Follow-up for Positive COVID-19 Cases and their Close Contacts
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Follow-up for Positive COVID-19
Cases and their Close Contacts
Tools for LBOHs
April 6, 2021
Hillary Johnson, MHS, Infectious Disease Epidemiologist
Scott Troppy, MPH, PMP, CIC, Surveillance Epidemiologist
Alexandra DeJesus, MPH, CIC, Infectious Disease Epidemiologist
Bureau of Infectious Disease and Laboratory Sciences
MA Department of Public Health
Updates for today, Tuesday, 4/6/2021 ▪ Variant’s of Concern Review with Dr. Catherine Brown ▪ LBOH Immediate Workflow – COVID-19 event only – please check your workflow TODAY and clear out the workflow ▪ LBOH Confirmed and Probable Report and the LBOH Notification for Immediate Disease (COVID only) Workflow ▪ Currently report is configured to run off of Event Date ▪ Updating MAVEN to address SARS-Coronavirus2 RdRp gene test so it will populate first positive specimen date in the Clinical QP#3 ▪ On-Call Stats – March #’s 2

COVID Variants of Concern
MAVEN Users Webinar
Dr. Catherine Brown
April 6, 2021
SARS-CoV-2 Variants
• Variant Classification Scheme
• Variant of interest - A variant with specific genetic markers that have been associated with
changes to receptor binding, reduced neutralization by antibodies generated against previous infection or
vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or
disease severity.
• Examples: B.1.526 and B.1.525 – New York, P.2 – Brazil
• Possible attributes of a variant of interest:
• Specific genetic markers that are predicted to affect transmission, diagnostics, therapeutics, or immune escape
• Evidence that demonstrates it is the cause of an increased proportion of cases or unique outbreak clusters
• Limited prevalence or expansion in the US or in other countries
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/variant-info.html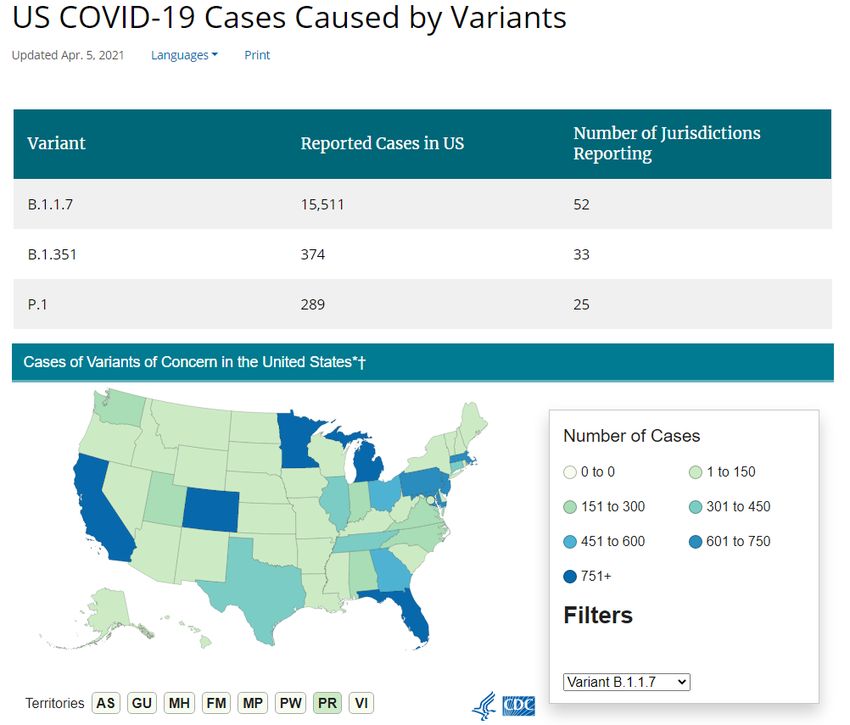
SARS-CoV-2 Variants
• Variant Classification Scheme
• Variant of concern - A variant for which there is evidence of an increase in transmissibility, more
severe disease (increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated
during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection
failures.
• Examples: B.1.1.7 (UK), B.1.351 (South Africa), P.1 (Brazil)
• Newly added: B.1.427 and B.1.429 – California
• Possible attributes of a variant of concern:
• Evidence of impact on diagnostics, treatments, and vaccines
• Widespread interference with diagnostic test targets
• Evidence of substantially increased resistance to one or more class of therapies
• Evidence of significant decreased neutralization by antibodies generated during previous infection or
vaccination
• Evidence of reduced vaccine-induced protection from severe disease
• Evidence of increased transmissibility
• Evidence of increased disease severity
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/variant-info.html
SARS-CoV-2 Variants
• Variant Classification Scheme
• Variant of high consequence - A variant of high consequence has clear evidence that
prevention measures or medical countermeasures (MCMs) have significantly reduced effectiveness relative to
previously circulating variants.
• None at this time
• Possible attributes of a variant of high consequence:
• Impact on Medical Countermeasures (MCM)
• Demonstrated failure of diagnostics
• Evidence to suggest a significant reduction in vaccine effectiveness, a disproportionately high number of
vaccine breakthrough cases, or very low vaccine-induced protection against severe disease
• Significantly reduced susceptibility to multiple Emergency Use Authorization (EUA) or approved therapeutics
• More severe clinical disease and increased hospitalizations
• A variant of high consequence would require notification to WHO under the International Health
Regulations, reporting to CDC, an announcement of strategies to prevent or contain transmission, and
recommendations to update treatments and vaccines.
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/variant-info.html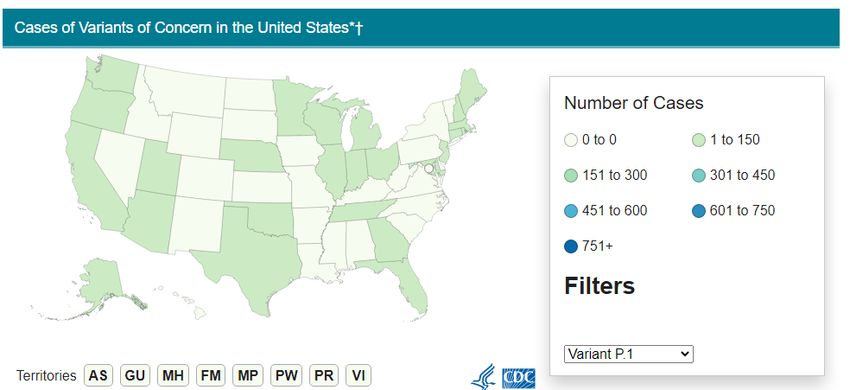

MA: 712
MA: 58 MA: 12

Variant Cases by Specimen Collection Date
60
50
40
P.1
30
B.1.351
B.1.1.7
20
10
060
50
40
30 P.1
B.1.351
20 B.1.1.7
10
0SEX Count Female 511 Male 516 Transgender 1 Grand Total 1028
Where we are right now
• B.1.1.7
• Community transmission
• Individual investigation not necessary
• B.1.351
• Remain very rare
• Individual investigation helpful
• Ask about recent travel or contact with someone with recent travel
• P.1
• Most common on Barnstable County – community
transmission
• Individual investigation helpful outside of Barnstable
• Ask about recent travel or contact with someone with recent traveSequencing/Variant Surveillance
• Massachusetts
• State Public Health Laboratory (200 samples/week)
• Broad
• BU/NEIDL – all positive cases from BU and certain cases from BMC
• Nationally
• LabCorp
• Quest
• Helix/Illumina
• Aegis
• CDC
• 10 days to 2 week time lag for sequencing results (from specimen
collection date)
https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant-cases.html
https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/genomic-surveillance-dashboard.htmlhttps://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-proportions.html
Estimated proportion of variants in jurisdictions
reporting > 300 sequences for the 4 week time
period ending 3/13/2021
State B.1.1.7 Variant P.1 Variant B.1.351 Variant B.1.427/B.1.429
FL 34.5% 1.2% 0.3% 9.4%
MI 39.0% 0.1% 0.1% 7.2%
CA 10.3% 0.7% 0.1% 56.1%
MA 18.6% 1.4% 0.2% 3.6%
GA 22.1% 0.2% 4.8%
MN 25.5% 0.2% 10.9%
MD 20.4% 1.6% 4.0%
CO 16.6% 0.3% 25.9%
PA 14.1% 0.3% 4.8%
TX 25.2% 0.1% 0.2% 8.0%
• Utilizes CDC and national vendor sequence data only
• less prone to collection bias
• Stable at the national level, less stable at smaller geographic levels
• Modeling-based estimates currently in development
• Conversations with CDC, APHL and CSTE about
• Right-sizing surveillance
• Metadata to indicate reason for sequencingCOUNTY B.1.1.7 B.1.351 P.1 Grand Total
BARNSTABLE
35 63 98
COUNTY
BERKSHIRE
3 3
COUNTY
BRISTOL COUNTY 36 2 38
ESSEX COUNTY 177 3 6 186
FRANKLIN COUNTY 3 3
HAMPDEN
17 1 18
COUNTY
HAMPSHIRE
11 11
COUNTY
MIDDLESEX
183 5 7 195
COUNTY
NORFOLK COUNTY 130 1 131
PLYMOUTH
65 3 68
COUNTY
SUFFOLK COUNTY 197 2 199
WORCESTER
117 1 118
COUNTY
Grand Total 974 12 82 1068
Courtesy of the Viral Genomics Lab at the Broad
Comments from the Viral Genomics Lab at the Broad re: P.1
• Indicates 5 distinct importations into MA
• 44/52 genomes – transmission cluster
• 4 cases which link closely to 2 cases in Nebraska
• 1 case links closely to Italian genomes
• Data suggest additional undetected P.1 cases
• Requires additional genomic and epidemiologic workSequencing • Surveillance • Random sample • Understand what is happening in our communities • Reinfections and vaccine breakthrough • Understand extent of impact
Ongoing work • Cluster investigations in Barnstable County with LBOH and CTC • Contributing specimens to CDC for random sampling of variants in MA • Collaborating with Broad CRSP and Viral Genomics to sequence more specimens • Randomly • Outbreak investigation • Participating in national discussions on • right-sizing surveillance • Electronic laboratory reporting of variant results
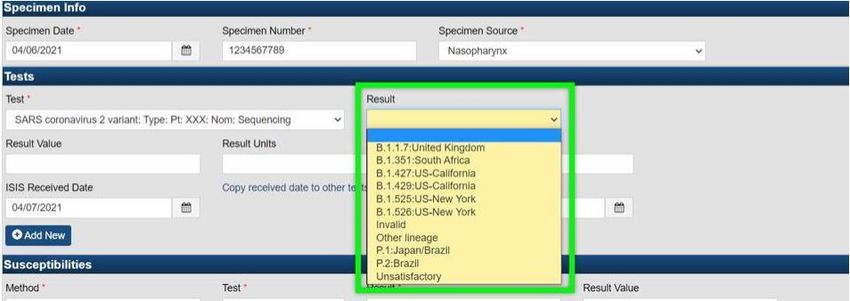
MAVEN 4/5/21 - Updates for Variant’s
COVID-19 Variant’s of Concern
▪ Added variable to capture if specimens were sequenced
and a new variant was identified (Variant of Concern) in
SARS events [MAEDSS-13037]
▪ Added question to the Clinical Question Package and COVID Wizard
▪ Not editable by local users
▪ If question is answered as Yes users will need to review lab data to
see which variant has been sequenced
▪ Information will be updated on an ongoing basis in the question
package
▪ Added to the LBOH Confirmed and Probable ReportCOVID Confirmed and Probable Report
22First Positive Specimen Date – Antigen Test
23First Positive Specimen Date – PCR Test
24On-Call Events, MAVEN Help Desk &
COVID-19 Weekly Webinars
Statistics
March 2021 Report
Reed Sherrill, Surveillance Epidemiologist
Scott Troppy, MPH, PMP, CIC, Surveillance Epidemiologist
Bureau of Infectious Disease and Laboratory Sciences
MA Department of Public HealthMAVEN User Requests & Training
3/1/2020 - 4/5/2021
Status Count
Pending Users 108
Processed Users 2,086
Total New Users Trained Or In Process 2,194
Total MAVEN Users 1,690*
Pending = User has submitted a URF and is in the training process
Processed = Trained internal and external staff with VG MAVEN accounts created and MAVEN accounts created by
ISIS staff and then access granted appropriate access.
Total MAVEN Users = Includes MDPH, LBOH, CTC, Higher Ed, Infection Prevention and other trained staff
*Total New Users Trained/in process exceeds total MAVEN users due to retraining and/or individuals coming
offline and back on again
26
*these data are accurate as of 4/5/2021 at 10:30AM.MAVEN On-Call Events
3/1/2021 – 3/31/2021
Program Area Count
Division of Global Populations 11
Epidemiology 170
Immunization (COVID-19) 1598
Immunization (non-COVID-19) 51
Informatics and Surveillance (ISIS) 74
STD 3
Total On-Call MAVEN Events 1,907
27
*these data are accurate as of 3/6/2021 at 6:30PMMAVEN On-Call Events
3/1/2020 – 3/31/2021
Program Area Count
Division of Global Populations 154
Epidemiology 3,725
Immunization (COVID-19) 37,744
Informatics and Surveillance (ISIS) 2,327
STD 23
Total On-Call MAVEN Events 43,973
28
*these data are accurate as of 4/5/2021 at 10:30AMFor Reference what our call volume
usually looks like….
Year Total On-Call Events
Created
2015 6,739
2016 12,830
2017 12,605
2018 9,296
2019 10,652
2020 40,029
29
2021 6,384
*these data are accurate as of 4/5/2021 at 10:30AMMAVEN Help Desk Emails
3/15/2020 – 3/31/2021
Month Count
March 2020 2,383
April 2020 7,816
May 2020 7,603
June 2020 6,602
July 2020 5,231
August 2020 6,280
September 2020 5,313
October 2020 9,587
November 2020 12,225
December 2020 13,273
January 2021 11,727
February 2021 8,244
30
March 2021 8,977
Total Emails received 105,261
*these data are accurate as of 4/5/2021 at 10:30AMTuesday and Friday Webinars
for COVID-19 Investigations/Follow-up
lead by Hillary Johnson and Scott Troppy
31Tuesday’s Webinar Attendance, 2020
3/24/2020 – 12/22/2020
1000
910
900
800
700
600 575 570
501 515
500 475 474 466
455
432
394 395 403
375 389 392 409
400 352 344 350
331 333 348
313 323 315 323
286 290 303 275 292 284
302 296
300 265 254 272
200
93
100
0
32Friday’s Webinar Attendance, 2020
4/8/2020 – 12/18/2020
600
500 468 481
432 419 422
398
400 374
356
309 309
288 275
300
243
221 212
196 196
200 161
148
107 120 122
92 104 104 105
100
0
*4/8 was a special Wednesday Introductory Contact Tracing Training
**9/18 started Friday DPH Office Hours (webinar live question session)
33Tuesday’s Webinar Attendance, 2021
1/5/2021 – 3/30/2021
500 466
447
450
391 402
400 379 369 379
328 338 338 329 345
350
300
250 235
200
150
100
50
0
34Friday’s Webinar Attendance, 2021
1/8/2021 – 3/26/2021
200
182 181
180
174
164 160
160 149 150 155
137 138
140 124
120
100 83
80
60
40
20
0
35You can also read

















































