Ictus: epidemiologia, fattori di rischio, sintomi d'esordio, importanza fattore tempo, aggiornamento sulle terapie disponibili - Francesca Romana ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ictus: epidemiologia, fattori di rischio, sintomi
d’esordio, importanza fattore tempo,
aggiornamento sulle terapie disponibili
Francesca Romana Pezzella, MD, PhD, BSc, MBA, FEESO
Stroke Unit AO S Camillo Folrnaini
Roma, Italia
In Italia • 105.000 ricoveri/anno • 7000 meno di 45 anni
3
Costs of stroke in 2015 in the EU total €45 billion
€4 billion
9%
€5.4 billion
12
% 44%
€20 billion
35%
€15.9 billion
Direct healthcare costs Informal care costs Productivity losses Losses due to death
King’s College London for the Stroke Alliance for Europe (SAFE). 2017.
ISBN 978-1-5272-0858-2.
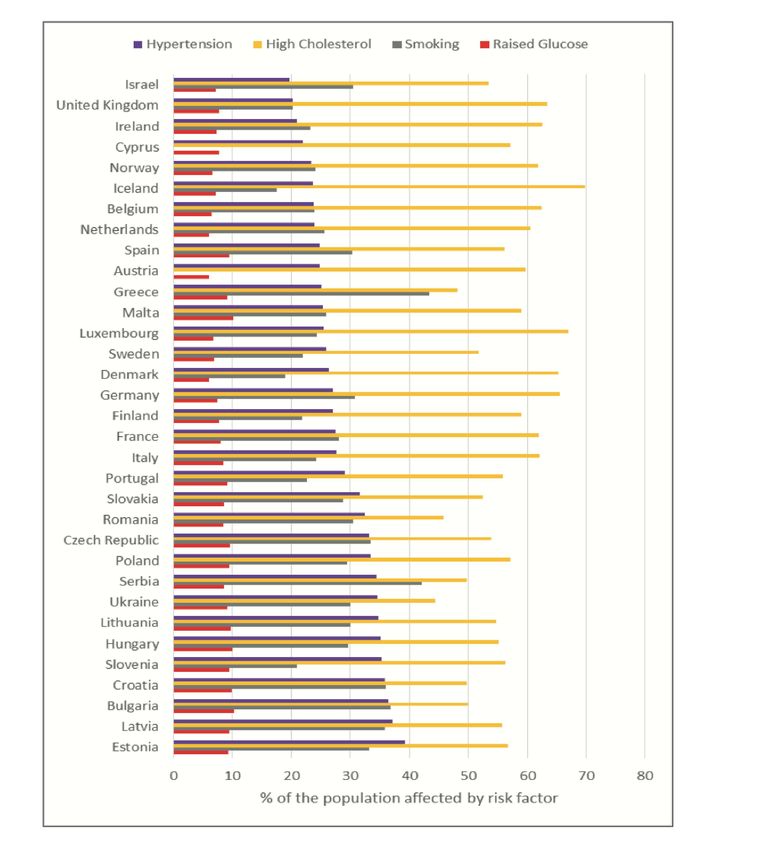
L’ictus si puo ̀
prevenire
• Dieci fattori di rischio
modificabili incidono sul 90%
di tutti gli ictus
• Ipertensione arteriosa,
dislipidemia, il fumo,
l’obesita ̀, il regime alimentare,
la fibrillazione atriale, il
diabete
Continuum of Stroke Prevention and Care
primary
prevention
family
Stroke Patient Associaion
stroke
social
onset
job
Stroke Awerness:
secondary Pre-hospital setting
prevention
Home In Hospital
long term Acute Phase
Care
Intensive
Rehab
Il tempo è cervello, il tempo è vita
Ischaemic core
(brain tissue
destined to die)
Penumbra
(salvageable
brain area)
An untreated patient loses Reperfusion offers the
approximately 2 million
neurons every minute in the
potential to reduce the
ischaemic area extent of ischaemic injury
Saver. Stroke 2006;37:263-266.
González. Am J Neuroradiol 2006;27:728-735.
Donnan. Lancet Neurol 2002;1:417-425.
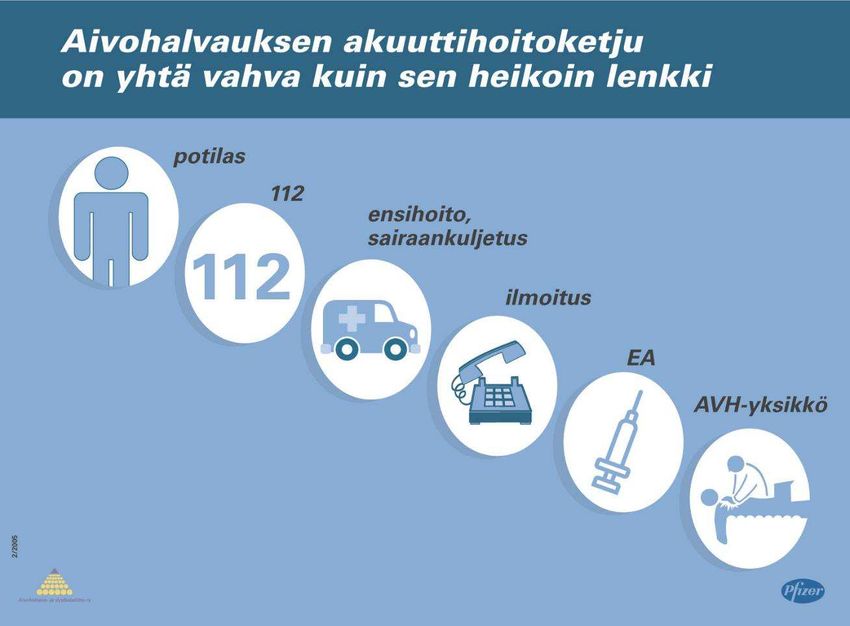
Ictus è una emergenza medica!
Patient Emergency
Call Centre
Emergency Medical
Services (EMS)
Notification
ER
Stroke Unit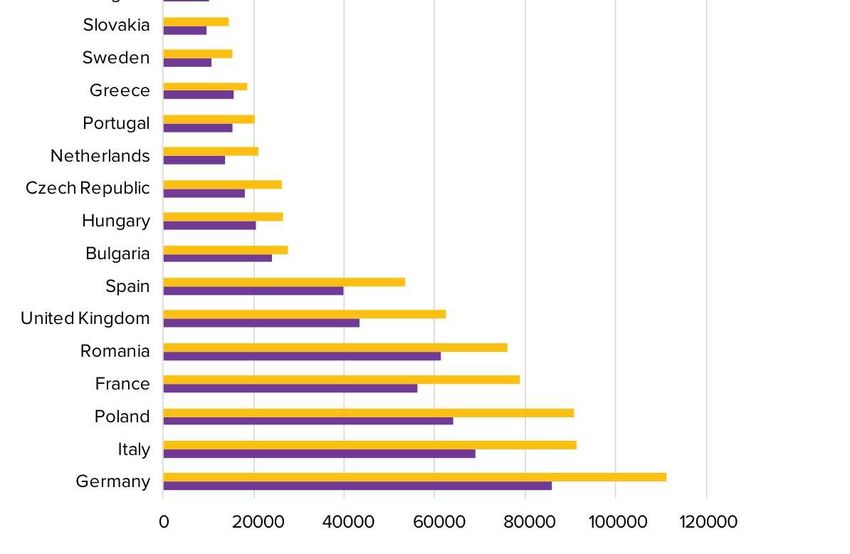
Terapie efficaci nell’ictus acuto
Intervention Evidence Death/handicap less Target Death/handicap less/
/ 1,000 patients 1m inhab.
Stroke unit Several RCTs + metaanalysis 50 (mRS 2-6) 100% 120
Aspirin 2 RCTs 12 (mRS 2-6) 80% 23
rt-PA < 3 h Several RCTs + metaanalysis 143 (mRS 2-6) 20% 69
rt-PA 3-4.5h Several RCTs + metaanalysis 71 (mRS 2-6) 10% 7
Interventional radiology 6 (+1) positive RCTs + 125 to 200 (mRS 3-6) 15% 19 to 30
metaanalysis (8 trials)
Hemicraniectomy Metaanalysis 500 (mRS 5-6) 1% 4 to 6
250 (mRS 4-6) 1% 2 to 3
Langhorne et al, Lancet 1993; IST, Lancet 1997; CAST, Lancet 1997; Emberson et al, Lancet 2014; Badhiwala
et al, JAMA 2015; Vahedi et al, Lancet Neurol 2007
Ricorda: Agisci in subito Il tempo è
cervello!
Most effective are:
Early recognition of stroke symptoms, including public education
Establishment of stroke networks
Prioritisation and direct transfer to specialised stroke centres
or stroke units
Management by multidisciplinary teams
Act fast to initiate treatment with thrombolysis as early as possible
Prima si inizia il trattamento, migliore sarà la prognosi!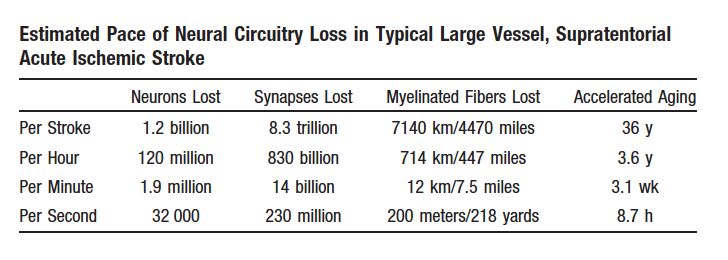
La Stroke unit è …
IMPACT OF SU
• A dedicated, well-defined area or ward in a hospital
ON AIS
• Patients are cared for by a multidisciplinary team (medical, nursing, and
therapy staff) who have specialist knowledge, training, and skills in stroke MANAGEMENT
care, with well-defined individual tasks, regular interaction with other
disciplines, and stroke leadership
• Stroke unit team coordinates stroke care through regular (weekly)
Stroke Unit (SU) multidisciplinary meetings
SU Departments SU Investigations SU Interventions SU Monitoring
INTRAVENOUS RT-PA
ACUTE STROKE BRAIN CT SCAN 24/7 HEART RATE
PROTOCOLS
STROKE OUTPATIENT CT PRIORITY FOR STROKE PTS RESPIRATORY SUPPORT OXYGEN SATS
EXTRACRANIAL DUPLEX ACCESS TO
INPATIENT REHAB BP
SONOGRAPHY HEMICRANIECTOMY
TRANSTHORACIC ACCESS TO HEMATOMA
OUTPATIENT REHAB BREATHING
ECHOCARDIOGRAPHY SURGERY
EXTERNAL REHAB TRANSOESOPHAGEAL ACCESS TO INTRA-ARTERIAL
TEMPERATURE
(COLLABORATION) ECHOCARDIOGRAPHY INTERVENTIONS
European Stroke Organisation
Ringelstein EB, et al. Stroke 2013;44:828-840.Protocollo infermieristico FeSS
Febbre Glicemia Deglutizione
(N=2 ELEMENTS) (N=5 ELEMENTS) (N=2 ELEMENTS)
FORMAL VENOUS GLUCOSE
EDUCATION PROGRAM AND
ON ADMISSION
COMPETENCY ASSESSMENT FOR
NURSES RUN BY SPEECH
4 - 6 HOURLY TEMPERATURE
1- 6 HOURLY FINGER-PRICK PATHOLOGISTS
READINGS FOR 72 HOURS
GLUCOSE FOR 72 HOURS
ON ADMISSION: 8-16 MMOL/L (ND)
SCREEN WITHIN 24 HOURS OF
OR 8-11 MMOL/L (D): SALINE
STROKE UNIT ADMISSION
INFUSION FOR THE FIRST SIX HOURS
GLUCOSE ≥16 MMOL/L (ND):
TEMPERATURE ≥37.5°C TREATED
WITH PARACETAMOL IV INSULIN
REFERRAL TO SPEECH PATHOLOGIST
FOR FULL ASSESSMENT FOR THOSE
GLUCOSE ≥11 MMOL/L (D): WHO FAILED THE SCREEN
IV INSULIN
Middleton S, McElduff P, Ward J, Grimshaw JM, et al. Lancet 2011;378(9804):1699-1706.IMPACT …
Independent QASC
Economic Evaluation
If FeSS protocols were
implemented in 65% of
the eligible Australian
patient populations for
one year the total
economic benefit (saving)
would be $281 M
Courtesy of QASC initiative15.7% reduction in death and disability 90 days post-
Clinical stroke (p=0.002; mRS)
significance 1%
Aspirin
5% Stroke
Unit
10% Thrombolysis
< 4.5 hrs
15.7% FeSS
Intervention
23% Hemicraniectomy
31% Endovascular Rx
(tPA plus thrombectomy)
Courtesy ofYou can also read

















































