Sindromi mielodisplastiche Highlights - Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sindromi mielodisplastiche
Highlights
Luca Malcovati, MD
Department of Molecular Medicine,
University of Pavia Medical School,
& Department of Hematology Oncology,
IRCCS Policlinico S. Matteo Foundation,
Pavia, Italy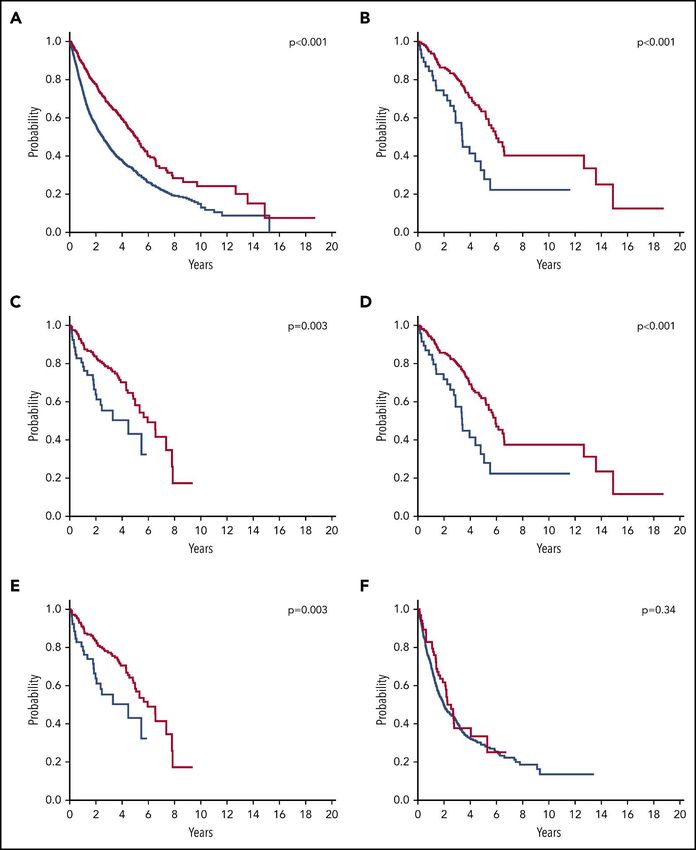
CONFLICT OF INTEREST DISCLOSURE Name of Research Employee Consultant Stockholder Speaker’s Advisory Other Company support Bureau Board NA NA NA NA NA NA NA NA

Learning Objectives • Relevance of somatic mutation analysis in the diagnostic work-up of suspected myeloid neoplasm with myelodysplasia • Recognition of genetically defined disease entities: SF3B1-mutant MDS • Prognostic implications of TP53 allelic state in MDS • Luspatercept in MDS with ring sideroblasts

Diagnostic approach to MDS
«The myelodysplastic syndromes are a group of clonal hematopoietic stem cell
diseases characterized by cytopenia, dysplasia in one or more of the major myeloid
lineages, ineffective hematopoiesis, recurrent genetic abnormalities and increased
risk of developing acute myeloid leukemia»
Diagnostic tool Diagnostic value
- Cytopenia in at least one hematopoietic Peripheral blood • Dysplasia in one or more cell lines
smear • Enumeration of blasts
lineage.
Bone marrow • Dysplasia in one or more cell lines
- Dysplastic features in ≥10% of the nucleated aspirate • Enumeration of blasts; ring sideroblasts
cells in one or more myeloid lineages,
Bone marrow biopsy • BM cellularity, CD34+ cells, and fibrosis
AND/OR
• Acquired clonal chromosomal
Cytogenetic analysis
- recurrent chromosomal abnormalities that abnormalities
provide presumptive evidence of primary • Targeted chromosomal abnormalities
FISH
MDS following failure of standard G-banding
Flow cytometry • Abnormalities in hematopoietic
immunophenotyping compartments
Landscape of somatic mutations in MDS
Papaemmanuil et al. Blood. 2013;122:3616-27
Diagnostic approach to MDS
Positive predictive value
• ≥1 mutation: 0.81 (0.76-0.84)
• ≥2 mutations: 0.88 (0.84-0.92)
Positive Predictive Negative Predictive
VAF
Value Value
0.05 0.84 0.75
0.10 0.86 0.77
0.20 0.87 0.68
Malcovati et al. Blood. 2017;129:3371-3378
Negative predictive value for myeloid neoplasm of genetic analysis
• No somatic mutation 0.76 (95% CI 0.70-0.81)
5% - Unmutated patients with cytogenetic abnormalities
• No genetic lesion 0.84 (95% CI 0.79-0.89)
5% - “False positive” MDS (patients receiving a diagnosis of
MDS based on mild dysplasia; no evidence of clonality; no
evidence of disease progression).
• No genetic lesion 0.92 (95% CI 0.88-0.95)
5% - Patients without clonal marker (1% MDS-MLD, 2% MDS-
EB, 1% MDS/MPN)
Malcovati et al. Blood. 2017;129:3371-3378
Q1 Donna, 39 anni Hb 12.1 g/dL, MCV 98 fL, GB 2.38x109/L (ANC 0.6x109/L), Plt 228x109/L Mieloaspirato: note displastiche (5-10%). Blasti 2% del MCN. BOM: cellularità 30%. Cellule CD34+ 1-2%. Citogenetica 46XX Quale delle seguenti definizioni è più corretta? a. Citopenia idiopatica di incerto significato b. Neutropenia cronica idiopatica c. Aplasia midollare non severa d. Sindrome mielodisplastica ipoplastica

Idiopathic Cytopenia of Undetermined Significance (ICUS)
Definition criteria
• Relevant cytopenia in one or more lineage
(Hb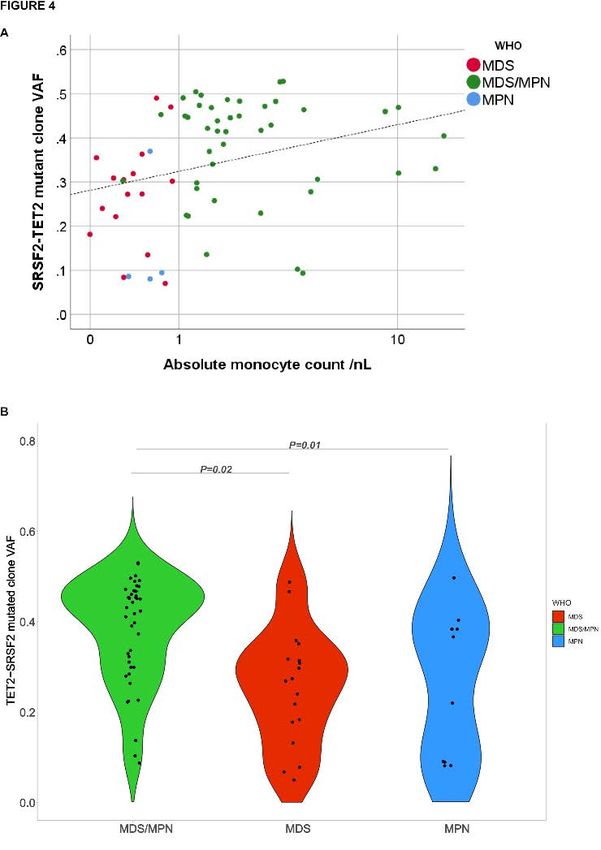
Mutation analysis in cytopenia of undetermined significance
Clonal Cytopenia of Undetermined
Significance (CCUS)
Unmutated Idiopathic Cytopenia of
Undetermined Significance (ICUS)
Malcovati et al. Blood. 2017;129:3371-3378Bone marrow hypocellularity and hypoplastic MDS
Bono et al. Leukemia. 2019;33:2495-2505Q2 Quale delle seguenti affermazioni relative alla correlazione genotipo- fenotipo nelle neoplasie mieloidi è corretta? a. Lo stato mutazionale è il solo determinante del fenotipo b. La gerarchia clonale non ha effetto sul fenotipo c. La dimensione del clone può influenzare l’espressività clinica e condizionare la classificazione d. Tutte le precedenti e. Nessuna delle precedenti
Myelodysplastic syndromes – WHO classification
- MDS with single lineage dysplasia
- MDS with ring sideroblasts (MDS-RS)
– MDS-RS and single lineage dysplasia
– MDS-RS and multilineage dysplasia
- MDS with multilineage dysplasia
- MDS with excess blasts
- MDS with isolated del(5q)
- MDS, unclassifiable
- Provisional entity: Refractory cytopenia of childhood
Entity name Number of Number of Ring sideroblasts as percentage Bone marrow (BM) and Cytogenetics by conventional karyotype analysis
dysplastic lineages cytopenias of marrow erythroid elements peripheral blood (PB) blasts
MDS-RS
MDS-RS-SLD 1 1-2 ≥ 15% / ≥ 5%b BM< 5%, Any, unless fulfils all criteria for MDS
PB < 1%, with isolated del(5q)
No Auer rods
MDS-RS-MLD 2-3 1-3 ≥ 15% / ≥ 5%b BM< 5%, Any, unless fulfils all criteria for MDS
PB < 1%, with isolated del(5q)
No Auer rods
b If SF3B1 mutation is present
Swerdlow et al. Revised 4th Edition IARC, Lyon 2017SF3B1 mutation identifies a distinct subset of MDS
Malcovati et al. Blood 2020; 136:157-170Proposed diagnostic criteria for the MDS with mutated SF3B1
Malcovati et al. Blood 2020; 136:157-170SRSF2-mutated neoplasms
+ JAK2 MPN
or MPL (PMF)
MDS/MPN
+ TET2
(CMML)
Mutant
SRSF2P95 + STAG2
MDS with
or RUNX1
or IDH2 EB or AML
+ other MDS
mutant genes without EB
Todisco et al. Leukemia 2020Clonal hierarchy and clone size concur to determine disease phenotype
of SRSF2-mutated neoplasms
Todisco et al. Leukemia 2020Implications of TP53 allelic state for genome stability,
clinical presentation and outcomes in MDS
Bernard et al. Nat Med 2020;26:1549-1556Luspatercept in MDS with RS and SF3B1 mutation
Adverse events
N Engl J Med 2020;382:140-151Luspatercept in MDS with RS and SF3B1 mutation
Indicazioni terapeutiche
Trattamento di pazienti adulti con anemia trasfusione-dipendente dovuta a sindrome mielodisplastica a
rischio molto basso, basso e intermedio, che presentano sideroblasti ad anello con risposta insoddisfacente
o non idonei a terapia basata su eritropoietina
Posologia
La dose iniziale raccomandata è di 1,0 mg/kg somministrata una volta ogni 3 settimane. Nei pazienti che
non sono liberi da trasfusioni di RBC dopo almeno 2 dosi consecutive alla dose iniziale di 1,0 mg/kg, la
dose deve essere aumentata a 1,33 mg/kg. Se i pazienti non sono liberi da trasfusioni di RBC dopo almeno
2 dosi consecutive al livello di dosaggio di 1,33 mg/kg, la dose deve essere aumentata a 1,75 mg/kg.
L’aumento della dose non deve avvenire con una frequenza maggiore di una volta ogni 6 settimane (2
somministrazioni) e non deve superare la dose massima di 1,75 mg/kg ogni 3 settimane.
Riduzione della dose
In caso di aumento di Hb >2 g/dl entro 3 settimane di trattamento con luspatercept in assenza di
trasfusione, la dose deve essere ridotta di un livello di dosaggio. Se l'Hb è ≥11,5 g/dl in assenza di
trasfusioni per almeno 3 settimane, la dose deve essere ritardata fino a quando l'Hb è ≤11,0 g/dl.
N Engl J Med 2020;382:140-151Key messages
• Somatic mutation analysis is potentially useful in the diagnostic work-up of patients with
suspected MDS, in particular in clinical conditions of uncertain classification.
• SF3B1 mutation is going to be recognized as genetically defined disease entity.
• TP53 allelic state is a major prognostic factor, and analysis of biallelic hits should be
implemented in the prognostic assessment of individual patients.
• Luspatercept has been approved for the use in RBC transfusion-dependent patients with MDS-
RS in whom erythropoietin is unsuitable or ineffective.Martin Jädersten Andrea Pellagatti
Antonio Bianchessi
Eva Hellström-Lindberg Jaqueline Boultwood
Elisa Bono
Silvia Catricalà
Anna Cattaneo
Guillermo Sanz
Esperanza Such Yusuke Shiozawa Chiara Elena
Seishi Ogawa Virginia Valeria Ferretti
Anna Gallì
Elisabetta Molteni
Claudia Haferalch Sara Pozzi
Ulrich Germing Gabriele Todisco
Torsten Haferlach
Andrea Kuendgen Martina Sarchi
Silvia Zibellini
Mario Cazzola
Elli Papaemmanuil
Ghulam Mufti
Judith MarshYou can also read

















































