How to Treat MYALGIC ENCEPHALOMYELITIS - Chronic fatigue syndrome Cathy Stephenson & Rose Silvester - New Zealand Doctor
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Online reading and accredited assessment Free Access Code:
available at www.howtotreat.co.nz/cfs DOCTOR
CFS
How to Treat
MYALGIC
ENCEPHALOMYELITIS
Chronic fatigue syndrome
Cathy Stephenson
& Rose Silvester
COMPLETE YOUR FREE EDUCATE MODULE ONLINE
➤Go to www.howtotreat.co.nz/cfs and use How much do you
the access code given on the cover of this reprint. already know?
Try this quiz
1 CR 1. There is a biomarker currently
DOCTOR
available that can confirm or
refute a diagnosis of ME/CFS.
True/False
EARN CPD CREDITS WITH
2. Post-exertional malaise is an
NEW ZEALAND DOCTOR RATA AOTEAROA EDUCATE increase in symptoms resulting
from the patient exceeding their
This continuing medical education activity has
energy envelope. True/False
been endorsed by the RNZCGP and has been
1 CR
approved for up to 1 CME credit for the General 3. Deconditioning is a significant
Practice Educational Programme and continuing contributor to the severity
professional development purposes. This activity of symptoms in ME/CFS.
will take up to 1 hour to complete (1 credit/hour). True/False
4. ME/CFS is a leading cause
Simply complete the online quiz-based assessment of long-term school absence.
True/False
at www.howtotreat.co.nz/cfs
5. Approximately 95 per cent
of children with ME/CFS are
undiagnosed. True/False
Educate is the clinical education content provided by 6. In order to diagnose ME/CFS,
a viral illness must precede
New Zealand Doctor Rata Aotearoa, published by The Health Media.
the onset of fatigue.
© The Health Media Ltd, 2021 True/False
Answers on page 7
Cover image: iStock.com – xavigm
DOCTOR
+HOW TO TREAT
Myalgic encephalomyelitis/
chronic fatigue syndrome
Fraz
Pull quote
Pull quote
pull quote
pull quote
pull quote
pull quote
pull quote
Myalgic encephalomyelitis/chronic fatigue syndrome is a common, debilitating and costly disease.
Diagnosing and managing complex chronic conditions such as this is not easy with
a 15-minute consultation, but this article, by Cathy Stephenson and Rose Silvester, provides
a framework of evidence-based information for GPs working with patients with ME/CFS
M
yalgic encephalomyelitis/ 1980s as the “Tapanui flu”. After an ini- predominance of autonomic nervous
Cathy Stephenson
chronic fatigue syndrome is a tial flurry of research, and concern for the system abnormalities. ME/CFS became
is a GP in
debilitating, chronic, multisys- fate of the New Zealanders who became a marginalised and neglected disease
Wellington and
tem disease that affects the neurological, unwell, interest waned. However, many a health column- with dramatic underfunding of research
autonomic, immune, endocrine, cardiac of these people remain unwell today, over ist. She has had Continued on page 4
and energy metabolism systems. It is diag- 30 years on. the privilege of
nosed with clinical criteria in the absence Although ME has been included in the learning about
of alternative diagnoses. International Classification of Diseases ME/CFS from her EARN RNZCGP
Though chronic fatigue is a symp- since the late 1960s, in 1988, the Centers patients, and is CME CREDITS
tom of ME/CFS, it is by no means the for Disease Control and Prevention (CDC) grateful to one of This continuing
only one. Core symptoms also include renamed it chronic fatigue syndrome. them for sharing medical education
their story here. activity has been
post-exertional malaise (PEM), cogni- Unfortunately, this name erroneously el-
endorsed by the
tive impairment, orthostatic intolerance evated fatigue to be the defining symptom
Rose Silvester RNZCGP and has been approved for up
(OI) and unrefreshing sleep. Importantly, and labelled it a syndrome rather than a to 1 CME credit for the General Practice
is a clinical
most people who present to general prac- disease. The supposition that aligned with psychologist and Educational Programme and continuing
tice with the symptom of chronic fatigue this was that CFS was a psychological carer of a person professional development purposes
do not fit the definition of ME/CFS. issue, not a physical one. with ME/CFS. She (1 credit/hour). To claim, complete the
The disease is known to occur both as This idea was compounded by the ab- is on the steering assessment at nzdoctor.co.nz. Click on
individual cases and in outbreaks. It first sence of a biomarker, the variable nature group of M.E. the Educate button.
came to Aotearoa’s attention in the early of the multisystem symptoms and the Awareness NZ
www.howtotreat.co.nz/cfs HOW TO TREAT 3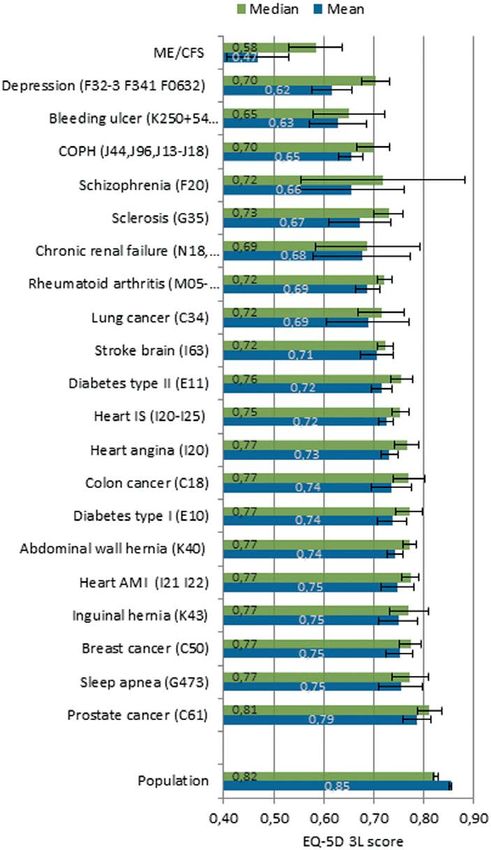
→ME / CFS DOCTOR
A wide range of seemingly unconnected
symptoms that vary by day or week
I
first met Amber a few years ago. She becoming increasingly difficult for her to neurological screen, I sent Amber for
was a 19-year-old student nearing attend her classes, and despite seeing a some blood tests. Of course, investiga-
the end of her first year at universi- range of doctors over the past two years, tions will vary from patient to patient,
ty. At our initial appointment, there were she was gradually getting worse. She de- but a basic screen would include:
no obvious clues as to what was going on scribed feeling like her body was a clock
with her: there was nothing in the way she that could not be wound up and was tick- Routine blood tests – complete blood
greeted me, or in the way she walked or ing more slowly each day. count, C-reactive protein, ferritin, electro
looked, to indicate how unwell she was She reminded me of a few patients I lytes, renal and liver function tests,
feeling. had met before who had similar expe- calcium, magnesium, blood glucose, thy-
She gave a two-year history of a wide riences – they all described a collection roid function tests, vitamin B12, folate,
range of symptoms, covering just about of seemingly unconnected symptoms vitamin D and coeliac antibodies (unless
every part of her body, without any ob- clustered around a central experience patient is on a gluten-free diet).
vious pattern to them. She talked about: of variability and a feeling of deep and
• fatigue ranging from mild to severe ongoing fatigue. I wondered whether Other tests if clinically indicated – im-
(sometimes so extreme she was bed- Amber, like them, might be experiencing munoglobulins, antinuclear antibodies,
bound) ME/CFS, and we discussed the steps we rheumatoid titres, creatinine kinase and
• “brain fog” or cognitive impairment could take to explore this possibility. cortisol.
• sleep problems – unrefreshing sleep
and insomnia Investigations If associated with a viral illness,
• muscle pains, aches and leg cramps – While there are clinical criteria that can consider – Epstein-Barr virus, cytomeg-
“as if I had run a marathon” help diagnose ME/CFS, it is important to alovirus and HIV testing. Also consider
• frequent cold and flu-like symptoms exclude other differentials – these are nu- testing for Lyme disease in patients who
She was
with chills merous and range from common things have travelled outside New Zealand,
pale, slow
• dizziness and weakness on standing we come across all the time in primary and a little if symptoms indicate.
• food sensitivities care, to obscure conditions we may have unsteady Amber returned the following week to
• urinary symptoms, including frequen- barely heard of (Panel 1, see page 5).2 on her feet, the news that all her blood tests were nor-
cy, urgency and pain After an unremarkable physical and reported mal, apart from a couple that were mildly,
• gastrointestinal problems. examination, including standing and feeling but not significantly, out of range. She did
Amber was worried because it was lying blood pressure and pulse, and a exhausted not look as well as she had the previous
week – she was pale, slow and a little un-
steady on her feet, and she reported feeling
Continued from page 3 Impaired oxygen consumption and acti- exhausted. When I remarked that she
vation of anaerobic metabolic pathways didn’t look well, she told me this was how
and lack of accurate training for medical in the early stages of exercise have been it was for her – the symptoms varied huge-
professionals. This vacuum of knowledge revealed in adults with ME/CFS. ly throughout the day and over the week.
allowed a proliferation of speculation that We discussed what she had done since
ME/CFS is a somatic symptom disorder. Neuroendocrine disturbances – dys- the previous appointment. She described
There is no evidence for this, however, regulation of the hypothalamic–pituitary– spending a night away with some friends,
and multiple pathophysiological chang- adrenal axis. Some patients have flat- and then being so shattered she was barely
es across multiple systems invalidate tened diurnal cortisol profiles compared able to get out of bed for two days.
any suggestion of malingering. with healthy people, despite normal I wondered if she was depressed, but
Research studies describe the following cortisol levels. although she described low energy, im-
pathophysiological changes, although it paired concentration, poor sleep, altered
is not known whether these occur before Blood pressure or heart rate regulation appetite and (on that day at least) had
the onset of the illness or because of it:1 abnormalities – many patients with ME/ quite marked slowing of speech and move-
CFS, particularly adolescents, experience ment, she did not describe low mood.
Immune system abnormalities – im- symptoms of OI – symptoms typically Also, she demonstrated a clear drive to
paired natural killer cell function and/or worsen when in an upright posture and do more, be in class and engage with peo-
T cell function, chronic increased pro- improve with recumbency. ple around her. She was clearly worried,
duction of inflammatory cytokines and, but objectively, her mood did not sug-
in some cases, slightly elevated levels of Many promising studies are cur- gest depression. Furthermore, depression
some autoantibodies (rheumatic factor, rently underway and will likely see our wouldn’t adequately explain the other
antithyroid antibodies, anti-gliadin understanding of pathophysiology symptoms she was describing (Table 1).3
antibodies, anti-smooth muscle antibod- substantially expanded in the next year.
ies and cold agglutinins). Focus is on establishing a biomarker, to
specifically test for ME/CFS, and sub It was as if my D-sized battery had
Cellular metabolism abnormalities typing of the condition – things that been taken out and replaced with a very
– impaired ability of cells to produce would certainly make life easier for health inadequate AA
energy from the usual “fuel” they use. providers and patients alike.
4 HOW TO TREAT www.howtotreat.co.nz/cfsDOCTOR
+HOW TO TREAT
Table 1 S
ymptom comparison between depression/anxiety disorders
Panel 1
and ME/CFS in children and adolescents3
Differential diagnosis2
Symptoms Depression/ ME/CFS Comments
anxiety Active medical conditions:
disorders u hypothyroidism/
hyperthyroidism
Fatigue, lack of Yes Yes In ME/CFS, fatigue tends to fluctuate u primary adrenal insufficiency
energy, difficulty during the day and from day to day
u diabetes
sleeping, cognitive
u iron deficiency anaemia
problems, weight
gain or loss u vitamin B12 deficiency
u iron overload syndrome
Absence Yes Yes ME/CFS is the most common medical u Cushing syndrome
from school cause of prolonged absence from school u coeliac disease
u depression
Depression, Yes Sometimes Patients with ME/CFS might be sad,
feeling sad for discouraged and fed up. Clinical depres-
u infectious diseases
no apparent sion is more likely in those who encounter (HIV, Epstein–Barr virus,
reason disbelief in the reality of their illness cytomegalovirus,
Lyme disease).
Anxiety Yes Sometimes In ME/CFS, anxiety can be associated
with having an undiagnosed illness, Rheumatological conditions:
ignorance about ME/CFS, and/or u rheumatoid arthritis
scepticism about the reality of the illness
u polymyalgia rheumatica
from family members, physicians or
u systemic lupus
school staff. Panic attacks are occasion
ally seen. There is a higher degree of u Sjögren syndrome.
anxiety in patients with comorbid OI and
joint hypermobility Other conditions:
u fibromyalgia
Feelings of Yes No Occasionally, young patients with u mast cell activation
worthlessness, ME/CFS feel guilty because the illness syndrome
guilt, low has caused family disruption. These
u orthostatic intolerance
self-esteem feelings are secondary to the illness
u small fibre polyneuropathy
Anhedonia Yes No Patients with ME/CFS often wish to u food intolerances
(lack of interest engage in, and still enjoy, previous u complex regional pain
and/or pleasure in activities but are limited by their energy syndrome
activities previously levels. Patients with depressive illness do u Ehlers–Danlos syndrome
enjoyed) not wish to engage in previous activities (hypermobility or
but are physically able to do so vascular type)
Severe Yes No Severe depression with suicidal thinking u underlying conditions
depression with is not present in ME/CFS without causing dysautonomias
suicidal thinking comorbid major depressive disorder u connective tissue conditions
(eg, Marfan syndrome)
Lack of interest Yes No Patients with ME/CFS often want to u multiple sclerosis
in friendships/ socialise but are physically and cognitively
u cardiovascular conditions
relationships unable to do so. Patients with depressive
u inflammatory bowel disease
illness often do not wish to socialise
u sleep disorders
Post-exertional No Yes A hallmark of ME/CFS. Patients with (eg, obstructive sleep
symptom depression/anxiety often feel better apnoea, narcolepsy)
worsening after exertion u craniospinal instability
u spinal stenosis
Orthostatic Occasionally Sometimes Much more common in patients with
intolerance ME/CFS
u cervical spinal fluid leak
u Chiari malformation
Hypersensitivities No Sometimes Common in patients with ME/CFS. u toxic substance exposure
to light, noise, Can contribute to feeling anxious and u malignancy
odours and overwhelmed u iatrogenic conditions such
medications
as medication side effects
Difficulty with No Sometimes Common in young patients with or interactions.
thermoregulation, ME/CFS
low body temper- Italicised conditions are
ature, intolerance commonly comorbid
to heat and cold
www.howtotreat.co.nz/cfs HOW TO TREAT 5→ME / CFS DOCTOR
An evidence-based approach to
diagnosis and classification is not easy
U
ntil other methods of diagnos-
ing ME/CFS become available, Post-exertional malaise is
we rely, to a large degree, on the a worsening of symptoms that
history we gain from our patients. In my occurs after patients exceed
conversations with Amber, it became clear their energy envelope
that she, like many others, was wary of the
ME/CFS label. This is not only because
of the historical stigma but also because
of the uncertainty around impact and
prognosis.
Considering this, I think it’s incredi-
bly important that, as doctors, we take
a thoughtful, considered and, where
possible, evidence-based approach to
diagnosis. In practice, this isn’t easy, with
inconsistencies between documents and
guidelines, and a plethora of other obsta-
cles getting in the way (Panel 2, see page 7).
Diagnostic criteria
When researching how best to proceed
with Amber, I came across the Institute
of Medicine’s (now the National Academy without cardiac arrhythmia, dyspnoea, just physical – for people at the severe end
of Medicine) 2015 revision of evidence sleep disturbance (hypersomnia, insomnia, of the spectrum, it could be as “minor” as
and proposal of diagnostic criteria. While sleep/wake reversal), small fibre neuro- brushing their teeth or having a conver-
this document has not been without pathy, OI, loss of thermostatic stability, sation with a friend.
its critics (some saying it oversimplifies sweating episodes, feverishness, acrocyan PEM is the symptom responsible for
a very complex problem), it has at least osis, chest pain, hypoglycaemia, PEM, the “push–crash” cycle: on a good day, a
provided a point from which ME/CFS can recurrent sore throat, flu-like symptoms, person may push themselves to do a little
be discussed, diagnosed and managed.4 new sensitivities to food/medications/ more, then crash afterwards, experienc-
If you want to look in more detail a di- chemicals,food allerg y, other allergic ing a worsening of symptoms as a result.
agnostic criteria, the CDC has published reactions/mast cell activation syndrome, This was exactly what Amber described
a useful summary of the symptom- widespread muscle pain, pelvic pain, allo after she spent a night with friends. Some
based case definitions that have been dynia, chest pain, joint pain, headaches, people report that this cycle results in an
used in clinical practice and research since unrefreshing sleep, swollen or tender ever-lowering baseline with each crash
1994 (https://bit.ly/39juMwa). lymph nodes, depression, anxiety/panic, joint (stepwise decline). While the mecha-
While the Institute of Medicine’s hypermobility, cold extremities and severe nisms of PEM are not well understood,
diagnostic criteria form the core fea- fatigue. exercise physiology researchers (some
tures of ME/CFS (Panel 3, see page 7), here in New Zealand) have shown that
patients will often have a multitude of Patients What is post-exertional ME/CFS patients have marked abnor-
additional symptoms and recognisable will often malaise? malities on two-day cardiopulmonary
syndromes that may require attention. have a While fatigue is often thought of as the exercise testing. When two sets of tests
These may represent underlying con- multitude defining symptom, it is obviously not are performed two days apart, patients
ditions that initially drove the patient of additional unique to ME/CFS. What is unique to with ME/CFS show a characteristic
towards ME/CFS, be contributing condi- symptoms ME/CFS is PEM. deterioration in exercise capacity on the
tions that perpetuate the problem, and/or PEM describes the unique energy pro- second day. This has helped to debunk
be part of the muddy downstream effect duction deficit of people with ME/CFS. any notion that ME/CFS is caused by
of the illness and of living with a chronic It is defined by a marked worsening of deconditioning.5,6
condition. symptoms (not just fatigue) in the period
If we highlight the diagnostic criteria following physical, mental or emotional
among the multitude of other symptoms exertion. A delay of 24 to 72 hours after Some days, I would have little-to-no
that sometimes cloud our vision, it can be exertion is usual, and symptom exacer energy and be confined to the sofa
easier to understand: bation may last days, weeks or much or bed. Other days, I had a decent
Perceptual and sensory disturbance, atax longer. For more information about PEM, amount of energy. I used to think,
ia, muscle weakness, fasciculations, visual refer to the M.E. Awareness NZ website wow, I have energy today – I must make
disturbance, cognitive impairment (brain (https://bit.ly/2JcqYlb and https://bit. the most of it! I’d go out and get things
fog), extreme pallor, nausea and gastro ly/3alBPoC). done, but then the next day, I would
intestinal symptoms, urinary frequency/ Note that the exertion required to trig- crash big time
bladder dysfunction, palpitations with or ger PEM can be mental or emotional, not
6 HOW TO TREAT www.howtotreat.co.nz/cfsDOCTOR
+HOW TO TREAT
Prevalence, onset and course of the
disease – ME/CFS does not discriminate
P
rior to meeting Amber, I had ME/CFS is a spectrum disorder
encountered only a handful of pa- Patients at the mild end of the spectrum At my worst, I remember being bedridden, having my
tients with ME/CFS, yet it’s not a can continue with their lives, albeit with flatmates bring me dinner, and attempting to eat while
rare disease. While prevalence estimates significant curtailing of usual activity. still lying down because I didn’t have the energy to sit up –
vary, ME/CFS is thought to affect 0.85 Patients who are moderately impaired the plate centimetres from my face, struggling to lift the
per cent of the population, and around have difficulty maintaining study or fork the short distance from the plate to my mouth
60 per cent of those affected are women. work, or standing or sitting for prolonged
We know that many people affected nev- periods.
er get a diagnosis (some estimates put this The approximately 20 per cent of ME/
as high as 91 per cent), which means many CFS patients who are severely affected are Panel 2
thousands of people are deprived of in- generally wheelchair-dependent, house or Obstacles to diagnosis1
terventions that may help and, sadly, are bed-bound and in need of full care. This
frequently recommended interventions level of severity can persist for months For healthcare providers, diagnosing ME/CFS
that can cause real harm.4 or even years. Those with severe ME/CFS can be complicated by the following factors:
Children are not spared, with adoles- may require home visits and/or Skype/ u As yet, there is no lab test or biomarker for ME/CFS.
cence being one of the two peak times of telephone contact to enable them to u Fatigue and other symptoms of ME/CFS are
onset (the other being in the 30s). A rigor- access healthcare. Read more about the common to many illnesses.
ous 2020 study in the US found prevalence care of severely ill patients on the CDC u For some patients, it may not be obvious to health-
rates of 0.75 per cent for children aged five website (https://bit.ly/3akjXKu). care providers that they are ill.
to 17. Less than 5 per cent of these young It surprised me that, although Amber u ME/CFS has an unpredictable pattern of remission
people had been diagnosed.7 ME/CFS is a had been on a reduced schedule of study and relapse.
leading cause of long-term school absence, and had all but eliminated other inter- u Symptoms vary from person to person in both
yet this is often misread by parents and ests, her presentation was considered frequency and severity – the most severely affected
authorities as school refusal. mild because she was still able to “func- may not seek care because they are too ill to go to
On further discussion with Amber, she tion” most of the time. However, she did a clinic.
described a fairly typical onset. She was describe periods of more severe exacerba- u The complexity and duration of the illness or
an active, healthy student in high school tions when study had not been possible prior healthcare experiences can contribute to
when she contracted a viral illness. While and she spent prolonged periods in bed. communication difficulties between patients and
she did gradually recover from this vi- She commented that the doctors she healthcare providers.
rus, a subsequent mild upper respiratory had seen previously appeared to minimise u There is a lack of adequate education about, and
tract infection saw her largely confined her reports of the severity of her symp- acceptance of, ME/CFS in the medical community.
to bed for many months. The respiratory toms. Yet at her worst, she had been too
symptoms were gone, but concomitant unwell to leave the house. Her symptoms
symptoms of malaise, body aches, chills during these times were invisible, as they
and dizziness on standing persisted. are for many others with ME/CFS. Panel 3
Though Amber’s viral illness was nev- Similar to many chronic conditions, Diagnostic criteria for ME/CFS4
er identified, common illnesses that recovery is possible for some patients
correlate with an acute onset of ME/CFS (around 5–10 per cent). Others improve Diagnosis requires the following
include herpesviruses (Epstein–Barr, cy- and are able to manage their illness to a three symptoms:
tomegalovirus, human herpesvirus 6 and point of minimal impact. The largest 1. a substantial reduction or impairment in the ability
7), enteroviral infections (eg, Coxsackie B) group, however, remains functionally dis- to engage in pre-illness levels of occupational,
and influenza. Less common triggers abled and significantly restricted by their educational, social or personal activities, which
include non-infectious immune prov- symptoms. A further group do not improve persists for more than six months and is accom
ocations (eg, anaesthetics), physical or may worsen over time. While there is panied by fatigue (often profound, of new or definite
or psychological trauma, and chemical or little research evidence, most experts agree onset, not the result of ongoing excessive exertion
toxin exposure. children have a slightly better outcome.1 and not substantially alleviated by rest)
Around 25 per cent of people will de- The impact of this condition should not 2. post-exertional malaise*
scribe a gradual or stepwise onset with be underestimated. Studies have shown 3. unrefreshing sleep.*
no obvious trigger. Although no gene has that patients with ME/CFS are typically
At least one of the two following manifestations
yet been identified, genetics does play more impaired in their functioning than
is also required:
a role. Twenty-seven per cent of people those with other chronic and disabling ill-
1. cognitive impairment*
with ME/CFS have first-degree relatives nesses, including congestive heart failure,
2. orthostatic intolerance.
diagnosed with ME/CFS or chronic depression, multiple sclerosis and end-
fatigue of unknown etiology.8 stage renal disease (Figure 1, see page 8).4,9 * Frequency and severity of symptoms should be
assessed – the diagnosis of ME/CFS should be
questioned if patients do not have these symptoms
Quiz answers at least half of the time with moderate, substantial or
severe intensity.
1. False 2. True 3. False 4. True 5. True 6. False
www.howtotreat.co.nz/cfs HOW TO TREAT 7→ME / CFS DOCTOR
Targeted management when no
pharmacological solutions are available
I
SOURCE: Falk Hvidberg M, et al. PLoS One 2015;10(7):e0132421. CC BY 4.0
t was hard to know where to start to
help Amber. As health professionals,
we are trained to “treat”, yet there
are no pharmacological solutions for
ME/CFS. However, there are a range of
management strategies that are sup-
portive for patients with ME/CFS. There
is both evidence and experience to show
that patients do better when their di-
agnosis and management is timely and
appropriate.
Validate the patient’s
experience
Amber commented a few months after
we first met that the most helpful thing I
did for her was to validate and affirm her
experience. This may sound simple, but
like many people with ME/CFS, Amber
had found it difficult to be heard. It had
been suggested to her that she was de-
pressed, overly focused on her symptoms,
and that she needed to “push through” the
fatigue. It felt important to partner with
Amber, and support her as best I could –
together, we would figure out what might
work for her.
Pacing
During the first few months after meet-
ing Amber, there remained considerable
uncertainty about what was causing her
symptoms. There was a lot to investi-
gate, and it was important to be thorough.
My hunch that this was ME/CFS was
sufficient to advise her to begin pacing im
mediately. Over the past few years, there
has been a fair amount of misunderstand-
ing about the role of pacing, largely due to
the popularity of a now debunked strat-
egy for managing ME/CFS called graded
exercise therapy.
Pacing is a strategy that reduces the
frequency and severity of PEM and poten-
tially mitigates longer term deterioration.
It involves determining the threshold at
which exertion (physical or cognitive)
elicits PEM, and then ensuring the sum
of all daily activities stays well beneath
that threshold (for more information:
https://bit.ly/3du3vJT).
As opposed to graded exercise therapy
(which promotes a rigid incremental in-
crease in exercise and is now known to be
harmful for those with ME/CFS), levels
of activity should only be very cautious-
Figure 1. A study by Falk Hvidberg and colleagues in 2015 reported that patients with ME/CFS ly increased if the patient experiences
have the lowest unadjusted EQ-5D-3L-based health-related quality of life compared with 20 improvement in energy levels. It is im-
other conditions, including multiple sclerosis and stroke9 portant to note that energy increase may
8 HOW TO TREAT www.howtotreat.co.nz/cfsDOCTOR
+HOW TO TREAT
Patients with Panel 4
severe ME/ Symptoms and
CFS may rely signs of orthostatic
on a wheelchair intolerance
and carers for
months or even OI presents as a worsening of
years symptoms on becoming upright
(in severe cases, this may be just
moving from fully to partially
recumbent) and on prolonged
standing.
Symptoms include:
u dizziness/light-headedness
u tachycardia
u changes in vision
u headache
u breathlessness
u syncope or presyncope
u pain, tingling or numbness
in feet (primarily), but also in
hands and face
u chest discomfort/pain
u acrocyanosis (discoloured ex-
tremities due to blood pooling)
u nausea
u distress/agitation
u loss of cognitive acuity.
1. PEM 2. OI 3. SLEEP 4. PAIN 5. BRAIN FOG Screen for OI using the NASA
Lean Test (https://bit.ly/38irsQK).
This requires 30 minutes or longer
Most troubling symptom Least troubling symptom
to carry out, a bed for the patient
to lie on and repeated measure
Figure 2. Amber’s stepwise symptom management ments of blood pressure and heart
rate, so needs planning if to be
done in a busy clinic. OI can be
never occur and should not be the goal. least troubling (Figure 2, above), which highly variable and may require
The variability of ME/CFS within a can be a really helpful way to prioritise multiple assessments to under-
day and across days/weeks, and the de- an approach when managing multiple stand the pattern. Patients may
lay between activity and the appearance symptoms. be able to conduct lean tests at
of PEM (up to three days), can make estab- Sleep, pain and cognitive issues are home, at different times of day
lishing the pacing threshold difficult. For common problems in general practice over several days, by recording
Amber, keeping a diary was helpful, as was populations, and GPs are well versed in heart rate with a fitness tracker
a heart rate monitor. Amber found main- how to manage them. We should approach or heart rate and blood pressure
taining her heart rate below 120 beats our symptom management for ME/CFS using a home device.
per minute was a useful way to minimise patients in the same way we would for In adults, postural orthostat-
PEM. anyone else, although these symptoms Energy ic tachycardia syndrome (POTS)
tend to be more persistent and resistant increase is defined by an increase in heart
to treatment in this group. may never rate of 30 beats per minute or
Since getting ME/CFS, I have had to As many people with ME/CFS find, occur and more within the first 10 minutes
adapt small things in my daily life, to Amber was very sensitive to medications, should not of standing, in the absence of
save energy where I can. Examples so the rule of “go low and slow” had to be be the goal hypotension. In children and
include using light cutlery, wearing carefully applied. As with other complex, adolescents, an increase of 40
clothes that are not too heavy or multisystem conditions, it was tempting beats per minute or more is used.
restrictive and wearing incredibly to prescribe medications for all her prob- Orthostatic hypotension is
comfortable shoes (to avoid muscle lems, but polypharmacy may have further defined by a decrease in systolic
aches). I also have short hair, so it’s complicated her situation. We stuck to blood pressure of 20mmHg or
easy to maintain and doesn’t take too tackling one thing at a time, in line with a decrease in diastolic blood
much energy to wash the symptom hierarchy. pressure of 10mmHg within three
One of Amber’s more troubling symp- minutes of standing.
toms was that of orthostatic intolerance Patients should be referred for
Stepwise symptom hierarchy (Panel 4). She described a cluster of symp- a tilt table test if results are well
Together, Amber and I agreed on a step- toms when standing still, which tended outside these limits or if symptoms
wise symptom hierarchy. This hierarchy to worsen on getting up from sitting or are unclear or severely disabling.
simply lists symptoms from most to lying. She felt light-headed, puffed, weak
www.howtotreat.co.nz/cfs HOW TO TREAT 9→ME / CFS DOCTOR
and muddled, with tingling/aching in While Amber did not meet the thresh- unable to attend full-time, support for
her feet. old for a diagnosis of POTS, she did learning can come from the Regional
OI is an abnormal autonomic nervous experience mild tachycardia on the NASA Health Schools (regionalhealth.school.
system response to orthostatic challenge, Lean Test (she had a sustained increase nz). Strong advocacy from a GP can sup-
and it is thought to be the most over- of 25 beats per minute with stable blood port families and can assist the RHS to
looked, yet potentially manageable, pressure) and reported that her symp- understand the capabilities and limita-
feature of ME/CFS. While OI does occur toms improved on resuming a recumbent tions of the child.
in adults with ME/CFS, it is almost uni- position. I am aware that this is coming last,
versal in adolescents, with >90 per cent The standard first-line strategy for which is ironic given its importance –
of young people experiencing it. Common managing OI is to increase daily fluid in- mental health. Adjusting to the losses
variants of OI are orthostatic hypoten- take (to 2–4L), and increase salt if blood that came with ME/CFS was hard for
sion, neurally mediated hypotension pressure is normal (Panel 5). This is of- Amber, and depression and anxiety sat
and postural orthostatic tachycardia ten enough to moderate the symptoms. alongside her at times, as they often do
syndrome. with chronic conditions. We worked to
Advocacy and support adapt the things she enjoyed – to bring
Although getting diagnostic clarity can be them within her “energy envelope” –
Panel 5 helpful as it enables us to use a targeted, and to find value in other manageable
Managing orthostatic intolerance evidence-based approach to management, things. It will be an ongoing adaptation
ME/CFS is a diagnosis that carries an un- – although Amber’s condition has stabi-
Advise the patient that they may benefit from: certain prognosis and has no definitive lised and she is able to predict and rely
u Being out of bed, as tolerated by fatigue (lying down treatment. Understandably, it is often upon her health a lot more, there are
for long periods will exacerbate postural symtoms), very difficult for our patients to accept. constant reminders that some things
and raising the head of the bed by 20cm. Patients with ME/CFS need the triad of are simply out of reach.
u Avoiding weight loss, but having regular, small support to optimise stability: clinical,
meals with smaller portions of carbohydrate. emotional and practical.
u Increasing fluid intake – begin with 2L per day and Most major centres have support net- Before the onset of ME/CFS, I had
assess response. This may be increased to up to works or groups for people with ME/ never struggled with mental health
4L per day. Water is best. Avoid caffeine drinks or CFS. These groups provide invaluable issues, but suddenly my ability
drinks with high sugar content as these may cause opportunities to connect with, and learn to carry out everyday tasks was
further dehydration. Drink a glass of water (at least from, others with ME/CFS. Some centres reduced and my life was impacted
400ml) to stimulate blood pressure control before also have field workers who can support in so many ways. It’s like losing
any orthostatic challenge, such as getting up in and advocate for patients. Information a limb – you have to learn how to
the morning, going shopping or showering. about these organisations can be found live within your new limitations
u Increasing salt intake if blood pressure is normal or on the M.E. Awareness NZ website and to cope with the strain it puts
low (in combination with increased fluid intake). (m.e.awareness.nz) or the Associated New on your mental health
Dose–response is individual but, as a guide, 5g salt Zealand ME Society website (anzmes.
per day is commonly required. Salt can be added to org.nz).
food or salty snacks can be introduced. Salt capsules NZcare4ME is an online, closed net- Referral for specialty
(eg, SaltStick) can provide a useful supplement and work of carers of young people with ME/ assessment and intervention
minimise nausea associated with high salt. These CFS. Entry to the group is via Facebook ME/CFS is complex and there is so
are costly, so consider including them in a disability (www.facebook.com/NZcare4ME). much yet to be discovered about this
allowance. Electrolyte drinks can substitute for some In terms of financial support, because disease. Making things more difficult
salt. Enerlyte can be obtained on prescription and ME/CFS is long-term, many people over for practitioners is that we receive
combined with a little lemon juice, or similar, to age 16 will be entitled to the Supported remarkably little training about it,
enhance taste. Sport shops stock electrolyte tablets Living Payment (https://bit.ly/2uP5Eyn). given it is a condition that is so preva-
that can be added to water. Avoid electrolytes Eligibility is not means tested, and the ap- lent and disabling. The need to make
containing high levels of sugar (eg, Powerade). plicant can be in part-time study or work differential diagnoses and to clarify
u Performing counter manoeuvres on standing/ to qualify. Care Plus, a programme that comorbid conditions can certainly
prolonged standing – these are manoeuvres that supports GPs and people with chronic stretch our capacity (particularly in a
increase muscle action in the legs and pelvis to health conditions, caters for higher needs 15-minute consultation), so referral
enhance blood flow against gravity (eg, walking on (https://bit.ly/2TEOYC2). to secondary care is almost certainly
the spot, foot raises prior to standing, crossing legs As Amber was functioning reason- going to be required.
in scissor fashion). ably well, she didn’t require home help or Ideally, there would be multidisci-
u Avoiding overly long or hot showers, or standing equipment. For patients who do, access is plinary teams of specialists to refer
or sitting for prolonged periods. via the somewhat convoluted Long Term to – ones that are able to integrate the
u Wearing pressure garments – over-the-counter Support-Chronic Health Conditions complexity of the multiple body sys-
garments can be trialled (ideally, toe to waist) or pathway, rather than through Disability tems involved – but the reality in New
medical-grade garments can be obtained on Support Services. This LTS-CHC fund- Zealand is that this is currently rarely, if
prescription. ing is administered by DHBs and accessed ever, available. The best advice I can give
u Encouraging recumbent exercise within limits of through Needs Assessment Service is to check your local HealthPathways,
pacing (eg, swimming, recumbent cycling). Coordination agencies. Unfortunately, to see if the pathway for ME/CFS has
u Reducing or stopping relevant medications. availability is limited to patients with been localised. If it has, refer according
“very high needs”. to their advice. If it hasn’t, discuss with
If the above strategies are ineffective, consider Young people with ME/CFS will usual- your colleagues or at your peer review
secondary referral where fludrocortisone, midodrine, ly require some support in their learning. group, and find out if there is a local
beta-blockers and pyridostigmine may be considered. For mildly affected children, school ac- specialist (physician, paediatrician
commodations may suffice.10 For those or rheumatologist) who has a special
10 HOW TO TREAT www.howtotreat.co.nz/cfsDOCTOR
+HOW TO TREAT
interest in these patients. Final thoughts
All too often, upon entering second-
ary health services, patients with ME/
This exploration of ME/CFS may have
thrown up more questions than it has
References
CFS report being passed from special- answered, but hopefully it can provide 1. Centers for Disease Control
ty to specialty and being reassessed a framework for working with this com- and Prevention. Myalgic
through a lens of doubt, speculation munity of patients. It is a challenging Encephalomyelitis/Chronic
or minimisation. Others report being diagnosis. Fatigue Syndrome: Information
told there is no help to be had. Add to Our obligation is to steer our patients for Healthcare Providers. April
that the infrequency of appointments, as away from interventions that have clear 2021. https://bit.ly/3cwkDhF
well as patients being unable to be seen harm and towards an understanding 2. US ME/CFS Clinician Coalition.
in their own home by secondary spe- that is based on evidence. However, we Diagnosing and Treating Myal-
cialists, and it is easy to see how many need to remain mindful that research has gic Encephalomyelitis/Chronic
patients can find it confusing, frustrating been scant, and the recommendations Fatigue Syndrome (ME/CFS).
and unrewarding. of experienced clinicians and researchers July 2020. https://bit.ly/38lsQlq
As GPs, we have the privilege of know- may precede the published evidence by 3. Rowe PC, Underhill RA,
ing our patients well, and we have the as much as 10 years. Friedman KJ, et al. Myalgic
opportunity to support and advocate It is likely that patients with ME/CFS encephalomyelitis/chronic
for them as they navigate this system will be immersed in this emerging infor- fatigue syndrome diagnosis
– ensuring their concerns are well repre- mation. From walking alongside Amber and management in young
sented, that myths or misunderstanding over the years, I have learnt a huge amount people: A primer. Front Pediatr
about the condition are not perpetuated – not only about my approach to the diag- 2017;5:121.
There is both
and that plans are progressing in a time- nosis and management of this condition 4. Institute of Medicine of the
evidence and
ly manner. At this stage, this may be the but also about the strength and resilience experience National Academies. Beyond
most valuable thing we can offer. of those whose lives are so affected by it. n to show that Myalgic Encephalomyelitis/
patients Chronic Fatigue Syndrome:
do better Redefining an Illness. 2015.
when their https://bit.ly/2To8mEJ
Useful resources diagnosis and
management
5. van Campen CMC, Visser FC.
The abnormal cardiac index
u Centres for Disease Control and Prevention. Myalgic Encephalomyelitis/ is timely and and stroke volume index
Chronic Fatigue Syndrome. January 2020. www.cdc.gov/me-cfs
appropriate
changes during a normal tilt
u Friedman KJ, Bateman L, Bested A, et al. Editorial: Advances in table test in ME/CFS patients
ME/CFS research and clinical care. Front Pediatr 2019;7:370. compared to healthy volunteers,
u Institute of Medicine of the National Academies. Beyond Myalgic are not related to decondition-
Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. ing. J Thrombo Circ 2018:107.
2015. www.nap.edu/read/19012 6. Hodges L, Nielsen T, Cochrane
u International Association for Chronic Fatigue Syndrome/Myalgic D, et al. The physiological time
Encephalomyelitis. Chronic Fatigue Syndrome Myalgic Encephalomyelitis: line of post‐exertional malaise
A Primer for Clinical Practitioners. 2014. https://bit.ly/36vm6TO in myalgic encephalomyelitis/
u Rowe PC, Underhill RA, Friedman KJ, et al. Myalgic encephalomyelitis/ chronic fatigue syndrome
chronic fatigue syndrome diagnosis and management in young people: (ME/CFS). Transl Sports Med
A primer. Front Pediatr 2017;5:121. 2020;00:1–7.
u Two RNZCGP-endorsed education modules on ME/CFS have been 7. Jason LA, Katz BZ, Sunnquist
created by ThinkGP: thinkgp.com.au/education M, et al. The prevalence of
pediatric myalgic encephalo
myelitis/chronic fatigue
syndrome in a community-
This publication has been reprinted by based sample. Child Youth Care
M.E. Awareness NZ to provide an update Forum 2020;49(4):563–79.
on the diagnosis and management of myalgic 8. Chu L, Valencia IJ, Garvert DW,
encephalomyelitis/chronic fatigue syndrome. et al. Onset patterns and course
The content is entirely independent and based of myalgic encephalomyelitis/
on published studies and the author’s opinion. chronic fatigue syndrome.
Front Pediatr 2019;7:12.
9. Falk Hvidberg M, Brinth LS,
M.E. Awareness NZ, m.e.awareness.nz@gmail.com, m.e.awareness.nz
Olesen AV, Petersen KD, Ehlers
L. The health-related quality of
This article has been reprinted from New Zealand Doctor Rata Aotearoa newspaper,
life for patients with myalgic en-
3 February 2021. The views expressed are not necessarily those of the publisher or sponsor.
cephalomyelitis/chronic fatigue
syndrome (ME/CFS). PLoS One
Produced by The Health Media, publisher of New Zealand Doctor Rata Aotearoa,
2015;10(7):e0132421.
PO Box 31905, Milford, Auckland 0741. Ph (09) 488 4286, Fax (09) 912 9257.
10. CDC. Myalgic Encephalomyeli-
tis/Chronic Fatigue Syndrome:
© The Health Media (NZ) Ltd, 2021.
Pediatric ME/CFS: Fact Sheet
For full details of our Terms of Use, visit
for Healthcare Professionals.
www.thehealthmedia.co.nz/terms-of-trade
July 2018. https://bit.ly/2uPn9yz
www.howtotreat.co.nz/cfs HOW TO TREAT 11You can also read