COMPREHENSIVE MEDICAL EVALUATION AND ASSESSMENT OF COMORBIDITIES: STANDARDSOF MEDICALCAREINDIABETESD2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
S40 Diabetes Care Volume 44, Supplement 1, January 2021
4. Comprehensive Medical American Diabetes Association
Evaluation and Assessment of
Comorbidities: Standards of
Medical Care in Diabetesd2021
Diabetes Care 2021;44(Suppl. 1):S40–S52 | https://doi.org/10.2337/dc21-S004
4. MEDICAL EVALUATION AND COMORBIDITIES
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes”
includes the ADA’s current clinical practice recommendations and is intended to
provide the components of diabetes care, general treatment goals and guidelines,
and tools to evaluate quality of care. Members of the ADA Professional Practice
Committee, a multidisciplinary expert committee (https://doi.org/10.2337/dc21-
SPPC), are responsible for updating the Standards of Care annually, or more
frequently as warranted. For a detailed description of ADA standards, statements,
and reports, as well as the evidence grading system for ADA’s clinical practice
recommendations, please refer to the Standards of Care Introduction (https://doi
.org/10.2337/dc21-SINT). Readers who wish to comment on the Standards of Care
are invited to do so at professional.diabetes.org/SOC.
PATIENT-CENTERED COLLABORATIVE CARE
Recommendations
4.1 A patient-centered communication style that uses person-centered and
strength-based language and active listening; elicits patient preferences and
beliefs; and assesses literacy, numeracy, and potential barriers to care
should be used to optimize patient health outcomes and health-related
quality of life. B
4.2 People with diabetes can benefit from a coordinated multidisciplinary team
that may draw from diabetes care and education specialists, primary care
providers, subspecialty providers, nurses, dietitians, exercise specialists,
pharmacists, dentists, podiatrists, and mental health professionals. E
A successful medical evaluation depends on beneficial interactions between the
patient and the care team. The Chronic Care Model (1–3) (see Section 1 “Improving
Suggested citation: American Diabetes Associa-
Care and Promoting Health in Populations,” https://doi.org/10.2337/dc21-S001) is a tion. 4. Comprehensive medical evaluation and
patient-centered approach to care that requires a close working relationship between assessment of comorbidities: Standards of Med-
the patient and clinicians involved in treatment planning. People with diabetes should ical Care in Diabetesd2021. Diabetes Care
receive health care from a coordinated interdisciplinary team that may include 2021;44(Suppl. 1):S40–S52
diabetes care and education specialists, physicians, nurse practitioners, physician © 2020 by the American Diabetes Association.
assistants, nurses, dietitians, exercise specialists, pharmacists, dentists, podiatrists, Readers may use this article as long as the work is
properly cited, the use is educational and not for
and mental health professionals. Individuals with diabetes must assume an active profit, and the work is not altered. More infor-
role in their care. The patient, family or support people, physicians, and health care mation is available at https://www.diabetesjournals
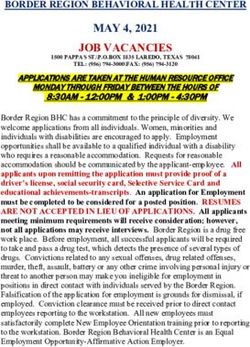
team should together formulate the management plan, which includes lifestyle .org/content/license.care.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S41 management (see Section 5 “Facilitating Provider communication with patients self-management. Empathizing and us- Behavior Change and Well-being to Im- and families should acknowledge that ing active listening techniques, such as prove Health Outcomes,” https://doi.org/ multiple factors impact glycemic man- open-ended questions, reflective state- 10.2337/dc21-S005). agement but also emphasize that collab- ments, and summarizing what the patient The goals of treatment for diabetes are oratively developed treatment plans said, can help facilitate communication. to prevent or delay complications and and a healthy lifestyle can significantly Patients’ perceptions about their own optimize quality of life (Fig. 4.1). Treat- improve disease outcomes and well- ability, or self-efficacy, to self-manage ment goals and plans should be created being (4–7). Thus, the goal of provider- diabetes are one important psychosocial with patients based on their individual patient communication is to establish a factor related to improved diabetes self- preferences, values, and goals. This in- collaborative relationship and to assess management and treatment outcomes in dividualized management plan should and address self-management barriers diabetes (9–13) and should be a target of take into account the patient’s age, cog- without blaming patients for “noncom- ongoing assessment, patient education, nitive abilities, school/work schedule and pliance” or “nonadherence” when the and treatment planning. conditions, health beliefs, support sys- outcomes of self-management are not Language has a strong impact on per- tems, eating patterns, physical activity, optimal (8). The familiar terms “noncom- ceptions and behavior. The use of em- social situation, financial concerns, cultural pliance” and “nonadherence” denote a powering language in diabetes care and factors, literacy and numeracy (mathemat- passive, obedient role for a person with education can help to inform and moti- ical literacy), diabetes history (duration, diabetes in “following doctor’s orders” vate people, yet language that shames complications, current use of medica- that is at odds with the active role people and judges may undermine this effort. tions), comorbidities, health priorities, with diabetes take in directing the day- The American Diabetes Association (ADA) other medical conditions, preferences for to-day decision-making, planning, mon- and the Association of Diabetes Care & care, and life expectancy. Various strate- itoring, evaluation, and problem-solving Education Specialists (formerly called gies and techniques should be used to involved in diabetes self-management. American Association of Diabetes Edu- support patients’ self-management ef- Using a nonjudgmental approach that cators) joint consensus report, “The Use forts, including providing education on normalizes periodic lapses in self-man- of Language in Diabetes Care and Edu- problem-solving skills for all aspects of agement may help minimize patients’ cation,” provides the authors’ expert diabetes management. resistance to reporting problems with opinion regarding the use of language by Figure 4.1—Decision cycle for patient-centered glycemic management in type 2 diabetes. Reprinted from Davies et al. (101).
S42 Comprehensive Medical Evaluation and Assessment of Comorbidities Diabetes Care Volume 44, Supplement 1, January 2021
health care professionals when speaking assessment, management of comorbid Glycemic Treatment,” https://doi.org/10
or writing about diabetes for people with conditions, and engagement of the pa- .2337/dc21-S009), antihypertension med-
diabetes or for professional audiences tient throughout the process. While a ication, and statin treatment intensity.
(14). Although further research is needed comprehensive list is provided in Table Additional referrals should be arranged
to address the impact of language on 4.1, in clinical practice the provider may as necessary (Table 4.4). Clinicians should
diabetes outcomes, the report includes need to prioritize the components of the ensure that individuals with diabetes are
five key consensus recommendations for medical evaluation given the available appropriately screened for complications
language use: resources and time. The goal is to provide and comorbidities. Discussing and imple-
the health care team information so it can menting an approach to glycemic control
c Use language that is neutral, nonjudg- optimally support a patient. In addition to with the patient is a part, not the sole goal,
mental, and based on facts, actions, or themedicalhistory,physical examination, of the patient encounter.
physiology/biology. and laboratory tests, providers should
c Use language free from stigma. assess diabetes self-management be-
IMMUNIZATIONS
c Use language that is strength based, haviors, nutrition, social determinants
respectful, and inclusive and that of health, and psychosocial health (see Recommendation
imparts hope. Section 5 “Facilitating Behavior Change 4.6 Provide routinely recommended
c Use language that fosters collabora- and Well-being to Improve Health Out- vaccinations for childrenand adults
tion between patients and providers. comes,”https://doi.org/10.2337/dc21-S005) with diabetes as indicated by age
c Use language that is person centered and give guidance on routine immuniza- (see Table 4.5 for highly recom-
(e.g., “person with diabetes” is pre- tions. The assessment of sleep pattern mended vaccinations for adults
ferred over “diabetic”). and duration should be considered; a meta- with diabetes). A
analysis found that poor sleep quality,
short sleep, and long sleep were associ- The importance of routine vaccinations
COMPREHENSIVE MEDICAL for people living with diabetes has been
ated with higher A1C in people with
EVALUATION elevated by the coronavirus disease
type 2 diabetes (15). Interval follow-up
Recommendations visits should occur at least every 3– 2019 (COVID-19) pandemic. Preventing
4.3 A complete medical evaluation 6 months individualized to the patient, avoidable infections not only directly
should be performed at the initial and then at least annually. prevents morbidity but also reduces hos-
visit to: Lifestyle management and psychoso- pitalizations, which may additionally re-
c Confirm the diagnosis and classify cial care are the cornerstones of diabetes duce risk of acquiring infections such as
diabetes. A management. Patients should be re- COVID-19. Children and adults with di-
c Evaluate for diabetes complica- ferred for diabetes self-management ed- abetes should receive vaccinations accord-
tions and potential comorbid ucation and support, medical nutrition ing to age-appropriate recommendations
conditions. A therapy, and assessment of psychosocial/ (16,17). The Centers for Disease Control
c Review previous treatment and emotional health concerns if indicated. and Prevention (CDC) provides vaccination
risk factor control in patients with Patients should receive recommended pre- schedules specifically for children, adoles-
established diabetes. A ventive care services (e.g., immunizations, cents, and adults with diabetes (see https://
c Begin patient engagement in the cancer screening, etc.); smoking cessation www.cdc.gov/vaccines/). The CDC Advisory
formulation of a care manage- counseling; and ophthalmological, dental, Committee on Immunization Practices
ment plan. A and podiatric referrals. (ACIP) makes recommendations based on
c Develop a plan for continuing The assessment of risk of acute and its own review and rating of the evidence,
care. A chronic diabetes complications and treat- provided in Table 4.5 for selected vaccina-
4.4 A follow-up visit should include ment planning are key components of tions. The ACIP evidence review has evolved
most components of the initial initial and follow-up visits (Table 4.2). The over time with the adoption of Grading
comprehensive medical evalua- risk of atherosclerotic cardiovascular dis- of Recommendations Assessment, De-
tion (see Table 4.1). A ease and heart failure (see Section 10 velopment and Evaluation (GRADE) in
4.5 Ongoing management should be “Cardiovascular Disease and Risk Man- 2010 and then the Evidence to Decision
guided by the assessment of agement,” https://doi.org/10.2337/dc21- or Evidence to Recommendation (EtR)
overallhealthstatus,diabetescom- S010), chronic kidney disease staging (see frameworks in 2018 (18). Here we dis-
plications, cardiovascular risk (see Section 11 “Microvascular Complications cuss the particular importance of specific
THE RISK CALCULATOR, Section 10 “Car- and Foot Care,” https://doi.org/10.2337/ vaccines.
diovascular Disease and Risk Man- dc21-S011), presence of retinopathy, and
agement,” https://doi.org/10.2337/ risk of treatment-associated hypoglyce- Influenza
dc21-S010),hypoglycemia risk,and mia (Table 4.3) should be used to in- Influenza is a common, preventable in-
shared decision-making to set dividualize targets for glycemia (see fectious disease associated with high
therapeutic goals. B Section 6 “Glycemic Targets,” https:// mortality and morbidity in vulnerable
doi.org/10.2337/dc21-S006), blood pres- populations, including youth, older adults,
The comprehensive medical evaluation in- sure, and lipids and to select specific and people with chronic diseases. Influ-
cludes the initial and follow-up evaluations, glucose-lowering medication (see Sec- enza vaccination in people with diabetes
assessment of complications, psychosocial tion 9 “Pharmacologic Approaches to has been found to significantly reducecare.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S43
Continued on p. S44S44 Comprehensive Medical Evaluation and Assessment of Comorbidities Diabetes Care Volume 44, Supplement 1, January 2021
influenza and diabetes-related hospital conditions such as diabetes are cautioned (21). There are two vaccination types, the
admissions (19). Given the benefits of the against taking the LAIV and are instead 23-valent pneumococcal polysaccharide
annual influenza vaccination, it is recom- recommended to receive the inactive or vaccine (PPSV23) and the 13-valent pneu-
mended for all individuals $6 months recombinant influenza vaccination. For in- mococcal conjugate vaccine (PCV13), with
of age who do not have a contraindica- dividuals $65 years of age, there may be distinct schedules for children and adults.
tion. Influenza vaccination is critically additional benefit from the high-dose quad- All children are recommended to re-
important in the next year as the severe rivalent inactivated influenza vaccine (20). ceive a four-dose series of PCV13 by 15
acute respiratory syndrome coronavirus months of age. For children with diabe-
2 (SARS-CoV-2) and influenza viruses will Pneumococcal Pneumonia tes who have incomplete series by ages
both be active in the U.S. during the Like influenza, pneumococcal pneumo- 2–5 years, the CDC recommends a
2020–2021 season (20). The live atten- nia is a common, preventable disease. catch-up schedule to ensure that these
uated influenza vaccine (LAIV), which is People with diabetes are at increased risk children have four doses. Children with
delivered by nasal spray, is an option for for the bacteremic form of pneumococ- diabetes between 6–18 years of age
patients beginning at age 2 years through cal infection and have been reported to are also advised to receive one dose
age 49 years, for those who are not have a high risk of nosocomial bacter- of PPSV23, preferably after receipt of
pregnant, but patients with chronic emia, with a mortality rate as high as 50% PCV13.care.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S45
Table 4.2—Assessment and treatment plan* that affect people with diabetes and may
Assessing risk of diabetes complications complicate management (24–28). Dia-
c ASCVD and heart failure history betes comorbidities are conditions that
c ASCVD risk factors and 10-year ASCVD risk assessment affect people with diabetes more often
c Staging of chronic kidney disease (see Table 11.1) than age-matched people without dia-
c Hypoglycemia risk (see Table 4.3)
betes. This section discusses many of the
Goal setting common comorbidities observed in pa-
c Set A1C/blood glucose target
tients with diabetes but is not necessarily
c If hypertension is present, establish blood pressure target
c Diabetes self-management goals
inclusive of all the conditions that have
Therapeutic treatment plans
been reported.
c Lifestyle management
c Pharmacologic therapy: glucose lowering Autoimmune Diseases
c Pharmacologic therapy: cardiovascular disease risk factors and renal
c Use of glucose monitoring and insulin delivery devices Recommendations
c Referral to diabetes education and medical specialists (as needed) 4.7 Patients with type 1 diabetes
ASCVD, atherosclerotic cardiovascular disease. *Assessment and treatment planning are essential should be screened for autoim-
components of initial and all follow-up visits. mune thyroid disease soon after
diagnosis and periodically there-
after. B
4.8 Adult patients with type 1 diabe-
For adults with diabetes, one dose of blood or through improper equipment tes should be screened for celiac
PPSV23 is recommended between the use (glucose monitoring devices or in- disease in the presence of gas-
ages of 19–64 years and another dose fected needles). Because of the higher trointestinal symptoms, signs, or
at $65 years of age. The PCV13 is no likelihood of transmission, hepatitis B laboratory manifestations sugges-
longer routinely recommended for pa- vaccine is recommended for adults with tive of celiac disease. B
tients over 65 years of age because of diabetes aged ,60 years. For adults aged
the declining rates of pneumonia due to $60 years, hepatitis B vaccine may be People with type 1 diabetes are at in-
these strains (22). Older patients should administered at the discretion of the creased risk for other autoimmune
have a shared decision-making discus- treating clinician based on the patient’s diseases, with thyroid disease, celiac
sion with their provider to determine likelihood of acquiring hepatitis B infection. disease, and pernicious anemia (vitamin
individualized risks and benefits. PCV13 B12 deficiency) being among the most
is recommended for patients with immu- COVID-19 common (29). Other associated condi-
nocompromising conditions such as as- During the coming year, it is expected tions include autoimmune hepatitis, pri-
plenia, advanced kidney disease, cochlear that vaccines for COVID-19 will become mary adrenal insufficiency (Addison
implants, or cerebrospinal fluid leaks (23). available and that people with diabe- disease), dermatomyositis, and myasthe-
Some older patients residing in assisted tes should be a priority population. The nia gravis (30–33). Type 1 diabetes may
living facilities may also consider PCV13. If COVID-19 vaccine will likely become a also occur with other autoimmune dis-
the PCV13 is to be administered, it should routine part of the annual preventive eases in the context of specific genetic
be given prior to the next dose of PPSV23. schedule for people with diabetes. disorders or polyglandular autoimmune
syndromes (34). Given the high preva-
Hepatitis B lence, nonspecific symptoms, and insid-
Compared with the general population, ASSESSMENT OF COMORBIDITIES
ious onset of primary hypothyroidism,
people with type 1 or type 2 diabetes Besides assessing diabetes-related compli- routine screening for thyroid dysfunc-
have higher rates of hepatitis B. This cations, clinicians and their patients need tion is recommended for all patients with
may be due to contact with infected to be aware of common comorbidities type 1 diabetes. Screening for celiac dis-
ease should be considered in adult pa-
tients with suggestive symptoms (e.g.,
Table 4.3—Assessment of hypoglycemia risk diarrhea, malabsorption, abdominal pain)
Factors that increase risk of treatment-associated hypoglycemia or signs (e.g., osteoporosis, vitamin de-
c Use of insulin or insulin secretagogues (i.e., sulfonylureas, meglitinides)
ficiencies, iron deficiency anemia) (35,36).
c Impaired kidney or hepatic function
c Longer duration of diabetes
Measurement of vitamin B12 levels should
c Frailty and older age
be considered for patients with type 1
c Cognitive impairment diabetes and peripheral neuropathy or
c Impaired counterregulatory response, hypoglycemia unawareness unexplained anemia.
c Physical or intellectual disability that may impair behavioral response to hypoglycemia
c Alcohol use
c Polypharmacy (especially ACE inhibitors, angiotensin receptor blockers, nonselective Cancer
b-blockers) Diabetes is associated with increased risk
In addition to individual risk factors, consider use of comprehensive risk prediction models (102). of cancers of the liver, pancreas, endo-
metrium, colon/rectum, breast, and blad-
See references 103–107.
der (37). The association may result fromS46 Comprehensive Medical Evaluation and Assessment of Comorbidities Diabetes Care Volume 44, Supplement 1, January 2021
Nutrition
Table 4.4—Referrals for initial care management
c Eye care professional for annual dilated eye exam
In one study, adherence to the Mediter-
c Family planning for women of reproductive age
ranean diet correlated with improved
c Registered dietitian nutritionist for medical nutrition therapy
cognitive function (48). However, a re-
c Diabetes self-management education and support cent Cochrane review found insufficient
c Dentist for comprehensive dental and periodontal examination evidence to recommend any specific di-
c Mental health professional, if indicated etary change for the prevention or treat-
c Audiology, if indicated ment of cognitive dysfunction (49).
Statins
A systematic review has reported that
shared risk factors between type 2 di- all-cause dementia, Alzheimer dementia, data do not support an adverse effect of
abetes and cancer (older age, obesity, and vascular dementia compared with statins on cognition (50). The U.S. Food
and physical inactivity) but may also be rates in those with normal glucose tol- and Drug Administration postmarketing
due to diabetes-related factors (38), such erance (43). See Section 12 “Older surveillance databases have also revealed
as underlying disease physiology or di- Adults” (https://doi.org/10.2337/dc21-S012) a low reporting rate for cognitive-related
abetes treatments, although evidence for a more detailed discussion regarding adverse events, including cognitive dys-
for these links is scarce. Patients with di- screening for cognitive impairment. function or dementia, with statin ther-
abetes should be encouraged to undergo apy, similar to rates seen with other
recommended age- and sex-appropriate commonly prescribed cardiovascular med-
cancer screenings and to reduce their Hyperglycemia ications (50). Therefore, fear of cognitive
modifiable cancer risk factors (obesity, In those with type 2 diabetes, the degree decline should not be a barrier to statin
physical inactivity, and smoking). New and duration of hyperglycemia are re- use in individuals with diabetes and a
onset of atypical diabetes (lean body lated to dementia. More rapid cognitive high risk for cardiovascular disease.
habitus, negative family history) in a decline is associated with both increased
middle-aged or older patient may pre- A1C and longer duration of diabetes (42).
The Action to Control Cardiovascular Risk Nonalcoholic Fatty Liver Disease
cede the diagnosis of pancreatic adeno-
carcinoma (39). However, in the absence in Diabetes (ACCORD) study found that Recommendation
of other symptoms (e.g., weight loss, each 1% higher A1C level was associated 4.10 Patients with type 2 diabetes or
abdominal pain), routine screening of all with lower cognitive function in individ- prediabetes and elevated liver
such patients is not currently recommended. uals with type 2 diabetes (44). However, enzymes (ALT) or fatty liver on
the ACCORD study found no difference in ultrasound should be evaluated
cognitive outcomes in participants ran- for presence of nonalcoholic stea-
Cognitive Impairment/Dementia domly assigned to intensive and standard tohepatitis and liver fibrosis. C
Recommendation glycemic control, supporting the recom-
4.9 In the presence of cognitive im- mendation that intensive glucose control Diabetes is associated with the develop-
pairment, diabetes treatment should not be advised for the improve- ment of nonalcoholic fatty liver disease,
regimens should be simplified ment of cognitive function in individuals including its more severe manifestations
as much as possible and tailored with type 2 diabetes (45). of nonalcoholic steatohepatitis, liver fibro-
to minimize the risk of hypogly- sis, cirrhosis, and hepatocellular carcinoma
cemia. B Hypoglycemia (51). Elevations of hepatic transaminase
In type 2 diabetes, severe hypoglycemia is concentrations are associated with higher
Diabetes is associated with a significantly associated with reduced cognitive func- BMI, waist circumference, and triglyceride
increased risk and rate of cognitive de- tion, and those with poor cognitive func- levels and lower HDL cholesterol levels.
cline and an increased risk of dementia tion have more severe hypoglycemia. In a Noninvasive tests, such as elastography
(40,41). A recent meta-analysis of pro- long-term study of older patients with or fibrosis biomarkers, may be used to
spective observational studies in people type 2 diabetes, individuals with one or assess risk of fibrosis, but referral to a
with diabetes showed 73% increased risk more recorded episodes of severe hypo- liver specialist and liver biopsy may
of all types of dementia, 56% increased glycemia had a stepwise increase in risk be required for definitive diagnosis
risk of Alzheimer dementia, and 127% of dementia (46). Likewise, the ACCORD (52). Interventions that improve meta-
increased risk of vascular dementia com- trial found that as cognitive function bolic abnormalities in patients with di-
pared with individuals without diabetes decreased, the risk of severe hypoglyce- abetes (weight loss, glycemic control,
(42). The reverse is also true: people with mia increased (47). Tailoring glycemic and treatment with specific drugs for hy-
Alzheimer dementia are more likely to therapy may help to prevent hypoglyce- perglycemia or dyslipidemia) are also
develop diabetes than people without mia in individuals with cognitive dys- beneficial for fatty liver disease (53,54).
Alzheimer dementia. In a 15-year pro- function. See Section 12 “Older Adults” Pioglitazone, vitamin E treatment, and
spective study of community-dwelling (https://doi.org/10.2337/dc21-S012) for liraglutide treatment of biopsy-proven
people .60 years of age, the presence of more detailed discussion of hypoglyce- nonalcoholic steatohepatitis have each
diabetes at baseline significantly increased mia in older patients with type 1 and been shown to improve liver histol-
the age- and sex-adjusted incidence of type 2 diabetes. ogy, but effects on longer-term clinicalcare.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S47
Table 4.5—Highly recommended immunizations for adult patients with diabetes (Advisory Committee on Immunization
Practices, Centers for Disease Control and Prevention)
GRADE evidence
Vaccination Age-group recommendations Frequency type* Reference
Hepatitis B ,60 years of age; $60 years Two- or three-dose 2 Centers for Disease Control
of age discuss with doctor series and Prevention (CDC). Use
of hepatitis B vaccination
for adults with diabetes
mellitus: recommendations
of the Advisory Committee
on Immunization Practices
(ACIP). MMWR 2011;60:
1709–1711
Human papilloma virus #26 years of age; 27–45 years Three doses over 2 for females, Meites E, Szilagyi PG, Chesson
(HPV) of age may also be 6 months 3 for males HW, Unger ER, Romero JR,
vaccinated against HPV after Markowitz LE. Human
a discussion with their health papillomavirus vaccination
care provider for adults: updated
recommendations of the
Advisory Committee on
Immunization Practices.
MMWR 2019;68:698–702
Influenza All patients; advised not to Annual – Demicheli V, Jefferson T, Di
receive live attenuated Pietrantonj C, Ferroni E,
influenza vaccine Thorning S, Thomas RE,
Rivetti A. Vaccines for
preventing influenza in the
elderly. Cochrane Database
Syst Rev 2018;2:CD004876
Pneumonia (PPSV23 19–64 years of age, vaccinate One dose 2 CDC. Updated recommendations
[Pneumovax]) with Pneumovax for prevention of invasive
pneumococcal disease
among adults using the
23-valent pneumococcal
polysaccaride vaccine
(PPSV23). MMWR
2010;59:1102–1106
$65 years of age, obtain One dose; if PCV13 has been 2 Falkenhorst G, Remschmidt C,
second dose of Pneumovax, given, then give PPSV23 $1 Harder T, Hummers-Pradier
at least 5 years from prior year after PCV13 and $5 E, Wichmann O, Bogdan C.
Pneumovax vaccine years after any PPSV23 at Effectiveness of the
age ,65 years 23-valent pneumococcal
polysaccharide vaccine
(PPV23) against
pneumococcal disease in
the elderly: systematic
review and meta-analysis.
PLoS ONE 2017;12:e0169368
Pneumonia 19–64 years of age, no None
(PCV13 recommendation
[Prevnar]) $65 years of age, without an One dose 3 Matanock A, Lee G, Gierke R,
immunocompromising condition Kobayashi M, Leidner A,
(e.g., chronic renal failure), Pilishvili T. Use of 13-valent
cochlear implant, or cerebrospinal pneumococcal conjugate
fluid leak, have shared decision- vaccine and 23-valent
making discussion with doctor pneumococcal polysac-
charide vaccine among
adults aged $65 years:
updated recommendations
of the Advisory Committee
on Immunization Practices.
MMWR 2019;68:1069–1075
Continued on p. S48S48 Comprehensive Medical Evaluation and Assessment of Comorbidities Diabetes Care Volume 44, Supplement 1, January 2021
Table 4.5—Continued
GRADE evidence
Vaccination Age-group recommendations Frequency type* Reference
Tetanus, diphtheria, All adults; pregnant women Booster every 10 years 2 for Havers FP, Moro PL, Hunter P,
pertussis (TDAP) should have an extra dose effectiveness, Hariri S, Bernstein H. Use of
3 for safety tetanus toxoid, reduced
diphtheria toxoid, and
acellular pertussis vaccines:
updated recommendations
of the Advisory Committee
on Immunization
PracticesdUnited States,
2019. MMWR 2020;69:
77–83
Zoster $50 years of age Two-dose Shingrix, even if 1 Dooling KL, Guo A, Patel M,
previously vaccinated et al. Recommendations of
the Advisory Committee on
Immunization Practices for
use of herpes zoster
vaccines. MMWR
2018;67:103–108
GRADE, Grading of Recommendations Assessment, Development and Evaluation; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23,
23-valent pneumococcal polysaccharide vaccine. *Evidence type: 1 5 randomized controlled trials (RCTs), or overwhelming evidence from
observational studies; 2 5 RCTs with important limitations, or exceptionally strong evidence from observational studies; 3 5 observational studies, or
RCTs with notable limitations; and 4 5 clinical experience and observations, observational studies with important limitations, or RCTs with several major
limitations. For a comprehensive list, refer to the Centers for Disease Control and Prevention at https://www.cdc.gov/vaccines/.
outcomes are not known (55–57). which may disrupt the global architecture disease factors should be carefully con-
Treatment with other glucagon-like or physiology of the pancreas, often sidered when deciding the indications
peptide 1 receptor agonists and with resulting in both exocrine and endocrine and timing of this surgery. Surgeries
sodium–glucose cotransporter 2 inhib- dysfunction. Up to half of patients with should be performed in skilled facilities
itors has shown promise in preliminary diabetes may have some degree of im- that have demonstrated expertise in islet
studies, although benefits may be me- paired exocrine pancreas function (63). autotransplantation.
diated, at least in part, by weight loss People with diabetes are at an approx-
(57–59). imately twofold higher risk of developing Fractures
acute pancreatitis (64). Age-specific hip fracture risk is signifi-
Hepatitis C Infection Conversely, prediabetes and/or diabe- cantly increased in both people with
Infection with hepatitis C virus (HCV) is tes has been found to develop in ap- type 1 diabetes (relative risk 6.3) and
associated with a higher prevalence of proximately one-third of patients after those with type 2 diabetes (relative risk
type 2 diabetes, which is present in up an episode of acute pancreatitis (65); 1.7) in both sexes (75). Type 1 diabetes
to one-third of individuals with chronic thus, the relationship is likely bidirec- is associated with osteoporosis, but in
HCV infection. HCV may impair glucose tional. Postpancreatitis diabetes may in- type 2 diabetes, an increased risk of hip
metabolism by several mechanisms, in- clude either new-onset disease or previously fracture is seen despite higher bone
cluding directly via viral proteins and unrecognized diabetes (66). Studies of mineral density (BMD) (76). In three large
indirectly by altering proinflammatory patients treated with incretin-based ther- observational studies of older adults,
cytokine levels (60). The use of newer apies for diabetes have also reported that femoral neck BMD T-score and the World
direct-acting antiviral drugs produces a pancreatitis may occur more frequently Health Organization Fracture Risk Assess-
sustained virological response (cure) with these medications, but results have ment Tool (FRAX) score were associated
in nearly all cases and has been re- been mixed and causality has not been with hip and nonspine fractures. Fracture
ported to improve glucose metabo- established (67–69). risk was higher in participants with di-
lism in individuals with diabetes (61). Islet autotransplantation should be abetes compared with those without
A meta-analysis of mostly observa- considered for patients requiring total diabetes for a given T-score and age or
tional studies found a mean reduction pancreatectomy for medically refractory for a given FRAX score (77). Providers
in A1C levels of 0.45% (95% CI 20.60 chronic pancreatitis to prevent postsur- should assess fracture history and risk
to 20.30) and reduced requirement gical diabetes. Approximately one-third factors in older patients with diabetes
for glucose-lowering medication use of patients undergoing total pancreatec- and recommend measurement of BMD if
following successful eradication of tomy with islet autotransplantation are appropriate for the patient’s age and sex.
HCV infection (62). insulin free 1 year postoperatively, and Fracture prevention strategies for people
observational studies from different cen- with diabetes are the same as for the
Pancreatitis ters have demonstrated islet graft func- general population and may include vi-
Diabetes is linked to diseases of the tion up to a decade after the surgery in tamin D supplementation. For patients
exocrine pancreas such as pancreatitis, some patients (70–74). Both patient and with type 2 diabetes with fracture riskcare.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S49
factors, thiazolidinediones (78) and sodium– signs of low testosterone (hypogonad- Current evidence suggests that peri-
glucose cotransporter 2 inhibitors (79) ism), a morning total testosterone level odontal disease adversely affects diabe-
should be used with caution. should be measured using an accurate tes outcomes, although evidence for
and reliable assay (89). In men who treatment benefits remains controversial
Sensory Impairment have total testosterone levels close to (28,99). In a randomized clinical trial, in-
Hearing impairment, both in high-frequency the lower limit, it is reasonable to de- tensive periodontal treatment was associ-
and low- to midfrequency ranges, is termine free testosterone concentra- ated with better glycemic control (A1C
more common in people with diabetes tions either directly from equilibrium 8.3% vs. 7.8% in control subjects and the
than in those without, with stronger dialysis assays or by calculations that intensive-treatment group, respectively)
associations found in studies of younger use total testosterone, sex hormone and reduction in inflammatory markers
people (80). Proposed pathophysiologic binding globulin, and albumin concen- after 12 months of follow-up (100).
mechanisms include the combined con- trations (89). Please see the Endocrine
tributions of hyperglycemia and oxida- Society Clinical Practice Guideline for References
tive stress to cochlear microangiopathy detailed recommendations (89). Further 1. Stellefson M, Dipnarine K, Stopka C. The
chronic care model and diabetes management
and auditory neuropathy (81). In a Na- tests (such as luteinizing hormone and
in US primary care settings: a systematic review.
tional Health and Nutrition Examination follicle-stimulating hormone levels) may Prev Chronic Dis 2013;10:E26
Survey (NHANES) analysis, hearing im- be needed to determine if the patient 2. Coleman K, Austin BT, Brach C, Wagner EH.
pairment was about twice as prevalent has hypogonadism. Testosterone replace- Evidence on the Chronic Care Model in the new
in people with diabetes compared with ment in older men with hypogonadism millennium. Health Aff (Millwood) 2009;28:75–85
has been associated with increased 3. Gabbay RA, Bailit MH, Mauger DT, Wagner EH,
those without, after adjusting for age and Siminerio L. Multipayer patient-centered medical
other risk factors for hearing impairment coronary artery plaque volume, with no home implementation guided by the chronic care
(82). Low HDL cholesterol, coronary heart conclusive evidence that testosterone model. Jt Comm J Qual Patient Saf 2011;37:265–273
disease, peripheral neuropathy, and gen- supplementation is associated with in- 4. UK Prospective Diabetes Study (UKPDS)
eral poor health have been reported as creased cardiovascular risk in hypogona- Group. Intensive blood-glucose control with
dal men (89). sulphonylureas or insulin compared with con-
risk factors for hearing impairment for
ventional treatment and risk of complications in
people with diabetes, but an association patients with type 2 diabetes (UKPDS 33). Lancet
of hearing loss with blood glucose levels 1998;352:837–853
has not been consistently observed (83). Obstructive Sleep Apnea 5. Nathan DM, Genuth S, Lachin J, et al.; Diabetes
In the Diabetes Control and Complications Age-adjusted rates of obstructive sleep Control and Complications Trial Research Group.
Trial/ Epidemiology of Diabetes Interven- apnea, a risk factor for cardiovascular The effect of intensive treatment of diabetes on
disease, are significantly higher (4- to the development and progression of long-term
tions and Complications (DCCT/EDIC) complications in insulin-dependent diabetes
cohort, time-weighted mean A1C was 10-fold) with obesity, especially with
mellitus. N Engl J Med 1993;329:977–986
associated with increased risk of hear- central obesity (90). The prevalence of 6. Lachin JM, Genuth S, Nathan DM, Zinman B,
ing impairment when tested after long- obstructive sleep apnea in the popula- Rutledge BN; DCCT/EDIC Research Group. Effect
term (.20 years) follow-up (84). Impair- tion with type 2 diabetes may be as high of glycemic exposure on the risk of microvascular
as 23%, and the prevalence of any sleep- complications in the Diabetes Control and Com-
ment in smell, but not taste, has also plications Trialdrevisited. Diabetes 2008;57:995–
been reported in individuals with di- disordered breathing may be as high as
1001
abetes (85). 58% (91,92). In obese participants en- 7. White NH, Cleary PA, Dahms W, Goldstein D,
rolled in the Action for Health in Diabetes Malone J, Tamborlane WV; Diabetes Control and
(Look AHEAD) trial, it exceeded 80% (93). Complications Trial (DCCT)/Epidemiology of Di-
Low Testosterone in Men Patients with symptoms suggestive of abetes Interventions and Complications (EDIC)
obstructive sleep apnea (e.g., excessive Research Group. Beneficial effects of intensive
Recommendation therapy of diabetes during adolescence: out-
4.11 In men with diabetes who have daytime sleepiness, snoring, witnessed
comes after the conclusion of the Diabetes
symptoms or signs of hypogo- apnea) should be considered for screen- Control and Complications Trial (DCCT). J Pediatr
nadism, such as decreased sex- ing (94). Sleep apnea treatment (lifestyle 2001;139:804–812
ual desire (libido) or activity, or modification, continuous positive airway 8. Anderson RM, Funnell MM. Compliance and
pressure, oral appliances, and surgery) adherence are dysfunctional concepts in diabe-
erectile dysfunction, consider tes care. Diabetes Educ 2000;26:597–604
screening with a morning se- significantly improves quality of life and
9. Sarkar U, Fisher L, Schillinger D. Is self-efficacy
rum testosterone level. B blood pressure control. The evidence associated with diabetes self-management across
for a treatment effect on glycemic con- race/ethnicity and health literacy? Diabetes Care
Mean levels of testosterone are lower in trol is mixed (95). 2006;29:823–829
10. King DK, Glasgow RE, Toobert DJ, et al. Self-
men with diabetes compared with age-
efficacy, problem solving, and social-environmental
matched men without diabetes, but Periodontal Disease support are associated with diabetes self-
obesity is a major confounder (86,87). Periodontal disease is more severe, and management behaviors. Diabetes Care 2010;33:
Testosterone replacement in men with may be more prevalent, in patients with 751–753
symptomatic hypogonadism may have diabetes than in those without and has 11. Nouwen A, Urquhart Law G, Hussain S,
McGovern S, Napier H. Comparison of the
benefits including improved sexual been associated with higher A1C levels
role of self-efficacy and illness representations
function, well-being, muscle mass and (96–98). Longitudinal studies suggest in relation to dietary self-care and diabetes
strength, and bone density (88). In men that people with periodontal disease distress in adolescents with type 1 diabetes.
with diabetes who have symptoms or have higher rates of incident diabetes. Psychol Health 2009;24:1071–1084S50 Comprehensive Medical Evaluation and Assessment of Comorbidities Diabetes Care Volume 44, Supplement 1, January 2021
12. Beckerle CM, Lavin MA. Association of self- 26. Tinetti ME, Fried TR, Boyd CM. Design- 43. Ohara T, Doi Y, Ninomiya T, et al. Glucose
efficacy and self-care with glycemic control in ing health care for the most common chronic tolerance status and risk of dementia in the
diabetes. Diabetes Spectr 2013;26:172–178 conditiondmultimorbidity. JAMA 2012;307:2493– community: the Hisayama study. Neurology
13. Iannotti RJ, Schneider S, Nansel TR, et al. Self- 2494 2011;77:1126–1134
efficacy, outcome expectations, and diabetes 27. Sudore RL, Karter AJ, Huang ES, et al. Symp- 44. Cukierman-Yaffe T, Gerstein HC, Williamson
self-management in adolescents with type 1 tom burden of adults with type 2 diabetes across JD, et al.; Action to Control Cardiovascular Risk in
diabetes. J Dev Behav Pediatr 2006;27:98–105 the disease course: Diabetes & Aging Study. Diabetes-Memory in Diabetes (ACCORD-MIND)
14. Dickinson JK, Guzman SJ, Maryniuk MD, et al. J Gen Intern Med 2012;27:1674–1681 Investigators. Relationship between baseline
The use of language in diabetes care and edu- 28. Borgnakke WS, Ylöstalo PV, Taylor GW, glycemic control and cognitive function in individ-
cation. Diabetes Care 2017;40:1790–1799 Genco RJ. Effect of periodontal disease on di- uals with type 2 diabetes and other cardiovascular
15. Lee SWH, Ng KY, Chin WK. The impact of abetes: systematic review of epidemiologic ob- risk factors: the Action to Control Cardiovascular
sleep amount and sleep quality on glycemic servational evidence. J Periodontol 2013; Risk in Diabetes-Memory in Diabetes (ACCORD-
control in type 2 diabetes: a systematic review 84(Suppl.):S135–S152 MIND) trial. Diabetes Care 2009;32:221–226
and meta-analysis. Sleep Med Rev 2017;31:91– 29. Nederstigt C, Uitbeijerse BS, Janssen LGM, 45. Launer LJ, Miller ME, Williamson JD, et al.;
101 Corssmit EPM, de Koning EJP, Dekkers OM. ACCORD MIND investigators. Effects of intensive
16. Robinson CL, Bernstein H, Poehling K, Associated auto-immune disease in type 1 di- glucose lowering on brain structure and function
Romero JR, Szilagyi P. Advisory Committee on abetes patients: a systematic review and meta- in people with type 2 diabetes (ACCORD MIND):
Immunization Practices recommended immuni- analysis. Eur J Endocrinol 2019;180:135–144 a randomised open-label substudy. Lancet Neu-
zation schedule for children and adolescents 30. De Block CE, De Leeuw IH, Van Gaal LF. High rol 2011;10:969–977
aged 18 years or younger - United States, prevalence of manifestations of gastric autoim- 46. Whitmer RA, Karter AJ, Yaffe K, Quesenberry
2020. MMWR Morb Mortal Wkly Rep 2020; munity in parietal cell antibody-positive type 1 CP Jr, Selby JV. Hypoglycemic episodes and risk of
69:130–132 (insulin-dependent) diabetic patients. The Bel- dementia in older patients with type 2 diabetes
17. Freedman MS, Hunter P, Ault K, Kroger A. gian Diabetes Registry. J Clin Endocrinol Metab mellitus. JAMA 2009;301:1565–1572
Advisory Committee on Immunization Practices 1999;84:4062–4067 47. Punthakee Z, Miller ME, Launer LJ, et al.;
recommended immunization schedule for adults 31. Triolo TM, Armstrong TK, McFann K, et al. ACCORD Group of Investigators; ACCORD-MIND
aged 19 years or older - United States, 2020. Additional autoimmune disease found in 33% of Investigators. Poor cognitive function and risk of
MMWR Morb Mortal Wkly Rep 2020;69:133– patients at type 1 diabetes onset. Diabetes Care severe hypoglycemia in type 2 diabetes: post hoc
135 2011;34:1211–1213 epidemiologic analysis of the ACCORD trial. Di-
18. Lee G, Carr W; ACIP Evidence-Based Rec- 32. Hughes JW, Riddlesworth TD, DiMeglio LA,
abetes Care 2012;35:787–793
ommendations Work Group; ACIP Evidence Miller KM, Rickels MR, McGill JB; T1D Exchange
48. Scarmeas N, Stern Y, Mayeux R, Manly JJ,
Based Recommendations Work Group. Updated Clinic Network. Autoimmune diseases in children
Schupf N, Luchsinger JA. Mediterranean diet and
framework for development of evidence-based and adults with type 1 diabetes from the T1D
mild cognitive impairment. Arch Neurol 2009;66:
recommendations by the Advisory Committee on Exchange Clinic Registry. J Clin Endocrinol Metab
216–225
Immunization Practices. MMWR Morb Mortal 2016;101:4931–4937
49. Ooi CP, Loke SC, Yassin Z, Hamid T-A. Car-
Wkly Rep 2018;67:1271–1272 33. Kahaly GJ, Hansen MP. Type 1 diabetes
bohydrates for improving the cognitive perfor-
19. Goeijenbier M, van Sloten TT, Slobbe L, et al. associated autoimmunity. Autoimmun Rev 2016;
mance of independent-living older adults with
Benefits of flu vaccination for persons with 15:644–648
normal cognition or mild cognitive impairment.
diabetes mellitus: a review. Vaccine 2017;35: 34. Eisenbarth GS, Gottlieb PA. Autoimmune
Cochrane Database Syst Rev 2011;4:CD007220
5095–5101 polyendocrine syndromes. N Engl J Med 2004;
50. Richardson K, Schoen M, French B, et al.
20. Grohskopf LA, Alyanak E, Broder KR, Blanton 350:2068–2079
LH, Fry AM, Jernigan DB, et al. Prevention and Statins and cognitive function: a systematic re-
35. Rubio-Tapia A, Hill ID, Kelly CP, Calderwood
control of seasonal influenza with vaccines: AH, Murray JA; American College of Gastroen- view. Ann Intern Med 2013;159:688–697
recommendations of the Advisory Committee terology. ACG clinical guidelines: diagnosis and 51. El-Serag HB, Tran T, Everhart JE. Diabetes
on Immunization Practices - United States, 2020- management of celiac disease. Am J Gastro- increases the risk of chronic liver disease and
21 influenza season. MMWR Recomm Rep 2020; enterol 2013;108:656–676; quiz 677 hepatocellular carcinoma. Gastroenterology 2004;
69:1–24 36. Husby S, Murray JA, Katzka DA. AGA clinical 126:460–468
21. Smith SA, Poland GA. Use of influenza and practice update on diagnosis and monitoring of 52. Chalasani N, Younossi Z, Lavine JE, et al. The
pneumococcal vaccines in people with diabetes. celiac disease-changing utility of serology and diagnosis and management of nonalcoholic fatty
Diabetes Care 2000;23:95–108 histologic measures: expert review. Gastroen- liver disease: practice guidance from the Amer-
22. Matanock A, Lee G, Gierke R, Kobayashi M, terology 2019;156:885–889 ican Association for the Study of Liver Diseases.
Leidner A, Pilishvili T. Use of 13-valent pneumo- 37. Suh S, Kim K-W. Diabetes and cancer: is Hepatology 2018;67:328–357
coccal conjugate vaccine and 23-valent pneu- diabetes causally related to cancer? Diabetes 53. American Gastroenterological Association.
mococcal polysaccharide vaccine among adults Metab J 2011;35:193–198 American Gastroenterological Association med-
aged $65 years: updated recommendations of 38. Giovannucci E, Harlan DM, Archer MC, et al. ical position statement: nonalcoholic fatty liver
the Advisory Committee on Immunization Prac- Diabetes and cancer: a consensus report. CA disease. Gastroenterology 2002;123:1702–1704
tices. MMWR Morb Mortal Wkly Rep 2019;68: Cancer J Clin 2010;60:207–221 54. Cusi K, Orsak B, Bril F, et al. Long-term
1069–1075 39. Aggarwal G, Kamada P, Chari ST. Prevalence pioglitazone treatment for patients with non-
23. Ahmed SS, Pondo T, Xing W, et al. Early of diabetes mellitus in pancreatic cancer com- alcoholic steatohepatitis and prediabetes or
impact of 13-valent pneumococcal conjugate pared to common cancers. Pancreas 2013;42: type 2 diabetes mellitus: a randomized trial.
vaccine use on invasive pneumococcal disease 198–201 Ann Intern Med 2016;165:305–315
among adults with and without underlying med- 40. Cukierman T, Gerstein HC, Williamson JD. 55. Belfort R, Harrison SA, Brown K, et al. A
ical conditionsdUnited States. Clin Infect Dis Cognitive decline and dementia in diabetes– placebo-controlled trial of pioglitazone in sub-
2020;70:2484–2492 systematic overview of prospective observa- jects with nonalcoholic steatohepatitis. N Engl J
24. Selvin E, Coresh J, Brancati FL. The burden tional studies. Diabetologia 2005;48:2460–2469 Med 2006;355:2297–2307
and treatment of diabetes in elderly individuals in 41. Biessels GJ, Staekenborg S, Brunner E, 56. Sanyal AJ, Chalasani N, Kowdley KV, et al.;
the U.S. Diabetes Care 2006;29:2415–2419 Brayne C, Scheltens P. Risk of dementia in di- NASH CRN. Pioglitazone, vitamin E, or placebo for
25. Grant RW, Ashburner JM, Hong CS, Chang Y, abetes mellitus: a systematic review. Lancet nonalcoholic steatohepatitis. N Engl J Med 2010;
Barry MJ, Atlas SJ. Defining patient complexity Neurol 2006;5:64–74 362:1675–1685
from the primary care physician’s perspective: 42. Gudala K, Bansal D, Schifano F, Bhansali A. 57. Armstrong MJ, Gaunt P, Aithal GP, et al.;
a cohort study [published correction appears in Diabetes mellitus and risk of dementia: a meta- LEAN trial team. Liraglutide safety and efficacy in
Ann Intern Med 2012;157:152]. Ann Intern Med analysis of prospective observational studies. J patients with non-alcoholic steatohepatitis
2011;155:797–804 Diabetes Investig 2013;4:640–650 (LEAN): a multicentre, double-blind, randomised,care.diabetesjournals.org Comprehensive Medical Evaluation and Assessment of Comorbidities S51
placebo-controlled phase 2 study. Lancet 2016; a long-term assessment of graft function. Pan- guideline. J Clin Endocrinol Metab 2010;95:
387:679–690 creas 2008;37:282–287 2536–2559
58. Shimizu M, Suzuki K, Kato K, et al. Evaluation 74. Wu Q, Zhang M, Qin Y, et al. Systematic 89. Bhasin S, Brito JP, Cunningham GR, et al.
of the effects of dapagliflozin, a sodium-glucose review and meta-analysis of islet autotransplan- Testosterone therapy in men with hypogonadism:
co-transporter-2 inhibitor, on hepatic steatosis tation after total pancreatectomy in chronic an Endocrine Society clinical practice guideline. J
and fibrosis using transient elastography in pa- pancreatitis patients. Endocr J 2015;62:227–234 Clin Endocrinol Metab 2018;103:1715–1744
tients with type 2 diabetes and non-alcoholic 75. Janghorbani M, Van Dam RM, Willett WC, Hu 90. Li C, Ford ES, Zhao G, Croft JB, Balluz LS,
fatty liver disease. Diabetes Obes Metab 2019; FB. Systematic review of type 1 and type 2 Mokdad AH. Prevalence of self-reported clini-
21:285–292 diabetes mellitus and risk of fracture. Am J cally diagnosed sleep apnea according to obesity
59. Kuchay MS, Krishan S, Mishra SK, et al. Effect Epidemiol 2007;166:495–505 status in men and women: National Health and
of dulaglutide on liver fat in patients with type 2 76. Vestergaard P. Discrepancies in bone min- Nutrition Examination Survey, 2005-2006. Prev
diabetes and NAFLD: randomised controlled trial eral density and fracture risk in patients with Med 2010;51:18–23
(D-LIFT trial). Diabetologia 2020;63:2434–2445 type 1 and type 2 diabetes–a meta-analysis. 91. West SD, Nicoll DJ, Stradling JR. Prevalence
60. Lecube A, Hernández C, Genescà J, Simó R. Osteoporos Int 2007;18:427–444 of obstructive sleep apnoea in men with type 2
Proinflammatory cytokines, insulin resistance, 77. Schwartz AV, Vittinghoff E, Bauer DC, et al.; diabetes. Thorax 2006;61:945–950
and insulin secretion in chronic hepatitis C Study of Osteoporotic Fractures (SOF) Research 92. Resnick HE, Redline S, Shahar E, et al.; Sleep
patients: a case-control study. Diabetes Care Group; Osteoporotic Fractures in Men (MrOS) Heart Health Study. Diabetes and sleep distur-
2006;29:1096–1101 Research Group; Health, Aging, and Body Com- bances: findings from the Sleep Heart Health
61. Hum J, Jou JH, Green PK, et al. Improvement position (Health ABC) Research Group. Associ- Study. Diabetes Care 2003;26:702–709
in glycemic control of type 2 diabetes after ation of BMD and FRAX score with risk of fracture 93. Foster GD, Sanders MH, Millman R, et al.;
successful treatment of hepatitis C virus. Di- in older adults with type 2 diabetes. JAMA 2011; Sleep AHEAD Research Group. Obstructive sleep
abetes Care 2017;40:1173–1180 305:2184–2192 apnea among obese patients with type 2 di-
62. Carnovale C, Pozzi M, Dassano A, et al. The 78. Kahn SE, Zinman B, Lachin JM, et al.; Diabetes abetes. Diabetes Care 2009;32:1017–1019
impact of a successful treatment of hepatitis C Outcome Progression Trial (ADOPT) Study 94. Bibbins-Domingo K, Grossman DC, Curry SJ,
virus on glyco-metabolic control in diabetic Group. Rosiglitazone-associated fractures in et al.; US Preventive Services Task Force. Screen-
patients: a systematic review and meta-analysis. type 2 diabetes: an analysis from A Diabetes ing for obstructive sleep apnea in adults: US
Acta Diabetol 2019;56:341–354 Outcome Progression Trial (ADOPT). Diabetes Preventive Services Task Force recommendation
63. Piciucchi M, Capurso G, Archibugi L, Delle Care 2008;31:845–851 statement. JAMA 2017;317:407–414
Fave MM, Capasso M, Delle Fave G. Exocrine 79. Taylor SI, Blau JE, Rother KI. Possible adverse 95. Shaw JE, Punjabi NM, Wilding JP, Alberti
pancreatic insufficiency in diabetic patients: effects of SGLT2 inhibitors on bone. Lancet Di- KGMM, Zimmet PZ; International Diabetes Fed-
prevalence, mechanisms, and treatment. Int J eration Taskforce on Epidemiology and Preven-
abetes Endocrinol 2015;3:8–10
Endocrinol 2015;2015:595649 tion. Sleep-disordered breathing and type 2
80. Baiduc RR, Helzner EP. Epidemiology of di-
64. Lee Y-K, Huang M-Y, Hsu C-Y, Su Y-C. Bi-
abetes and hearing loss. Semin Hear 2019;40: diabetes: a report from the International Di-
directional relationship between diabetes and
281–291 abetes Federation Taskforce on Epidemiology
acute pancreatitis: a population-based cohort
81. Helzner EP, Contrera KJ. Type 2 diabetes and Prevention. Diabetes Res Clin Pract 2008;81:
study in Taiwan. Medicine (Baltimore) 2016;95:
and hearing impairment. Curr Diab Rep 2016; 2–12
e2448
16:3 96. Khader YS, Dauod AS, El-Qaderi SS, Alkafajei
65. Das SLM, Singh PP, Phillips ARJ, Murphy R,
82. Bainbridge KE, Hoffman HJ, Cowie CC. Di- A, Batayha WQ. Periodontal status of diabetics
Windsor JA, Petrov MS. Newly diagnosed di-
abetes and hearing impairment in the United compared with nondiabetics: a meta-analysis. J
abetes mellitus after acute pancreatitis: a sys-
States: audiometric evidence from the National Diabetes Complications 2006;20:59–68
tematic review and meta-analysis. Gut 2014;63:
Health and Nutrition Examination Survey, 1999 97. Casanova L, Hughes FJ, Preshaw PM. Di-
818–831
to 2004. Ann Intern Med 2008;149:1–10 abetes and periodontal disease: a two-way re-
66. Petrov MS. Diabetes of the exocrine pan-
83. Bainbridge KE, Hoffman HJ, Cowie CC. Risk lationship. Br Dent J 2014;217:433–437
creas: American Diabetes Association-compliant
factors for hearing impairment among U.S. adults 98. Eke PI, Thornton-Evans GO, Wei L,
lexicon. Pancreatology 2017;17:523–526
67. Thomsen RW, Pedersen L, Møller N, Kahlert with diabetes: National Health and Nutrition Borgnakke WS, Dye BA, Genco RJ. Periodontitis
J, Beck-Nielsen H, Sørensen HT. Incretin-based Examination Survey 1999-2004. Diabetes Care in US Adults: National Health and Nutrition
therapy and risk of acute pancreatitis: a nation- 2011;34:1540–1545 Examination Survey 2009-2014. J Am Dent Assoc
wide population-based case-control study. Di- 84. Schade DS, Lorenzi GM, Braffett BH, et al.; 2018;149:576–588.e6
abetes Care 2015;38:1089–1098 DCCT/EDIC Research Group. Hearing impairment 99. Simpson TC, Weldon JC, Worthington HV,
68. Tkáč I, Raz I. Combined analysis of three large and type 1 diabetes in the Diabetes Control and et al. Treatment of periodontal disease for
interventional trials with gliptins indicates in- Complications Trial/Epidemiology of Diabetes glycaemic control in people with diabetes
creased incidence of acute pancreatitis in pa- Interventions and Complications (DCCT/EDIC) mellitus. Cochrane Database Syst Rev 2015;11:
tients with type 2 diabetes. Diabetes Care 2017; Cohort. Diabetes Care 2018;41:2495–2501 CD004714
40:284–286 85. Rasmussen VF, Vestergaard ET, Hejlesen O, 100. D’Aiuto F, Gkranias N, Bhowruth D, et al.;
69. Egan AG, Blind E, Dunder K, et al. Pancreatic Andersson CUN, Cichosz SL. Prevalence of taste TASTE Group. Systemic effects of periodontitis
safety of incretin-based drugs–FDA and EMA and smell impairment in adults with diabetes: treatment in patients with type 2 diabetes:
assessment. N Engl J Med 2014;370:794–797 across-sectional analysis of data from the Na- a 12 month, single-centre, investigator-masked,
70. Bellin MD, Gelrud A, Arreaza-Rubin G, et al. tional Health and Nutrition Examination Survey randomised trial. Lancet Diabetes Endocrinol
Total pancreatectomy with islet autotransplan- (NHANES). Prim Care Diabetes 2018;12:453– 2018;6:954–965
tation: summary of an NIDDK workshop. Ann 459 101. Davies MJ, D’Alessio DA, Fradkin J, et al.
Surg 2015;261:21–29 86. Dhindsa S, Miller MG, McWhirter CL, et al. Management of hyperglycemia in type 2 diabe-
71. Sutherland DER, Radosevich DM, Bellin MD, Testosterone concentrations in diabetic and non- tes, 2018: a consensus report by the American
et al. Total pancreatectomy and islet autotrans- diabetic obese men. Diabetes Care 2010;33: Diabetes Association (ADA) and the European
plantation for chronic pancreatitis. J Am Coll Surg 1186–1192 Association for the Study of Diabetes (EASD).
2012;214:409–424; discussion 424–426 87. Grossmann M. Low testosterone in men with Diabetes Care 2018;41:2669–2701
72. Quartuccio M, Hall E, Singh V, et al. Glycemic type 2 diabetes: significance and treatment. J Clin 102. Karter AJ, Warton EM, Lipska KJ, et al.
predictors of insulin independence after total Endocrinol Metab 2011;96:2341–2353 Development and validation of a tool to identify
pancreatectomy with islet autotransplantation. 88. Bhasin S, Cunningham GR, Hayes FJ, et al.; patients with type 2 diabetes at high risk of
J Clin Endocrinol Metab 2017;102:801–809 Task Force, Endocrine Society. Testosterone hypoglycemia-related emergency department or
73. Webb MA, Illouz SC, Pollard CA, et al. Islet auto therapy in men with androgen deficiency syn- hospital use. JAMA Intern Med 2017;177:1461–
transplantation following total pancreatectomy: dromes: an Endocrine Society clinical practice 1470You can also read