Myths and Beliefs In the Use of Folic Acid - Klaus Kraemer and Monika Potter Hidden Hunger - From Assessment to Solutions
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Myths and Beliefs
In the Use of
Folic Acid
Klaus Kraemer and Monika Potter
Sight and Life, Switzerland
Hidden Hunger - From
Assessment to Solutions
Overview of myths and beliefs Folic acid (FA) supplementation recommendations effectively reduce the risk of neural tube defects (NTDs) FA fortification… …masks vitamin B12 deficiency …leads to intakes above the tolerable upper intake level (UL) …increases the risk of cancer …changes the properties of drugs

FA supplementation recommendations
effectively reduce the risk of NTDs
Rates of NTDs per 10,000 births (1988 to 1998):
Conclusion:
NTDs/10 000 births
NTDs/10 000 births
NTDs/10 000 births
“Recommendations on use of folic acid have had
no detectable impact on incidence of neural tube defects,
regardless of the recommendations’
form, timing, and intended target”
“ In addition to actively promoting the use of supplements,
public health agencies and medical professionals
should strongly consider
implementing food fortification programmes”
indicates time of supplement intake recommendations in each country
Blank top indicates terminated pregnancies
Incidence rate ratio (IRR) estimates the average yearly change in rate
Botto et al. BMJ. 2005;
(1 indicates increasing rates)
330(7491):571
Botto et al. BMJ. 2005; 330(7491):571.
FA fortification… …masks vitamin B12 deficiency

FA fortification masks vitamin B12 deficiency
Folic Acid Metabolic Pathway:
Methylated Product Substrate
(e.g. DOPA, myelin basic protein, methylated lipids) (e.g. Lipids, proteins)
S-Adenosylhomocysteine S-Adenosylmethionine
Homocysteine Methionine
Methionine synthase
Vitamin B12
5-Methyl- Tetrahydrofolate
tetrahydrofolate
Anemia
5,10-Methylene-
tetrahydrofolate
reductase Purines
5,10-Methylene- 10-Formyl- Dihydrofolate
tetrahydrofolate tetrahydrofolate
Pyrimidines
Folic acid
Adapted from Kraemer and Zimmermann. Nutritional Anemia. Sight and Life. 2007 (p.113)
FA fortification masks vitamin B12 deficiency
USA: Effect of FA Grain Fortification
(median age: 67 years)
Subjects
with low NO EFFECT:
vitamin percentage of people
B12 but
without Conclusion: with low vitamin B12
anemia but without anemia
(%) before, during, and
“There are no reports from countries
after fortification:
that have introduced mandatory fortification
not significantly
indicating deleterious effects on older people with
different
low vitamin B12 status.”
- Scientific Advisory Committee on Nutrition 2006
Optional fortification: Mandatory fortification:
March 1996 January 1998
Mills et al. Am J Clin Nutr. 2003;77(6):1474-7.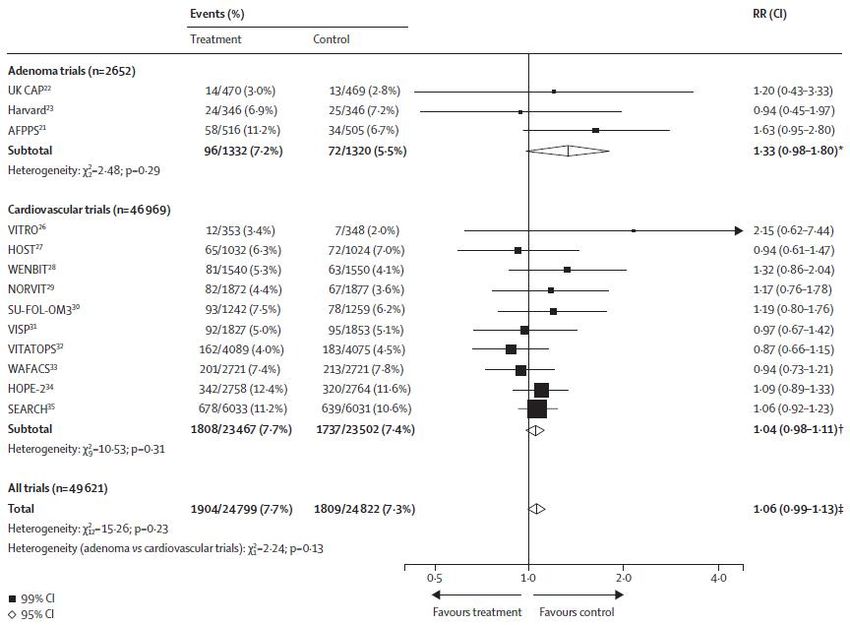
FA fortification… …leads to intakes above the UL

FA fortification leads to intakes above the UL
Canada: Intakes above the UL
Children and adolescents (1 – 19 years)
UL (1-3 years): 300 µg FA/day
UL (4-8 years): 400 µg FA/day
UL
UL
(9-13 years):
(14-18 years):
600 µg FA/day
800 µg FA/day
Conclusion:
In Canada only children and adults who
dietary FA intake: consumed
above the UL
based on mandated fortification levels: 0%
FA supplements had
adjusted for overages in fortified foods:
FA intakes above the
0%
UL.
adjusted for overages in fortified foods plus supplements: 1.2 to 4.0%
In the USA children 1 to 8 years might exceed the UL
based on folate intake from food alone which is probably due to
Adults (>19 years)
higher FA fortification levels in the USA.
UL (>19 years): 1000 µg FA/day
dietary FA intake: above the UL
based on mandated fortification levels: 0%
adjusted for overages in fortified foods: 0%
Shakur et al. Am J Clin Nutr.
adjusted for overages in fortified foods plus supplements: 1.2 to 5.0%
2010;92(4):818-25.
Hennessy-Priest et al. Public Health Nutr.
2009;12(9):1548-55.
Bailey et al. Am J Clin Nutr.
2010;92(2):353-8.
Shakur et al. Am J Clin Nutr. 2010;92(4):818-25.
FA fortification… …increases the risk of cancer

FA fortification increases the risk of cancer
Incidence of Colorectal Cancer (CRC)
USA Canada
Fortification of flour and
all cereal products
1996-1998 Fortification of flour
1998
Mason et al. Cancer Epidemiol Biomarkers Prev. 2007;16(7):1325-9.FA fortification increases the risk of cancer Herrmann and Obeid Dtsch Arztebl Int 2011; 108(15): 249–54.
FA fortification increases the risk of cancer
Effects of FA supplementation (0.5 mg to 5 mg/day) on overall first cancer incidence:
n=49 621
Conclusion:
FA treatment:
NO significant
“allocation to folic acid (0.5mg–5mg/day) effect on overall
for an average duration of 5 years cancer incidence
had no significant effect on
overall or site-specific cancer incidence
during the scheduled treatment period.”
“Nationwide dietary fortification involves doses of folic acid
that are an order of magnitude lower
than the doses studied in these trials.”
Vollset et al. 2013. Lancet.
Vollset et al. 2013. Lancet. RR=rate ratio; ICD=International Classification of DiseasesFA fortification… …changes the properties of drugs Reference:Dzinjalamala et al. Am J Trop Med Hyg. 2005;72(3):267-72.
FA fortification changes the properties of drugs
Malaria:
Gambia: Pregnant women received:
500–1,500 µg of FA per day
+
Sulfadoxine-pyrimethamine (SP) - folate antagonists
“…in an area of low SP resistance,
administration of folic acid to pregnant women
in a dose of 500–1,500 µg/day
will not interfere with the protective effect of SP when used for IPTp”
(IPTp: intermittent preventive treatment)
Mbaye et al. Am J Trop Med Hyg. 2006;74(6):960-4.FA fortification changes the properties of drugs
Malaria:
WHO recommendations (2012)
for areas of the Sahel sub-Region of
Africa:
“The (malaria prevention) strategy involves
the administration of monthly courses of
amodiaquine plus sulfadoxine-
pyrimethamine to all children under 5 years
of age during the high transmission season.”
http://www.who.int/mediacentre/factsheets/fs094/en/ (accessed 7.2.2013)FA fortification changes the properties of drugs
Malaria: Pemba substudy (Children 1-35 months of age):
Daily tablet [Iron (12.5 mg), FA (50 µg), with or without Zn (10 mg)] or Placebo
(half a tablet if 100 8.00 7.44 1.08 (0.58-1.98) 0.8
Iron-replete and anaemic 8.33 4.17 2.00 (0.46-8.75) 0.36
Iron-replete and non-anaemic 7.63 5.06 1.51 (0.57-3.98) 0.41
Iron-deficient and anaemic 5.13 10.11 0.51 (0.31-0.83) 0.006
Iron-deficient and non-anaemic 8.29 9.09 0.91 (0.42-1.98) 0.82
*deaths, hospital admissions
suggests: additional treatments at community level reduces hospital
admissions and deaths
Sazawal et al. Lancet. 2006; 367(9505):133-43.FA fortification changes the properties of drugs
Malaria: South Africa
Number of under-five deaths from malaria
100
90 Initiation of FA
80 fortification
70 Number of under-
Conclusion:
60 five deaths from
50 malaria
40
30
The role
20 and dose of FA in malaria endemic areas is not conclusive.
10
0
The management of malaria needs to improve.
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
2008:
90% of wheat flour and 70% of maize flour on the market were fortified
> 20 million people (66.5% of the population) consumed fortified wheat flour and maize meal
http://gainmap.gainhealth.org/admin/pdf/Africa.pdf
http://apps.who.int/ghodata/?vid=18400&theme=country#Conclusions Recommendations on the use of FA supplements have no detectable impact on incidence of neural tube defects. There are no reports as yet from countries that have introduced mandatory fortification indicating an increase of elderly with a low vitamin B12 status but without anemia. Intakes above the UL are unlikely, even with supplementation, if appropriate mandated fortification levels are followed. FA supplementation has no significant effect on the overall cancer incidence. The role of FA drug interactions in malaria endemic areas are not conclusive.
Thank you!
You can also read

















































