NZ ADOLESCENT & ADULT ASTHMA GUIDELINES 2020 - NZ Respiratory ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NZ ADOLESCENT & ADULT
ASTHMA GUIDELINES
2020
NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716 © NZMA
www.nzma.org.nz/journal

NZ Adolescent and Adult Asthma Guidelines
Asthma and Respiratory
Foundation NZ Adolescent
and Adult Asthma Guidelines
2020: a quick reference guide
Richard Beasley, Lutz Beckert, James Fingleton, Robert J Hancox,
Matire Harwood, Miriam Hurst, Stuart Jones, Susan Jones, Ciléin Kearns,
David McNamara, Betty Poot, Jim Reid
ABSTRACT
The purpose of the 2020 Asthma and Respiratory Foundation NZ Adolescent and Adult Asthma Guidelines
is to provide simple, practical and evidence-based recommendations for the diagnosis, assessment and
management of asthma in adolescents and adults (aged 12 and over) in a quick reference format. The
intended users are health professionals responsible for delivering asthma care in the community and
hospital settings, and those responsible for the training of such health professionals. The main changes
in the 2020 update are: 1) combining the recommendations for both adolescents and adults in a single
document, 2) the recommendation to avoid SABA-only treatment in the long-term management of asthma,
3) the use of budesonide/formoterol reliever, with or without maintenance budesonide/formoterol, is
preferred to SABA reliever, with or without maintenance ICS or ICS/LABA, across the spectrum of asthma
severity, 4) introduction of the terminology ‘anti-inflammatory reliever (AIR)’ therapy to describe the use
of budesonide/formoterol as a reliever medication, with or without maintenance budesonide/ formoterol
therapy. This approach encompasses and extends the ‘Single combination ICS/LABA inhaler Maintenance
And Reliever Therapy’ (SMART) approach recommended in the previous guideline, 5) the inclusion of two
stepwise management algorithms, 6) a clinical allergy section, 7) the role of LAMA therapy in severe asthma,
8) the role of omalizumab in severe allergic asthma and mepolizumab in severe eosinophilic asthma, 9) an
appendix detailing educational materials.
Abbreviations:
AIR Anti-inflammatory reliever
COPD Chronic obstructive pulmonary disease
FeNO Fraction of expired Nitric Oxide
FEV1 Forced expiratory volume in one second
FVC Forced vital capacity
GINA Global Initiative for Asthma
ICS Inhaled corticosteroid
IgE Immunoglobulin E
LABA Long-acting beta2-agonist
LAMA Long-acting muscarinic antagonist
pMDI Pressurised Metered Dose Inhaler
PaO2, PaCO2 Arterial oxygen and carbon dioxide tension
PEF Peak expiratory flow
SABA Short-acting beta2-agonist
SMART Single combination ICS/LABA inhaler Maintenance And Reliever Therapy
SpO2 Oxygen saturation measured by pulse oximetry
1 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMA
NZ Adolescent and Adult Asthma Guidelines
Context1–7 Grading
Asthma is a major public health problem No levels of evidence grades are provided
in New Zealand with up to 20% of children because the guidelines are formatted as a
and adults having asthma. The prevalence Quick Reference Guide. Readers are referred
rates, particularly in Māori and Pacific to the GINA 2019 Update strategy and
adults, are among the highest in the world. handbooks for the level of evidence for the
Providing health professionals with recommendations on which the guidelines
current best practice guidance sits within are based.
the Asthma and Respiratory Foundation Guideline development group
New Zealand’s work programme as a This group primarily includes members
priority action towards reducing New of the Asthma and Respiratory Foundation
Zealand’s significant respiratory health New Zealand Scientific Advisory Group and
burden. Three important documents were comprises representatives from a range of
released by the Foundation in 2015; Te Hā professions and disciplines relevant to the
Ora: The National Respiratory Strategy, scope of the guidelines. Development of
The Impact of Respiratory Disease in New the Adolescent & Adult Asthma Guidelines
Zealand: 2014 update and He Māramatanga was funded by the Asthma and Respiratory
huangō: Asthma health literacy for Māori Foundation New Zealand. No funding was
children in New Zealand. These place in sought or obtained from pharmaceutical
context the high prevalence and impact companies.
of asthma in New Zealand, the inequities
suffered by Māori, Pacific peoples and low
Peer review
The draft guidelines were peer-reviewed
income families, and the need for a holistic
by a wide range of respiratory health
approach when providing asthma care.
experts and key professional organisations,
Guidelines review8–10 including representatives from Asthma
The Asthma and Respiratory Foundation New Zealand, Can Breathe, New Zealand
New Zealand published the Adult Asthma Nurses Organisation Te Rūnanga o Aotearoa,
Guidelines in 2016 and the Childhood and Nurse Practitioner New Zealand, Compre-
Adolescent Asthma Guidelines in 2017. hensive Care, Hutt Valley DHB, Capital and
Since their publication, there have been a Coast DHB, Auckland DHB, Ngā Kaitiaki o te
number of major advances in the treatment Puna Rongoā, PHARMAC, Thoracic Society
of asthma in adolescents and adults. There of Australia and New Zealand, Internal
has also been greater recognition that the Medicine Society of Australia and New
investigation and management of asthma in Zealand, University of Auckland, Wellington
adolescents and adults (aged 12 and over) Free Ambulance Service and the Global
has a similar evidence base, which warrants Initiative for Asthma Scientific Committee.
the combining of guideline recommen-
dations across these age groups. For this
Presentation
The guidelines are primarily presented
reason, the 2020 update includes recommen-
through bullet points, key practice points,
dations for both adolescents and adults, and
tables and figures. Key references are
incorporates recent advances in knowledge
provided where necessary to support recom-
based on high-quality scientific evidence.
mendations that may differ from previous
The major document which has been
guidelines or current clinical practice.
reviewed to formulate the 2020 update is
An educational slide set is available on
the Global Initiative for Asthma (GINA) 2019
the website. The Asthma and Respiratory
Update strategy. As previously, a systematic
Foundation New Zealand encourages the
review was not performed; relevant refer-
integration of the graphs and figures into
ences were reviewed where necessary
local clinical pathways.
to formulate this guideline version and
referenced as required to support key Dissemination plan
recommendations. Readers are referred The guidelines will be translated into tools
to the GINA 2019 Update strategy for the for practical use by health professionals, and
more comprehensive detail that it provides, used to update Health Pathways and existing
accessed at https://ginasthma.org. consumer resources. The guidelines will
be published in the New Zealand Medical
2 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMA
NZ Adolescent and Adult Asthma Guidelines
Journal and on the Asthma and Respi- It is defined by the history of
ratory Foundation New Zealand website, respiratory symptoms such as
and disseminated widely via a range of wheeze, shortness of breath,
publications, training opportunities and chest tightness and cough that
other communication channels, to health vary over time and in intensity,
professionals, nursing and medical schools, together with variable expiratory
primary health organisations and district airflow limitation.
health boards.
Diagnosis10–12
Implementation • The diagnosis of asthma starts with
The implementation of the guidelines by the recognition of a characteristic
organisations will require communication, pattern of symptoms and signs, in the
education and training strategies. absence of an alternative explanation.
Expiry date • The key to making the diagnosis of
2024. asthma is to take a clinical history,
undertake a focused physical exam-
Definition10 ination, document variable expiratory
• The GINA consensus definition of
airflow limitation and assess response
asthma is:
to inhaled bronchodilator and/or ICS
• Asthma is a heterogeneous treatment (Table 1, Figure 1). There is
disease, usually characterised by no reliable single ‘gold standard’ diag-
chronic airway inflammation. nostic test.
Table 1: Clinical features that increase or decrease the probability of asthma.
A. Asthma more likely
• Two or more of these symptoms:
- Wheeze (most sensitive and specific symptom of asthma)
- Breathlessness
- Chest tightness
- Cough
• Symptom pattern:
- Intermittent
- Typically worse at night or in the early morning
- Provoked by exercise, cold air, allergen exposure, irritants, viral infections, beta blockers, aspirin or other non-ste-
roidal anti-inflammatory drugs
- Recurrent or seasonal
- Began in childhood
• History of atopic disorder or family history of asthma
• Widespread wheeze heard on chest auscultation
• Symptoms rapidly relieved by inhaled SABA or budesonide/formoterol
• Airflow obstruction on spirometry (FEV1/FVC < Lower limit of normal)
• Increase in FEV1 following bronchodilator ≥12%; the greater the increase the greater the probability
• Variability in PEF over time (highest-lowest PEF/mean) ≥15%; the greater the variability the greater the probability
B. Asthma less likely
• Chronic productive cough in absence of wheeze or breathlessness
• No wheeze when symptomatic
• Normal spirometry or PEF when symptomatic
• Symptoms beginning later in life, particularly in people who smoke
• Increase in FEV1 following bronchodilator
NZ Adolescent and Adult Asthma Guidelines
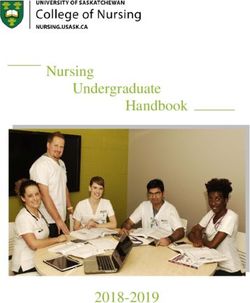
Figure 1: An approach to the diagnosis of asthma.
Modified from BTS/SIGN asthma guidelines.11
Practice points does not exclude asthma. There is a
• An increase in FEV1 ≥12% and substantial overlap in bronchodilator
≥200ml from baseline after bron- reversibility between individuals
chodilator therapy, has traditionally with asthma, COPD and those with no
been considered as a diagnostic respiratory disease, and as a result no
criterion for asthma. However, most clear-cut divisions can be suggested.
people with asthma will not exhibit The greater the magnitude of bron-
this degree of reversibility at one chodilator reversibility the greater
assessment, and normal spirometry the likelihood that there is an asthma
component to the disease.
4 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMA
NZ Adolescent and Adult Asthma Guidelines
• Alternative methods to identify • For symptomatic patients, asthma
variable airflow obstruction include severity can be determined only after
repeat measures of spirometry with a therapeutic trial of ICS for at least
bronchodilator reversibility, peak flow eight weeks. Start the therapeutic trial
variability with repeat measures at and book the follow-up appointment
different times of the day, and other for eight weeks later.
specialist tests such as measures of • Patients who initially present with
bronchial challenge testing. Once the frequent symptoms often have mild
diagnosis has been confirmed it is asthma, which can be well controlled
not necessary to routinely undertake with ICS-based therapy.
bronchodilator reversibility testing.
• Asthma symptom control is defined
• In most patients, observing a symp- by the frequency of symptoms, the
tomatic response to treatment may degree to which symptoms affect sleep
help confirm the diagnosis, however a and activity, and the need for reliever
limited response to bronchodilator or medication.
ICS does not rule out asthma. It may
be difficult to distinguish between Practice point
a diagnosis of asthma and COPD, in Many patients under-report their asthma
adults with a smoking history, as symptoms. Different methods for assessing
they may have clinical features of asthma symptom control are available
both disorders. If asthma is believed including:
to be part of the presentation, the i) Asthma Control Test (ACT)
management must include an ICS. This test has been widely validated and is
• The possibility of an occupational recommended with the following cut points:
cause should be considered in all 20–25: well controlled
cases of adult onset asthma. If occupa-
16–19: partly controlled
tional asthma is suspected, it needs to
be formally investigated and this may 5–15: poorly controlled
require specialist referral. The latest version of the test can be
accessed via http://www.asthmacontrol.
Assessing asthma severity, control
co.nz/.
and future risk10–14
Evaluation of asthma severity, the level of ii) Australian Asthma Handbook
control and the risk of future events are all This provides useful alternative questions
important components of the assessment of that might be used to assess control (Table 2).
individuals with asthma. Assessment of the risk of adverse
Severity of asthma is defined by the outcomes including severe exacerbations
treatment needed to maintain good control. and mortality (Table 3).
Table 2: Definition of levels of recent asthma control in adults and adolescents (regardless of current
treatment regimen).
Good control Partial control Poor control
All of: One or two of: Three or more of:
Daytime symptoms ≤2 days Daytime symptoms >2 days per Daytime symptoms >2 days per
per week week week
Need for SABA reliever ≤2 days Need for SABA reliever >2 days Need for SABA reliever >2 days
per week† per week† per week†
No limitation of activities Any limitation of activities Any limitation of activities
No symptoms during night or Any symptoms during night or Any symptoms during night or
on waking on waking on waking
† SABA, not including doses taken prophylactically before exercise. (Record this separately and take into account
when assessing management.)
Note: Recent asthma symptom control is based on symptoms over the previous four weeks.
Modified from the Australian Asthma Handbook.12
5 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMA
NZ Adolescent and Adult Asthma Guidelines Table 3: Clinical features associated with increased risk of severe exacerbations and mortality. A. Asthma • Poor symptom control • One or more exacerbation requiring oral corticosteroids in the last year • Hospitalisation or emergency department visit in the last year • High SABA use (≥3 canisters per year) • Home nebuliser • History of sudden asthma attacks • Impaired lung function (FEV1

NZ Adolescent and Adult Asthma Guidelines
Figure 2:
Adapted from GINA Update.10
It is recommended that for the regular Reliever therapy10,17–23
administration of ICS or ICS/LABA, if a pMDI • SABA reliever as sole therapy (without
is used, it is self-administered with a spacer ICS or ICS/LABA) is no longer recom-
device. There are two methods for inhaling mended in the long-term management
via a spacer: one deep slow inhalation and a of asthma in adolescents or adults.
10 second breath-hold; or 5–6 tidal breaths,
• Long-term treatment with ICS/fast-
with one actuation of medication into the
onset beta2-agonist reliever therapy is
spacer at a time.
superior to SABA reliever in reducing
Adherence can be checked using multiple exacerbation risk in adolescents and
techniques (questioning, diaries, apps, adults, across the range of asthma
pharmacy dispensing records). Patients’ severity.
understanding of the regimen should be
• In New Zealand the only ICS/fast-onset
confirmed, including their health beliefs,
beta2-agonist combination product
with their regimen tailored accordingly
that is available is budesonide/formo-
where possible. Fears and misconceptions
terol and to date this is only approved
are common barriers to adherence.
as reliever therapy using the Turbu-
Good inhaler technique and adherence haler device. As a result budesonide/
should be confirmed before any increase formoterol Turbuhaler is the
in treatment is initiated. Practice nurses preferred reliever treatment for inter-
and pharmacists may be well placed to mittent, mild, moderate and severe
undertake these checks. asthma. One actuation of budesonide/
Practice points formoterol 200/6µg or 100/6µg via
• Check adherence and inhaler tech- Turbuhaler is taken as required to
nique (and instruct patients using relieve symptoms, rather than the
a physical demonstration of correct two puffs at a time traditionally used
technique) at every visit. with SABA pMDI reliever inhalers.
The budesonide/formoterol 400/12µg
• Consider alternative inhaler devices if
formulation should not be used as
persistent difficulty with technique.
reliever therapy.
7 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMA
NZ Adolescent and Adult Asthma Guidelines
• Repeat administration of budesonide/ Anti-Inflammatory Reliever (AIR)
formoterol or salbutamol in the ratio
therapy
of 6µg formoterol to 200µg salbutamol
• AIR therapy (Figure 3) uses the combi-
results in a similar short-term bron-
nation budesonide/formoterol inhaler
chodilator response in the treatment
taken as-needed to relieve symptoms.
of acute asthma.
This can be done:
• Budesonide/formoterol 200/6µg
i) without maintenance ICS: just using
one inhalation as-needed, as sole
the combined budesonide/formoterol
reliever therapy, reduces the risk of a
inhaler to relieve symptoms in mild
severe exacerbation by at least 60%
asthma.
compared with SABA sole reliever
therapy in adolescents and adults ii) with maintenance budesonide/
with mild asthma. This regimen is formoterol: using the combined
recommended as the preferred initial budesonide/formoterol inhaler taken
treatment in patients with inter- regularly, with an additional dose
mittent or mild asthma. taken as-needed to relieve symptoms
in moderate and severe asthma. This
• Budesonide/formoterol as reliever
approach is also known as ‘Single
therapy reduces the risk of a severe
combination ICS/LABA inhaler Mainte-
exacerbation by about one-third
nance and Reliever Therapy’ (SMART).
compared with SABA reliever therapy
in adolescents and adults taking • AIR therapy requires a fast-onset
maintenance ICS/LABA therapy. beta-agonist combined with an ICS in
As a result budesonide/formoterol a single inhaler for as-needed use to
maintenance and reliever therapy is relieve symptoms. At present the only
preferred to maintenance ICS/LABA such combination inhaler available
and SABA reliever therapy for the in New Zealand is budesonide/formo-
treatment of patients with moderate terol, and it is only approved for use
to severe asthma. as a reliever therapy with the Turbu-
haler device. While there is evidence
• This evidence has led to the term
of efficacy/safety with budesonide/
‘Anti-Inflammatory Reliever’ (AIR)
formoterol pMDI used as a reliever
therapy to describe the use of
therapy, the pMDI formulation is
budesonide/formoterol as a reliever
not licensed for reliever use and
medication, with or without mainte-
therefore this would represent an
nance budesonide/formoterol therapy.
off-label prescription.
This approach encompasses and
extends the ‘Single inhaler Mainte- • Other ICS/LABA combinations
nance and Reliever Therapy’ (SMART) available in New Zealand that do not
approach recommended in previous contain formoterol, such as fluti-
guidelines (see below). casone propionate/salmeterol or
fluticasone furoate/vilanterol, should
ICS treatment10,17–22,24–30 not be used in this way.
ICS are the preferred anti-inflammatory
• Patients should not be prescribed
‘preventive‘ therapy. ICS may be adminis-
budesonide/formoterol as a reliever
tered as:
therapy in addition to maintenance
A) Budesonide/formoterol ‘Anti-Inflam- fluticasone propionate/salmeterol or
matory Reliever’ (AIR) therapy with fluticasone furoate/vilanterol, as there
or without maintenance budesonide/ is no evidence base for the use of two
formoterol different ICS/LABA products together.
B) Maintenance ICS together with SABA • When using budesonide/formoterol
reliever therapy combination inhaler for both regular
C) Maintenance ICS/LABA with SABA maintenance use (once or twice daily),
reliever therapy and for relief of symptoms (one actu-
ation as required), patients should not
be prescribed a SABA reliever inhaler.
8 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Maintenance fixed dose ICS plus LABA inhalers are a risk if patients
are poorly adherent with ICS therapy.
SABA reliever
LABAs should not be prescribed in a
• Regularly scheduled ICS may be taken
separate inhaler from ICS in patients
as maintenance therapy together with
with asthma.
SABA reliever therapy.
• When taken as regular mainte- Stepwise approach to asthma
nance therapy, the daily doses of ICS treatment22,31
which achieve 80–90% of maximum Pharmacological treatment
obtainable efficacy are shown in Table In the stepwise approach to asthma
4. These can be considered ‘standard’ management, patients step up and down as
doses for ICS, rather than ‘low’ doses. required to achieve and maintain control of
Some patients with severe asthma will their asthma and reduce the risk of
require higher doses of ICS. exacerbations.
• It is recommended that when ICS i) AIR therapy-based algorithm: This
therapy is initiated as a regular is the preferred algorithm, and is
maintenance treatment, either as a based on the use of budesonide/
separate inhaler or in combination formoterol as reliever therapy, with
with a LABA as an ICS/LABA inhaler, or without regular maintenance
these standard doses are used. There budesonide/ formoterol therapy.
is no greater benefit with initiation of The use of budesonide/formoterol
ICS therapy at higher doses. as both maintenance and reliever
Maintenance fixed dose ICS/LABA therapy at steps 2 and 3 is also known
plus SABA reliever therapy as ‘Single combination ICS/LABA
• A combination ICS/LABA inhaler may inhaler Maintenance and Reliever
also be taken as regular maintenance Therapy (SMART)’. The budesonide/
therapy together with SABA reliever formoterol 200/6µg Turbuhaler
therapy. The maintenance ICS/LABA formulation is used as the basis for the
with SABA reliever therapy regimen algorithm as this is the only formu-
is less effective than budesonide/ lation which has both an evidence
formoterol maintenance and reliever base and regulatory approval for
therapy regimen at reducing severe AIR therapy with or without regular
exacerbations in patients with a maintenance budesonide/formoterol
history of severe exacerbations. therapy. At step 2 the choice of one
inhalation twice daily or two inhala-
• Fluticasone furoate/vilanterol
tions once daily will depend on patient
100/25µg one inhalation once daily
preference.
represents an option for patients who
may prefer once daily medication use. ii) SABA reliever therapy-based algo-
This regimen does not reduce the risk rithm: This alternative algorithm is
of severe exacerbations compared based on the use of a SABA as reliever
with optimised usual care. therapy, in addition to ICS or ICS/LABA
maintenance therapy.
• LABA monotherapy is unsafe in
patients with asthma and separate
Table 4: The recommended standard daily dose of ICS in adult asthma.
Beclomethasone dipropionate 400–500µg/day
Beclomethasone dipropionate extrafine 200µg/day
Budesonide 400µg/day
Fluticasone propionate 200–250µg/day
Fluticasone furoate 100µg/day
9 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Figure 3: Stepwise anti-inflammatory reliever (AIR) based algorithm.
Figure 4: Stepwise anti-inflammatory reliever based algorithm.
10 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Practice points New Zealand for asthma. The alternative
• Although current evidence indicates approach of prescribing an ICS/LABA/
that the AIR-based strategy is more LAMA ‘triple therapy’ is neither MEDSAFE
effective at preventing exacerbations, approved nor funded in New Zealand.
the traditional treatment approach LAMA therapy is funded for patients with
may be preferred for individual COPD with or without co-existent asthma,
patients if their asthma is already well diagnosed using spirometry, as long as
controlled on this regimen, or if they the prescription is endorsed accordingly.
have poor technique with the Turbu- As a result it is currently recommended
haler device. that a LAMA may be considered in asthma
patients with features of COPD, who are not
• Consider stepping up if uncontrolled
controlled at step 3.
symptoms, exacerbations or at
increased risk, but check diagnosis, Biological treatments35–37
adherence, inhaler technique and Monoclonal antibody treatments targeting
modifiable risk factors first. specific inflammatory pathways now have
• Consider stepping down if symptoms an established role in severe uncontrolled
are controlled for three months asthma. They may be effective for patients
and the patient is at low risk for with severe asthma and elevated serum
exacerbations. IgE or markers of Th-2 inflammation (high
blood eosinophil counts). Omalizumab
• At each step check inhaler technique,
(targeting IgE) and both mepolizumab and
adherence to treatment, under-
benralizumab (targeting Interleukin-5)
standing of self-management plan and
are currently licensed in New Zealand for
barriers to self-care.
administration by sub-cutaneous injection.
• Stopping ICS completely is not At the time of writing, omalizumab is publi-
advised. The minimum level of cally funded in people aged six and above
treatment recommended is as-needed and mepolizumab is funded in people aged
budesonide/formoterol. Treatment 12 and above, meeting specific criteria. The
with a SABA reliever alone, without choice of agent is determined by the inflam-
maintenance ICS or ICS/LABA therapy matory pathway to be targeted and likely
is not recommended. to be influenced by the funding guidelines
• Consider referral for specialist review and cost of treatment. There is insufficient
and consideration of addition of other evidence regarding comparative efficacy
treatments if persistent exacerba- between the different drugs. They should be
tions or poor control despite step 3 considered as add-on treatments in patients
treatment. with severe disease and are likely to remain
• Asthma is common in older people specialist-only treatments for the fore-
and multi-dimensional assessment seeable future.
may be required to address compli- Other medications10,38
cating factors such as comorbidities Alternative therapies such as sodium
and frailty. cromoglycate or nedocromil may be
Add-on treatments considered in some patients with mild
asthma. Montelukast should also be
LAMAs32–34 considered as add-on therapy in patients not
Long-acting muscarinic antagonists
controlled on standard treatment and in all
(LAMAs) have efficacy in severe asthma
patients with aspirin-exacerbated respi-
not well-controlled on ICS/LABA. When
ratory disease. Prescribers should be aware
added to ICS/LABA treatment they modestly
of the risk of neuropsychiatric events asso-
reduce the risk of severe exacerbations,
ciated with montelukast.
and improve lung function and symptom
control. The strongest evidence is with Additional high dose ICS, oral corticoste-
tiotropium 5µg/day delivered via the roids, oral theophylline and azithromycin
Respimat device. The addition of tiotropium may be considered as other add-on treat-
to maintenance ICS/LABA is a MEDSAFE ments, with specialist review. Both risks
approved indication, but is not funded in and benefits of these treatments should be
considered.
11 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
The provision of a home nebuliser for • As people in low income households
administration of bronchodilator medi- have a higher burden of disease
cation is discouraged, due to the high dosing and can face barriers to accessing
and the potential for delay in seeking healthcare provision and medi-
medical review with its repeated use in a cations, it is appropriate to check
severe exacerbation. whether patients are accessing their
government support entitlements
Non-pharmacological measures39,40
and refer to support services as
• Key non-pharmacological measures
appropriate.
to improve asthma outcomes include
smoking cessation (including Specific allergy issues41–48
cannabis, e-cigarettes and vaping), A diagnosis of allergy requires a history
weight loss, asthma education, regular of reaction to a given allergen, and is
exercise and breathing exercises. confirmed by detection of specific IgE
• Avoid triggers that have been iden- antibodies, either on serum or by skin
tified to provoke attacks in particular prick testing. Skin prick testing has a high
attacks associated with features of negative predictive value for allergy to the
anaphylaxis. Specifically question antigen used and a low risk of systemic
about sensitivity to aspirin and allergic reactions, but serum specific
non-steroidal anti-inflammatory IgE may be more appropriate in certain
drugs, and consider aspirin-exac- settings, eg, patient unable to stop anti-
erbated respiratory disease in such histamine medications, unstable asthma,
patients, especially if there is a history pregnancy or dermatographism. Aeroal-
of nasal polyps. lergens such as house dust mite, pollens or
pet dander are the most common allergic
• Currently available house dust mite
triggers for asthma.
avoidance measures are not effective.
Allergen immunotherapy can offer
• Modifications to diet are unlikely
clinical improvements in asthma. Confir-
to improve asthma control. Food
mation of specific IgE is required prior to
avoidance should not be recom-
starting. Both sublingual and subcutaneous
mended unless an allergy or
immunotherapy are available but unfunded
sensitivity has been confirmed.
in New Zealand for aeroallergens; treatment
• Exercise should be encouraged. If can be expensive and time-consuming.
exercise provokes asthma this is a Aspirin desensitisation for patients with
marker of poor control and should aspirin-exacerbated respiratory disease
lead to a review of treatment, rather should be done under immunologist/
than exercise avoidance. In addition, allergist guidance.
reliever may be taken pre-exercise.
Asthma is the most significant risk factor
• Limitation of exposure or removal for fatal food-related anaphylaxis. Failure to
from the workplace is crucial in the recognise and treat anaphylaxis contributes
management of occupational asthma. to the risk of fatality.
Early removal from exposure may
lead to a complete remission. Practice points
• Consider testing for allergen-specific
• Asthma control may be improved by
IgE to aeroallergens in patients with
a warm, dry domestic environment.
allergic asthma.
Where a patient is living in poor
quality or damp housing, referral • Allergen immunotherapy may be
to locally available support services considered in patients with allergic
such as the healthy homes initiative is asthma and allergic rhinitis who have
appropriate. evidence of allergy to house dust mite
and/or pollens.
• Unflued gas heaters may worsen
asthma symptoms; electric heat • All patients with food-related
pumps are recommended. anaphylaxis should be referred to an
immunologist/allergist.
12 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Treatable traits49–52 discussed with all people with asthma.
In patients with difficult to treat asthma Copies should be kept in their medical
a key feature of management is the recog- records. A variety of formats are available
nition and treatment of overlapping for patients and their families, and the most
disorders, comorbidities, environmental appropriate source of information for the
and behavioural factors for which specific patient should be assessed, whether written,
treatment is available, recently referred pictorial, electronic, app etc.
to as ‘treatable traits’. The assessment Practice points
and management of some of the treatable • Asthma action plans should be based
traits may require specialist referral and on symptoms with or without peak
consideration of additional interventions. flow measurements and comprise
Systematic assessment of treatable traits either three or four stages depending
in the severe asthma clinic is associated on patient and health professional
with improved outcomes. One schema to preference.
consider is as follows:
• Asthma and Respiratory Foundation
Table 5: Treatable traits in asthma.
NZ asthma action plans can be down-
Overlapping disorders loaded from their website http://
asthmafoundation.org.nz/:
• COPD
• Bronchiectasis • Budesonide/formoterol reliever ±
maintenance (AIR plan)
• Allergic bronchopulmonary aspergillosis
• Dysfunctional breathing including vocal • ICS plus SABA (four-stage plan)
cord dysfunction • ICS or ICS/LABA plus SABA (three-
stage plan)
Comorbidities
• Obesity • The peak flow level at which patients
are guided to recognise worsening
• Gastro-oesophageal reflux disease
asthma is around 80% (of best), severe
• Rhinitis
asthma at 60–70% of best and an
• Chronic rhinosinusitis ± nasal polyps asthma emergency at around 50% of
• Obstructive sleep apnoea best.
• Depression/anxiety • The four-stage plan has been shown
Environmental to be effective in the management
• Smoking of asthma. In this plan there is an
• Damp, mouldy, cold or crowded housing extra step giving patients the option
• Occupational exposures of increasing the dose of ICS, up to
• Provoking factors including aeroallergens four-fold, through increasing the
frequency of use, and/or the dose at
• Drugs such as aspirin, other non-steroidal
each use, in response to worsening
anti-inflammatory drugs and beta blockers
asthma symptoms or deteriorating
• Insufficient income to access healthcare peak flow. Patients should be advised
Behavioural to return to their normal ICS dose
• Adherence once asthma symptoms and peak
• Inhaler technique flows have improved.
• Health literacy • The recommended action plans can
be modified as required depending on
Practice point patient and practitioner preference.
The treatable traits approach is particu- • The standard regimen for a course of
larly important for a patient who has poorly prednisone in the situation of severe
controlled asthma and/or poor respiratory asthma is 40mg daily for five days.
health. An alternative regimen is 40mg daily
Self-management53–56 until definite improvement, and then
Self-management based on a written, 20mg daily for the same number of
personalised, action plan improves health days. These regimens may need to be
outcomes and should be offered to and adjusted according to clinical factors
13 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
such as weight, comorbidities and • Inhaler technique should be routinely
interactions with other medications. assessed at consultations and training
• Adherence to treatment should provided as part of self-management
be routinely assessed and encour- education. If using a pMDI, it is pref-
agement provided as part of the erable to administer via a spacer.
self-management education. For • A four-step adult asthma consultation,
example, encourage patients to link which includes guidance for writing
their inhaler use with some other an asthma action plan, is provided in
activity such as cleaning their teeth the Appendix.
(and then rinsing their mouth).
AIR asthma action plan with budesonide/formoterol reliever ± maintenance therapy
14 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Maintenance ICS & SABA reliever four-stage asthma action plan
Maintenance ICS/LABA & SABA reliever three-stage asthma action plan or maintenance
ICS & SABA reliever three-stage asthma action plan
15 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Adolescents57–59 Education & Employment, Activities,
The recommendations in this guideline Drugs, Sexuality, Suicide/Depression)
apply to people aged 12 and above. Adoles- or holistic psychosocial assessment if
cence is a period of increased risk taking practicable.
and decreased adherence, which may be • Consider simple treatment regimens.
due to forgetfulness, lack of routines, denial, Ensure that the young person is aware
beliefs about asthma or medication, diffi- of what to do if symptoms escalate,
culty using inhalers, fear of side effects and and has someone to contact if they
embarrassment in front of peers. They may have concerns.
be taking on risky activities such as smoking, • Arrange follow-up appointments and
e-cigarettes, vaping or drug taking. Parents/ ensure the adolescent knows how and
caregivers/whānau may play a key role when to instigate appointments.
in reminding and otherwise encouraging
adolescents to take their medication. Asthma in Māori60–66
Māori rights in regard to health,
Adolescents require an approach that
recognised in Te Tiriti of Waitangi and
enables them to take increasing respon-
other national and international decla-
sibility while feeling empowered and
rations, promote Māori participation in
confident to do so. Many adolescents
health-related decision making, as well
report difficulties in communicating with
as equity of health outcomes for all New
their healthcare professional. Ensure that
Zealanders. Currently Māori with asthma
adolescents have a developmentally appro-
are more likely to be hospitalised or die
priate understanding of their asthma and
due to asthma than New Zealand European.
treatment. If they have had asthma for
Despite this, Māori with asthma are less
a long time, it will be necessary to tran-
likely to be prescribed ICS, have an action
sition from the childhood to adult-centric
plan or receive adequate education. Major
approach to care.
barriers to good asthma management which
Practice points may affect Māori include access to and cost
• Prioritise the relationship, offer of care, services and approaches that do not
continuity of care, and emphasise meet their needs, discontinuity and poor
confidentiality. It is important to quality care, lack of culturally appropriate
establish trust and explore barriers to services and health professionals, failure to
access. provide information that is understandable
to the individual, trust and confidence in
• Attempt to instil a sense of control,
the health system. Be mindful of institu-
that adherence will improve the
tional/structural racism (barriers) when
adolescent’s control over their asthma
treating Māori patients. Māori whānau have
and their lives. Consider if a practice
greater exposure to environmental triggers
nurse could play a coaching role.
for asthma, such as smoking and poor
• See adolescents individually first, and
housing. It is recommended that for Māori
then with parents/caregivers as appro-
with asthma:
priate. Ensure they know that as they
• Asthma providers should undertake
transition to adulthood they need to
clinical audit or other similar quali-
take more responsibility for their own
ty-improvement activities to monitor
healthcare and can make appoint-
and improve asthma care and
ments for themselves.
outcomes for Māori. The asthma
• Explain risks of sharing inhalers with
action plan system of care, and the
others (infection, inhaler runs out
anti-inflammatory reliever (AIR)
more quickly).
regimen have been shown to improve
• Ask about smoking, vaping, and drug outcomes in Māori.
taking and advise accordingly.
• A systematic approach to health-lit-
• Assume that the young person is eracy and asthma education for Māori
likely to have other health and social whānau is required. The evidence
issues and questions. Complete a of the health literacy demands,
brief HEADSS (Home & Environment, the barriers and facilitators, and
16 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
steps to delivering excellent asthma • Oral corticosteroids should be
management with Māori that are used as normal when indicated for
described in He maramatanga severe asthma exacerbations during
huango: Asthma health literacy for pregnancy.
Maori children in New Zealand apply • Acute severe asthma in pregnancy is
just as much to adults as they do to a medical emergency and should be
children. treated in hospital.
• Asthma providers should support • Consider early referral for specialist
staff to develop culturally safe skills review in pregnant patients with
for engaging Māori with asthma and poor asthma control or a history of
their whānau in line with professional exacerbations.
requirements. https://www.mcnz.org.
nz/our-standards/current-standards/ Practice point
cultural-safety/ Treatment as usual for asthma in preg-
nancy, and early referral if there is poor
• Māori leadership is required in the
asthma control or a recent exacerbation.
development of asthma management
programmes that improve access Management of acute severe
to asthma care and facilitate ‘wrap asthma (Primary care, afterhours
around’ services to address the wider or ED)10,67–73
determinants (such as housing or • Acute asthma management is based
financial factors) for Māori with on:
asthma.
• objective measurement of
Asthma in Pacific peoples severity (Table 6)
Similar considerations as for Māori are • assessment of the need for
likely to apply to asthma in Pacific peoples referral to hospital and/or
who also have a disproportionate burden hospital admission (Table 7)
of asthma, including high rates of hospital
• administering treatment appro-
admission, and should be considered a
priate for the degree of severity,
high-risk group requiring targeted care.
and
Inclusive in this targeted approach is
addressing risk factors such as poor housing, • repeatedly assessing the response
over-crowding, health literacy, obesity, to treatment.
smoking and poor access to healthcare • Direct measurement of airflow
services. Be mindful of institutional/struc- obstruction is the most objective
tural racism (barriers) when treating Pacific marker of asthma severity. This can
patients. be based on either the measurement
Asthma in pregnancy10 of PEF or preferably FEV1, if available
• Pregnancy can affect the course of at the time of assessment, with both
asthma and women should be advised measures expressed as percent of the
of the importance of maintaining good previous best or predicted reference
asthma control during pregnancy to values.
avoid risk to both mother and baby. • The levels of FEV1 or PEF to signify
• The risks to the baby of poor asthma severe and life-threatening asthma
control and associated exacerbations in these situations, differ from, and
in pregnancy outweigh any theo- are lower than, those used by patients
retical risks associated with asthma in action plans in a non-healthcare
medications. setting.
• ICS, ICS/LABA and SABAs should be • Key priorities include identification
used as normal during pregnancy. of a life-threatening attack requiring
urgent admission to an intensive
• Stopping usual asthma medications
care unit or high dependency unit,
during pregnancy is associated with
and a severe asthma attack requiring
adverse outcomes for both the mother
hospital admission (Table 7).
and her baby.
17 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Table 6: Levels of severity of acute asthma exacerbation.
Mild/moderate asthma • Increasing symptoms
exacerbation: • FEV1 or PEF >50% best or predicted
• No features of acute severe asthma
Acute severe asthma: Any one of:
• FEV1 or PEF 30-50% best or predicted
• Respiratory rate ≥25/min
• Heart rate ≥110/min
• Inability to complete sentences in one breath
Life-threatening asthma: Any one of the following in a patient with severe asthma:
• FEV1 or PEFNZ Adolescent and Adult Asthma Guidelines
For practical purposes, the FEV1 and PEF are considered interchangeable when expressed as % predicted for the
purpose of assessment of acute asthma severity.
• There is insufficient evidence to ventilation in life-threatening asthma,
support the use of intramuscular outside an intensive care unit or high
adrenaline in severe asthma without dependency unit setting, and as a
anaphylaxis, and so intramuscular result it is not recommended in other
adrenaline is not recommended settings.
unless there are signs or clinical • For patients who are treated in
suspicion of anaphylaxis. primary care or discharged from
• Intravenous magnesium sulphate may the afterhours or ED, long-term
be administered in life-threatening management should be reviewed and
asthma. There is no role for intra- an early follow-up appointment with
venous beta-2 agonists, unless inhaled their primary healthcare team should
treatment cannot be given. Simi- be arranged (Table 8).
larly, there is no role for intravenous • All patients not taking ICS should have
aminophylline. an ICS dispensed and appropriate
• There is insufficient evidence to technique taught before going home.
support the use of non-invasive
Table 8: Pre-discharge considerations.
1. Most patients presenting with acute exacerbations of asthma should have a course of oral prednisone, 40mg daily for at least five
days.
2. An acute exacerbation is an opportunity to consider switching patients to AIR therapy with ICS/formoterol as the maintenance and
reliever treatment, as the optimal treatment to reduce the risk of future severe exacerbations.
3. It is recommended that patients have prednisone and ICS dispensed prior to discharge to ensure there are no barriers to taking
medication.
4. Consider referral to a specialist respiratory service.
5. Before the patient goes home, ensure that the patient:
• Can use their inhalers correctly, and has a supply of their medication (including ICS).
• Has a written self-management plan which includes the treatment prescribed, and when to seek further urgent medical review.
• Knows when to contact emergency medical help if worsens.
• Arranges an early follow-up appointment with their primary healthcare team for review.
19 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Appendix: the four-step asthma consultation
1. Assess asthma control 2. Consider other relevant 3. Decide if increase or 4. Complete the asthma action plan
clinical issues decrease in maintenance
therapy required
Complete the Asthma Ask & investigate (eg Is a step up in the level of Decide which plan to use:
Control Test (ACT) score prescribing records) treatment required if asthma is • AIR budesonide/formoterol reliever ±
20–25: well controlled about medication use, not adequately controlled, poor maintenance therapy
16–19: partly controlled including adherence with lung function or recent severe • 3-stage maintenance ICS or ICS/LABA + SABA
5–15: poorly controlled maintenance treatment exacerbation? reliever
• 4-stage maintenance ICS + SABA reliever
Review lung function tests Check inhaler technique Is a change to the AIR regimen [This includes the instruction to increase dose and
Peak flow monitoring and/or required in patients who frequency of ICS in worsening asthma]
Spirometry Enquire about clinical have had a recent severe
features associated with an exacerbation? For those with peak flow instructions, enter personal
Review history of severe increased risk best recent peak flow and peak flow at each level
asthma attacks in last Is a step down in the level of in the plan. The recommended cut points ofNZ Adolescent and Adult Asthma Guidelines
Completing the budesonide/formoterol reliever ± maintenance therapy
(AIR) asthma action plan
Completing the maintenance ICS & SABA reliever four-stage asthma
action plan
21 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Completing the maintenance ICS/LABA & SABA reliever or maintenance
ICS & SABA reliever three-stage asthma action plan
Useful documents/resources/IT support/educational tools/audit tools
section
Health professionals
Asthma control
The Asthma Control Test can be used during a consultation/appointment to standardise
the review of asthma symptoms: http://www.asthmacontrol.co.nz/.
Asthma self-management plans (action plans)
Every person with asthma should have an individualised written asthma plan, which
is updated yearly. The plan should be appropriate for level of treatment, asthma severity,
health literacy, culture and ability to self-manage. There is a range of plans available:
https://www.nzasthmaguidelines.co.nz/resources
Inhaler technique
Correct inhaler technique is central for good asthma control. Incorrect use of an inhaler
may lead to worsening asthma control due to inadequate drug delivery to the airways.
Information and videos on correct inhaler technique can be found here:
https://www.nationalasthma.org.au/living-with-asthma/how-to-videos; https://www.health-
navigator.org.nz/medicines/i/inhaler-devices/?tab=10755#Overview
Dispensing records
Clinicians are encouraged to check pharmacy dispensing records for a patient when
assessing concordance with asthma medication. These records may be available through
primary care, pharmacy or district health board patient records systems.
22 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Audit Tools
Health professionals providing asthma care are encouraged to participate in audit
https://bpac.org.nz/Audits/docs/bpac_audit_asthma_management2017.pdf
https://www.thoracic.org.au/researchawards/new-zealand-national-asthma-audit
Resource for school teachers
The Teachers’ Asthma Toolkit is a free online tool that covers information about asthma,
how asthma affects education, how asthma is treated, common triggers and what to do in an
asthma emergency. The toolbox is interactive, featuring video clips, animations, classroom
resources and child-friendly activities.
https://learnaboutlungs.asthmaandrespiratory.org.nz/
Resources for those who have asthma and their families
Asthma apps
The My Asthma App provides educational information on asthma, signs and symptoms,
triggers, treatment, medication, ACT, helpful contacts and resources. It includes the ability to
include an individualised asthma action plan. This resource was developed by the Asthma
and Respiratory Foundation New Zealand and can be downloaded from: Android: bit.ly/
AsthmaAppAndroid or
Apple: bit.ly/AsthmaAppApple
Websites providing guidelines, educational information and e-learning
course
Online information on asthma is readily available. There are several New Zealand and
Australian websites which provide high-quality information and downloadable resources
on asthma and other conditions which may impact on asthma management. These include:
Asthma and Respiratory Foundation New Zealand https://www.asthmafoundation.org.nz/
https://www.asthmafoundation.org.nz/health-professionals/copd-asthma-fundamentals
Asthma New Zealand https://www.asthma.org.nz/
Allergy New Zealand http://www.allergy.org.nz/
Severe asthma toolkit https://toolkit.severeasthma.org.au/
National Asthma Council Australia https://www.nationalasthma.org.au/
The New Zealand Formulary has information on drugs in sport http://www.nzf.org.nz
Australian Society of Clinical Immunology and Allergy website has a range of information,
action plans, treatment plans, patient handouts and e-learning course for health profes-
sionals https://www.allergy.org.au/
National Institute for Clinical Excellence has a useful patient inhaler
decision aid https://www.nice.org.uk/guidance/ng80/resources/
inhalers-for-asthma-patient-decision-aid-pdf-6727144573
23 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMANZ Adolescent and Adult Asthma Guidelines
Competing interests:
Richard Beasley has received payment for lectures from and been a member of the
AstraZeneca, Avillion, GlaxoSmithKline and Theravance advisory boards, and received
research grants from AstraZeneca, Cephalon, Chiesi, Genentech, GlaxoSmithKline and
Novartis. Lutz Beckert has received payment for lectures and/or advisory boards from
AstraZeneca, GlaxoSmithKline, Novartis, and Boehringer Ingelheim. James Fingleton reports
research grants from AstraZeneca, payment for lectures and non-financial support from
AstraZeneca, research grants from Genentech, payment for lectures and non-financial
support from Boerhinger Ingleheim. Robert Hancox has received payment to his institution
for lectures and/or advisory boards from AstraZeneca, GlaxoSmithKline, and Novartis and
non-financial support from Boehringer Ingelheim. Stuart Jones has received payment for
educational lectures from AstraZeneca and GlaxoSmithKline. Jim Reid is a member of the
GlaxoSmithKline Expert Advisory Committee and has received payment for lectures or
educational activities form GSK, AstraZeneca, and Boehringer Ingelheim. Matire Harwood,
Miriam Hurst, Susan Jones, Betty Poot and Ciléin Kearns have no conflicts to declare.
Author information:
Richard Beasley, Medical Research Institute of New Zealand, Wellington; Capital & Coast
District Health Board, Wellington; Lutz Beckert, University of Otago, Christchurch;
James Fingleton, Medical Research Institute of New Zealand, Wellington; Capital & Coast
District Health Board, Wellington; Robert J Hancox, Waikato District Health Board, Hamilton;
University of Otago, Dunedin; Matire Harwood, University of Auckland, Auckland;
Miriam Hurst, Auckland District Health Board, Auckland; Stuart Jones, Counties-Manukau
Health, Auckland; Susan Jones, Waikato District Health Board, Hamilton;
Ciléin Kearns, Medical Research Institute of New Zealand, Wellington; Capital & Coast
District Health Board, Wellington; David McNamara, Starship Children’s Hospital, Auckland;
Betty Poot, Hutt Valley District Health Board, Lower Hutt; School of Nursing, Midwifery and
Health Practice, Victoria University of Wellington, Wellington; Jim Reid, University of Otago,
Dunedin.
Corresponding author:
Professor Richard Beasley, Medical Research Institute of New Zealand, Private Bag 7902,
Newtown, Wellington 6242.
richard.beasley@mrinz.ac.nz
URL:
XXX
REFERENCES:
1. Asthma and Respiratory 2018 update. Wellington: 6. Lai CKW, et al. Global
Foundation of New Asthma Foundation 2019. variation in the prevalence
Zealand 2015. Te Hā 4. Holt S, Beasley R. The and severity of asthma
Ora (The Breath of Life): Burden of Asthma in symptoms: Phase Three
National Respiratory New Zealand. Asthma & of the International Study
Strategy. Wellington: The Respiratory Foundation of Asthma and Allergies
Asthma Foundation. NZ and Medical Research in Childhood (ISAAC).
2. Jones B, Ingham T. He Institute of New Zealand. Thorax 2009; 64:476–83.
Māramatanga huangō: Auckland: Adis Interna- 7. Masoli M, et al. Global
Asthma health literacy tional Ltd 2002; 48p. Burden of Asthma.
for Māori children in 5. ISAAC Steering Committee. Global Initiative for
New Zealand: Report to Worldwide variation in Asthma (GINA) 2004.
the Ministry of Health. prevalence of symptoms www.ginasthma.com
Wellington: Ministry of asthma, allergic rhino- 8. Beasley R, et al. Asthma and
of Health 2015. conjunctivitis and atopic Respiratory Foundation NZ
3. Telfar Barnard L, et al. eczema: ISAAC. Lancet adult asthma guidelines:
The impact of respiratory 1998; 351:1225–32. A quick reference guide.
disease in New Zealand: NZMJ 2016; 129:83–102.
24 NZMJ 26 June 2020, Vol 133 No 1517
ISSN 1175-8716
www.nzma.org.nz/journal
© NZMAYou can also read