Efforts to Reduce Primary Cesarean Delivery - AIM BUNDLES AIM BUNDLES TOOLKITS Latent Labor Checklist - Obstetrics Initiative
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Efforts to Reduce Primary Cesarean Delivery
AIM BUNDLES
AIM BUNDLES
TOOLKITS
ARREST
DISORDER
TOOLS
Latent Labor Checklist Promoting Spontaneous Progress in Labor
Option A Option B
2019 Program Options to Optimize First Stage of Labor Option A: OBI Checklist Emphasis on Timing of Admission, Shared Decision making, Coping, and a Support person. Option B: Promoting Spontaneous Progress in Labor Bundle*: Implement approaches that support spontaneous progress of labor during the first stage of labor. *Adapted from the American College of Nurse-Midwives Healthy Birth Initiatives Reducing Primary Cesareans Bundle: Promoting Spontaneous Progress in Labor

The OBI Checklist
Option A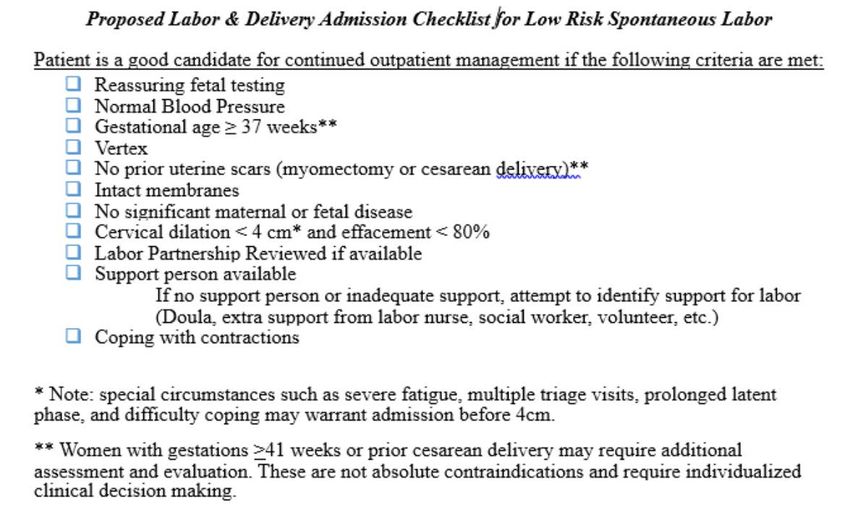
Why use a checklist?

When to use a checklist?
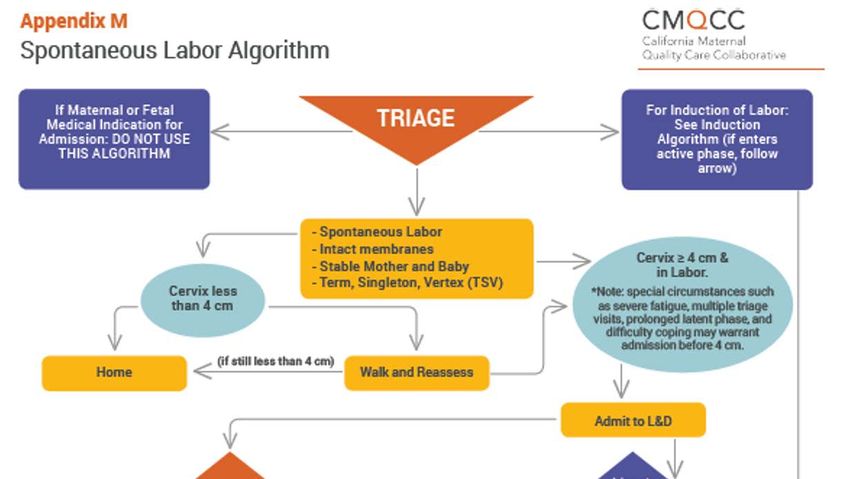
What checklist?

Why wait until active labor?
Admitted BEFORE Admitted IN
MODE OF Active Labor onset Active Labor
(n = 18,405)* No. (%) (n= 8,672) No. (%)
BIRTH P
< .001
Vaginal – Spontaneous 12,889 (70.0) 7,184 (82.2)
Vaginal – Assisted 2,205 (12.0) 862 (9.9)
Cesarean 3,311 (18.0) 626 (7.2)
*Nulliparous, term, singleton, vertex patients, with spontaneous labor and documentation of first exam
Neal JL, et al. Birth. 2018.
What might we save?
• Objective:
• Assess outcomes and
cost of hospital
admission during the
latent versus active
phase of labor
• Theoretical cohort:
• 3.2 million women
(number term
deliveries in US
without prior CD)
• Cost estimates from
the literature
Tilden EL, et al. Birth. 2015
What might we save?
672,000 fewer epidurals
Estimated cost savings of $694 million annually in the United States
67,232 fewer cesarean deliveries
9.6 fewer maternal deaths
Tilden EL, et al. Birth. 2015Labor Partnership Document
“Birth Plan” often inspires dread from labor
and delivery staff
A “Labor Partnership” is designed to help initiate
conversations prenatally to developed a shared
understanding of knowledge and desires for labor
care and to support informed choices about
options.Why Bother with a Labor Partnership?
There are no RCTs that prove labor
partnerships/birth plans will reduce the
cesarean delivery rate.Reasons for the Labor Partnership
• Feedback from our OBI meeting in April 2018
• Supported by CMQCC
• Gives all women an opportunity to learn about labor and
express their values1
• Allows values expressed in prenatal care to be efficiently
shared with all Labor and Delivery staff
• Shared decision making is the standard of care2
1Attanasi LB, et al. Pateint Educ Couns. 2018
2 ACOG Committee Opinion 587, 2014 Reaffirmed 2018How do I make a Labor Partnership Document? Obstetrics Initiative OBI Hospital Resources Page: www.obstetricsinitiative.org/obi-hospitals-resources-tools/ 1. OBI Labor Partnership 2. Birth Partnership Document by Megan Danielson, CNM, DNP 3. California Maternal Quality Care Collaborative (CMQCC) Birth Plan
Support Person Available “The nurses at our hospital provide excellent labor support, why do I need to ask about this?”
Continuous Labor Support
Can be provided trained by family member, hospital staff, or Doula
Cochrane Review, 2017: 26 trials 15,858 women
DIRECTION NUMBER OF NUMBER OF
OUTCOME OF RR TRIALS IN WOMEN IN
CHANGE ANALYSIS ANALYSIS
•
Cesarean Birth
0.75
(95% CI 0.64 to 0.88)
24 trials 15,347
0.62 14 trials 12,615
Low five minute (95% CI 0.46 to 0.85)
Apgar
1.08 21 trials 14,369
Vaginal Birth (95% CI 1.04 to 1.12)
Bohren MA, et al. Cochrane Database of Systematic Reviews 2017Why use a Coping Scale?
Traditional pain scores do not consider patient
anxiety, fear, or suffering.
ACOG Committee Opinion 687, Reconfirmed 2018Reviews of the Coping Scale
• Developed by a team of nurses and midwives
• Nurses studied at the University of Utah
- Beneficial to patients
- Improved nurses’ assessment of the patient
• Approved by The Joint Commission as an appropriate pain
assessment tool
Roberts, J Midwifery Women’s Health, 2010How do I share?
References for OBI Checklist
1. Smith H, Peterson N, Lagrew D, Main E. 2016. Toolkit to Support Vaginal Birth and Reduce Primary Cesareans:
A Quality Improvement Toolkit. Stanford, CA: California Maternal Quality Care Collaborative
2. Neal JL, Lowe NK, Caughey AB, et al. Applying a physiologic partograph to Consortium on Safe Labor data to
identify opportunities for safely decreasing cesarean births among nulliparous women. Birth. 2018
3. Tilden EL, Lee VR, Allen AJ, Griffin EE, Caughey AB. Cost-Effectiveness Analysis of Latent versus Active
Labor Hospital Admission for Medically Low-Risk, Term Women. Birth. 2015;42(3):219-26.
4. Effective patient-physician communication. Committee Opinion No. 587. American College of Obstetricians
and Gynecologists. Obstet Gynecol 2014;123:389-93.
5. Bohren MA, Hofmeyr G, Sakala C, Fukuzawa RK, Cuthbert A. Continuous support for women during
childbirth. Cochrane Database of Systematic Reviews 2017, Issue 7.
6. Approaches to limit intervention during labor and birth. Committee Opinion No. 687. American College of
Obstetricians and Gynecologists. Obstet Gynecol 2017;129:e20–8.
7. Roberts J, Hanson L. Best practices in second stage labor care: maternal bearing down and positioning. J
Midwifery Womens Health. 2007;52(3):238-45.
8. Attanasio LB, Kazhimannil KB, Kjerulff KH. Factors influencing women’s perception of shared decision
making during labor and delivery: Results from a large-scale cohort of first childbirth. Patient Educ Couns.
2018;101(6):1130-1136.
9. Roberts L, Gulliver B, Fisher J, Cloyes KG. The coping with labor algorithm: an alternate pain assessment tool
for the laboring woman. J Midwifery Womens Health. 1010;55(2)107-16.You can also read

















































