goldrick RB. Fibrinolysis and body abolically Healthy Obese Adults: A Randomized
bulid. Interrelationships between blood fibrino- Clinical Trial. JAMA Intern Med 2017; 177: 930-
lysis, body composition and parameters of lipid 938.
and carbohydrate metabolism. J Atheroscler Res 44) Griffin NW, Ahern PP, Cheng J, Heath AC, Ilka-
1968; 8: 705-719. yeva O, Newgard CB, Fontana L, Gordon JI. Pri-
34) Kaptoge S, Di Angelantonio E, Lowe G, Pepys or Dietary Practices and Connections to a Human
MB, Thompson SG, Collins R, Danesh J. C-re- Gut Microbial Metacommunity Alter Responses
active protein concentration and risk of coronary to Diet Interventions. Cell Host Microbe 2017; 21:
heart disease, stroke, and mortality: an individual 84-96.
participant meta-analysis. Lancet 2010; 375: 132- 45) Dey N, Wagner VE, Blanton LV, Cheng J, Fontana
140. L, Haque R, Ahmed T, Gordon JI. Regulators of
35) Rohm TV, Meier DT, Olefsky JM, Donath MY. In- gut motility revealed by a gnotobiotic model of di-
flammation in obesity, diabetes, and related dis- et-microbiome interactions related to travel. Cell
orders. Immunity 2022; 55: 31-55. 2015; 163: 95-107.
36) Burcelin R, Garidou L, Pomié C. Immuno-micro- 46) Plovier H, Everard A, Druart C, Depommier C,
biota cross and talk: the new paradigm of meta- Van Hul M, Geurts L, Chilloux J, Ottman N,
bolic diseases. Semin Immunol 2012; 24: 67-74. Duparc T, Lichtenstein L, Myridakis A, Delzenne
37) Guilherme A, Virbasius JV, Puri V, Czech MP. Ad- NM, Klievink J, Bhattacharjee A, van der Ark
ipocyte dysfunctions linking obesity to insulin re- KC, Aalvink S, Martinez LO, Dumas ME, Mait-
sistance and type 2 diabetes. Nat Rev Mol Cell er D, Loumaye A, Hermans MP, Thissen JP, Bel-
Biol 2008; 9: 367-377. zer C, de Vos WM, Cani PD. A purified mem-
brane protein from Akkermansia muciniphila or
38) Eguchi K, Manabe I, Oishi-Tanaka Y, Ohsugi M, the pasteurized bacterium improves metabolism
Kono N, Ogata F, Yagi N, Ohto U, Kimoto M, Mi- in obese and diabetic mice. Nat Med 2017; 23:
yake K, Tobe K, Arai H, Kadowaki T, Nagai R. 107-113.
Saturated fatty acid and TLR signaling link β cell
dysfunction and islet inflammation. Cell Metab 47) Shen Z, Zhu C, Quan Y, Yang J, Yuan W, Yang Z,
2012; 15: 518-533. Wu S, Luo W, Tan B, Wang X. Insights into Rose-
buria intestinalis which alleviates experimental
39) Stienstra R, Joosten LAB, Koenen T, van Tits
colitis pathology by inducing anti-inflammatory re-
B, van Diepen JA, van den Berg SAA, Rensen
sponses. J Gastroenterol Hepatol 2018; 33: 1751-
PCN, Voshol PJ, Fantuzzi G, Hijmans A, Ker-
1760.
sten S, Müller M, van den Berg WB, van Rooijen
N, Wabitsch M, Kullberg BJ, van der Meer JWM, 48) Chen P, Zhang Q, Dang H, Liu X, Tian F, Zhao J,
Kanneganti T, Tack CJ, Netea MG. The inflam- Chen Y, Zhang H, Chen W. Antidiabetic effect of
masome-mediated caspase-1 activation controls Lactobacillus casei CCFM0412 on mice with type
adipocyte differentiation and insulin sensitivity. 2 diabetes induced by a high-fat diet and strepto-
Cell Metab 2010; 12: 593-605. zotocin. Nutrition 2014; 30: 1061-1068.
40) Vandanmagsar B, Youm YH, Ravussin A, Galgani 49) Hoffmann TW, Pham HP, Bridonneau C, Aubry
JE, Stadler K, Mynatt RL, Ravussin E, Stephens C, Lamas B, Martin-Gallausiaux C, Moroldo M,
JM, Dixit VD. The NLRP3 inflammasome insti- Rainteau D, Lapaque N, Six A, Richard ML, Far-
gates obesity-induced inflammation and insulin gier E, Le Guern ME, Langella P, Sokol H. Mi-
resistance. Nat Med 2011; 17: 179-188. croorganisms linked to inflammatory bowel dis-
ease-associated dysbiosis differentially impact
41) Beli E, Yan Y, Moldovan L, Vieira CP, Gao R,
host physiology in gnotobiotic mice. ISME J 2016;
Duan Y, Prasad R, Bhatwadekar A, White FA,
10: 460-477.
Townsend SD, Chan L, Ryan CN, Morton D, Mol-
dovan EG, Chu FI, Oudit GY, Derendorf H, Adorini 50) Zhu C, Song K, Shen Z, Quan Y, Tan B, Luo W,
L, Wang XX, Evans-Molina C, Mirmira RG, Boul- Wu S, Tang K, Yang Z, Wang X. Roseburia intes-
ton ME, Yoder MC, Li Q, Levi M, Busik JV, Grant tinalis inhibits interleukin‑17 excretion and pro-
MB. Restructuring of the Gut Microbiome by In- motes regulatory T cells differentiation in colitis.
termittent Fasting Prevents Retinopathy and Pro- Mol Med Rep 2018; 17: 7567-7574.
longs Survival in Mice. Diabetes 2018; 67: 1867- 51) Wang X, Ota N, Manzanillo P, Kates L, Zava-
1879. la-Solorio J, Eidenschenk C, Zhang J, Lesch
42) Blasco-Baque V, Serino M, Vergnes JN, Riant J, Lee WP, Ross J, Diehl L, van Bruggen N,
E, Loubieres P, Arnal JF, Gourdy P, Sixou M, Kolumam G, Ouyang W. Interleukin-22 alleviates
Burcelin R, Kemoun P. High-fat diet induces metabolic disorders and restores mucosal immu-
periodontitis in mice through lipopolysaccharides nity in diabetes. Nature 2014; 514: 237-241.
(LPS) receptor signaling: protective action of es- 52) Sun KY, Xu DH, Xie C, Plummer S, Tang J, Yang
trogens. PLoS One 2012; 7: e48220. XF, Ji XH. Lactobacillus paracasei modulates
43) Trepanowski JF, Kroeger CM, Barnosky A, Klem- LPS-induced inflammatory cytokine release by
pel MC, Bhutani S, Hoddy KK, Gabel K, Freels S, monocyte-macrophages via the up-regulation of
Rigdon J, Rood J, Ravussin E, Varady KA. Effect negative regulators of NF-kappaB signaling in
of Alternate-Day Fasting on Weight Loss, Weight a TLR2-dependent manner. Cytokine 2017; 92:
Maintenance, and Cardioprotection Among Met- 1-11.
346Intermittent fasting in type 2 diabetes: from fundamental science to clinical applications
53) Breyner NM, Michon C, de Sousa CS, Vilas Boas 64) Martin CR, Osadchiy V, Kalani A, Mayer EA. The
PB, Chain F, Azevedo VA, Langella P, Chatel Brain-Gut-Microbiome Axis. Cell Mol Gastroen-
JM. Microbial Anti-Inflammatory Molecule (MAM) terol Hepatol 2018; 6: 133-148.
from Shows a Protective Effect on DNBS and 65) Fukuda T, Bouchi R, Takeuchi T, Amo-Shiinoki
DSS-Induced Colitis Model in Mice through Inhi- K, Kudo A, Tanaka S, Tanabe M, Akashi T, Hi-
bition of NF-κB Pathway. Front Microbiol 2017; 8: rayama K, Odamaki T, Igarashi M, Kimura I, Ta-
114. nabe K, Tanizawa Y, Yamada T, Ogawa Y. Im-
54) Klement RJ, Pazienza V. Impact of Different portance of Intestinal Environment and Cellular
Types of Diet on Gut Microbiota Profiles and Can- Plasticity of Islets in the Development of Post-
cer Prevention and Treatment. Medicina (Kaunas) pancreatectomy Diabetes. Diabetes Care 2021;
2019; 55: 84. 44: 1002-1011.
55) Tan J, McKenzie C, Potamitis M, Thorburn AN, 66) Bercik P. The Brain-Gut-Microbiome Axis and Irri-
Mackay CR, Macia L. The role of short-chain fatty table Bowel Syndrome. Gastroenterol Hepatol (N
acids in health and disease. Adv Immunol 2014; Y) 2020; 16: 322-324.
121: 91-119. 67) Zhao L, Zhang F, Ding X, Wu G, Lam YY, Wang
56) Ding S, Lund PK. Role of intestinal inflamma- X, Fu H, Xue X, Lu C, Ma J, Yu L, Xu C, Ren Z, Xu
tion as an early event in obesity and insulin resis- Y, Xu S, Shen H, Zhu X, Shi Y, Shen Q, Dong W,
tance. Curr Opin Clin Nutr Metab Care 2011; 14: Liu R, Ling Y, Zeng Y, Wang X, Zhang Q, Wang
328-333. J, Wang L, Wu Y, Zeng B, Wei H, Zhang M, Peng
57) Xiao S, Fei N, Pang X, Shen J, Wang L, Zhang B, Y, Zhang C. Gut bacteria selectively promoted by
Zhang M, Zhang X, Zhang C, Li M, Sun L, Xue Z, dietary fibers alleviate type 2 diabetes. Science
Wang J, Feng J, Yan F, Zhao N, Liu J, Long W, 2018; 359: 1151-1156.
Zhao L. A gut microbiota-targeted dietary inter- 68) Iepsen EW, Lundgren J, Holst JJ, Madsbad S,
vention for amelioration of chronic inflammation Torekov SS. Successful weight loss maintenance
underlying metabolic syndrome. FEMS Microbiol includes long-term increased meal responses of
Ecol 2014; 87: 357-367. GLP-1 and PYY3-36. Eur J Endocrinol 2016; 174:
58) Zhang X, Zhao Y, Xu J, Xue Z, Zhang M, Pang 775-784.
X, Zhang X, Zhao L. Modulation of gut microbi- 69) Chen P, Wang YY, Chen C, Guan J, Zhu HH,
ota by berberine and metformin during the treat- Chen Z. The immunological roles in acute-on-
ment of high-fat diet-induced obesity in rats. Sci chronic liver failure: An update. Hepatobiliary
Rep 2015; 5: 14405. Pancreat Dis Int 2019; 18: 403-411.
59) Canfora EE, Jocken JW, Blaak EE. Short-chain 70) Hatori M, Vollmers C, Zarrinpar A, DiTacchio L,
fatty acids in control of body weight and insu- Bushong EA, Gill S, Leblanc M, Chaix A, Jo-
lin sensitivity. Nat Rev Endocrinol 2015; 11: 577- ens M, Fitzpatrick JAJ, Ellisman MH, Panda S.
591. Time-restricted feeding without reducing calor-
60) Jorsal T, Rhee NA, Pedersen J, Wahlgren CD, ic intake prevents metabolic diseases in mice
Mortensen B, Jepsen SL, Jelsing J, Dalbøge LS, fed a high-fat diet. Cell Metab 2012; 15: 848-
Vilmann P, Hassan H, Hendel JW, Poulsen SS, 860.
Holst JJ, Vilsbøll T, Knop FK. Enteroendocrine K
71) Zarrinpar A, Chaix A, Yooseph S, Panda S. Diet
and L cells in healthy and type 2 diabetic individ-
and feeding pattern affect the diurnal dynamics of
uals. Diabetologia 2018; 61: 284-294.
the gut microbiome. Cell Metab 2014; 20: 1006-
61) Lebrun LJ, Lenaerts K, Kiers D, Pais de Bar- 1017.
ros JP, Le Guern N, Plesnik J, Thomas C, Bour-
72) Kim KH, Kim YH, Son JE, Lee JH, Kim S, Choe
geois T, Dejong CHC, Kox M, Hundscheid IHR,
MS, Moon JH, Zhong J, Fu K, Lenglin F, Yoo JA,
Khan NA, Mandard S, Deckert V, Pickkers P,
Bilan PJ, Klip A, Nagy A, Kim JR, Park JG, Hus-
Drucker DJ, Lagrost L, Grober J. Enteroendo-
sein SM, Doh KO, Hui CC, Sung HK. Intermit-
crine L Cells Sense LPS after Gut Barrier Inju-
tent fasting promotes adipose thermogenesis and
ry to Enhance GLP-1 Secretion. Cell Rep 2017;
metabolic homeostasis via VEGF-mediated alter-
21: 1160-1168.
native activation of macrophage. Cell Res 2017;
62) Lewis JE, Miedzybrodzka EL, Foreman RE, 27: 1309-1326.
Woodward ORM, Kay RG, Goldspink DA, Gribble
FM, Reimann F. Selective stimulation of colonic L 73) Li G, Xie C, Lu S, Nichols RG, Tian Y, Li L, Pa-
cells improves metabolic outcomes in mice. Dia- tel D, Ma Y, Brocker CN, Yan T, Krausz KW,
betologia 2020; 63: 1396-1407. Xiang R, Gavrilova O, Patterson AD, Gonzalez
FJ. Intermittent Fasting Promotes White Adipose
63) Sun EW, Iepsen EW, Pezos N, Lumsden AL, Mar- Browning and Decreases Obesity by Shaping
tin AM, Schober G, Isaacs NJ, Rayner CK, Nguy- the Gut Microbiota. Cell Metab 2017; 26: 672-
en NQ, de Fontgalland D, Rabbitt P, Hollington 685.e4.
P, Wattchow DA, Hansen T, Holm JC, Liou AP,
Jackson VM, Torekov SS, Young RL, Keating DJ. 74) Liu B, Page AJ, Hutchison AT, Wittert GA, Heil-
A Gut-Intrinsic Melanocortin Signaling Complex bronn LK. Intermittent fasting increases energy
Augments L-Cell Secretion in Humans. Gastroen- expenditure and promotes adipose tissue brown-
terology 2021; 161: 536-547.e2. ing in mice. Nutrition 2019; 66: 38-43.
347You can also read