Right IOL? What is the - SPECIAL FOCUS - EuroTimes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

SPECIAL FOCUS
CATARACT & REFRACTIVE LENS
February 2019 | Vol 24 Issue 2
What is the
Right IOL?
CATARACT & REFRACTIVE | CORNEA | RETINA | GLAUCOMA
PAEDIATRIC OPHTHALMOLOGY
Treq-Blue
the purest of all
dyes tested
The Treq-Blue stain has been developed
to enable clear visualization of the
capsulorhexis rim. This added
clarity helps prevent
surgical complications.
Dye Impurities measured Purity*
at 530 nm
Treq-Blue 2% 98% • Unmatched purity due to two-step
Competition purification process
Competitor 1 Western Europe 5% 95%
Competitor 2 Western Europe 13% 87%
• High quality, ultra purified,
safe surgical dye
Competitor 3 Southern Europe 20% 80%
Competitor 4 India 18% 82% • Siliconized plunger and finger flanges
for smooth intraocular injection
Conclusion
Treq-Blue is the purest of all dyes tested!
Competitor 1 contained twice as much impurities (measured
at 530 nm) as Treq-Blue. All other dyes contain between six
and nine times as much impurities as Treq-Blue.
* Purity of the dyes was monitored by HPLC chromatography, carried out at Department
of Life Sciences and Chemistry, Jacobs University Bremen, Bremen, Germany.
Treq-Blue Competition
Chromatography show the absence of foreign dyes in Treq-Blue vitreq.com bvimedical.com
P.38
Publisher
Carol Fitzpatrick
Executive Editor
Colin Kerr
Editors
Sean Henahan
Paul McGinn
Managing Editor
Caroline Brick
Content Editor
Aidan Hanratty
Senior Designer
Lara Fitzgibbon
CONTENTS
Designer
Ria Pollock
Circulation Manager
Angela Morrissey
Contributing Editors A EUROPEAN OUTLOOK ON THE WORLD OF OPHTHALMOLOGY www.eurotimes.org
Howard Larkin
Dermot McGrath
Roibeard Ó hÉineacháin
Contributors SPECIAL FOCUS RETINA
P.31
Maryalicia Post
Leigh Spielberg
CATARACT 20 Advances in imaging
Gearóid Tuohy
technology vital in the
Priscilla Lynch & REFRACTIVE LENS understanding and treatment
Soosan Jacob
of neovascular AMD
Colour and Print
W&G Baird Printers 04 Choosing the right IOL
for you and your patient 21 Treating highly myopic
Advertising Sales macular holes
Amy Bartlett 06 New IOLS – a view from
ESCRS
the industry 22 Collaboration with
Tel: 353 1 209 1100 rheumatologists can aid
email: amy.bartlett@escrs.org
08 IOLs and the risk of retinal treatment of uveitis
detachment
Published by the European
23 Opting for vitrectomy
Society of Cataract and earlier in cases of
proliferative diabetic
Refractive Surgeons,
Temple House, Temple Road,
Blackrock, Co Dublin, Ireland.
CATARACT
& REFRACTIVE
retinopathy REGULARS
No part of this publication 31 Hospital diary
may be reproduced without
the permission of the 12 Better understanding GLAUCOMA 33 Books
managing editor. of phaco fluidics
Letters to the editor and other
improves the safety of the
34 Travel
unsolicited contributions are 24 New methods of drug
assumed intended for this procedure
delivery should improve 35 Industry News
publication and are subject
to editorial review and 13 JCRS update compliance and reduce 36 Society News
acceptance. side-effects
ESCRS EuroTimes is not 14 New FLACS approach 37 ESCRS News
can reduce operating time 26 Consensus not universal
responsible for statements
on the net benefit of 38 Random thoughts
made by any contributor.
These contributions are 15 Using corneal refractive minimally-invasive 39 Calendar
presented for review and techniques to correct glaucoma surgeries
comment and not as a high astigmatism
statement on the standard of
care. Although all advertising 28 Structural imaging is
material is expected to being used to complement
conform to ethical medical CORNEA functional testing
Supplement
February 2019
Supplement
February 2019
standards, acceptance does RayOne Trifocal &
not imply endorsement by Sulcoflex Trifocal:
Leading the Way to Offer
16 Newer technologies
More Patients a Trifocal Solution
ESCRS EuroTimes.
PAEDIATRIC
Michael Amon (Austria)
Early results from the new Sulcoflex Trifocal
Fernando Llovet-Osuna (Spain)
RayOne Trifocal: Premium lens outcomes in 150 eyes at Multisite Refractive Clinica Baviera
ISSN 1393-8983
Tiago Ferreira (Portugal)
Prospective comparative study of bilaterally implanted RayOne Trifocal versus
can improve results
Finevison POD F in 60 eyes
Alessandro Mularoni (Italy)
RayOne Trifocal vs PanOptix: Visual Outcomes and IOL stability
Martin Kacerovsky (Czech Republic)
OPHTHALMOLOGY
Comparing RayOne and PanOptix Trifocal outcomes
Georges Cherfan (Lebanon)
Contralateral implantation of the RayOne Trifocal IOL and FineVision Trifocal IOL
Diagnosing and Treating Ocular
in moderate-to-high Surface Disease in Surgical Patients
Supported by an unrestricted educational grant f rom
myopia
29 Updating the classification Included with
18 Rise in endothelial this issue...
keratoplasty may be system for Coats’ disease
As certified by ABC, linked to increase in Rayner Supplement
the EuroTimes average 30 Cross-linking in the
net circulation for the fungal endophthalmitis children with progressive ESCRS/EuCornea Education
10 issues distributed
between 01 January keratoconus Forum Supplement
2017 and 31 December
2017 is 45,316.
EUROTIMES | FEBRUARY 2019
2 EDITORIAL
A WORD FROM OLIVER FINDL MD, MBA, FEBO
GUEST EDITORIAL
How do you know
which IOL to use?
Deciding on the choice of IOL can be
a difficult task, not only for the patient
Oliver Findl but also often for their surgeon
I
am very pleased to be invited to write this editorial for
EuroTimes, which has a special focus this month on IOLs.
As my colleague Soosan Jacob points out in this issue,
deciding on the choice of IOL to implant can sometimes
MEDICAL EDITORS be a difficult task, not only for the patient but also often
for the surgeon who counsels the patient. The numerous types of
available IOLs as well as relative advantages and disadvantages of
each can be challenging.
As a surgeon, my advice to younger colleagues is always to use
the lens that you are most comfortable with, but also the one that
you think is best suited to the individual patient.
As we are all aware, as more exciting technologies come on
the market our patients may have higher expectations of the
improvement in vision that can result after a lens is implanted.
Emanuel Rosen José Güell In my opinion, when talking to our patients before we enter
Chief Medical Editor the operating theatre, we
As a surgeon, my must always stress that
we can never guarantee
advice to younger perfect vision or a dramatic
colleagues is always improvement in vision
to use the lens after a lens is implanted.
We must always be honest
that you are most with our patients and advise
comfortable with them that while we will
always do our best for them,
there is no such thing as the
Thomas Kohnen Paul Rosen perfect procedure. We should follow the motto “underpromise
and overdeliver”.
As ophthalmologists, we are always looking for the next big
innovation and with that in mind, I was also very interested to
read Howard Larkin’s report from the Ophthalmology Futures
Forum held in Vienna in September 2018.
At this forum, Julian Stevens said that designing successful
accommodating IOLs remains daunting and he noted that several
mechanical and flexible gel lens IOL designs have lost accommodative
range over time due to capsule fibrosis. He also pointed out that lens
mineralisation has developed as much as five years after implant. My
personal experience with the so-called accommodating IOLs has been
INTERNATIONAL EDITORIAL BOARD very disappointing, I do not use them at all. Even though electronic
Noel Alpins (Australia), Bekir Aslan (Turkey), accommodating IOLs still appear futuristic, prolonged battery life
may make them realistic sooner than expected.
Roberto Bellucci (Italy), Hiroko Bissen-Miyajima (Japan), This is a discussion that we will return to in the future, and as
John Chang (China), Béatrice Cochener-Lamard (France), always part of the excitement of being an ophthalmologist is looking
Oliver Findl (Austria), Nino Hirnschall (Austria), Soosan Jacob (India), forward to what lies ahead and to see the benefits that years of
research can bring in real life situations in our daily surgeries.
Vikentia Katsanevaki (Greece), Daniel Kook (Germany),
Boris Malyugin (Russia), Marguerite McDonald (USA),
Cyres Mehta (India), Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands), Leigh Spielberg (The Netherlands),
Sathish Srinivasan (UK), Robert Stegmann (South Africa),
Ulf Stenevi (Sweden), Marie-José Tassignon (Belgium),
Manfred Tetz (Germany), Carlo Enrico Traverso (Italy)
Oliver Findl is Secretary of the ESCRS and Chairperson of the
Young Ophthalmologists Committee
EUROTIMES | FEBRUARY 2019
ADVERTISING FEATURE 3
THE MOST BALANCED
TRIFOCAL IOL
STRONG NEAR VISION DESIGN MATTERS
One of the main strengths of Liberty Trifocal IOL (Medicontur) in com- Premium technology also demands premium design. The square edges
parison to other trifocal IOLs is the higher and extended range of of the optic in Liberty (≤10 µ; 360°) are designed to prevent posterior
near vision. Patients achieve a higher depth of focus at near and this capsule opacification (PCO), which is often one of the factors limiting
is the most important for us in a premium IOL implant that aims for success of multifocal IOLs.
spectacle independence. You will always find surprises with multifocal The large size of the IOL and its double loop haptic design are consid-
IOLs, but when you maintain a sufficient range of near vision focus ered to be very important features for postoperative stability, particular-
these surprises tend to be less critical than those experienced with oth- ly for toric MIOLs.
er trifocal IOLs from the past.
After one year of experience with Liberty we have realised that not
EFFICIENCY THROUGH USING all hydrophilic IOLs produce the same rate of PCO. With Liberty, after
OCULAR PHYSIOLOGY 12 months 83% of our patients remained in grade 0 and 17% in grade
We got used to incorrectly labelling IOLs as “pupil-dependent” or “pu- 1 for PCO classification, whereas the previous hydrophilic IOL we im-
pil-independent” while we forget that it is the patient who is “pupil-de- planted achieved percentages of 44% in grade 0, 29% in grade 1 and
pendent”, not the IOL design. The function of the pupil plays an impor- 27% with higher degrees of PCO after the same follow-up time. In short,
tant role in the performance of trifocal IOLs, as it controls the intensity with Liberty we reduced our PCO rates at 12 months.
of light going through the specific lens zones. CONTRAST SENSITIVITY, DYSPHOTOPSIA
Once you measure the pupils you discover that Liberty can maintain AND LIGHT SCATTERING
near vision in low light conditions. We usually test our patients There is always some level of compromise in contrast sensitivity with
in low photopic light conditions (90 lux) and in these conditions they diffractive multifocal IOLs. Light scattering induced by IOLs is caused
achieve a mean of 20/25 for near and 20/32 for intermediate monoc- by each single diffractive step and, depending on the manufacturing
ular vision, and one additional line of visual acuity in binocular vision. quality, these light scatters can occur on multiple points on each step.
Liberty has an intermediate vision weakness in patients with pupils Therefore not only the quality but also the quantity of the manufac-
larger than 3.5 mm in low photopic conditions. In these cases patients tured steps can have a great impact on the amount of correctly utilized
should increase environmental light, which decreases pupil size lead- light energy within the eye and influence contrast sensitivity. Liberty
ing to improved intermediate vision. achieves trifocality with only 7 diffractive rings which is the lowest num-
ber amongst the leading MIOLs today.
We are truly convinced that the 7-ring technology is enough to
maximize visual performance at multiple distances with the
main advantage of avoiding additional light scattering produced by the
narrow peripheral rings in night vision. Although dysphotopsia with
MIOLs is a topic which needs more relevant scientific evidence, theoret-
ical simulations confirmed our expectations of reduced glare and halos
with Liberty.
Nevertheless, in our experience dysphotopsia is a short-term phenome-
non, decreasing in the long-term. Furthermore, while dysphotopsia and
loss of contrast sensitivity are limiting factors for implantation of multi-
focal IOLs today, it should not be forgotten that dysphotopsia and con-
trast sensitivity reduction are also experienced by patients with cataract.
One of our main worries was to determine the proper age and preoper-
ative degree of cataract that can lead to the highest positive experience
after surgery, increasing not only close and intermediate range visual
performance but also producing a positive experience in dysphotopsia
and contrast sensitivity. With Liberty 50% of patients at around 60 years
of age or with a cataract degree of CN1 on the LOCS III scale will actually
improve their contrast sensitivity and experience less dysphotopsia in
comparison to their preoperative vision with best spectacle refraction.
Joaquín Fernández, MD, PhD
joaquinfernandezoft@qvision.es
4 SPECIAL FOCUS: CATARACT & REFRACTIVE LENS
What is the Right IOL?
Choosing and using IOLs can be a daunting task.
Soosan Jacob MD sets out how to go about it
D
eciding on the choice various types of IOLs available, it is wise to can help set the stage for a one-on-one
of IOL to implant can try and find out what activities matter most direct discussion with the patient.
sometimes be a difficult to the patient, how they feel about wearing Understanding the patient’s lifestyle
task, not only for the glasses some/all of the time and to know and visual preferences – whether there is a
patient but also often for if they want/ expect complete spectacle requirement for greater clarity at distance,
the surgeon who counsels the patient. The independence. This conversation helps in intermediate or near vision is important. It
numerous types of available IOLs as well guiding patients towards the possible best is also important to set realistic expectations
as relative advantages and disadvantages choice for them as well as helps in setting regarding a reasonably but not completely
of each can be daunting. realistic expectations preoperatively. glasses-free life, and clear understanding
At the outset, before explaining the Questionnaires and informational videos that some activities will need glasses.
EUROTIMES | FEBRUARY 2019
SPECIAL FOCUS: CATARACT & REFRACTIVE LENS 5
It is generally advisable to focus on good
distance visual acuity in the dominant eye
and either have better intermediate or near
vision in the non-dominant eye depending
on the patient’s requirement.
Taller patients have a slightly farther
requirement for their near point than
shorter patients and the body build should
also be considered.
Possible need for postoperative laser
vision correction for any residual refractive
error should be kept in mind by the
surgeon and informed to the patient. There
should be preoperative clarity about the
financial considerations for this possible
enhancement.
STANDARD MONOFOCALS
I still use monofocal IOLs for many of
my patients who do not want premium
IOLs. Knowing their visual demands
helps to plan better. Patients opting for
monovision or micromonovision have the
dominant eye focused for distance and the
other for near/ intermediate by aiming for
slight myopia. These patients should be
given a monovision trial prior to surgery
to check suitability and to get a first-hand
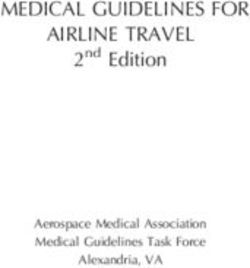
preoperative experience of monovision. Fig A: Toric IOL seen being implanted. Alignment marks on cornea are visible (yellow arrows); B: IOL implanted in-the-bag. Alignment
marks on IOL are visible (black arrows); C: IOL is rotated to lie short of the corneal alignment marks following which viscoelastic is
completely removed; D: IOL is rotated into its final position
PREMIUM IOLS
Before choosing a premium IOL, I always
try to make sure the patient is a good
candidate. A healthy ocular surface allows
accurate IOL power calculations and a
(Alsanza) and Acriva Reviol (VSY option. Standard toric IOLs are available
satisfied patient post-operatively. History,
Biotech) – provide better intermediate in the range of 1.5D to 6.0D cylinder (to
variable measurements and irregular
vision with fewer side-effects. Most also correct 0.75D to 4.75DC). Higher powers
patterns on topography and ocular staining
have toric versions. are available when required. It is important
are important and any dry eye is treated
to assess posterior corneal astigmatism to
pre-operatively if present. A macular OCT Extended Depth of Focus (EDOF) IOLs: avoid errors in IOL calculation.
helps rule out early maculopathy. I also I like EDOF IOLs because of the better
look for large-angle kappa and increased intermediate vision they provide with
higher-order aberrations, which may lesser side-effects of glare, halos or loss FUTURE
result in unhappiness with multifocal of contrast as compared to multifocals. Preoperative decision making needs to
IOLs. Astigmatism on topography and EDOFs would be preferred more than become yet more refined in terms of
keratometry help determine the need for multifocal IOLs in maculopathy or extremely precise IOL power calculations
toric or multifocal toric IOLs. irregular corneas, though monofocals in complex eyes as well as in having
would still be the first choice in these cases. the ability to preoperatively simulate
Multifocals: These IOLs use diffractive realistically to each patient the kind of
They have an elongated focal area, giving
optics and split light into far and near vision they can expect postoperatively from
an extended depth of focus, minimal effect
foci, thereby creating peaks at individual a particular lens choice. This becomes
on peak resolution and give reasonably
focal points that the patient can focus on. especially important with presbyopic IOLs
clear vision at all distances (especially far
However, blurry vision in between the as these patients form the most demanding
and intermediate). However, near vision
two foci and glare and haloes from the group and it would definitely help decrease
with a higher add multifocal is better,
other images are disadvantages. chair time if they could be made precisely
therefore, bilateral EDOF with -0.5 to
I prefer implanting multifocals after aware as to what to expect postoperatively.
-0.75D micromonovision strategy or a
a detailed conversation with the patient Intraoperative and postoperative factors
mix-and-match strategy with EDOF in the
about the expected benefits as well as such as toric IOL alignment, postoperative
dominant eye together with +3.25 near add
the visual symptoms that may occur, rotation etc are other factors which need
multifocal in the non-dominant eye may be
especially during night driving. to be perfected yet more. Another problem
used if the patient desires more near vision.
A mix-and-match policy can help that also needs to be further refined is
I like both the Tecnis Symfony
expand the range of vision offered by postoperative IOL power adjustment
IOL (AMO, California) and the AT
different multifocals. Newer rotationally and the ability to have effective dropless
LARA 829MP (Carl Zeiss Meditec).
asymmetric segmented bifocal IOLs with surgery via canalicular or punctal sustained
Postoperatively, patients can show over
sector-shaped near vision segment give far release drug-delivery systems.
minus values on both autorefractor and
and near (+3D add) focus zones for better
manifest refraction. The highest plus
depth of focus and include the Mplus, Dr Soosan Jacob is Director and Chief
possible should therefore be prescribed by
Mplus X (Oculentis) and SBL-3 (Lenstec). of Dr Agarwal’s Refractive and Cornea
using a fogging technique.
Trifocals – AT LISA (Carl Zeiss Foundation at Dr Agarwal’s Eye
Meditec), FineVision (PhysIOL, Toric IOLs: When astigmatic correction Hospital, Chennai, India and can be
Belgium), PanOptix (Alcon), Alsafit is also required, toric IOLs provide a good reached at dr_soosanj@hotmail.com
EUROTIMES | FEBRUARY 2019
6 SPECIAL FOCUS: CATARACT & REFRACTIVE LENS
NEW IOL
TECHNOLOGIES
There may be many paths forward, though
technical challenges remain.
Howard Larkin reports
M
ultiple intraocular lens
(IOL) technologies,
including multifocal,
EDOF, adjustable,
and both mechanical
and electronic accommodating lenses,
will continue developing over the
next few years as industry and ocular
surgeons seek better treatments for
presbyopia, according to presenters
at the Ophthalmology Futures Forum
Vienna 2018.
However, designing IOLs that
provide reliable and durable presbyopia
correction remains daunting, said Julian
Stevens MRCP, FRCS, FRCOphth, DO
of Moorfields Eye Hospital. He noted
that accommodating mechanical and
flexible gel lens IOL designs that rely on
ciliary contraction to physically move or
reshape lenses often lose accommodative
range as capsules contract and stiffen
over time due to fibrosis.
Similarly, lens implants can develop
long-term unpredictable change with MK Raheja PhD, Jan Willem de Cler and Julian Stevens MRCP, FRCS, FRCOphth, speaking at the Ophthalmology Futures Forum in Vienna
shift in position, and recently for one
manufacturer mineralisation developing
as much as five years after surgery. world what do we need for safety and optical trade-offs that may be more
This severely degrades multifocal efficacy? How many years do you wait acceptable for some patients than others,
performance and makes lens exchange before you say ‘yes, that’s good enough’?” and this takes time to assess. “We need
extremely difficult, particularly following There should be a European database to better understand patient needs as well
posterior capsulotomy, Dr Stevens for long-term follow-up at 10, 15 and 20 as physiology of their eye to increase the
said. Attempts to induce multifocality years and beyond, he believes. probability of success with the presbyopia
in adjustable lenses after implantation solution that we provide”.
can result in optical complexities and MULTIPLE SOLUTIONS Laurent Attias, senior vice president
optical irregularity, which is challenging How much development time is needed for corporate development at Alcon, sees
for patients and very difficult to correct, depends on the technology, said MK merit in continuing development of light-
he added. Raheja PhD, head of ophthalmic implants splitting, accommodating and adjustable
Detecting such problems lengthens R&D for Johnson & Johnson Vision. lenses. “Each has its own challenges,” he
development time, but is necessary, Mechanical accommodating designs rely said. Multifocals must balance a mix of
Dr Stevens said. “Given that we are on performance of the capsular bag and near, intermediate and far vision while
implanting these lenses in younger and ciliary muscles, which can deteriorate with minimising dysphotopsias, mechanical
younger people for refractive reasons, time and therefore require more time to accommodating lenses must preserve
how long would you like to see outcomes demonstrate efficacy. Multifocal, EDOF an acceptable range of movement and
data? Forget the regulations, in the real and adjustable lens technology involves the precision and long-term safety
EUROTIMES | FEBRUARY 2019
SPECIAL FOCUS: CATARACT & REFRACTIVE LENS 7
of adjustable lenses must be proven. not that far off… we’ve seen [lifespan]
“The good news is each are viable improvements from four years to 20 years.”
routes toward the same golden egg Rapid progress is also being made on
called presbyopia.” other issues that will make electronic
Dr Stevens believes electronic accommodating lenses usable. These
accommodating IOLs that adjust refractive include managing the speed and precision We need to simplify
power by varying lens refractive index will
be an attractive solution. However, battery
of accommodation, which are critical to
patient acceptance, and developing foldable
using [presbyopia-
technology must improve to provide a electronics that will enable insertion correcting IOLs]
40-to-50-year lifespan with enough energy accommodating IOLs through monofocal-
density to be light enough to implant. size incisions of 2.5mm or so. and simplification
“Once that comes in it will be a total game- In fact, Attias sees electronic will take time. We
changer,” he said. However, any electronic accommodating IOLs pulling ahead of
lens implant will not be compatible with contact lenses due to the challenges of are counting on
MRI scanning, and this will likely be a
serious drawback.
keeping contacts comfortable. “Unless you
solve for comfort, nothing else matters.”
the early adopters
Alcon is making progress on electronic Raheja believes that future presbyopic to demonstrate the
accommodating IOLs and contact lenses, IOL solutions may combine approaches.
Attias said. “The battery technology is Every technology has its advantages concepts
and limits and all are at an early stage, Julian Stevens, MRCP, FRCS, FRCOphth
he said. “We need to push forward on
every front.”
SIMPLIFYING SURGERY
According to Carl Zeiss Meditec, another this becomes a barrier to use. “We need
critical factor in boosting acceptance of to simplify using [presbyopia-correcting
We need to better presbyopia-correcting lenses is providing IOLs] and simplification will take time.
understand patient diagnostics that support predictable We are counting on the early adopters to
patient outcomes. The company reports demonstrate the concepts.”
needs as well as that it is very important not to look at Dr Stevens said lenses optimised to fit
physiology of their the IOL in isolation as it is also a process
of diagnostics, using information to
into a precision-cut anterior capsulotomy
are a step toward increasing success
eye to increase the perfect the technique so the end result is because they allow centring the lens
what is expected. precisely and permanently on the visual
probability of success Failing to recognise this can lead to axis. “You don’t have lateral movement
with the presbyopia the avoidance of prescribing presbyopia- and you don’t have decentration.” He
correcting IOLs not because of any problem believes that optimising lens design to
solution that with the lens itself, but a lack of knowing take advantage of the potential precision
we provide how to implant it accurately.
Attias agreed. Even today’s toric lenses
offered by femtosecond laser technology
will eventually increase use of presbyopia-
MK Raheja, PHD require extra time and skill to implant, and correcting and other speciality lenses.
The beginning
of a new era.
«A clever design is not only pleasing
on the eye. A clever design integrates
well into your workflow and seam-
lessly becomes part of your system.
Think about mobility, simplicity
and safety significantly to enhance
at
Visit us efficiency.»
019
APAO 2 8
3
Booth Z Thomas Köppel
CEO This AG
Please note: Device is not yet approved. It has been
submitted for EU-market (CE) approval but cannot
be purchased until approval has been granted. www.sophi.info
EUROTIMES | FEBRUARY 2019
8 SPECIAL FOCUS: CATARACT & REFRACTIVE LENS
Refractive surgery
Pentacam® AXL for high myopia
The All-in-One Differences in risk something to
consider when weighing alternatives.
Unit! Cheryl Guttman Krader reports
E
ach of the surgical options for correcting high
Visit our booth at ESCRS myopia has a unique set of pros and cons, but
Winter Meeting, Athens! only refractive lens exchange (RLE) appears
to be associated with an increased risk of
retinal detachment.
Speaking at the 18th EURETINA Congress in Vienna,
Austria, Andrzej Grzybowski MD, PhD, MBA, reviewed
the literature on risk of retinal detachment in high
myopes and with cornea and lens-based refractive surgery
techniques. He concluded that RLE increases the risk
significantly, while phakic IOL implantation does not.
Although excimer laser keratorefractive surgery might be
excluded from consideration for other reasons, there is no
evidence that it increases the risk of retinal detachment,
said Dr Grzybowski, Chair of Ophthalmology, University of
Warmia and Mazury, Olsztyn, Poland.
According to published reports, the risk of retinal
detachment in non-operated myopic eyes ranges between
0.71% and 3.2%. Compared with the general population, the
risk of retinal detachment is estimated to be about 50-fold
higher in the subgroup with myopia -15D.
“In addition, the risk of retinal detachment in myopes
is particularly high during the second, third and fourth
decades of life, mainly owing to atrophic retinal holes,” Dr
Grzybowski said.
REFRACTIVE SURGERY-RELATED RISK
In an article reviewing published data on RLE, Dr
Grzybowski and colleagues found that the reported rate
of retinal detachment ranged from 0% in some studies to
8.1% in one paper (Alió JL, Grzybowski A, Romaniuk D.
Eye Vis (Lond). 2014 Dec 10;1:10.).
“It is quite well known that phacoemulsification itself
increases the risk of retinal detachment by 10-fold, and
young age is one of the risk factors,” said Dr Grzybowski.
The proposed mechanism involves induction of
Optical biometry and inbuilt IOL posterior vitreous detachment, which might occur in
formulas for any eye status close to 80% of highly myopic patients undergoing RLE,
he explained.
Use Total Corneal Refractive Power (TCRP) keratometry Traumatic effects resulting from placement of the
to account for individual total corneal astigmatism of microkeratome suction ring combined with the shock-
every patient and select suitable aspheric, toric and wave and thermal effects of the excimer laser create
multifocal IOL candidates more confidently. Perform a mechanistic basis for an increased risk of retinal
swift IOL calculations using the inbuilt IOL Calculator, detachment after excimer laser keratorefractive surgery.
However, the rate of retinal detachment after LASIK for up
avoid manual transcription errors and optimize your
to -10D myopia was very low in a study of almost 12,000
personal constants. eyes (Arevalo JF, Lasave AF, Torres F, Suarez E. Graefes
Included: Barrett IOL formulas and customized Arch Clin Exp Ophthalmol. 2012;250(7):963-970.).
“Studies comparing PRK and LASIK found no difference
formulas for post-corneal refractive patients
between the procedures in the rate of retinal detachment,”
Dr Grzybowski said.
Only a few studies evaluated the rate of retinal
detachment in myopic eyes that underwent phakic
www.pentacam.com IOL implantation, and they did not find an increased
Follow us! risk, he added.
Andrzej Grzybowski: ae.grzybowski@gmail.com
EUROTIMES | FEBRUARY 2019Seeing to succeed
in cataract surgery.
ZEISS OPMI LUMERA 700
»We are able to give our
patients a much more
predictable outcome. That
I think is key for today’s
cataract surgeons, the
ability to predict and deliver
what we tell them we’re
going to do.«
Ronald Yeoh, MD
Eye and Retina Surgeons
Camden Medical Centre, Singapore
Passionate about his profession, Dr. Yeoh is committed to
providing cataract patients with the best possible outcome.
The superb imaging and markerless toric IOL alignment
capabilities of the OPMI LUMERA® 700 and CALLISTO® eye
from ZEISS enable him to deliver on patient expectations.
We share his commitment to his calling. What´s your calling?
www.zeiss.com/mycalling10 ADVERTISING FEATURE
HOYA Evening Symposium, Vienna 2018
Clinical Research and
Product Innovation Update
At a symposium held during the 36th ESCRS Congress in Vienna, a group of world experts on
intraocular lens performance met to provide an update on HOYA’s research into IOL technology,
with presentations on the new multiSert™ injector system and studies comparing the Vivinex™
lens to other lenses in terms of rotational stability, PCO and glistenings
Performance of the new HOYA multiSert™ Preloaded
Injector System for the Vivinex™ IOL
Gerd U Auffarth MD FEBO
International Vision Correction Research Centre (IVRC)
The David Apple International Laboratory University Eye Clinic
University Eye Clinic Heidelberg, Germany
T
he new multiSert ™ Injector System very controlled and consistent delivery
for the Vivinex™ IOL provides an of the IOL into the capsular bag for both
increased range of flexibility to push and screw modes. The multiSert™
the cataract surgeon, allowing injection injector system adds further options with
with either a single-handed push mode an adjustable mechanism, the insert
or a two-handed screw mode. Previous shield, that serves as a depth-limiting
preloaded injectors from the HOYA iSert® device when choosing to perform a wound- The glistening-free hydrophobic Vivinex IOL
series like model PY-60AD or model 251 assisted IOL implantation. Moreover, the
were designed for the two-handed screw Vivinex™ lens comes preloaded with the
mode only. device, which requires only a very simple surgery. Screwing two-handed or
The multiSert™ injector’s tip has an preparation prior to the injection. pushing single-handed are both possible
outer diameter of 1.7mm, allowing delivery In summary, by combining the options with or without use of the advanced
of the IOL into the capsular bag through of both a push and a screw mode for IOL insert shield for insertion through the
a sub-2.2mm incision. At The David Apple injection, the 4-in-1 multiSert® provides wound tunnel or direct implantation in
International Laboratory, we observed a the best of two worlds in cataract the capsular bag.
Defining and Assessing True Rotational degrees. Similarly, in eyes with the
Stability of Toric IOLs Johnson & Johnson Vision TECNIS®
1-Piece IOL the mean rotation was only
Rupert Menapace, MD 2.2 degrees but there were two outliers
Professor of Ophthalmology & Optometry with around 40 degrees of rotation.
University of Vienna Medical School, Vienna General Hospital, Vienna, Austria Furthermore, in eyes with the Bausch +
Lomb EnVista® lens there was a mean
S
rotation of 3.2 degrees but there were
ignificant secondary rotation of an position directly after implantation and outliers of up to 44.9 degrees.
implanted toric lens once it has then at one hour, one day, one week, Most of the rotation with all lens types
been implanted is uncommon in one month and six months afterwards, occurred in the first hour after surgery
most of the leading IOL models on the using haptic junctions and fixed and almost none occurred after the first
market, but some of the lenses have landmarks on globe as reference points. postoperative week. That is because
outliers that can be enough to annihilate We found that in eyes with the HOYA by one week the capsule is closed and
the anti-stigmatic effect of the lens. Vivinex™ IOL, the mean rotation at to-six by one month the capsular leaves have
Therefore, it is important to determine months was only 1.5 degrees, and in no fused. Therefore, what counts is not
the true rotational stability of a lens. eyes was there rotation greater than the deviation from the intended axis but
We have compared the amount of five degrees. By comparison, although the positional change starting from the
postoperative rotation for each of four the mean rotation in eyes with the Alcon end of surgery, and not from one hour,
different single-piece hydrophobic IOL AcrySof® IQ lens was only 1.7 degrees one day or even later. What also count
models. The patients all underwent at six months postoperative, in a few are the outliers, not the mean values or
examination of their implanted lens outliers the lens rotated by up to 15.8 standard deviations.ADVERTISING FEATURE 11
Comparative PCO Performance Analysis of the HOYA mimic post-surgical inflammatory
events, and allows for the observation
Vivinex™ IOL and a Leading Competitor and definitive measurement of different
Michael Wormstone FARVO phases of PCO formation following IOL
implantation in an in-vitro setting.
Professor of Ophthalmology, School of Biological Sciences,
This improved graded culture system
University of East Anglia, Norwich, UK
has been used to compare the PCO-
T
performance of the Vivinex™ lens with
he human capsular bag model contributions from Prof David Spalton’s that of a leading competitor in a series
is one of the premier in vitro group in St Thomas’ Hospital in London. of match-paired human capsular bag
systems to understand the Based on the findings of studies experiments. The team found cell growth
biological regulation of PCO and how using flare measurements of protein on the posterior capsule to be slower
implanted IOLs can influence this concentrations in the anterior chamber on the HOYA Vivinex™ when compared
common condition. This model was following cataract surgery, the team at to the leading competitor. Cell growth
first pioneered by a team of scientists UEA have developed a graded culture on the posterior capsule was retarded,
and clinicians at the University of East system whereby the delivery of human light-scatter in the central visual axis
Anglia (UEA) in the 1990s and has serum and transforming growth factor-β was found to be lower and growth on the
developed in to several iterations since, levels is carefully controlled over time. IOL surface was markedly reduced with
through continued work at UEA and This approach is designed to closely Vivinex™ versus the leading competitor.
Comparison of Two Hydrophobic Intraocular Lenses: A Prospective Study
Dominique Monnet MD PhD
Université Paris Descartes, l’hôpital Cochin, Paris, France
T
he two-year interim results of At two years’ follow-up in 34 eyes, out so far was in an eye implanted
a prospective, ongoing three- we found that both lenses performed with the AcrySof® lens. The Vivinex™
year multi-centre study we are almost identically in terms of refractive lens also developed significantly less
carrying out indicates that new Vivinex™ predictability and stability. The mean “glistenings”, which by two years were
IOL is highly resistant to PCO and is less BCDVA of both lenses was equivalent absent or of low-grade density in eyes
prone to glistening than the AcrySof® with 0.0±0.1 logMAR at two years. with the Vivinex™ lens but were present
lens. The trial involves an intent-to- The two lenses also had identical and and of a high-grade density in most
treat population of 85 patients with a very low, quantitative PCO scores. eyes with the AcrySof® eyes.
mean age of 73.6 years. All underwent However, there was a trend towards
randomised implantation of the Vivinex™ less PCO in the Vivinex™ group, and
IOL in one eye and the implantation of the only YAG-laser capsulotomy carried
the AcrySof® lens in their fellow eyes.
The two IOLs investigated are similar in
being single-piece lenses composed of a
hydrophobic material and having a
sharp optic edge. In the Vivinex™
lens, the optic’s posterior surface
has additionally undergone an “active
oxygen” surface treatment.
The 4-in-1 multiSert™ preloaded delivery system
How to Optimise Monovision Outcomes?
Peter Hoffmann MD myopised. However, with a 1.0D add,
myopisation of the non-dominant
Castrop-Rauxel, Germany
eye resulted in a slightly lower
W
intermediate visual acuity than when
e tested the visual acuity “...63% of participants the dominant eye was myopised. In
and subjective reports of addition, 63% of participants reported
46 bilaterally pseudophakic
reported a worse sensation a worse sensation of binocularity with
patients under simulated monovision of binocularity with a a myopisation of 1.0D compared to
conditions. We measured their myopisation of 1.0D compared emmetropia, compared to only 2%
emmetropised monocular and binocular when myopised by 0.5D. Moreover,
visual acuity at 6m, 80cm and 40cm, to emmetropia...” in a study of fusional amplitude in
first with 0.5D add in the dominant eye 12 bilateral pseudophakic patients,
and then with the same add in the non- We found that with a binocular acuity we found that good binocularity
dominant eye. We also performed the with a 0.5D add was identical whether would be achieved in most eyes if
same sequence of testing with a 1.0D add. the dominant or non-dominant eye was anisometropia was limited to 0.75D.12 CATARACT & REFRACTIVE
Cataract and glaucoma
Optimised fluidics key to safe and uncomplicated surgery in glaucomatous eyes.
Roibeard Ó hÉineacháin reports
T
he fluidics of the phacoemulsification
system in cataract patients with
glaucoma should be optimised to
ensure a stable, low-pressure anterior
chamber during surgery and prevent
damage to the optic nerve, Roberto Bellucci MD,
Verona, Italy, told the 36th Congress of the ESCRS
in Vienna.
“Better understanding of phaco fluidics
improves the safety of cataract surgery especially in
glaucomatous eyes,” he emphasised.
Microincision cataract surgery (MICS) is the
best option in glaucomatous eyes because it has
gentler fluidics than standard incision surgery,
whether using a Venturi or peristaltic pump settings.
Femtosecond laser-assisted cataract surgery is
indicated in glaucoma eyes with shallow anterior
chambers, pseudoexfoliation and low endothelial
cell counts, he said.
FLUIDICS OPTIMISATION
But what is most important is the optimisation
of fluidics to avoid IOP elevation and anterior Roberto Bellucci MD
chamber oscillation, which can further damage
the already compromised optic nerve, Dr Bellucci
stressed.
Using a high bottle height is a poor solution. Raising the the anterior chamber. Furthermore, leakage provides a
bottle height one metre above the eye will increase the pressure reservoir of fluid, which helps in avoiding chamber collapse
within the anterior chamber to 70 mmHg. If the bottle is raised when aspiration increases abruptly. It also maintains some
to 1.3m the pressure will rise to 100 mmHg. Raising the bottle fluid stream within the anterior chamber during occlusion
in this way will not only increase the patient’s pain but will also or clogging.
increase the oscillation of the anterior chamber depth. That,
in turn increases the difficulty of the surgery and raises the PRESSURE SENSORS
risk of complications and damage to the optic nerve head. The The latest evolution in phaco fluidics control are irrigation
potential complications include posterior capsule rupture and systems that use feedback from sensors that detect the anterior
cystoid macular oedema. chamber pressure. The result is better and more delicate fluidics
Fluidics optimisation can instead be achieved by reducing control. The increase of vacuum that the system allows and the
the aspiration ports and system hysteresis, separate control of small tip improve fragment hold-ability, and the reduced flow
aspiration and ultrasound, avoiding occlusion, allowing some improves fragment follow-ability.
leakage and varying infusion pressure according to the pressure “What is nice is that you can select the IOP you want; I use
in the anterior chamber, Dr Bellucci summarised. 25mmHg, which corresponds to a bottle height of 40mmHg.
In MICS procedures, rigid low hysteresis tubing must be Nobody was using such low bottle heights before these machines
used, together with low hysteresis pumps possessing small came along,” Dr Bellucci said.
ports and pressure sensors and double venting systems. The choice of IOL also requires special consideration in cataract
Separate control of aspiration and ultrasound allows the patients with glaucoma. For example, “soft” hydrophilic IOLs with
activation of ultrasound power at any vacuum level and weak haptics are contraindicated in eyes with weak zonules, as in
also avoids excessive pressure within the anterior chamber eyes with pseudoexfoliative glaucoma, because they will not resist
and resulting hydration of the vitreous. Venturi pumps and capsular bag contraction.
peristaltic pumps perform equally well in separately controlled IOLs that decrease contrast sensitivity like multifocal IOLs
aspiration and ultrasound systems, provided that they are are also contraindicated in patients with glaucoma. On the
properly adjusted. other hand, aspheric IOLs that enhance contrast sensitivity are
The use of micro-pulse ultrasound delivery and small phaco beneficial in such cases.
tips will generate very small fragments, thereby avoiding At the conclusion of surgery, thorough viscoelastic
occlusion of the aspiration line. Phaco tips with transverse/ removal is essential to avoid post-op IOP spikes. IOP should
rotational needle movement appear to work very effectively be brought under control the same day, with attention
when used with a peristaltic pump, Dr Bellucci said. to possible aqueous misdirection syndrome, he advised.
He added that some incision leakage during surgery can
be helpful. It avoids excessive pressure and deepening of Roberto Bellucci: robbell@tin.it
EUROTIMES | FEBRUARY 2019CATARACT & REFRACTIVE 13
CONGRATULATIONS!
THOMAS KOHNEN 2017 OBSTBAUM AWARD FOR
European editor of JCRS BEST ORIGINAL ARTICLE
JCRS HIGHLIGHTS Functional magnetic
resonance imaging to assess
VOL: 44 ISSUE: 12 MONTH: DECEMBER 2018
neuroadaptation to multifocal
PREDICTING POSTERIOR CAPSULE RUPTURE intraocular lenses
Anterior segment OCT (AS-OCT) can successfully predict the risk for
posterior capsule rupture during phacoemulsification in eyes with
Andreia M. Rosa, Ângela C. Miranda,
posterior polar cataract, a recent study suggests. The prospective Miguel M. Patrício, Colm McAlinden,
observational study included 64 eyes of 62 patients with posterior Fátima L. Silva, Miguel Castelo-Branco,
polar cataract who had phaco. All underwent preoperative and Joaquim N. Murta
AS-OCT to assess the integrity of the posterior capsule. Phaco
was performed by the same surgeon, who was masked from the
J Cataract Refract Surg 2017; 43:1287–1296
AS-OCT findings, and who evaluated the integrity of the posterior
capsule intraoperatively. Preoperative AS-OCT showed eight eyes
(12.5%) to have probable posterior capsule dehiscence and 56 2017 ROSEN AWARD FOR
eyes (87.5%) to have intact posterior capsules. Intraoperatively, the
surgeon noted posterior capsule dehiscence in five eyes (7.8%) and BEST TECHNICAL ARTICLE
an intact posterior capsule in 59 eyes (92.2%). The sensitivity and
specificity of AS-OCT for detecting posterior capsule dehiscence
was 100% and 94.92%, respectively. The negative predictive value
Artificial iris implantation
of AS-OCT was 100%. GP Kumaret al., JCRS, “Can preoperative
anterior segment optical coherence tomography predict posterior
in various iris defects and
capsule rupture during phacoemulsification in patients with posterior lens conditions
polar cataract?”, Vol. 44, Issue 12, 1441-4.
Christian Mayer, Tamer Tandogan,
Andrea E. Hoffmann, and Ramin Khoramnia
HOAs AND HIGH MYOPIA
A new study looking at corneal aberrations in high myopes J Cataract Refract Surg 2017; 43:724–731
provides support for using aspheric IOLs in those cataract
patients. The study of 287 high myopia patients found no
negative primary spherical aberrations of the total or anterior The JCRS as we know it today was born out
corneal surface. The study did note differences between the of the amalgamation of two peer-reviewed
myope group and control group in terms of central corneal
journals, the Journal of Cataract & Refractive
thickness, astigmatism, primary spherical aberration, vertical
coma and oblique trefoil. However, these differences were not Surgery from the ASCRS and the European
consistent between different age subgroups. Higher-order Journal of Implant and Refractive Surgery from
aberrations were correlated with age. Posterior corneal vertical ESCRS. The merged journal, which marked
coma was correlated with axial length. M Zhang et al, JCRS,
its 20th year in 2016, is the direct outcome
“Analysis of corneal higher-order aberrations in cataract patients
with high myopia”, Vol. 44, Issue 12, 1482-90. of the spirit of friendship and cooperation
that developed between the two societies, in
particular between the editors at the time of
CXL – ON OR OFF?
the merger, Stephen A. Obstbaum, MD, in the
Epi-off corneal collagen cross-linking might be better than
the transepithelial technique for the treatment of progressive United States and Emanuel S. Rosen, MD,
corneal ectasia in terms of steepest keratometry, a new meta- FRCSEd, in Europe.
analysis concludes. The meta-analysis included seven randomised
clinical trials involving 505 eyes that met eligibility criteria for In honor of their passion and foresight, the editors
the review. The epi-off CXL group showed significantly better are pleased to announce the creation of two
outcomes in post-op changes in maximum keratometry during annual awards for articles published in the JCRS,
one-year observation periods. Transepithelial CXL resulted in
significantly greater post-treatment central corneal thickness and
the Obstbaum Award for Best Original Article
best spectacle-corrected visual acuity. The presence of a post-op and the Rosen Award for Best Technique Article.
demarcation line was significantly more frequent after epi-off
CXL than that after transepithelial CXL. H Kobashi et al., JCRS,
“Transepithelial versus epithelium-off corneal crosslinking for
corneal ectasia”, Vol. 44, Issue 12, 1507-16.
Become a member of ESCRS to receive a copy of EuroTimes and JCRS journal
EUROTIMES | FEBRUARY 201914 CATARACT & REFRACTIVE
FLACS and
dense cataract
Randomised, controlled study finds
grid pattern reduces phaco time
and endothelial cell loss.
Howard Larkin reports
F
ragmenting very dense cataract nuclei with a
femtosecond laser using a grid pattern before
European Union phacoemusification significantly reduced effective
phaco time (EPT) and endothelial cell count loss
(ECC) compared with manual phacoemulsification
Web-Based Registry or femtosecond laser-assisted cataract surgery (FLACS) using
a 16-segment fragmentation approach, Soon-Phaik Chee MD
told the 36th Congress of the ESCRS in Vienna.
In a prospective, randomised, controlled study, Dr Chee
The aim of the project is to build a
and colleagues at the Singapore National Eye Centre assigned
common assessment methodology 94 patients with nuclear cataracts of LOCS III NO grade 5, 6
and establish an EU web-based registry or more to receive manual phacoemulsification, FLACS using
and network for academics, health a 600-micron grid fragmentation pattern (FLACS grid) or
FLACS using a 16-segment pattern (FLACS 16) followed by
professionals and authorities to assess
phacoemulsification in a 2:1:1 ratio.
and verify the safety quality and All FLACS patients were treated with a Victus
efficacy of corneal transplantation. femtosecond laser (Bausch + Lomb, Munich, Germany), and
all patients received phacoemulsification using a Stellaris
system (Bausch + Lomb, Rochester, New York, USA). All
procedures were done by Dr Chee using a direct phaco
Join
chop technique. The study examined corneal safety using
the three approaches, examining effective phaco time and
endothelial cell loss one month after surgery.
EPT RESULTS
The study found nuclear density and treatment method both
the ECCTR Registry affected effective effective phaco time, Dr Chee reported.
Perhaps not surprisingly, the 49 cases with NO5-6 required
significantly less mean phaco time than the 44 of higher than
Track
grade 6 (p6 group.
These results vary from two non-randomised studies in
the literature, which found reduced effective phaco time and
endothelial cell with FLACS, Dr Chee noted. However, these
studies examined softer cataracts, and used 300-micron grid
patterns and a stop-and-chop phaco approach, which may
ECCTR is co-funded by have influenced the outcomes (Hatch KM et al. J Cataract
Refract Surg. 2015;41:1833-1838. Chen X et al. J Cataract
Refract Surg. 2017;42(4):486-491.).
Co-funded by “FLACS grid but not FLACS 16 segment significantly
the Health Programme
of the European Union reduced mean effective phaco time and lowered mean
endothelial cell loss at one month compared with manual
phacoemulsification in dense cataracts,” Dr Chee concluded.
Soon-Phaik Chee: chee.soon.phaik@snec.com.sg
EUROTIMES | FEBRUARY 2019CATARACT & REFRACTIVE 15
Corneal
astigmatism options
Correction of high astigmatism is now feasible with a variety of
corneal refractive techniques. Roibeard Ó hÉineacháin reports
S
urgeons have a number of corneal refractive procedures PRK VS LASIK VS SMILE
to choose from that can produce good results in eyes Photoablative techniques like PRK and LASIK can correct
with regular and irregular high astigmatism, Jesper higher amounts of astigmatism and with greater accuracy than
Hjortdal MD told the 36th Congress of the ESCRS in incisional techniques and their results appear to be roughly
Vienna, Austria. comparable, he noted. In a study comparing the two techniques
The general aim in correcting regular astigmatism is to flatten in eyes with more than 3.0D of astigmatism, there was no
the steep axis of the cornea or compensate for the astigmatism statistically significant difference between the efficacy and the
intraocularly with a toric IOL, said Dr Hjortdal, Aarhus University two techniques had similar predictability. That is, in the PRK and
Hospital, Denmark. LASIK groups, 39% and 54%, respectively, had less than 0.5D of
Whichever technique is used, accurate determination of the astigmatism postoperatively, and 88% and 94% had less than
correct axis pre- and 1.0D (Katz et al, J Refract
intraoperatively is Surg. 2013;29(12):824-831).
necessary to bring about The results with SMILE®
the desired effect. If the appear to be comparable to
actual alignment axis is LASIK in eyes with high
off the target alignment myopic astigmatism. In a
axis by 30 degrees, the recent retrospective study,
procedure will have no Dr Chan and his associates
anti-stigmatic effect at all, found no significant
he pointed out. between-group difference
Indications for in uncorrected distance
surgery in eyes with high visual acuity and manifest
astigmatism include poor spherical equivalent in
vision with spectacles, patients undergoing the
intolerance or discomfort procedures for myopic
with contact lenses and astigmatism. At three
concomitant cataract. months, 90% and 95.4%
The corneal surgical of eyes in the SMILE and
techniques include LASIK groups, respectively,
incisional and photo- Jesper Hjortdal MD
were within ±0.5D of the
ablative varieties, and attempted cylindrical
most recently stromal lenticule excision, he said. correction (p=0.423) (Chan et al, J Cataract Refract Surg. 2018
Jul;44(7):802-810).
LIMITED EFFECT OF ARCUATE KERATOTOMY
Topography-supported customised laser PRK is another
The oldest of the techniques currently in use is paired arcuate technique that has been used in eyes with irregular astigmatism
keratotomy. The approach involves the creation of almost fully due to PK or keratoconus. However, early results in a study
penetrating incisions in the peripheral steep axis of the cornea. It involving penetrating keratoplasty patients showed significant
can achieve very good reductions in high astigmatism, although haze following the procedure.
it can leave considerable amount of residual astigmatism in More recently Dan Reinstein MD, PhD, UK, has introduced
highly astigmatic eyes and there can be considerable scatter in the transepithelial phototherapeutic keratectomy (TE-PTK).
technique’s predictability. The ablation is based on population epithelial thickness
As an illustration, he cited a study he and his associates measurements determined using very high-frequency digital
conducted 20 years ago involving highly astigmatic post-PK eyes. ultrasound. Results to date with the technique suggest that
It showed that arcuate keratotomy reduced mean keratometric TE-PTK can be a safe and effective method of reducing
cylinder by 50%, from 7.0D to 3.25D. However, the procedure was stromal surface irregularities by taking advantage of the natural
safe and he noted that the greater the magnitude of preoperative masking effect of the epithelium.
astigmatism, the greater was the anti-astigmatic effect (Hjortdal et Last but not least are intracorneal ring segments (ICRS) for
al, Acta Ophthalmol. Scand. 1998: 76: 138-141). the treatment of keratoconus. Several studies confirm safety and
In a more recent study arcuate keratotomy incisions produced efficacy of ICRS. However, predictability remains a key challenge
with a femtosecond laser produced a similar reduction in corneal and current nomograms are insufficient to cover all cases.
astigmatism, from 9.45D to 4.64D, and despite the precision of the
technique there remained some scatter in the results (Loriaut et al, Jesper Hjortdal: jesper.hjortdal@clin.au.dk
Cornea 2015:34:1063-1066).
EUROTIMES | FEBRUARY 2019You can also read