Drug Price Forecast January 2019 - Vizient
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Drug Price Forecast January 2019 © 2019 Vizient, Inc. All rights reserved.

Table of contents Executive summary 3 Projected timeline and approvals 10 A closer look by segment 12 Acute care 12 Non-acute care 13 Specialty pharmaceuticals 16 Pediatrics 19 Key therapeutic class summaries 24 Oncology 24 Infectious disease agents 29 Immunomodulators and disease-modifying therapies 36 Plasma critical care products: IgIV and albumin 40 Hot topics 42 Overcoming the shortage of solutions to the drug shortage problem 42 Will favorable polices usher in a ‘biosimilar wave’ in 2019? 46 New technology add-on payment 52 Combating counterfeit drugs 53 Exploring the reasons for rising drug prices 56 Continued challenges and new options in the opioid crisis 57 Conclusions 60 Contributors 62 © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 2

Executive summary
The January 2019 Drug Price Forecast is our best estimate of the change in the cost of pharmaceuticals that
participants in the Vizient Pharmacy Program will be purchasing between July 1, 2019, and June 30, 2020. The
forecast focuses on pharmaceutical products used across multiple health-system settings, including inpatient and
non-acute environments, and provides a year-over-year estimate of the expected price change.
Price change predictions for contract and noncontract product segments are shown in Table 1, along with the
overall drug price inflation number for existing drugs as calculated by Vizient.
Table 1. Summary of projected drug price inflation
Estimated price
change weighted by
Product group Vizient purchases, %
Contract purchases 1.12
Noncontract purchases 3.16
Total weighted average drug price inflation estimate 4.28
Estimates based on Vizient member data.
In addition to price changes, the American Journal of Health-System Pharmacy advises that other factors — such
as volume changes and new product introductions — must be considered when preparing a drug budget.1
According to a May 2018 article, volume and mix decreased 5 percent in nonfederal hospitals in calendar year
2017, but increased 4.6 percent in clinics (including both physician offices and outpatient clinics).1 In addition, the
introduction of new products accounted for 2.8 percent of expenditure growth for nonfederal hospitals and 5.3
percent of growth for clinics during the same time frame.1 Both sets of statistics reveal the increasing influence the
expansion of non-acute care continues to have on health-system practice and expense. Table 2 shows the
therapeutic classes that account for the most spend among Vizient members.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 3
Table 2. Summary of highest-spend therapeutic classes among Vizient members
Therapeutic category Key products in class
Antineoplastic agents Rituxan, Keytruda, Avastin
Disease-modifying antirheumatic Remicade, Humira, Enbrel
agents
Immunomodulatory agents Tysabri, Copaxone, Ocrevus
Anti-infectives
Hepatitis C Harvoni, Epclusa, Zepatier
Antibacterials/antifungals Daptomycin, Invanz, AmBisome
(systemic)
Plasma critical care
Immune globulin, intravenous Gamunex, Privigen, Gammaguard
Albumin AlbuRx, Albutein, Flexbumin
Hematopoietic agents Neulasta, Aranesp, Procrit
Vaccines Prevnar, Gardasil, Pneumovax
Vizient member data for September 2017 to August 2018.
Table 3 shows the ten drugs with the highest total spend for Vizient members. Table 4 shows the drugs with the
largest projected increases in member spend due to price growth.
Table 3. Top 10 drugs by total spend among Vizient members
Rank Drug (brand name)
1 Adalimumab (Humira)
2 Infliximab (Remicade)a
3 Rituximab (Rituxan)a
4 Pegfilgrastim (Neulasta)a
5 Etanercept (Enbrel)
6 Alteplase (Activase)
7 Pembrolizumab (Keytruda)
8 Denosumab (Prolia, Xgeva)
9 Nivolumab (Opdivo)
10 Ustekinumab (Stelara)
Vizient member data for September 2017 to August 2018.
a
Biosimilar currently available or expected in 2019.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 4
Table 4. Top 10 drugs by size of projected price increase
Rank Drug (brand name)
1 Adalimumab (Humira)
2 Etanercept (Enbrel)
3 Denosumab (Prolia, Xgeva)
4 Ustekinumab (Stelara)
5 Alteplase (Activase, Cathflo Activase)
6 Vasopressin (Vasostrict)
7 Vedolizumab (Entyvio)
8 Pneumococcal 13-valent conjugate
vaccine (Prevnar 13)
9 Abatacept (Orencia)
10 Octreotide (Sandostatin LAR Depot)
Forecast highlights and overview
As can be seen by the analysis above, two things are consistent: (1) Oncology medications, disease-modifying
agents and immunomodulatory agents continue to account for the majority of spend, and (2) the projected rate of
price inflation continues to moderate. Although the FDA has approved many new specialty, orphan and other
high-cost drugs, these agents are used in very small populations. No other category has yet created a scenario
similar to the hepatitis C market, in which an expensive therapy is used across a rather broad patient population.
But even small price increases can have a substantial impact on drug spend, given the overall total of drug costs.
A number of events, both positive and negative, affected the pharmacy landscape in 2018. New product
approvals and increases in competition expanded treatment options and helped lower costs, while natural
disasters, exacerbation of drug shortages and reimbursement limitations added to already challenging
circumstances. Pharmacy’s critical role in coping with these changes to help manage the cost and quality of
health care make it a strong focus of improvement efforts.
A substantial number of high-spend agents are currently or will soon be subject to competition from biosimilars,
including pegfilgrastim, infliximab, rituximab and trastuzumab. The importance of continued adoption of
biosimilars to long-term efforts at mitigating price growth cannot be overstated. In addition, several of these
molecules are primarily used in the outpatient setting and therefore eligible for separate reimbursement, which
increases the importance of accurate billing and ongoing collaboration between the pharmacy and finance
departments.
Also, we would note that all significant expenditures are associated with outpatient and specialty pharmacy–
focused medications. Two agents, Vasostrict (vasopressin) and Cathflo Activase (alteplase),that are heavily used
in the inpatient setting will further challenge budgets due to expected price increases.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 5
Positive elements
As in the past, changes affecting pharmacy practice are a mix of positive and negative. Some recent favorable
events include:
• As of November 17, the FDA has approved 16 biosimilars in several therapeutic classes, the most recent of
which is a competitor for trastuzumab.2 Although only six of the 16 products have reached the market
because of lingering patent protections and exclusivities, the increased competition has already resulted in
lower relative prices. Payer coverage has also improved; more biosimilars are now included on formularies
at levels at least equivalent to the originator brands. The Centers for Medicare & Medicaid Services (CMS)
now assigns each biosimilar a unique reimbursement code and has granted pass-through status recognition
to all biosimilars, steps that should also encourage the use of these products.3 In the last year, the FDA
commissioner has made numerous statements about the need to remove regulatory and other barriers that
can limit the uptake of biosimilars and has signaled a new strategic plan to improve the efficiency of this
market. The FDA also held an open public hearing, in which Vizient participated, on additional steps the
agency can take to advance the uptake and marketing of biosimilars.4 These efforts are critically important
given the substantial growth of marketed biosimilars slated to take place in 2019.
• Although there are fewer generic versions of blockbuster drugs reaching the market than in past years, the
added competition for small-molecule drugs continues to help lower costs. For example, the pricing of
daptomycin has eroded by more than 60 percent since its loss of exclusivity. While biosimilars have not
caused price erosion of this magnitude, the imminent launch of competition has at least halted further price
increases.
• The CMS followed up its comprehensive initiative to lower the prices of medications5 with a proposal for
comment on a mechanism to reduce Medicare drug costs to levels that are closer to what other developed
nations pay.6 This new proposed concept also attempts to eliminate incentives to use more expensive drugs
to obtain higher levels of reimbursement.6 Although the details of these strategies have not yet been
clarified, the continued attention from the federal government increases the likelihood that changes will be
implemented.
• Last year also saw significant efforts to address drug shortages. In July, the FDA formed a drug shortages
task force to look at long-term strategies to address the supply challenges that have plagued pharmacy.7
The task force invited written comments to the FDA on ways to improve the current environment, conducted
listening sessions with various stakeholders (including Vizient) and hosted an open public hearing to obtain
additional feedback.7 Statistics shared by the FDA show that the agency has prevented more than 800
shortages of injectable drugs since 2011.8 Nevertheless, drug shortages remain an ongoing threat to our
capacity to deliver high-quality care.
Challenges
Ongoing and new challenges in the pharmacy landscape in the last year have included:
• The fragility of the pharmaceutical supply chain, which has been subject to interruption for almost two
decades and shows no signs of sustained improvement. For the first time since 2014, both new and existing
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 6
shortages increased in 2018. Critical categories like antimicrobials, chemotherapy products, electrolytes and
central nervous system drugs are still greatly affected by supply problems.9
• Issues in the pharmaceutical supply chain have been exacerbated by efforts to address the opioid epidemic
by reducing opportunities for diversion and misuse. One such effort was the quotas of active pharmaceutical
ingredients imposed on pharmaceutical suppliers by the Drug Enforcement Administration (DEA).10 The
quotas restricted manufacturers’ ability to compensate for unexpected supply interruptions, as those that had
spare production capacity did not have access to enough ingredients to enable them to pick up any slack. As
a result of advocacy efforts the DEA recognized the need to adjust these quotas,11 but the example
highlights the fragility of the market.
• Novel products continue to be introduced at higher and higher prices. Previous publications have noted the
approval of the first chimeric antigen receptor T-cell (CAR-T) agents, tisagenlecleucel (Kymriah; Novartis)
and axicabtagene ciloleucel (Yescarta; Kite Pharma/Gilead Sciences), both of which are notable for their
high cost (reduced to $373,000 from an initial price of $475,000).12 Those costs were then surpassed by the
introduction of voretigene neparvovec-rzyl (Luxturna; Spark Therapeutics), the first in vivo gene therapy
product to treat a rare form of vision loss, whose price for treatment of both eyes is $850,000.13
• Reimbursement-related issues continued in 2018, including the reduced payments for disproportionate share
hospitals imposed by CMS, which threaten many members’ ability to provide care for vulnerable
populations.14 Payers are also increasing their focus on cost differences for administering medications in
different locations (e.g., physician office vs. outpatient infusion clinic).15 And as described above, the
administration continues to propose ideas to lower the cost of health care to the government.6 Some of these
proposals could dramatically affect the way in which outpatient providers (health-systems and physicians)
purchase and charge for pharmaceuticals.6
Our advice
The Drug Price Forecast is intended to help Vizient members anticipate and adapt to the specific and overall
challenges that continue to confront health care. The forecast includes reviews of the acute and non-acute care,
specialty pharmaceutical and pediatric markets, reflecting the diversity of practice environments and patient
populations served by our members. In addition, we include pricing projections for the therapeutic categories that
tend to drive the majority of spend and are consistent across care settings: oncology medications, anti-infective
agents, therapies for multiple sclerosis (MS) and rheumatoid arthritis (RA), and plasma-derived pharmaceuticals.
Critical areas that merit close attention include:
• Strategic focus on pharmacy: Vizient has consistently held that pharmacy must be treated as an essential
element of any organization’s strategic plan given its impact on the cost and quality of patient care across
practice environments. Whether an organization is attempting to reduce inpatient length of stay, expand
medication management to include retail or specialty pharmacy, promote population health or decrease
opioid abuse, pharmacy is an integral component of those efforts. This concept was articulated convincingly
in the April 1, 2018, issue of the American Journal of Health-System Pharmacy, in which several articles
discussed the need for senior pharmacy leadership to support the concept of a “pharmacy enterprise” that
effectively and efficiently extends across all sites of care.16
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 7• Specialty pharmacy: Health systems must have a well-defined approach to the management of specialty
pharmaceuticals as these agents consume more spend and increasingly contribute to rising drug costs. The
specialty pharmacy section of the forecast provides an update on this market and describes ways to
integrate services to improve outcomes.
• Biosimilars: We have stated this concept before and we will continue to vocalize it. We must take full
advantage of the opportunity to lower costs presented by the expanding portfolio of biosimilars. A number of
competing versions of blockbuster biologics are likely to reach the market in 2019. Pharmacists must be
well-versed on these agents so that they can address clinical and economic questions of increasing
complexity, particularly as oncology biosimilars reach the supply chain.
• Advocacy: Successfully addressing the many issues confronting pharmacy requires advocacy. The 2018
Vizient Pharmacy Charter, developed with the members of the Vizient Pharmacy Executive Council, can
serve as a resource for targeting advocacy initiatives. Even with the changes in government resulting from
the 2018 midterm elections, drug costs and prices will remain a hot topic for bipartisan scrutiny and potential
additional intervention.
The pharmacy landscape continues to be extremely complex — regulatory issues, financial pressures, clinical
requirements and forecast expectations must all be anticipated and managed. However, organizations that can
successfully navigate these challenges will not just succeed, but thrive. Our goal, as always, is to help our
members thrive.
Forecast preparation, process and assumptions
Some things to keep in mind when reviewing the Drug Price Forecast:
• The forecast presents the Vizient pharmacy team’s best estimate of likely drug price behavior during the
identified period. However, it is important to recognize the uncertainty inherent in the projection process.
• This analysis was conducted using data from Vizient Pharmacy Program participants’ purchases (price and
volume) in hospital and non-acute facilities. The product mix covered by this forecast is based on
participants’ aggregated purchases and will differ from that of any individual facility.
• The products analyzed comprise the top 80 percent of pharmaceutical purchases (using dollars spent on a
line-item basis) made through pharmacy Authorized Distributors by Vizient Pharmacy Program participants
in hospital, non-acute and pediatric settings from Sept. 1, 2017, through Aug. 31, 2018. Purchases made
through the 340B program were excluded from the analysis.
• Purchasing sterile preparations from outsourced compounders is a sizeable expense for many health
systems. This forecast does not analyze these purchases as they are not reported by our Authorized
Distributors. If your facility uses outsourced compounding services, remember to factor those purchases into
your budget plans. Vizient has noted regular price increases from our contracted suppliers in this area and
we believe that this trend will continue.
• Vizient uses price change history for the last 36 months (where available), as well as experience and
knowledge of current contract allowances and marketplace factors such as expiring patents and anticipated
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 8new competition, to develop an inflation estimate for each line item in the projection. The analysis does not
take into account other market dynamics such as raw material scarcity and finished goods supply shortages.
• Information on possible patent expirations is provided solely as a courtesy and is based on sources available
at the time of publication; actual expiration dates can change because of patent challenges and litigation
processes. There is also no guarantee that an approved generic product will be ready to enter the market by
the expiration date. Manufacturers also may file a request for exclusive marketing rights with the FDA for
periods ranging from 180 days to seven years depending on the category. If granted, this period of
exclusivity may or may not be synchronized with the patent status and can further delay the introduction of
competition into the market.
Finally, this document is a projection of price behavior only. When preparing a drug expenditure budget, also
consider changes in volume and mix for your organization and the effects of introduction and adoption of new
drugs.
1. Schumock GT, Stubbings J, Wiest MD, et al. National trends in prescription drug expenditures and projections for 2018. Am J Health
Syst Pharm. 2018;75(14):1023-1038.
2. Biosimilar product information. FDA website.
https://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicap
plications/biosimilars/ucm580432.htm. Accessed November 18, 2018.
3. CMS revises Medicare Part B biosimilar coding and payment policies. Covington & Burling LLC website. https://www.cov.com/-
/media/files/corporate/publications/2017/11/cms_revises_medicare_part_b_biosimilar_coding_and_payment_policies.pdf. Published
November 8, 2017. Accessed November 6, 2018.
4. Sagonowsky E. Gottlieb calls out “rigged” system that’s hurting biosimilars, pledges FDA fight to boost uptake. FiercePharma. March 7,
2018. https://www.fiercepharma.com/pharma/fda-chief-gottlieb-calls-out-rigged-system-thats-hurting-biosim-use. Accessed May 22,
2018.
5. American Patients First: The Trump Administration Blueprint to Lower Drug Prices and Reduce Out-of-Pocket Costs. Washington, DC:
Department of Health and Human Services; May 2018. https://www.hhs.gov/sites/default/files/AmericanPatientsFirst.pdf. Accessed
November 6, 2018.
6. Gingery D. US throws drug pricing weight around, but still depends on pharma decisions. The Pink Sheet. October 28, 2018.
https://pink.pharmaintelligence.informa.com/PS124148/US-Throws-Drug-Pricing-Weight-Around-But-Still-Depends-On-Pharma-
Decisions. Accessed October 31, 2018.
7. Statement by FDA Commissioner Scott Gottlieb, MD, on formation of a new drug shortages task force and FDA’s efforts to advance long-
term solutions to prevent shortages [press release]. Silver Spring, MD: Food and Drug Administration; July 12, 2018.
https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm613346.htm. Accessed October 31, 2018.
8. Drug shortages infographic. Food and Drug Administration website.
https://www.fda.gov/Drugs/DrugSafety/DrugShortages/ucm441579.htm. Updated August 13, 2018. Accessed October 31, 2018.
9. University of Utah Drug Information Services. Drug shortages statistics. American Society of Health-System Pharmacists website.
https://www.ashp.org/Drug-Shortages/Shortage-Resources/Drug-Shortages-Statistics. Accessed October 31, 2018.
10. Balick R. DEA mandates reduction in opioid manufacturing for 2018. American Pharmacists Association website.
https://pharmacist.com/article/dea-mandates-reduction-opioid-manufacturing-2018. Published November 28, 2017. Accessed
November 6, 2018.
11. DEA working to avoid US drug shortages [press release]. Washington, DC: US Drug Enforcement Administration; April 10, 2018.
https://www.dea.gov/divisions/hq/2018/hq040918.shtml. Accessed November 6, 2018.
12. Bell J. Medicare to pay hundreds of thousands for CAR-T therapies. BioPharma Dive. April 6, 2018.
https://www.biopharmadive.com/news/medicare-to-pay-hundreds-of-thousands-for-car-t-therapies/520806. Accessed November 6, 2018.
13. Sagonowsky E. Spark sets off gene therapy debate with $850K sticker on Luxturna. FiercePharma. January 3, 2018.
https://www.fiercepharma.com/pharma/spark-prices-gene-therapy-luxturna-at-850k-grabbing-top-spot-pharma-s-costliest-drugs.
Accessed November 6, 2018.
14. Forys A. 340B changes: what biosimilar manufacturers need to know. Center for Biosimilars website.
http://www.centerforbiosimilars.com/contributor/amanda-forys/340b-changes-what-biosimilar-manufacturers-need-to-know. Published
February 19, 2018. Accessed November 6, 2018.
15. Magellan Rx Management. Medical Pharmacy Trend Report 2017. 8th ed. https://www1.magellanrx.com/magellan-
rx/publications/medical-pharmacy-trend-report.aspx. Accessed November 6, 2018.
16. Abramowitz PW, Chen DF, Cobaugh DJ. Multihospital health systems: growing complexity of pharmacy enterprise brings opportunities
and challenges. Am J Health Syst Pharm. 2018;75(7):417-418.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 9Projected timeline and approvals New drug approvals Drug Indication PDUFA date Ruxolitinib Graft-vs.-host disease Q1 2019 Biosimilar trastuzumab (PF-0528001) HER2-positive breast/gastric cancer Feb 2019 Iclaprim ABSSSI Feb 13, 2019 Ravulizumab Paroxysmal nocturnal hemoglobinuria Feb 18, 2019 Tagraxofusp AML Feb 21, 2019 N8-GP (turoctocog alfa pegol) Hemophilia A Feb 27, 2019 Siponimod (BAF312) SPMS Mar 2019 Ozanimod (RPC1063) RRMS Mar 2019 Herceptin SQ Breast cancer Mar 2019 Sotagliflozin Type 1 diabetes Mar 22, 2019 Meloxicam IV Moderate to severe pain, including postoperative pain Mar 24, 2019 Fosphenytoin, captisol enabled Seizures Mar 30, 2019 Iclaprim ABSSSI/HABP Q2 2019 RI-002 (IgIV) RSV in patients with primary immune deficiency disease Apr 2, 2019 Selinexor Multiple myeloma Apr 6, 2019 Risankinzumab Moderate to severe plaque psoriasis Apr 25, 2019 Esketamine Depression May 4, 2019 Sacituzumab govitecan Metastatic breast cancer May 21, 2019 Biosimilar bevacizumab (PF-06439535) Nonsquamous NSCLC Jun 2019 AXVS-101 SMA type 1 Jun 18, 2019 Erdafitinib Bladder cancer Q3 2019 Imipenem/relebactam MDR gram-negative organisms Q3 2019 Lefamulin CABP Q3 2019 Fosfomycin MDR gram-negative organisms Q3 2019 Biosimilar adalimumab (SB5) RA Jul 2019 Biosimilar rituximab (PF-05280586) Non-Hodgkin’s lymphoma Jul 2019 Crenolanib AML Aug 31, 2019 Cefidercol MDR gram-negative organisms Q4 2019 Biosimilar filgrastim (TX-01) Chemotherapy-induced neutropenia Oct 1, 2019 Abbreviations: ABSSSI = acute bacterial skin and skin structure infection; AML = acute myeloid leukemia; CABP = community-acquired bacterial pneumonia; HABP = hospital-associated bacterial pneumonia; IgIV = immune globulin, intravenous; IV = intravenous; MDR = multidrug-resistant; NSCLC = non–small-cell lung cancer; PDUFA = Prescription Drug User Fee Act; RA = rheumatoid arthritis; RRMS = relapsing-remitting multiple sclerosis; RSV = respiratory syncytial virus; SMA = spinal muscular atrophy; SPMS = secondary progressive multiple sclerosis. © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 10
Regulatory and accreditation events
Event Effective date
CMS MACRA Performance measures (MIPS) enforced Jan 1, Jan 2019
2017
CMS Conditions of Participation for Long-Term Deadline extended for facilities to have an Reimbursement penalties
Care: Antibiotic Stewardship Program antibiotic stewardship program in place (original will not go into effect until
implementation deadline Nov 28, 2017) May 2019
DSCSA Wholesalers must verify serialized product Nov 27, 2019
identifier for saleable returns
Enforcement of USP Chapter
Enforcement of USP Chapter
Dec 1, 2019
Enforcement of USP Chapter Final versions to be published Jun 1, 2019
Enforcement of USP Chapter
DSCSA Dispensers must receive only product with 2D Nov 27, 2020
data matrix bar code and product identifiers
Abbreviations: CMS = Centers for Medicare & Medicaid Services; DSCSA = Drug Supply Chain Security Act; MACRA = Medicare Access and
CHIP Reauthorization Act; MIPS = Merit-based Incentive Payments System; USP = US Pharmacopeia.
Anticipated availability of new generics and biosimilarsa
Generic name Brand name Earliest possible introduction
Minocycline Solodyn Feb 2019
Azithromycin (ophthalmic) AzaSite Mar 31, 2019
Atazanavir Reyataz (oral powder) Jun 2019
Thalidomide Thalomid Aug 1, 2019
Fosaprepitant dimeglumine Emend (injection) Sep 5, 2019
Hydrocodone bitartrate Zohydro ER Nov 1, 2019
Carfilzomib Kyprolis Jan 20, 2020
Posaconazole Noxafil suspension Jan 20, 2020
Alvimopan Entereg Jan 27, 2020
Enzalutamide Xtandi Feb 29, 2020
Lanreotide acetate Somatuline Depot Mar 8, 2020
Lenalidomide (5, 10, 15, 25 mg) Revlimid Apr 5, 2020
Melphalan HCl Evomela May 9, 2020
Apixaban Eliquis 2.5 mg Jun 28, 2020
Oxycodone HCl Xtampza ER Jul 10, 2020
Lenalidomide (2.5, 20 mg) Revlimid Aug 26, 2020
Dimethyl fumarate Tecfidera Sep 27, 2020
Vasopressin Vasostrict Oct 17, 2020
Acetaminophen (intravenous) Ofirmev Dec 6, 2020
Tiotropium bromide Spiriva Dec 26, 2020
a
Projected dates of loss of exclusivity for originator drugs and generic or biosimilar entrants to the market are subject to change.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 11A closer look by segment Acute care Prescription drugs are one of the fastest-growing elements of health care spending, accounting for approximately 17 percent of the $3.3 trillion in total annual spend in the U.S.1,2 Table 5. Acute care drugs with the highest share of spend among Vizient members Drug Rituximab Pegfilgrastim Alteplase Infliximab Pembrolizumab Nivolumab Trastuzumab Bevacizumab Immune globulin, gamma (IgG)/Proline/IgA Ocrelizumab Vizient member data on inpatient spend from September 2017 to August 2018. The recent approval of Truxima (Celltrion/Teva Pharmaceuticals), the first biosimilar for rituximab, the acute care drug that accounts for the highest share of Vizient member drug spend, is expected to have a significant impact on the U.S. market. Overall, however, the approval of biosimilars has so far not had the expected impacts on market share and costs, due to prior authorization requirements of various payer protocols and formularies. As noted in the July 2018 edition of the Drug Price Forecast, the increase in drug spend is due to higher drug costs rather than increased utilization. And many additional high-cost cell and gene biotherapies have been approved since voretigene neparvovec (Luxturna), tisagenlecleucel (Kymriah) and axicabtagene ciloleucel (Yescarta), with their accompanying sticker shock, came on the market. Medication cost management is therefore a critical concern for pharmacy leaders and at the top of their list of challenges.3 The health system’s sustainability is being threatened by the flood of high-cost drugs for rare and ultra-rare disorders that are priced at levels far above traditional cost-effectiveness thresholds.4 FDA Commissioner Scott Gottlieb expressed concern about reimbursement for rare disease treatments and the need for reform at the Milken Institute’s annual Future of Health Summit in Washington in October 2018.5 His statement comes on the heels of the federal approval of right-to-try legislation and the uncertainty about its financial effect on the health system. Another factor in rising drug spending is persistent shortages of important drugs, including small-volume parenteral fluids, emergency medications and injectable opioids including morphine, hydromorphone and fentanyl. © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 12
(Pfizer, which controls about 60 percent of the U.S. market for injectable opioids, expects to return to full supply
capacity in the second quarter of 2019.)
The current administration has made reducing prescription drug prices a top priority. One result of this focus was
the release of American Patients First: The Trump Administration Blueprint to Lower Drug Prices and Reduce
Out-of-Pocket Costs in May 2018. Since then, the FDA has created a working group to consider prescription drug
importation and a record number of generic drugs have been approved, including many biosimilars.
1. National health expenditure data. Centers for Medicare & Medicaid Services website. http://www.cms.gov/research-statistics-data-and-
systems/statistics-trends-and-reports/nationalhealthexpenddata/nationalhealthaccountshistorical.html. Updated January 8, 2018.
Accessed November 1, 2018.
2. A look at drug spending in the U.S. The Pew Charitable Trusts website. http://www.pewtrusts.org/en/research-and-analysis/fact-
sheets/2018/02/a-look-at-drug-spending-in-the-us. Published February 27, 2018. Updated August 28, 2018. Accessed November 1,
2018.
3. Brown T. What keeps hospital CEOs up at night? Infor website. http://blogs.infor.com/healthcare/2018/04/what-keeps-hospital-ceos-up-
at-night.html. Published April 26, 2018. Accessed November 1, 2018.
4. Lasser KE, Mickle K, Emond S, et al. Inotersen and Patisiran for Hereditary Transthyretin Amyloidosis: Effectiveness and Value — Final
Evidence Report. Institute for Clinical and Economic Review website. https://icer-review.org/wp-
content/uploads/2018/02/ICER_Amyloidosis_Final_Evidence_Report_101718.pdf. Published October 4, 2018. Accessed November 6, 2018.
5. Statement by FDA Commissioner Scott Gottlieb, MD, on FDA’s new steps to modernize drug development, improve efficiency and
promote innovation of targeted therapies [press release]. Silver Spring, MD: Food and Drug Administration; October 15, 2018.
https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm623411.htm. Accessed November 21, 2018.
Non-acute care
The ability to deliver high-quality, cost-effective care outside of an inpatient hospital setting continues to grow in
importance. Providers and payers are focusing their energies on finding the least expensive site of care for
increasingly complicated services, including the administration of many medications.1 Given the growth of health
care expenditures, this trend is unlikely to change. As a result, it is critical to understand the factors affecting the
non-acute environment. Some of the challenges facing non-acute providers are specific to those settings — for
example, changes in reimbursement for home infusion and long-term care — but in many cases, the concerns of
non-acute facilities are the same as those of hospitals and health systems.
Two challenges that both acute and non-acute providers alike must deal with are drug shortages and compliance
with regulations governing the safety and sterility of medications, especially injectable products.
Drug shortages update
After remaining at fairly consistent levels for the last few years, the number of drug shortages, both new and
continuing, has actually started to climb.2 Recent data from the University of Utah Hospitals and Clinics shows
that as percentages, more injectable than noninjectable drugs are in short supply. Therapeutic categories
commonly used in various outpatient infusion settings, such as antimicrobials, electrolytes, nutrition-related
agents and intravenous fluids, also continue to be affected by supply issues.2 Vizient works aggressively to
provide members with the most current information on drug shortages as well as expanded clinical materials for
therapeutic alternatives to products affected by supply problems. In addition, the Vizient team has worked with the
FDA and other industry stakeholders to find solutions to these challenges.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 13Mastering the requirements for sterile compounding Another area requiring time, attention and resources from pharmacy providers in multiple sites of care is meeting the requirements for safe compounding of sterile and hazardous pharmaceuticals.3 Standards established in the United States Pharmacopeia (USP) general chapters and require a thorough understanding of current practices and the capacity to plan the necessary investments in technology and possibly construction.3 Vizient has been working for several years to increase clinicians’ understanding of these requirements and help them adapt to the changing standards and follow adjustments in the dates of enforcement. Now that the enforcement dates are set for Dec. 1, 2019, definitive action is required. Changing reimbursement across practice settings: focus on non-acute practices Given the increasing expense of pharmaceuticals and the greater costs imposed by stricter regulatory requirements, ensuring effective reimbursement is essential to maintaining the capacity to provide effective patient care. Within the non-acute landscape, two recent reimbursement changes could greatly affect the economic viability of home infusion programs and long-term care institutions.4,5 As with drug shortages, awareness and advocacy are critical to advancing the perspective of the member community and preventing regulatory action that could compromise patient care capabilities. Home infusion: what looked promising is now a concern One area where regulatory actions are prompting substantial worry is home infusion. One strategy for addressing rising drug costs that has been proposed by many stakeholders is to migrate as much care as possible, particularly for infused pharmaceuticals, to outpatient settings including patients’ homes. While not appropriate for all patients, home infusion services can allow providers to maintain a high quality of care in a less expensive setting than a hospital or clinic. Some patients, with proper training, may even be able to self-infuse certain complex medications.6 Two recent pieces of legislation, the 21st Century Cures Act and the Bipartisan Budget Act of 2018, appeared to promote the financial viability of home infusion care by recognizing professional services as explicitly reimbursable activities within Medicare.4 The 21st Century Cures Act instituted a professional services reimbursement structure that would begin in 2021.4 In the interim, the Bipartisan Budget Act of 2018 provided for temporary transition payments with specific rates for defined drugs, to be implemented prior to the 2021 date. However, in the Home Health Prospective Payment System for calendar year 2019, CMS has proposed limiting reimbursement for professional services to days when a nurse is physically present with a patient.4 As many home infusion providers and their professional trade group, the National Home Infusion Association, have pointed out, this requirement fails to take into consideration the numerous additional services provided by other professionals, including pharmacists, for critically important activities such as compounding, preparation and virtual monitoring of patient outcomes.4 The CMS approach is being challenged by numerous stakeholders and even by bipartisan sponsors of the already-passed legislation.7 Vizient will continue to monitor the ongoing debate and any potential future changes to this rule. Long-term care: pulling the ‘RUG’ out from under skilled nursing facility reimbursement Another change that appears less subject to debate, but nevertheless will be a huge transition, relates to the payments for long-term care and skilled nursing facility services.5 Beginning Oct. 1, 2019, CMS is adopting a per- © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 14
diem payment system called the Patient-Driven Payment Model (PDPM).5 The PDPM approach replaces the
Resource Utilization Group (RUG) methodology, which has been used since the Balanced Budget Act of 1997.8
However, one criticism of RUGs has been that utilization is driven by the number of therapy minutes provided,
which could encourage the delivery of additional intervention without clinical need.8 Under the new system,
therapy minutes will continue to be recorded but will no longer drive payment. Instead, patients will be assigned to
a case-mix group based on the clinical information in their admission minimal data sets (MDS).8
Most critically for pharmacists, in the PDPM system pharmacy services are considered a separate Non-Therapy
Ancillary Service (NTAS).5,8 The NTAS has a variable per-diem adjustment factor for the first three days of care
because of the increased use of services such as intravenous medication administration during this period.5,8
Therefore, pharmacists must ensure that all relevant data, including comorbidities, are adequately captured on
the patient’s MDS to receive appropriate reimbursement, particularly for the first three days of patient care.
Summary
As in other areas of practice, the non-acute care market continues to face many challenges. Drug shortages
continue to make the task of patient care more complex, and the increasing cost of specialty drugs, as
demonstrated by the most commonly used products in the non-acute setting (Table 6), will keep pharmaceutical
expenditures trending higher.
Table 6. Top 10 drugs based on non-acute spend among Vizient members
Rank Drug (brand name)
1 Adalimumab (Humira)
2 Etanercept (Enbrel)
3 Ustekinumab (Stelara)
4 Dimethyl fumarate (Tecfidera)
5 Glatiramer acetate (Copaxone)
6 Fingolimod HCl (Gilenya)
7 Ledipasvir/sofosbuvir (Harvoni)
8 Secukinumab (Cosentyx)
9 Apremilast (Otezla)
10 Abiraterone acetate (Zytiga)
Vizient member data for September 2017 through August 2018.
The movement of patient care away from the traditional inpatient setting will continue as stakeholders look for
ways to offset rising costs. As a result, pharmacy providers must be knowledgeable about the differences in and
potential changes to reimbursement patterns in order to succeed in this market and provide consistent care to
their patients. Familiarity with and knowledge of the home infusion space is particularly critical, as is expertise in
the specialty pharmacy arena, which will be discussed in the next section.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 15Vizientinc.com resource
Drug compounding and handling resources page
1. Magellan Rx Management. 2018 Employer Market Insights Report. 1st ed.
https://www1.magellanrx.com/media/746514/2018_mrx_employer-market-insights-report.pdf. Accessed October 29, 2018.
2. University of Utah Drug Information Services. Drug shortages statistics. American Society of Health-System Pharmacists website.
https://www.ashp.org/Drug-Shortages/Shortage-Resources/Drug-Shortages-Statistics. Accessed October 29, 2018.
3. Thompson G. Complying with pharmacy standards: USP 797/USP 800. The Oncology Pharmacist website.
http://theoncologypharmacist.com/top-resources/online-only/17542-complying-with-pharmacy-standards. Updated August 8, 2018.
Accessed October 29, 2018.
4. NHIA executive summary of CMS proposed rule implementing home infusion services temporary transitional payment and permanent
payment, National Home Infusion Association website. http://nhia.org/new_site/docs/NHIA_Executive_Summary_of_CMS.pdf. Published
July 9, 2018. Accessed October 29, 2018.
5. Baldwin P, Smith E. New focus for Medicare SNF reimbursement: CMS PDPM final rule for FY 2019 and FY 2020. Long Term Care
Pharmacy News. http://ltcpharmacynews.com/docs/PDF%20Docs/August%202018%20Elise%20Smith.pdf. Accessed October 29, 2018.
6. Infusion FAQs. National Home Infusion Association website. https://www.nhia.org/faqs.cfm. Accessed October 29, 2018.
7. Congressman Sessions letter to CMS relays concern over proposed rule on Medicare Part B home infusion reimbursement. National
Home Infusion Association website. http://www.nhia.org/documents/Sessions_Home_Infusion_Rule_Letter_SIGNED.pdf. Published
August 7, 2018. Accessed October 29, 2018.
8. Patient-Driven Payment Model (PDPM) resource center. American Health Care Association website.
https://www.ahcancal.org/facility_operations/medicare/Pages/PDPM-Resource-Center.aspx. Accessed October 29, 2018.
Specialty pharmaceuticals
The number and cost of specialty pharmaceuticals continues to draw the attention of the health care community
as providers, payers and patients work to manage the increasing expense of these medications. Since the
publication of the July 2018 Drug Price Forecast, the FDA has approved 21 additional new molecular entities.1 Of
those, 12 (57 percent) are considered specialty pharmaceuticals based on factors like indication and intended
population, administration and monitoring considerations, cost, or limited distribution processes.1,2
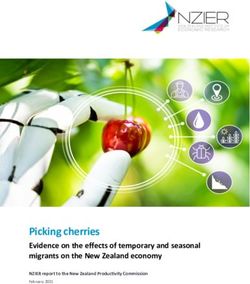
Over the five years from 2013 through 2017, total U.S. expenditures for specialty drugs nearly doubled, from
$83 billion to $157 billion.2 If orphan drugs (i.e., “ultra-specialty” medications) are included, the total spend on
specialty drugs reached $200 billion in 2017.2 Combined, the costs of specialty pharmaceuticals and orphan
drugs nearly equal the total amount spent on traditional medications in the U.S. (Figure 1).
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 16Figure 1. Annual spend by drug type as a percentage of total U.S. drug spend Data derived from IQVIA Institute.2 The increasing financial challenge presented by specialty pharmaceuticals has a substantial impact on health care providers and an even greater impact on patients, for whom the burden imposed by high-cost drugs is significant. A recent analysis of dispensed prescriptions and out-of-pocket expense for U.S. patients in 2017 reveals the size of the problem.2 Of the 5.4 billion prescriptions filled that year, 31 percent resulted in no out-of- pocket expenditures for patients, and another 48.9 percent cost between $0.01 and $9.99.2 Only 0.2 percent of prescriptions cost patients $250 or more, but although the percentage of prescriptions in this category seems small, it actually translates to 14.1 million prescriptions with a price tag of $250 or more. Another 3.4 million prescriptions cost $500 or more. The size of the burden for patients will likely continue to increase as insurers and payers implement additional strategies to limit their exposure to increasingly expensive medications.2,3 For example, payers have now added coinsurance payments and pharmacy deductibles on top of the specialty pharmacy tiers, limited distribution strategies and prior authorization requirements that were already in place.2 Another strategy is copay accumulators — programs that apply only a patient’s own out-of-pocket payments towards the deductible, excluding the value of manufacturers’ coupons.2,3 As a result, providers — particularly the academic medical centers, integrated health systems, community-based hospitals and pediatric facilities that comprise the Vizient membership — must consider the impact of specialty pharmaceutical costs not only on their organizations, but also on their patient populations. Biosimilars in specialty pharmacy: waiting for 2023 As discussed in other sections of this forecast, 2019 will be a seminal year for biosimilars, as competing versions of monoclonal antibodies commonly used in oncology, such as rituximab, bevacizumab and trastuzumab, are expected to enter the market.4 In addition, a second biosimilar for pegfilgrastim will likely enter the market by © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 17
January 2019. These four molecules alone account for approximately $14 billion in spend over 12 months.5
Specialty pharmacy providers should work to encourage acceptance of biosimilars as comparable therapeutic
alternatives.
However, it increasingly appears that we will have to wait until 2023 for the biggest biosimilar opportunity within
the specialty pharmacy space. The total expenditure for adalimumab (Humira; AbbVie) eclipses the total for all
four of the biologics listed above, with an annual spend of $17 billion.5 Providers, payers and patients have been
eagerly waiting for competition for this high-cost molecule. But as a result of several recent settlements,
biosimilars for adalimumab are still about four years away.6 As of November 2018, AbbVie has reached patent
settlements with Amgen, Merck, Mylan, Sandoz and Momenta to delay launches of biosimilars, as noted in
Table 7. One supplier that has a biosimilar already approved and does not have a settlement agreement with
AbbVie, Boehringer Ingelheim, continues to engage in litigation.6
Table 7. Anticipated dates of introduction for adalimumab biosimilars
Settlement-allowed
Supplier Drug (brand name) Approval date launch date
Amgen Adalimumab-atto (Amjevita) Sep 23, 2016 Jan 31, 2023
Merck/Samsung SB5 Jul 2019 (estimated) Jun 30, 2023
Mylan MYL-1401A Not filed Jul 31, 2023
Sandoz Adalimumab-adaz (Hyrmioz) Oct 30, 2018 Sep 30, 2023
Momenta M923 Not filed Nov. 20, 2023
Boehringer Ingelheim Adalimumab-adbm (Cyltezo) Aug 5, 2017 Ongoing litigation
6-8
Data derived from Sandberg, IPD Analytics, and Drugs@FDA website.
The timing of pharmaceutical launches can change dramatically as a result of unanticipated legal rulings, so it is
possible that adalimumab biosimilars could become available earlier, but in light of the legal settlements that have
been made thus far, direct competition is not expected for several years.
Since biosimilar competition for the most commonly purchased drug, both in the specialty pharmacy category and
overall, is still four years away, it is critical that health systems continue to expand their specialty pharmaceutical
management strategies.
Summary
Given the existing population of specialty pharmaceuticals, the continued increase in the cost of these
medications and the dynamics of the investigational drug pipeline, a defined specialty pharmacy strategy is a
necessity, not an option, for health systems. A health system that does not address the challenges posed by
specialty pharmacy may risk loss of reimbursement in an accountable care environment, loss of patients and
revenue to competitors with established ambulatory and specialty pharmacies, and lower provider and patient
satisfaction across multiple service lines. Increasing availability of biosimilars over the next several years should
eventually result in meaningful competition, and providers should continue to promote these alternative products
where possible. In addition, providers must consider the financial impact of expensive specialty pharmaceuticals
not only on their organizations, but also on the patients they serve.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 181. Novel drug approvals for 2018. Food and Drug Administration website.
https://www.fda.gov/drugs/developmentapprovalprocess/druginnovation/ucm592464.htm. Accessed October 27, 2018.
2. IQVIA Institute. Orphan Drugs in the United States: Growth Trends in Rare Disease Treatments.
https://www.iqvia.com/institute/reports/orphan-drugs-in-the-united-states-growth-trends-in-rare-disease-treatments. Published October
2018. Accessed October 27, 2018.
3. Silverman E. Backlash against copay accumulators. Manag Care. 2018;27(9):15.
https://www.managedcaremag.com/archives/2018/9/backlash-against-copay-accumulators. Accessed October 27, 2018.
4. Pending biosimilars. The Pink Sheet. https://pink.pharmaintelligence.informa.com/PS120038/Pending-Biosimilars. Published February
13, 2017. Accessed October 27, 2018.
5. Schumock GT, Stubbings J, Wiest MD, et al. National trends in prescription drug expenditures and projections for 2018. Am J Health
Syst Pharm. 2018;75(14):1023-1038.
6. Sandburg B. AbbVie inks sixth Humira biosimilar settlement, battles Boehringer’s ‘Unclean Hands’ Claim. The Pink Sheet.
https://pink.pharmaintelligence.informa.com/PS124226/AbbVie-Inks-Sixth-Humira-Biosimilar-Settlement-Battles-Boehringers-Unclean-
Hands-Claim. Published November 8, 2018. Accessed November 18, 2018.
7. IPD Analytics Biologics/Biosimilars database [database online]. Bay Harbor Island, FL: IPD Analytics; 2018. http://www.ipdanalytics.com.
Accessed October 27, 2018.
8. FDA approved drug products. Drugs@FDA website. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm. Accessed November 1,
2018.
Pediatrics
Pediatric inflation rate: 4.14%
Recent approvals
In 2018, approvals of drugs for the pediatric population are focused in three categories: specialty drugs, gene
therapy and chimeric antigen receptor T-cell treatments. All three of these treatments raise budgetary and
revenue capture obstacles. To alleviate the burden they impose, additional evaluations must be made before
including these medications for rare diseases in hospital formularies.
The approval of elapegademase-lvlr (Revcovi; Leadiant Biosciences) in October added another enzyme
replacement therapy option for both pediatric and adult patients with adenosine deaminase severe combined
immune deficiency (ADA-SCID). The disorder mainly affects infants and young children. ADA-SCID is an inherited
genetic disorder in which deficiency of the ADA enzyme renders the immune system nonfunctional, resulting in
SCID.1 Elapegademase-lvlr is a recombinant product providing an alternative to pegadmease bovine (Adagen;
Leadiant Biosciences).
In August 2018 three drugs received approval or expansion of indications to include patients under 18 years of
age. Lanadelumab (Takhzyro; Shire) is the first monoclonal antibody approved for hereditary angioedema (HAE),
a rare genetic disorder in which patients have poorly functioning C1-INH protein, resulting in random episodes of
angioedema.2
Patients with Dravet syndrome, which requires combination therapy because of the potential for drug-resistant
increase in seizures, had two big wins in 2018. The approval of stiripentol (Diacomit; Biocodex) as adjunctive
therapy to clobazam (Onfi; Lundbeck) in patients 2 years of age and older3 adds a new therapeutic option. It will
also add an average of $14,000, depending on dosage, to the current annual average of $100,000 in health care
costs associated with Dravet syndrome, including multidrug therapy, hospitalizations and in-home medical care
visits.4
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 19In June the long-awaited epilepsy medication cannabidiol (Epidiolex; GW Pharmaceuticals) was approved on the
basis of improvements in quality of life and reductions in seizure frequency in patients with refractory epilepsy,
including those with Lennox-Gastaut and Dravet syndromes.5 Cannabis-based therapy is derived from cannabidiol
(CBD), the nonpsychoactive components of the marijuana plant. Release and availability of the product was
delayed awaiting the DEA schedule classification. In late September, cannabidiol medications were given a
Schedule 5 designation, allowing GW to manufacture its product. It is expected to cost about $32,500 per year.6
In patients with intestinal-failure–associated liver disease (IFALD) and parenteral nutrition–associated cholestasis
(PNAC), maintaining nutritional status with minimal risk to the liver requires reduction in intravenous lipid
emulsion. For several years, such patients in the U.S. used alternative fatty acid sources under compassionate-
use protocols. In August, an omega-3 fatty acid fish oil triglycerides emulsion, (Omegaven, Fresenius Kabi), was
approved as a source of fatty acids in patients with PNAC.7
Cost increases driven by specialty drugs, outpatient care
As in other areas, pediatric pharmaceutical costs are rising as a result of the targeting of rare diseases that
require specialty or orphan drugs.
Table 8 lists the top 10 drugs based on total expenditures among self-governed children’s hospitals as well as the
drug’s ranking from the July 2018 Drug Price Forecast and based on overall spend among Vizient members for
Sept. 1, 2017, through Aug. 31, 2018. Dinutuximab (Unituxin; AbbVie), indicated for high-risk neuroblastoma,
retained its previous position as the highest-spend drug for the current period. Pegaspargase (Oncaspar; Shire), a
modified enzyme used in the treatment of acute lymphoblastic leukemia, and infliximab (Remicade; Janssen
Biotech, Inc.), a monoclonal antibody used in the treatment of autoimmune diseases, have remained in the top 3
for year-over-year spend. One newcomer to the top 10 in the July 2018 forecast, eculizumab (Soliris; Alexion), a
monoclonal antibody directed against C5 complement protein, increased to fifth in spend for this group.8
Table 8. Top 10 pediatric drugs based on spenda among self-governed children’s hospitals that
participate in the Vizient group purchasing organization
Generic drug name (brand name; manufacturer)
Dinutuximab (Unituxin; United Therapeutics)
Pegaspargase (Oncaspar; Baxalta)
Infliximab (Remicade; Janssen Biotech)
Palivizumab (Synagis; Astra Zeneca)
Eculizumab (Solaris; Alexion)
Sildenafil (Revatio; Pfizer)
Asparaginase (Erwinaze; Jazz Pharmaceuticals)
Dornase alfa (Pulmozyme, Genentech)
Pneumococcal 13-valent conjugate vaccine (Prevnar-
13, Pfizer)
Pegfilgrastim (Neulasta, Amgen)
a
340B purchases were excluded from the analysis.
© 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 20The high cost of CAR-T and gene therapy agents such as tisagenlecleucel (Kymriah) and voretigene neparvovec (Luxturna) remains a consideration for pediatric care centers.9 The cost of a single infusion of tisagenlecleucel was reduced in 2018 from $475,000 to $373,000.10 Discussions between Novartis and CMS about indication- based pricing were abandoned in July 2018, leaving reimbursement under the unclassified drug/biologic J- codes.11 Voretigene neparvovec, a gene replacement therapy for RPE65-medicated inherited retinal dystrophy, which can cause complete blindness,12,13 continues to be priced at a total of $850,000 for treatment of both eyes. The costs of these and other novel agents continue to weigh on pediatric pharmacy budgets. These drugs may also have significant restrictions on handling, storage and administration. For example, tisagenlecleucel can only be administered at preapproved centers and patients must be able to reach the center within two hours for at least four weeks after administration in case of emergency. Institutions must therefore review their procurement and administration policies for these therapies. In the pipeline The investigational pipeline in pediatrics continues to focus on treatment of targeted diseases using monoclonal antibodies, gene therapy and orphan drugs. One gene therapy to treat type 1 spinal muscular atrophy, AVXS-101 (AveXis), is intended to be an intravenous alternative to intrathecal nusinersen (Spinraza; Biogen). An open-label, single-arm, single-dose, multicenter trial, known as STR1VE, is being conducted to evaluate the efficacy and safety of a one-time intravenous infusion of AVXS-101.14 Another trial of a gene therapy for the treatment of Duchenne muscular dystrophy, a genetic degenerative disease that leads to progressive weakness of muscles, has begun to enroll human subjects. The goal of this therapy to is replace the affected mRNA with mutations between exons 18 and 58.15 Table 9 lists additional products currently in development that, in some cases, are expected to have substantial costs associated with their use. © 2019 Vizient, Inc. All rights reserved. January 2019 Drug Price Forecast 21
You can also read