Refractory Heartburn: Approach to the PPI "Addicted" Patient
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Pennsylvania Society of Gastroenterology : September 24, 2010
Refractory Heartburn:
Approach to the PPI “Addicted” Patient
Joel E Richter, MD, FACP, MACG
Richard L Evans Chair and Professor
D
Department
t t off Medicine
M di i
Temple University School of MedicineFailure of PPI Therapy
• 10 ‐ 40% of GERD patients fail to respond symptomatically
to standard once daily dose of PPIs
Fass R. Aliment Pharmacol Ther 2005
• Over 7 years (1997‐2004), Manitoba province had 50%
increase in use of BID PPIs (9.7%
(9 7% to 15.2%)
15 2%)
Targownik LE. Am J Gastroenterol 2007
• Only 58% of GERD patients receiving PPIs report a high
level of satisfaction with their therapy
Bytzer P. Clinical Gastroenterol and Hepatol 2009Confirming GERD as Cause
0% Misc Yes
Asthma
Prevalence of Need to
GERD ENT investigate
role of acid
Chest Pain (pH test)
Non‐erosive Reflux Disease
Erosive Esophagitis
100% NoFailure to Respond to Once a Day PPI • After 4‐8 weeks on single dose AM PPI, 10% to 40% fail to respond • What to do next?? Check compliance Dose appropriately Switch PPI Increase to BID PPI (up to 25% improve)
Sub‐Optimal Proton Pump Inhibitor
Dosing
100 pts
R f
Referred
dbby
PCPs
46% dosed
optimally
p y
Gunaratnam NT, et al. Alimentary Pharmacol Ther 2006FAILURE TO RESPOND TO ONCE DAILY PPI: SWITCH PPI
OR DOUBLE DOSE?
• Multicenter randomized double blind, double dummy trial
• 328 pts with persistent heartburn on lansoprazole 30 mg
• Randomly assigned to esomeprazole 40 mg
l
lansoprazolel 30 mg BID
• Both equally effective for:
‐ heartburn free days:
y 55% eso vs 58% lanso
‐ symptom score improvement for heartburn, acid
regurgitation and epigastric pain
‐rescue antacid use
Fass R et al Clin Gastroenterol and Hepatology 2006Persistent Heartburn Symptoms
S it h or Double
Switch D bl Dose
D PPI ?
PPIs
None Mild Moderate Severe
100
90
80
70
Paatients (%)
60
50
40
30
20
10
0
Esomeprazole Lansoprazole Esomeprazole Lansoprazole
40 mg once daily 30 mg twice daily 40 mg once daily 30 mg twice daily
(n=138) (n=144) (n=138) (n=44)
Week 4 Week 8
P=.25 P=.35
Fass R, et al. Clin Gastroenterol Hepatol. 2006;4:50‐56.Initial Treatment and Diagnostic Approach
GERD Symptoms
Presence of esophagitis is unknown
Single dose PPI
Failure to improve
• Dose appropriately
• Switch to newer PPI
• BID PPI
Failure to improve –
Refractory GERDUGI Findings in Refractory GERD
PPI failures No Treatment
N=105
N 105 N=91
N 91
• Normal 54% p=.04 41%
• Esophagitis 7% p< 001
pInitial Treatment and Diagnostic Approach
Failure to improve –
Refractory GERD
Upper Endoscopy
Esophagitis—10% Non‐esophagitis—90%
1. Pill esophagitis
2. Skin disease with esophagitis
3 Hypersecretor – ZE syndrome
3.
4. CYP2C19 Genotype differences
5. Eosinophilic esophagitisFosamax Pill Esophagitis
PILL INDUCED ESOPHAGEAL INJURY • 92 patients in 5 years—6% EGDs 59 women, mean age 59, 25‐87 • Common symptoms: odynophagia 75% chest pain 60% heartburn 55% vomiting 58% dysphagia 33% hematemesis 15% • Causative pills: NSAIDs/ASA 41% tetracyclines 22% KCL tablets 10% alendronates 9% Other 16%‐‐ascorbic acid, quinidine, antibiotics S Abid et al Endscopy 2005
Eosinophilic Esophagitis
D
Demographics
hi andd Presenting
P ti Symptoms
S t
• Presenting symptoms:
y p g >90% Food impaction:
Dysphagia: p 50%
Heartburn: 33% Chest pain/ vomiting: 20%
Most carry a diagnosis of GERD
Potter JW GIE 2004, Desai TK GIE 2005, Remedios M GIE 2005Prevalence of Eosinophilic Esophagitis in Patients
with Dysphagia
yp g
A Prospective Study
• 376 patients with dysphagia undergoing endoscopy
• Findings:
Total # Biopsied #EoE(%)
Normal 180 102 10(10%)
Reflux esophagitis 84 48 7(14%)
Schatzki ring 28 18 1( 5%)
Stricture 17 8 (
4(50%) )
Suggestive EoE 21 21 8(38%)
Other* 46 30 3(10%)
*achalasia, Barretts, ulcer, cancer
Overall rate: 14.5%
Prasad G Am J Gastro 2007Initial Treatment and Diagnostic Approach
Failure
Failureto
toimprove
improve – –
Refractory GERD
Refractory GERD
Upper Endoscopy
Esophagitis—10%
Esophagitis 10% Non‐esophagitis—90%
Non esophagitis 90%
•Persistent acid reflux
1. Pill esophagitis •Weak or non‐acid GER
2. Skin disease with esophagitis •Sensitive esophagus
3. Hypersecretor – ZE syndrome •Missed GER
•Wrong diagnosis
4. Genotype differences
•Achalasia
A h l i
5. Eosinophilic esophagitis •Gastroparesis
•“Functional” heartburnPPI Resistant Patients—What is the
Clinical
l l Question??
??
• Insuffient PPIs??ROLE OF PH MONITORING IN SYMPTOMATIC
PATIENTS ON THERAPY
30
e pH < 4
25
Total Time
20
15
% Distal T
10 Upper limit of normal
5
0
QD BID QD BID
TYPICAL GERD ATYPICAL GERD
(n = 175) ) (n = 145) )
Sa mer and Vaezi, A m J Gastroenterol 2005Symptom Analysis
SI>50%
SSI>10%Calculation of the SAP
Reflux event
+ ‐
S R
S+R+ S R
S+R‐
mptom
+
Fisher’s exact test
Sym
S‐R+ S‐R‐ two‐tailed
‐
SAP = [1 – p value] X 100%
Weusten BLAM et al. Gastroenterology 1994Concordance of Symptom
p
Assessments with Omeprazole Test
Taghavi SA et al. Gut 2005Sensitive Esophagus (SI+/SI‐)
Response to Omeprazole 20 mg BID for 4 Weeks
All had normal % total time pH,4
Reflux symptom score Days per week of reflux symptoms
Watson, et al. Gut 1997PPI Resistant Patients—What is the
Clinical
l l Question??
??
• Insuffient PPIs??
• Uncontrolled Weak or Non‐Acid
Non Acid Reflux??Impedance pH Monitoring
• Resistance to the flow
of alternating current
Air
E h
Esophageall Li
Lining
i
pedance
Saliva
Food
Imp
RefluxateNumber of Reflux Episodes Off and On
PPIs
Hemmink GJM, et al Am J Gastro 2008Symptom Episodes Off and On PPIs Hemmink GJM, et al Am J Gastro 2008
Etiology of Refractory GERD
Persistent
Acid Reflux 1% ‐ 15%
Refractory
“
“GERD””
Symptoms on
PPIs
Non‐
Acid
Not GERD
GERD 50% ‐ 60%
30% ‐ 40%
GER Controlled on Another Diagnosis
Mainie et al Gut 2006 PPIs
Zerbid et al Am J Gastro 2006Symptom Relief in Patients With and
Without Pathological
g Findings
g of Imp‐pH
pp
Testing
Becker V, et al. Aliment Pharmacol Ther 2007PPI Resistant Patients—What is the
Clinical
l l Question??
??
• Insuffient PPIs??
• Uncontrolled Non‐Acid Reflux??
• Patient does not have acid reflux??
L k for
Look f other
th didiagnoses
Refer patients with extraesopheal complaints
back to ENT, Lung, and Cardiac specialists
Stop unnecessary and expensive PPIsCatheter‐Free pH Monitoring
Placement methods
Transoral during endoscopy
Transoral without endoscopy
Transnasal after manometry
• Capsule device with pH sensor
• Attachment to distal esophageal mucosa
• Radiotransmission of pH dataExtended Recording Time Identifies More
Abnormal GER
Prakash C et al Clin Gastro Hepatology 2005Positive Bravo with Upright
p g RefluxPPIs and Esophageal pH Testing
High Probability GERD Low Probability GERD
• Classic Symptoms
y p • Atypical Symptoms
• Suggestive EGD • Extraesophageal Sx
• Hx of Previous PPI Response • Normal endoscopy
• Previous Failure on PPI
PPBID PPIs
Off PPI
Improved No or Partial Response pH Testing
•Diagnosis Made •R/O Non‐acid Reflux Bravo Capsule
•Transnasal pH
•Impedance pH
Impedance pH on BID PPIsPPIs
Normal
Normal Abnormal pH
↑Non-Acid ↑Acid
•Baclofen •Switch PPIs •GER or no •St •BID PPI Trial
op
•? Surgery •? Surgery GER?? PPI
sAre We Underestimating Acid Reflux? Fletcher etal. Gut 2004
24 Hour Acid Exposure at 6 and 1
cm above
b GE Junction
Bansal, et al. Am J Gastroenterol 2009WRONG DIAGNOSIS
• Achalasia
esophagus minimally dilated
g
diagnosis made byy manometryy
• Delayed gastric emptying
usually postprandial pain and regurgitation are major
symptoms‐not heartburn
• “Functional “ heartburn—up to 58%Stepping Down from Twice Daily PPIs
• Two VA studies have addressed this issue
• Inadomi JM et al: Am J Gastroenterol 2003
117 patients—80% success of 6 months
Cost savings--$33,708 for entire group
• Cote GA et al: Aliment Pharmacol Ther 2007
223 pts switched from lansoprazole 30 mg BID
to rabeprazole 20 mg AM
50%--maintained on once day PPIs
10% off all meds
10%--off
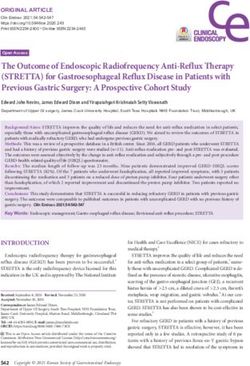
40%--failed shiftRebound Dyspepsia Symptoms
P t
Pantoprazole
l vs Pl
Placebo
b
Pantoprazole Placebo
Niklasson, et al. Am J Gastroenterol 2010Initial Treatment and Diagnostic Approach
Failure
Failureto
to improve
improve – –
GERD
Refractory GERD
Refractory
Upper Endoscopy
Esophagitis—10%
Esophagitis 10% Non‐esophagitis—90%
Non esophagitis 90%
Bravo 48 hr pH Impedance pH
1. Pill esophagitis Low p
probabilityy High
g probability
p y
2. Skin disease with esophagitis
3. Hypersecretor – ZE syndrome •Persistent acid reflux
4. Genotype differences •Weak or non‐acid GER
•Sensitive esophagus
5. Eosinophilic esophagitis
•Missed GER
•Wrong diagnosis
•Achalasia
h l
•Gastroparesis
•“Functional” heartburnTEMPLE UNIVERSITY SCHOOL OF
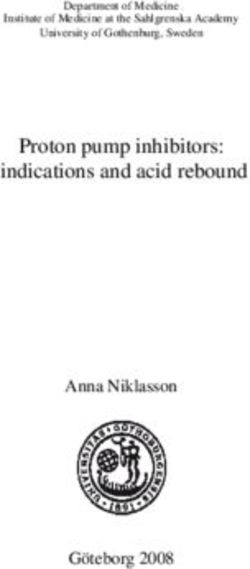
MEDICINEWeekly Dyspepsia Scores
Pl
Placebo
b vs Pantoprazole
P l
Niklasson, et al. Am J Gastroenterol 2010You can also read