CLINICAL ISSUES OF THE DAY - REGISTER FOR THE 51ST CRITICAL CARE CONGRESS DETAILS INSIDE!
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

VOL. 20 NO. 3 // SUMMER 2021
CLINICAL
ISSUES
OF THE DAY
REGISTER FOR THE 51ST CRITICAL CARE CONGRESS
February 6-9, 2022,
Puerto Rico Convention Center | San Juan, Puerto Rico | Smart Event
DETAILS INSIDE!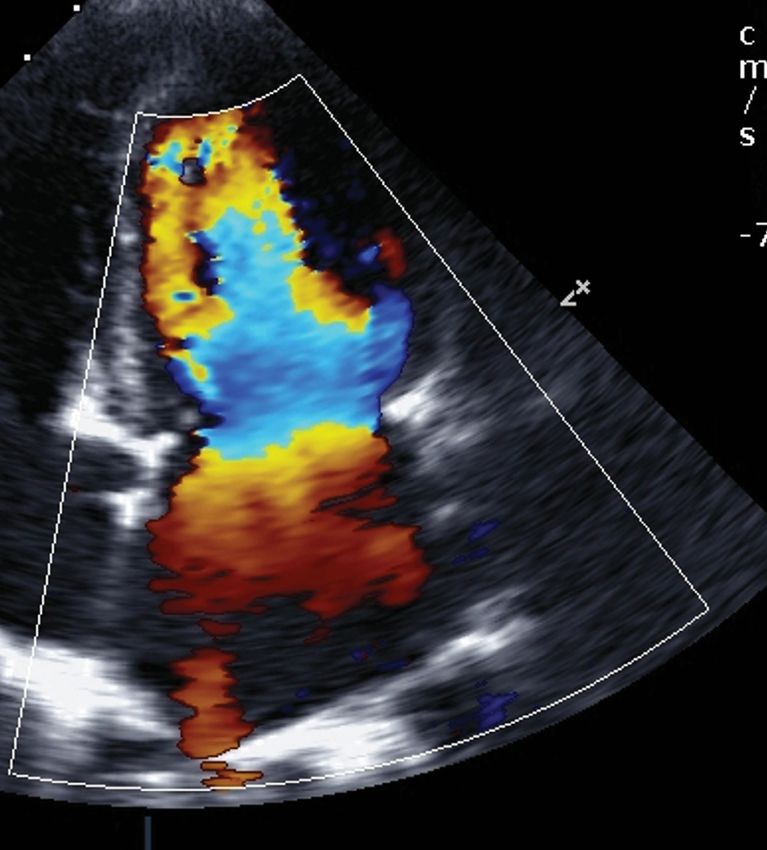
MULTIPLE blood purification therapies. ONE solution.
With or without CRRT, the
OXIRIS blood purification
device is designed to
remove inflammatory
mediators in the treatment
of COVID-19 patients.
OXIRIS can be used for any
of the following conditions:
• Respiratory failure
• Septic shock
• Multiple organ
dysfunction/failure
Visit usrenalacute.baxter.com/oxiris for more info.
The OXIRIS Set device is authorized under EUA200164 (Emergency Use Authorization) to treat patients 18 years
of age or older with confirmed Coronavirus Disease 2019 (COVID-19) infection admitted to the intensive care unit
(ICU) with confirmed or imminent respiratory failure in need of blood purification, including use in continuous
renal replacement therapy. This device has neither been cleared or approved for the indication to treat patients
with COVID-19 infection. The device is authorized only for the duration of the declaration that circumstances exist
justifying the authorization of the emergency use of the OXIRIS Set under section 564(b)(1) of the Act, 21 U.S.C.
§360bbb-3(b)(1), unless the authorization is terminated or revoked sooner.
Rx Only. For safe and proper use of products mentioned herein, refer to the appropriate Instructions for Use or Operator’s Manual.
Baxter and Oxiris are trademarks of Baxter International Inc, or its subsidiaries.
US-AT11-210008 (v1.0) 04/21
VOL. 20 NO. 03 // SUMMER 2021
Contents
Clinical Spotlight: Clinical Issues of the Day
16 18 22 24
Care of the Critically The Rural Rapid ARDS: Will Precision Ethical Considerations
Injured Patient: Trends Response Team: How Approaches Move for a COVID-19
Expected for 2021 embedded Navy teams the Needle? Vaccine Mandate
and Beyond provided COVID-19
response in small South
Texas hospitals
Departments Exploring Ethics
Editor’s Message . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Implicit Versus Explicit Limitation of Scarce Critical Care
President’s Message . . . . . . . . . . . . . . . . . . . . . . . . . . 14 Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
Coding and Billing
Section and Chapter News. . . . . . . . . . . . . . . . . . . . . . 40
SCCM Update Pay Attention When Coding Critical Care.. . . . . . . . . . . 38
An SCCM Member Responds to a Call for Volunteers. . 28
Drug Shortages
Infusion Pumps Outside Patient Rooms: Clinical
Considerations and Medication Safety . . . . . . . . . . . . . 30 REGISTER FOR THE 51ST CRITICAL CARE CONGRESS
ICU Liberation Smart Event | February 6-9, 2022
Puerto Rico Convention Center | San Juan, Puerto Rico
Considerations For Implementing the ICU Liberation
Bundle in a Subspecialty ICU . . . . . . . . . . . . . . . . . . . . 32
SEE PAGES 5 – 11
SCCM.ORG SUMMER 2021 // CriticalConnections // 3
Editor’s Message
THE COMPLETE NEWS SOURCE FOR
Clinical Issues of the Day
CRITICAL CARE PROFESSIONALS
VOL. 20 NO. 3 // SUMMER 2021
I
Editor
Jose L. Pascual, MD, PhD, FACS, FCCM
SICU Co-Medical Director
am thrilled to present to you this summer 2021 issue of Critical Perelman School of Medicine
Connections. We begin with a preliminary glimpse of the excep- Philadelphia, Pennsylvania, USA
tional program of the 51st Critical Care Congress that will take Editorial Advisory Board
place in San Juan, Puerto Rico, February 6-9, 2022. Take note of the President Secretary
five extraordinary plenary sessions to be presented by world-renowned Greg S. Martin, MD, MSc, FCCM Vinay M. Nadkarni, MD, FCCM
Professor, Master Clinician, Professor
experts alongside other award-winning sessions, workshops, panel dis- and Executive Associate University of Pennsylvania
cussions, and case discussions that promise to delight all critical care Division Director Perelman School of Medicine
Jose L. Pascual, MD, professionals. Congress sessions will also cover the current state of the Division of Pulmonary, Allergy, Philadelphia, Pennsylvania, USA
PhD, FACS, FRCS(C), Critical Care and Sleep Medicine
COVID-19 pandemic, particularly highlighting post-COVID sequelae. Emory University
Treasurer
FCCM, is an associate Lauren Sorce, PhD, RN, CPNP-AC/PC, FCCM
School of Medicine
professor of surgery SCCM President Greg S. Martin, MD, MSc, FCCM, opens this issue Research Director, Emory
Founders Board Nurse Scientist
and neurosurgery at Associate Director Nursing Research
with a discussion of post-COVID symptoms persisting beyond the initial Critical Care Center
Pediatric Critical Care Nurse Practitioner
the Perelman School four weeks of infection or acute SARS-CoV-2 infection. COVID-19 symp- Director, Emory/Georgia Tech
Ann & Robert H. Lurie Children’s
of Medicine and a Predictive Health Institute
Hospital of Chicago
clinical associate toms persisting for up to 12 weeks after initial infection can be followed Atlanta, Georgia, USA
Assistant Professor, Division of
at the University of by a longer chronic phase termed long COVID or post-acute sequelae President-elect Pediatric Critical Care Medicine
Pennsylvania School Sandra L. Kane-Gill, PharmD, Northwestern University, Feinberg
of COVID-19 (PASC). Increasing numbers of patients are manifesting MSc, FCCP, FCCM School of Medicine
of Nursing. He is also PASC symptoms of fatigue, dyspnea, brain fog, cough, chest pain, joint Professor of Pharmacy, Chicago, Illinois, USA
co-director of the School of Pharmacy
surgical intensive care or muscle pain, headache, dizziness, depression, anxiety, and loss of Professor of Critical Care
Past President
taste or smell. Lewis J. Kaplan, MD, FACS, FCCM
unit at the Hospital Medicine, Biomedical
Department of Surgery
of the University of Informatics, and Clinical
Another fascinating article is brought to you by some of SCCM’s & Translational Science
Division of Trauma, Surgical Critical
Pennsylvania. He Emergency Medicine Section and Surgery Section members high- (secondary appointments),
Care and Emergency Surgery
practices critical Perelman School of Medicine,
Faculty, Center for Critical Care
care, neurocritical lighting the stark increase in critical injury, particularly violent injury, Nephrology, School of Medicine,
University of Pennsylvania
involving firearms beginning in 2020 and continuing to the present Philadelphia, Pennsylvania, USA
care, trauma, and University of Pittsburgh
Section Chief, Surgical Critical Care
emergency surgery and day. Paradoxically they also describe a rise in vehicular crashes and Critical Care Medication
Director, Surgical Intensive Care Unit
Safety Pharmacist,
runs a basic science injury during this same time period despite fewer vehicles on the road UPMC
Corporal Michael J. Crescenz
traumatic brain injury VA Medical Center
Pittsburgh, Pennsylvania, USA
Lab in Philadelphia due to prolonged lockdowns and quarantines. The authors seek social Philadelphia, Pennsylvania, USA
Pennsylvania, USA. determinants for these near-double injury numbers in the setting of
disrupted American societal norms caused by isolation from family Critical Connections Staff
and social contacts, rapidly rising unemployment, food insecurity, and resource scarcity Managing Editor Director of Marketing
Melissa Nielsen Danny Lysouvakon
bringing about a sense of desperation in many people. mnielsen@sccm.org
+1 847 827-7405
Chief Executive Officer and
While these tragic trends were happening in many urban American cities, another was
Executive Vice President
taking place in Texas small towns, where authors Commander Michael J. Kavanaugh, MD; Advertising David Julian Martin, CAE
Desiree Ng
Captain Sean A. McKay, MD; and Commander Joseph Zeman, MD, describe how embedded dng@sccm.org Graphic Designer
navy critical care teams deployed rapid response assistance to rural communities during +1 847 827-7188 Randy Schirz
this crisis. This is another remarkable example of how, during the past 18 months, military
Contributing Author: Marc Zarefsky
medicine has reached well beyond the call of duty to support civilian medical personnel
Editorial Contributions: You are invited to share your expertise and perspective.
when disease burden exceeded local hospital systems’ capacity. Please contact the Staff Partner, Kara Mercer at +1 847 493-6438 or
Also noteworthy is a captivating discussion on the ethical considerations of mandating kmercer@sccm.org.
COVID-19 vaccination for healthcare workers. Preeti R. John, MD, MPH, FACS, HEC-C, and Critical Connections reserves the right to edit all articles and
other authors present opposing viewpoints on the perennial pillars of beneficence, nonma- classified ads.
leficence, autonomy, and justice. Italy and other countries have begun to mandate COVID-19 Critical Connections is published quarterly by the Society of Critical Care
Medicine, 500 Midway Dr.,Mount Prospect, IL 60056-5811 USA.
vaccinations nationally. In the United States, more and more groups and institutions have
Critical Connections’ mission is to provide SCCM members and critical care
implemented such mandates. More than 50 healthcare professional organizations are in professionals with timely information regarding the practice of critical care and
favor of all healthcare employers requiring employees to be vaccinated against COVID-19 the Society’s activities.
to protect the safety of patients, healthcare workers, and communities. Postmaster: Send address changes to Critical Connections,
Society of Critical Care Medicine,
Finally, an interesting article from the Drug Shortages and Medication Safety Committee 500 Midway Dr., Mount Prospect, IL 60056-5811 USA.
addresses the use of extension IV tubing to permit placement of infusion pumps outside Canadian return mail address is Station A, Box 54, Windsor ON, N9A 6J5
patient rooms. This practice limits delays in initiating and adjusting medications while also Copyright © 2021 by the Society of Critical Care Medicine.
preventing multiple reentries in and out of patient rooms. While extension tubing was used All rights reserved. Statements of fact and opinion are the responsibility of the
before the pandemic in the context of the MRI suite, this practice must be implemented with authors alone and do not imply an opinion on the part of the officers or members.
caution to prevent harm to patients.
4 \\ CriticalConnections \\ SUMMER 2021
51st CONGRESS PRELIMINARY PROGRAM
FEBRUARY 6-9, 2022
SMART EVENT FEATURING FLEXIBLE LEARNING OPTIONS
IN PERSON: LEARN LIVE FEBRUARY 6-9, 2022, AT THE PUERTO RICO CONVENTION CENTER IN SAN JUAN, PUERTO RICO
ONLINE: LEARN VIRTUALLY THROUGH SELECT LIVE SESSION BROADCASTS, SESSION RECORDINGS, AND VIRTUAL Q&A WITH EXPERTS
51st CONGRESS PRELIMINARY PROGRAM 51ST CRITICAL
CARE
CONGRESS
COCHAIRS
Jose J. Diaz Jr, MD, CPE, CNS,
FEBRUARY 6-9, 2022 • SAN JUAN, PUERTO RICO • SMART EVENT FACS, FCCM
Professor of Surgery, Epidemiology, and
Public Health
Join the Society of Critical Care Medicine (SCCM) for the 51st Critical
University of Maryland School of
Care Congress and dive into the latest knowledge and research.
Medicine
SCCM offers a smart event experience with flexible learning options.
Chief, Division of Acute Care Surgery
IN PERSON:
Program Director, Acute Care Surgery
• Learn live February 6-9, 2022, in San Juan, Puerto Rico.
Fellowship Program in Trauma
• Receive a unique, high-quality educational experience while
building relationships and networking, learning from peers, and Surgery Quality Officer
interacting with world-renowned thought leaders. University of Maryland Medical Center
• Immerse yourself in the local island culture with plenty of
President
opportunities to unwind, have fun, and gather with friends.
Maryland Chapter of the American
ONLINE:
College of Surgeons
• Learn as your time permits on an easy-to-use platform.
• Receive an efficient, high-quality educational experience, perfect Baltimore, Maryland, USA
for busy professionals and those who cannot get away.
• Save on travel costs while still earning accredited continuing
education (ACE) credit.
Meghan B. Lane-Fall, MD, MSHP,
• Access programming from anywhere for one year. FCCM
DECIDE AT ANY TIME. Vice Chair of Inclusion, Diversity, and
Equity
The critical care community has made an incredible impact
on the world. SCCM looks forward to recognizing these key David E. Longnecker Associate
Professor of Anesthesiology and Critical
accomplishments and the opportunity to reconnect with its
Care
members, colleagues, and friends.
Associate Professor of Epidemiology
University of Pennsylvania Perelman
School of Medicine
Senior Fellow of the Leonard Davis
Institute of Health Economics
REGISTER EARLY TO SECURE YOUR TOP University of Pennsylvania
CHOICES AND ACCOMMODATIONS AT THE Philadelphia, Pennsylvania, USA
LOWEST RATES.
EARLY RATE: Register by December 8, 2021
Heather H. Meissen, DNP, ACNP,
ADVANCE RATE: Register by January 12, 2022
FCCM
Director, NP/PA Critical Care
View rates and register at sccm.org/congress2022 Fellowship
or contact customer service at +1 847 827-6888.
Emory Healthcare
Atlanta, Georgia, USA
6 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869
1year of access to On Demand content
100+ CE/ACE Hours
200+ world- Flexible
30+
renowned
expert learning
critical care
speakers options
1300+
abstracts presented In person Online
topic bundles
covering critical
care topics
TOP REASONS TO ATTEND:
ACCESS EXPLORE NETWORK DISCOVER CELEBRATE SHARE
training and new tools and and collaborate the latest the critical care key takeaways
resources needed technologies and with colleagues research, community and with your critical
to attain your gain knowledge and critical care exchange recognize key care team
personal and to improve experts from knowledge, and accomplishments. and improve
professional goals. patient care. around the world. find solutions to patient care.
common issues.
SCCM.ORG SUMMER 2021 // CriticalConnections // 7
For complete details on
Congress events, visit
51st CONGRESS PRELIMINARY PROGRAM sccm.org/congress2022
PLENARY SESSIONS
Engage in discussions on innovative developments in critical care with world- THOUGHT LEADER SESSIONS
renowned experts during the unopposed Congress plenary sessions.
Explore hot topics in critical care with
Max Harry Weil Memorial Lecture distinguished thought leaders.
What Has COVID-19 Taught Us About ECMO?
Peta M.A. Alexander, MBBS, FRACP, FCICM
Staff Physician Lifetime Award
Department of Cardiology Recipient
Boston Children’s Hospital Philip S. Barie, MD,
Assistant Professor MCCM
Department of Pediatrics
Harvard Medical School Genetics and
Boston, Massachusetts, USA Genomics
Karin Reuter-Rice,
Peter Safar Memorial Lecture PhD, CPNP-AC, FAAN,
Health System Readiness 2.0 FCCM
Brendan G. Carr, MD, MA, MS
Professor and System Chair The Future of Critical
Department of Emergency Medicine Care: Artificial
Icahn School of Medicine at Mount Sinai Intelligence to Zoom
New York, New York, USA Family Meetings
Michelle N. Gong,
Ake Grenvik Honorary Lecture MD, MS
The Role of Critical Care Professionals in Allocating Scarce
Rebecca A. Aslakson,
Resources
MD, PhD
Douglas B. White, MD, MAS
Professor of Critical Care Medicine, Medicine, and Clinical and
Critical Care Nurses
Translational Science
and COVID-19
Vice Chair for Faculty Development, Department of Critical Care Medicine
John J. Gallagher, DNP,
Director, Program on Ethics and Decision Making in Critical Illness,
RN, CCNS, CCRN-K,
CRISMA Center
TCRN, RRT, FCCM
Chair, Committee on Tenured Faculty Promotions and Appointments
Core Faculty, University of Pittsburgh Center for Bioethics and Health Law
Prehospital Critical
University of Pittsburgh School of Medicine
Care
Pittsburgh, Pennsylvania, USA
James Houser, MSN,
Norma J. Shoemaker Honorary Lecture APRN
Cultivating Leadership From Within
Beth A. Wathen, MSN, RN, CCRN-K Critical Care
President Disparities: The Fierce
American Association of Critical-Care Nurses Urgency of Now
Clinical Practice Specialist Joy D. Howell, MD,
Pediatric Intensive Care Unit FAAP, FCCM
Children’s Hospital Colorado
Aurora, Colorado, USA
LATE-BREAKING PLENARY AND THOUGHT LEADER SPEAKERS WILL BE ANNOUNCED IN FALL 2021!
8 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869
= TICKETED SESSION REQUIRING ADVANCE REGISTRATION.
= FEE REQUIRED TO ATTEND. SEE REGISTRATION DETAILS AT SCCM.ORG/CONGRESS2022.
POPULAR CONGRESS EVENTS AND SESSIONS DON’T MISS THESE POPULAR
Educational Leadership Luncheon CONGRESS EVENTS
Monday, February 7, 2022
Critical care program directors, fellows, members of
Critical Care Quiz Show
Gather to watch and root for your team during this friendly
multiprofessional ICU teams, and those with a passion for critical
competition as contestants show off their critical care knowledge in
care education are invited to attend. This year’s luncheon topic,
this fast-paced game show.
How to Debate Dr. Internet: Dealing With Misinformation and Fake
News, will provide attendees with new ideas and strategies to deal
with misinformation found while searching the internet.
Advanced Practice Providers Luncheon
Tuesday, February 8, 2022
Critical care advanced practice providers (APPs) are invited
to attend and engage in informal networking and roundtable
discussions on topics related specifically to APPs and their
professional success.
Critical Crosstalk Theater
Educational Symposia
Hear discussion and debate focused on critical care topics in the
Learn about clinical breakthroughs and advances that lead to better
fields of internal medicine, anesthesiology, surgery, and more.
patient care during these thought-provoking sessions. Led by
critical care experts, each symposium offers a thorough analysis of
the developments and controversies affecting most intensive care
unit environments.
SCCM ABSTRACT PRESENTATIONS
Research Snapshot Theaters
Authors of abstracts and case reports will present their submissions
with time for questions and answers. Presentations will be held in Roundtable Discussions
designated sections of the Exhibit Hall from Sunday, February 6, Discuss critical care topics led by experienced moderators and
through Tuesday, February 8, 2022. network with peers on a variety of professional, career, and
leadership subjects.
Star Research Presentations
The top 64 abstracts and case reports will be highlighted during
Star Research presentations, held on Monday and Tuesday,
February 7 and 8, 2022.
Research Awards Ceremony
Recipients of SCCM’s abstract and case report awards will be
recognized during an awards ceremony on Sunday, February 6,
2022, at 3:30 p.m. Atlantic Time.
Luminary Lounge
Join past SCCM presidents as they share their experience and
wisdom about critical care and SCCM.
BE ON THE LOOKOUT FOR A VARIETY OF NEW OPPORTUNITIES FOR SMALL GROUP INTERACTION AND LEARNING
THROUGHOUT CONGRESS.
SCCM.ORG SUMMER 2021 // CriticalConnections // 9
For complete details on
Congress events, visit
51st CONGRESS PRELIMINARY PROGRAM sccm.org/congress2022
PRE-CONGRESS EDUCATIONAL OPPORTUNITIES COMPREHENSIVE
Each course is packed with essential clinical information to keep you well informed on
PROGRAM TOPICS
various critical care topics. Course prices vary. Many courses sell out; register early to Learning Objectives
secure your seat!
At the conclusion of the 51st Critical Care
Congress, participants should be able to:
FRIDAY, FEBRUARY 4, OR SATURDAY, FEBRUARY 5, 2022 ▲ Apply new knowledge and strategies
to optimize the care provided by the
multiprofessional team to the critically ill
Critical Care Ultrasound: Adult*
patient
▲ Examine research results and evidence-
Critical Care Ultrasound: Pediatric and Neonatal* based medicine techniques to evaluate
and improve patient care
FRIDAY, FEBRUARY 4, AND SATURDAY, FEBRUARY 5, 2022 ▲ Review and integrate guidelines to
measure performance and identify areas
Advanced VV ECMO Workshop for further study and improvement
Held in partnership with the Extracorporeal
Life Support Organization • Administration
• Cardiovascular
• Data Science
Airway and Mechanical Ventilation
• Diversity, Equity, and Inclusion
• Disaster
Current Concepts: Adult
• Endocrine
• Epidemiology/Outcomes
Current Concepts: Pediatrics
• Ethics/End of Life
• Gastrointestinal/Nutrition
ICU Liberation Simulation
• Hematology
Become a qualified instructor!
• Immunology
• Infection
SATURDAY, FEBRUARY 5, 2022 • Integument (Skin)
• Neurology
Fundamental Critical Care Support: Crisis Management New! • Obstetrics
• Patient and Family Support
Master Class: Cardiovascular Physiology • Pediatrics
Half-day course • Pharmacology
• Procedures
Master Class: Saving the Kidneys New! • Professional Development
Half-day course • Pulmonary
• Quality and Patient Safety
Advanced Critical Care Ultrasound: Adult* • Renal
(select morning or afternoon course)
New!
• Resuscitation
• Sepsis
• Shock (Non-Sepsis)
*Skill stations only. The session content will be provided via self-directed course.
• Trauma
Attendees should complete the self-directed course before attending the skill stations.
• Year In Review
FOR A MORE DETAILED
FOR COMPLETE DETAILS ON THESE COURSES, LIST OF PROGRAM TOPICS
PLEASE VISIT SCCM.ORG/CONGRESS2022. AND SESSIONS, VISIT
SCCM.ORG/CONGRESS2022.
10 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869= TICKETED SESSION REQUIRING ADVANCE REGISTRATION.
= FEE REQUIRED TO ATTEND. SEE REGISTRATION DETAILS AT SCCM.ORG/CONGRESS2022.
HOTEL ACCOMMODATIONS AIR TRAVEL
Take advantage of discounted Congress hotel rates by SCCM has arranged for discounted airfare of up to 10% off with United
making your reservation through the SCCM Housing Bureau. Airlines and Delta Airlines for travel to San Juan, Puerto Rico, for the 51st
All reservations are subject to availability. Critical Care Congress.
The deadline for booking at discounted
SCCM rates is Friday, January 7, 2022. United Airlines
Visit sccm.org/congress2022 to make your Website: united.com
reservation. By phone: +1 800 426-1122
By email: groupmeetings@united.com
Discount Booking Code: ZK4D830186
Congress Headquarters Hotel
Caribe Hilton Please note: When booking online, select “Advanced search” to find the offer
1 San Geronimo Street code field. Booking by phone or email may incur an additional service fee per
San Juan, Puerto Rico ticket. Such service fee is nonrefundable and applies to all itineraries, one-way
or round-trip. Please allow 24 hours for email requests to be processed.
Set on 17 acres of lush tropical gardens, the ever-iconic
Caribe Hilton is a paradise resort destination located just seven
Delta Airlines
miles from Luis Muñoz Marín Airport and a short distance from
Website: delta.com
historic Old San Juan, the lively Condado district, and the
By phone: +1 800 328-1111
Puerto Rico Convention Center. Guests are welcomed through
Discount Booking Code: NMUY3
an expansive open-air lobby and will enjoy colorful guest rooms
inspired by this island of enchantment. Birthplace of the famous
piña colada, an oceanfront pool complex, exclusive beach,
full-service spa, and choice of 11 dining options, provide a
delightful respite right on the property. CAR RENTAL
SCCM has negotiated special car rental rates for Congress attendees.
Enterprise National
Website: enterprise.com Website: nationalcar.com
Phone: +1 800 736-8222 Phone: 1-877-222-9058
Promotion Code: XZP1SCC Promotion Code: XZP1SCC
CHILDCARE SERVICES
SCCM has secured complimentary childcare services through KiddieCorp.
Children aged 6 months to 12 years can attend KiddieCorp at the Sheraton
Other Official Congress Hotels
Puerto Rico Hotel & Casino in San Juan, Puerto Rico, on a first come, first-
Condado Plaza Hilton served basis. Space is limited.
DoubleTree by Hilton San Juan
Childcare services will be available during the following times:
Fairmont El San Juan Hotel Sunday, February 6, 2022 6:00 a.m. – 10:00 p.m.
Royal Sonesta San Juan Monday, February 7, 2022 6:30 a.m. – 10:00 p.m.
Tuesday, February 8, 2022 6:30 a.m. – 10:00 p.m.
San Juan Marriott Resort & Stellaris Casino
Wednesday, February 9, 2022 6:30 a.m. – 5:00 p.m.
Sheraton Old San Juan Hotel
Sheraton Puerto Rico Hotel & Casino For more information, visit sccm.org/congress2022 .
Verdanza Hotel
SCCM.ORG SUMMER 2021 // CriticalConnections // 1151st CRITICAL CARE CONGRESS
FEBRUARY 6-9, 2021 • SAN JUAN, PUERTO RICO • SMART EVENT
Come together with the critical care community for the Society of Critical Care Medicine’s (SCCM) 51st Critical
Care Congress and dive into the latest knowledge and research.
SCCM offers a smart event experience with flexible learning options. Experience a Congress like never before.
In Person: Online:
• Learn live in person, February 6-9, 2022, in San • Learn as your time permits on an easy-to-use
Juan, Puerto Rico platform
• Receive a unique, high-quality educational • Receive an efficient, high-quality educational
experience while building relationships and experience perfect for busy professionals and those
networking, learning from peers, and interacting who cannot get away
with world-renowned thought leaders • Save on travel costs while still earning continuing
• Immerse yourself in the local island culture with education credit
plenty of opportunities to unwind, have fun, and • Access programming from anywhere for one year
gather with friends
Decide at any time. Both formats include On Demand access for one year and the opportunity to earn continuing
education credit.
The critical care community has made an incredible impact on the world. SCCM looks forward to recognizing
these key accomplishments and the opportunity to reconnect with our members, colleagues, and friends.
Register today to receive the best rates! Visit sccm.org/congress2022
© 2021 Society of Critical Care Medicine
The Society of Critical Care Medicine, SCCM, and Critical Care Congress are
registered trademarks of the Society of Critical Care Medicine.Critical Care
ECHOCARDIOGRAPHY
Review Course
November 9-11, 2021
OLC Education & Conference Center
Rosemont, IL
SCCM offers a smart event
experience with flexible learning
options. Attend in person or
Sara Nikravan,
access the programming online
Cochair
from anywhere.
Michael J. Lanspa,
Held in partnership between the Cochair
Society of Critical Care Medicine
and the American Society of Course benefits include:
Echocardiography, the Critical • Preparation for the critical care
Care Echocardiography Review echocardiography board examination
led by highly skilled multiprofessional
Course will educate attendees in
faculty
all aspects of echocardiography
• Valuable information for staying up to
for critically ill patients and will
date on the latest in team-based care
prepare attendees for the critical and ultrasound and echocardiography
care echocardiography board education
examination offered by the National • Access to published guidelines, expert
Board of Echocardiography. The consensus, and evidence-based
course is intended for critical care recommendations
practitioners who are already • CE/Accredited Continuing Education
familiar with ultrasound and (ACE)* and MOC available
echocardiography.
*formerly Continuing Medical Education (CME)
Register early to secure your spot and receive the lowest rates. For more information
and to register, visit sccm.org/echoreview.President’s Message
COVID-19: A Clinical Issue
4 to 12 weeks after the onset of COVID-19) or
the post-acute sequelae of COVID-19 (PASC)
or long COVID, that describe individuals with
signs and symptoms that persist beyond 12
With Lasting Effects
weeks from the acute infection or illness.
PASC may involve any organ system and also
includes other late sequelae of SARS-CoV-2
infection besides persistent symptoms, such as
the delayed syndromes known as multisystem
An exploration of post-COVID, post-acute sequelae inflammatory syndrome in adults (MIS-A) and
children (MIS-C).1
of COVID-19, and post-intensive care syndrome Together, the post-COVID syndromes include
a variety of symptoms that can last weeks or
months after the initial infection or illness or may
THE NOVEL SARS-COV-2 CORONAVIRUS AND THE GLOBAL appear as new problems weeks after the initial
COVID-19 PANDEMIC ARE THE CLINICAL ISSUE OF THE infection. PASC, identified by the persistence of
YEAR, OF THE DECADE, and very possibly (hopefully) will symptoms several weeks after the initial illness,
be the major clinical issue of the 21st century. COVID-19 has occurs in 30% to 70% of people who develop
affected people on all continents and challenged healthcare in COVID-19, with rates as high as 90% at 2 months
every country, with critical care medicine being among the most after COVID-19.2 PASC is most strongly predicted
impacted professions. As critical care professionals, we are very by the presence of chronic comorbidities and ad-
familiar with COVID-19. We know that about 1 in 5 individuals vancing age and may be more common in people
infected with SARS-CoV-2 who develop symptomatic COVID-19 of color, and it appears to be more common in
will be hospitalized, and that 1 in 4 of these hospitalized patients those who experienced symptomatic COVID-19
Greg S. Martin, MD, MSc, may become critically ill and require care in an intensive care unit versus asymptomatic SARS-CoV-2 infection.3-5
FCCM, is professor of
medicine, master clinician, (ICU). The most common forms of critical illness with COVID-19 The most frequent symptoms of long COVID
and executive associate are manifestations of infection-related organ dysfunction, making are fatigue, dyspnea, “brain fog,” cough, chest
division director in the COVID-19 a viral form of sepsis, with patients often experiencing pain, joint or muscle pain, headache, dizziness,
Division of Pulmonary, acute respiratory distress syndrome (ARDS), coagulopathy, acute depression, anxiety, and loss of taste or smell. It
Allergy, Critical Care and
Sleep Medicine at Emory kidney injury, encephalopathy, and shock. is noteworthy that prior coronavirus epidemics
University in Atlanta, such as severe acute respiratory syndrome and
Georgia, USA. Dr. Martin Post-COVID, Long COVID, and Post-Acute Middle East respiratory syndrome identified
also serves as research Sequelae of COVID-19 frequent persistence of symptoms or decrements
director for the Emory
Critical Care Center and Long COVID is the term used to describe signs and symptoms that in long-term health,6 while brain fog and other
as chair of the Critical continue or develop after the acute phase of SARS-CoV-2 infection neuropsychiatric sequelae of severe viral in-
Care Committee at Grady or COVID-19 illness. Acute COVID is limited to the first 4 weeks of fection were reported after the 1880s and 1918
Memorial Hospital in Atlanta. infection, while the post-COVID syndromes encompass two groups, influenza pandemics.7 Importantly, PASC or long
@SCCMPresident
either with ongoing symptomatic COVID-19 (generally between COVID may be more common in people who
14 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869References and disclosures:
see page 45
experienced the more severe forms of COVID-19 improve outcomes not just for COVID-19 but strategies that address the underlying causes
including critical illness.8 for all critically ill patients.1,15,16 The resources and manifestations.
we have for PICS are a valuable head start on In the meantime, patients will continue to
Post-Intensive Care Syndrome the post-COVID syndromes such as PASC.11,17 benefit from established evidence for how best
In the past decade, SCCM and the THRIVE to care for critically ill patients, and we must
initiative have made the post-intensive care The Path Forward redouble our efforts at delivering the high-
syndrome (PICS) part of our daily ICU vocab- We are fortunate to know much more about est-quality care to every patient. COVID has
ulary. 9-11 PICS is particularly common among COVID-19 now than we did a year ago, and challenged us to implement our core quality
those with acute respiratory failure requiring equally fortunate to know so much more about processes that improve survival and mean-
mechanical ventilation or circulatory shock, PICS than we did a decade ago. For patients with ingful outcomes for our critically ill patients,
with 3 out of 4 patients experiencing new or COVID-19 who experience critical illness, the such as the ICU Liberation Bundle (A-F).20 As
worsened impairments in physical, cognitive, similarities between PICS and long COVID are we have done with sepsis and for PICS, we will
mental health, or occupational functioning.12,13 unmistakable, and our experience with PICS develop the research and quality improvement
While many of the manifestations of PICS over- and the THRIVE initiative shines a light to show projects that guide the future for post-COVID,
lap with those of long COVID and PASC, the risk the path forward.9,18,19 We must: 1) increase our PASC, and PICS. The nature of critical care
factors have several similarities as well, such understanding of the pathogenesis of PASC and medicine to work collaboratively and deliver
as illness severity, chronic comorbidities, and of the group and individual manifestations team-based care lends itself to the creation
medications.14 The key now is to disentangle the of the post-COVID syndrome after critical of multiprofessional post-COVID clinics to
post-COVID syndrome to better understand illness; 2) determine the predictors of PASC, address the complex combination of physical,
PASC, as we do PICS—both the similarities and together and separately from PICS, and develop cognitive, mental health, emotional, spiritual,
differences. In the process, we will increase screening tools to identify patients at higher and other elements that provide indispensable
our understanding of both conditions and risk; and 3) develop prevention and treatment post-COVID care.21,22
TRANSFORM CARE WITH US
Join an organization united by purpose
Sound Physicians is seeking purpose-driven physicians and
advanced prac�ce providers to help transform cri�cal care
medicine in community hospitals throughout the country.
At Sound Physicians, you will benefit from:
• Career growth and flexibility
• A proven program focused on crea�ng value in the ICU
• Formal leadership development programs
• Comprehensive benefits package
Visit careers.soundphysicians.com
to view our current cri�cal care opportuni�es
SCCM.ORG SUMMER 2021 // CriticalConnections // 15Clinical Spotlight: Clinical Issues of the Day
Changing Patterns of Injury
Care of the Amid the emerging public health crisis of COVID-19, overall trauma
volume increased, and two major epidemiologic trends emerged in
the care of injured patients during 2020 and 2021—marked increases
Critically
in gun violence and traffic injuries. Observational data from large
urban centers revealed an increase in firearm injuries early in 2020.1,2
By year-end, the increase in gun violence had become stark. New
York City Police recorded a 97% increase in shootings during 2020
Injured Patient
(over 1500 victims), 2 and Chicago shootings increased 35% (4033). 3 A
preliminary analysis of 2020 data from 800 U.S. trauma centers that
submit injury and outcome data to the Trauma Quality Improvement
Program (TQIP) revealed an increase in trauma volumes overall, a
sharp rise in the percentage of patients sustaining a firearm injury,
and an increase in injuries associated with alcohol.
Trends Expected for 2021 and Beyond Firearm injury and mortality data are difficult to trend nationally
because of federal restrictions on funding and research. The inde-
pendent data repository gunviolencearchive.org has tracked firearm
statistics since 2013 using open-source, database-driven reporting
D
from state and national sources. Their data show a nearly 25% in-
uring the COVID-19 pandemic, overwhelmed hospital crease in gun-related homicides in 2020 (3955 additional victims,
systems required intensivists of all specialties to care totaling 19,402 victims). 4 Furthermore, this trend in increased gun
for critically ill patients with COVID-19. All types of violence has continued as we entered the summer of 2021.
patients treated and admitted to hospitals had signif- Paradox ica lly, t raf f ic fata lit ies rose 7.2% overa ll during 2020
icant variations from baseline. As part of statewide, regional, and according to the National Highway Traffic Safety Administration
national systems, trauma centers use an all-hazards approach to (N H TSA) stat ist ics despite fewer overa l l d r ivers on t he roads,
disaster preparedness and are poised to respond to situations such as work-from-home orders, and prolonged lockdowns. The t ypes of
pandemics. This article covers trends and care of injured patients in vehicular crashes during the pandemic changed, with increased
the United States during the pandemic as well as a look into possible single-vehicle crashes (up 9%), rollover crashes (up 9%), passenger
trends for the future. ejection injuries (up 20%), and alcohol-related accidents (up 9%)
16 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869References and disclosures:
see page 46
over the previous year, coupled with less frequent use of seat belts allowed it to adapt to deliver time-sensitive critical care while trauma
(down 15%). 5 Likely contributing to these shifts is an increase in volumes dipped during the initial surge in spring 2020.
impaired operation of vehicles. An observational study from NHTSA As of mid-June 2021, the Extracorporeal Life Support Organization
showed that there were statistically significant increases in traffic (ELSO) reported a total of 7223 COVID ECMO runs, with 4550 in
injuries and deaths involving alcohol, THC, and opioids (especially North America, and an additional 1644 in Europe and the rest of
fentanyl) after March 2020. 6,7,8 the world. The current survival rate to discharge is 51%. To date, at
T he soc ia l deter m i na nt s cont r ibut i ng to i nter persona l g u n the Shock Trauma Center, more than 400 V V ECMO consults were
violence, substance abuse, and traffic crashes are vast and varying. triaged, with nearly 100 patients having received ECMO therapy
The prolonged lockdown only served to uncover the stress fractures for COVID-19, the most in the United States. The current survival
underlying the disrupted American societal norms. Strictly enforced rate to hospital discharge is 67%. At the peak of the COVID-19 surge
home quarantines caused isolation from family and social contacts, in May 2020, 29 patients were on ECMO at a single time at UMMC.
rapidly rising unemployment revealed food insecurity and resource “We were able to rapidly get the right patient to the right place
scarcity, homelessness subsequently rose, insecurity caused a surge in the right amount of time. In the final analysis, we made a clear,
in firearm sales, and lack of access to mental health services caused unwavering commitment to do whatever was necessary to provide
destabilization and desperation. Compounded by continual fear of care for the sickest of the sick and then delivered on that commit-
an emerging pandemic disease and a polarized media landscape ment,” said Thomas M. Scalea, MD, MCCM, physician-in-chief of
spread i ng of ten-con f l ic t i ng na r rat ives to t hei r c apt ive home the R. Adams Cowley Shock Trauma Center.
audiences, changes in risk tak ing-behav ior and desperation are
not surprising. As the COVID-19 pandemic recedes and America Preparing for the Future
reopens, the trends in injury epidemiolog y will likely continue to Following lockdowns implemented in many U.S. states, injury vol-
change in unexpected ways. umes temporarily decreased but then emerged at high levels in 2020.
Injury volumes in 2021 continue to surpass those of 2020 overall,
Trauma Centers Step Up in a Crisis with violence-related and vehicular injuries remaining high. Along
Trauma centers form the backbone of disaster preparedness. On w ith COV ID-related hospitalizations declining since early 2021,
any given day in the United States, mass casualty events cause an increasing vaccination rates have allowed many locales to reopen
unexpected surge of patients—whether due to gun violence, motor to pre-COVID activity. It remains to be seen whether we will witness
vehicle collisions, natural disasters, or other incidents. Trauma an additional surge in COVID-19 hospitalizations. In the meantime,
centers and the personnel who contribute to the care of injured it is important that we develop best practices to prepare for the next
patients—trauma surgeons, emergency physicians, intensiv ists, local, regional, national, or worldwide disaster. The adaptabilit y
advanced practice prov iders (APPs), nurses, pharmacists, respi- and preparation of trauma centers and trauma systems involving
ratory therapists, and others—stand ready for a potential disaster multiple trauma and non-trauma center hospitals is uniquely struc-
from the moment they arrive at the hospital each day. Thus, it only tured to care not only for injured patients but also for adults and
makes sense that many trauma centers have been at the forefront children who require care as a result of potential future man-made
of the COVID-19 pandemic. and natural disasters.
An example of a trauma center’s ability to adapt and surge is the
R. Adams Cowley Shock Trauma Center at the University of Mary-
land Medical Center (UMMC) in Baltimore, Mar yland, USA. The
Program in Trauma was at the forefront of the State of Maryland’s
COVID-19 response. With a robust regional trauma system serving
as the framework for the state’s critical care network, triage systems
were revamped to distribute patients across the 14-hospital network
based on resource availability, with only the most critically ill pa-
tients brought to the Shock Trauma Center.
The lung rescue unit (LRU) is a preexisting intensive care unit Luke J. Duncan, MD, is Daniel J. Haase, MD, Deborah A. Kuhls, MD,
(ICU) at the Shock Trauma Center that is dedicated to venovenous an associate professor of RDMS, RDCS, is an FACS, FCCM, is professor
emergency medicine and assistant professor of of surgery and assistant
extracorporeal membrane ox ygenation (V V ECMO). The LRU ex-
surgical critical care at emergency medicine and dean of research at the
panded to a 32-bed biocontainment unit (BCU) with capabilities for Albany Medical Center in surgery at the University Kirk Kerkorian School of
16 ECMO patients at a time. The critical care resuscitation unit, the Albany, New York, USA. He of Maryland School of Medicine at UNLV in Las
only ICU in the United States dedicated to the interhospital transfer is also chief of the Division Medicine. He is the medical Vegas, Nevada, USA. She is
of Critical Care in the director of the Critical also Chair of the Critical Care
of patients, also served a major role in the triage and resuscitation
Department of Emergency Care Resuscitation Unit Committee at University
of these patients. Medicine, medical director at the R. Adams Cowley Medical Center, Nevada’s
W hile the BCU was a collaborative effort by a multidisciplinary of the Extracorporeal Life Shock Trauma Center and only Level I Adult Trauma
team of individuals throughout UMMC, the trauma center’s surgeons, Support Program and associate program director Center and only Pediatric
medical director of LifeNet of the Surgical Critical Care Trauma Center in Las Vegas,
intensiv ists, APPs, nurses, and pharmacists primarily staffed it.
New York. Fellowship. Nevada, USA. @dakuhls
The Shock Trauma Center’s experience with disaster preparedness
SCCM.ORG SUMMER 2021 // CriticalConnections // 17Clinical Spotlight: Clinical Issues of the Day
Rural Rapid Response Team 34 at Starr County Memorial Hospital, September 2020.
The Rural Rapid
Response Team
T hroughout the COVID-19 pandemic, military medicine has
been called on to support medical personnel when the high
disease burden exceeded the hospital or medical system’s
capacity. The traditional military deployment plan is based
on trauma response with a stepwise increase in capabilities at higher
levels, referred to as echelons. Echelons 3 and above provide care at
the level of the intensive care unit (ICU). The initial military response
in March and April 2020 used these large echelon 3 level teams such as
How embedded Navy
the hospital ships USNS Mercy and USNS Comfort in Los Angeles and
New York as well as a large Army alternative care facility at the Jacob
K. Javits Center in New York. This article describes our experience with
teams provided COVID-19 the transition to the smaller embedded care response teams.
From June to July 2020, the number of positive COVID-19 tests in
response in small South Texas increased from 3000 per day to over 15,000 per day. ICUs and
hospital wards were overwhelmed. In addition to the outstanding work
Texas hospitals of healthcare professionals in Texas, contract agencies augmented
hospital staff. Support from the federal government was also requested,
so Federal Emergency Management Agency (FEMA) played a major
leadership role, but additional manpower was needed. The military
responded with a joint operation lead by U.S. Army North, which is the
military command in charge of all U.S. military land-based forces in
North America. Several teams provided embedded response in Texas,
18 \\ CriticalConnections \\ SUMMER 2021 +1 847 827-6869References and disclosures:
available at sccm.org/criticalconnections
including an Army 85-person urban augmentation medical response COVID-19 unit by building two sets of double doors surrounded by
team (UAMTF), Nav y 44-person acute care teams (ACT), and Nav y plywood and insulation. All 29 COVID-19 patient beds were full, and
seven-person rural rapid response teams (RRRTs). UAMTFs were 13 to 20 patients a day had ICU-level acuity, typically due to respiratory
capable of ICU-level care; their role was to support large hospitals failure requiring advanced support.
by setting up additional ICU capability in a previously ICU-capable The Navy RRRT 34 arrived in July with two ICU physicians, 10 ICU
hospital, essentially creating a hospital within a hospital. ACTs were nurses, and two respiratory therapists, who provided 24-hour support.
ward-level care units, and RRRTs created ICU capability in hospitals Over the seven-week course, the SCMH team cared for 189 patients with
with the most austere conditions. COVID-19, of which 114 met ICU criteria. There were 42 intubations,
142 ventilator days, 275 bilevel positive airway pressure days, and
RRRT Starr County Experience (July to September 2020) seven central lines and three chest tubes placed, with an overall 91%
One RRRT team of seven responded for both Eagle Pass and Del Rio, survival rate to transfer or discharge.
Texas. Two 14-member teams responded for Rio Grande City, Texas,
which was the most resource-limited site of the group. Rio Grande Resource-Limited Focus
City has a population of approximately 15,000 and is the largest city in The militar y has a long histor y of operating in resource-limited
Starr County, with a population of approximately 50,000. Starr County environments for trauma. On the battlefield, equipment, medication,
Memorial Hospital (SCMH) had 36 medical-surgical beds and no ICU staff, and time for medical interventions are all limited. Battlefield
capability. Historically, they transferred anyone with ICU-level acuity or disaster triage is based on a utilitarian ethical theory: perform the
to Hidalgo County, which is approximately an hour away and has greatest good for the group by spending resources on the critically
multiple hospitals with ICU beds. ill as opposed to the expectant or the walking wounded. During the
In July 2020, SCMH went from four inpatients to six to completely full RRRT response in Texas, each team created a site-specific battlefield
and they were unable to transfer any of them because the accepting triage script prospectively for the management of limited resources to
facilities were also over capacity. Overnight, SCMH created a 29-bed include disease-modifying experimental medications (e.g., remdesivir),
Table 1. Remdesivir Triage Script for Starr County Memorial Hospital, July 2020
Based on a rubric develop by Rural Rapid Response Team 34
Positive Neutral Negative
Age (years) < 55 55-65 > 65
Days after admission 1-5 5-10 > 10
Type of oxygen support HFNC, BiPAP NRB, SFM, NC Ventilated
Number of comorbidities 0-1 2 >3
Disease complications Low or no risk Moderate or no risk One or more complication
Disease severity (CFS) >6 4-5 1-3
Abbreviations: BiPAP, bilevel positive airway pressure; CFS, Clinical Frailty Scale; HFNC, high-flow nasal cannula; NC, nasal cannula; NRB, nonrebreather; SFM, simple face mask.
The views expressed in this Commander Michael J. Kavanaugh, MD, is a naval officer and infectious diseases/critical care physician who serves as
presentation are those of the the director of the Military Tropical Medicine Course. He also serves as associate program director for the Walter Reed National
authors and do not necessarily Military Medical Center internal medicine program. In 2020, he deployed as the Officer in Charge of Rural Rapid Response
reflect the official policy or position Team 34 with Expeditionary Medical Facility Lima under Task Force 46 to Rio Grande Valley, Texas, USA, in support of COVID-19
of the Department of the Navy, pandemic care. He is a member of the Society of Critical Care Medicine who is actively involved as a course director and
Department of Defense, or the consultant for both Fundamental Critical Care Support (FCCS) and FCCS: Resource Limited.
United States Government.
Captain Sean A. McKay, MD, serves as the consultant to the Navy Surgeon General for Pulmonary and Critical Care Medicine.
We are military service members. He is board certified by the American Board of Internal Medicine in internal medicine, pulmonary medicine, and critical care
This work was prepared as part of medicine. Captain McKay is also a diplomate of the American Association of Bronchology and Interventional Pulmonology and
my official duties. Title 17 U.S.C. is a member of the Murtha Cancer Center’s Thoracic Oncology Team at the Walter Reed National Military Medical Center in
105 provides that “Copyright Bethesda, Maryland, USA. In 2020, he deployed as the Officer in Charge of a rural rapid response team with Expeditionary
protection under this title is not Medical Facility (EMF) Lima under Task Force 46 to the Texas-Mexico border in support of domestic COVID-19 pandemic
available for any work of the operations.
United States Government.” Title
17 U.S.C. 101 defines a United Commander Joseph Zeman, MD, currently serves as the deputy director for medical services at Walter Reed National
States Government work as a work Military Medical Center in Bethesda, Maryland, USA. He is board certified by the American Board of Internal Medicine in
prepared by a military service internal medicine, pulmonary disease, and critical care medicine. He is the associate program director for the pulmonary and
member or employee of the United critical care medicine fellowship at Walter Reed. In 2020, he deployed as the Officer in Charge of a rural rapid response team
States Government as part of that with Expeditionary Medical Facility (EMF) Lima under Task Force 46 to Rio Grande Valley, Texas, USA, in support of domestic
person’s official duties. COVID-19 pandemic care.
SCCM.ORG SUMMER 2021 // CriticalConnections // 19Clinical Spotlight: Clinical Issues of the Day
equipment (e.g., ventilators), and staffing (e.g., ICU vs. ward nurses). care skills. Cardiac arrest carts were reformatted and rapid sequence
The triage scripts used previously validated COVID-19 risk assessment intubation kits were created to assist in standardizing COVID-19 care
models that estimated prognosis based on demographics, comorbidities, during emergency patient scenarios.
disease complications, and severity of disease at presentation. An Additional resource-limited innovations occurred with RRRT 1 in Del
example of a sample triage script for remdesivir is shown in Table Rio, Texas. When the team arrived at the hospital, RRRT 1 supported
1. By prospectively designing triage scripts for the use of equipment the hospital’s newly created 17-bed COVID-19 isolation ward and
and medications, the RRRT could transparently discuss resource 12-bed COVID-19 ICU. But there was a staff shortage because several
management and expectations with the native hospital staff and with staff members had tested positive for COVID-19. On review, the RRRT
patients’ family members during a stressful COVID-19 surge. determined that the staff required further training on PPE donning
In addition to creating triage scripts that the native hospital could and doffing procedures and that the wards were not negative pressure.
use for limited-resource management, one of the RRRT’s main missions The RRRT met with hospital leadership and environmental services
was to ensure that the hospital could sustain the care of patients with and were able to create isolated negative-pressure wards using plastic
COVID-19 after the military teams departed. Toward this goal, the mil- sheeting and duct tape, strategically removing certain windows, and
itary ICU nurses and physicians took time to teach the native nursing purchasing industrial fans at a local hardware store. This construction
and physician staff how to create and maintain an ICU. They wrote 16 was based on the recommendations set forth in the Centers for Disease
distinct site-specific standard operating procedures for the use and Control and Prevention and the State of Minnesota’s Airborne Infectious
maintenance of ventilators, vasoactive medications, patient feeding, Disease Management guidelines. The team also put together a nursing
and COVID-19 management. In addition, more than 10 training sessions skills fair on critical care processes, policies, and procedures and were
were provided on ICU care and COVID-19-specific considerations such able to train all of the staff caring for patients with COVID-19. With
as the donning and doffing of personal protective equipment (PPE). these changes and training, they were able to expand ICU bed capacity
Cardiac arrest team roles were assigned with combinations of native to 20, reduce COVID-19 exposures by 96%, and care for 160 critically
and visiting staff to ensure experience and sustainment of critical ill patients with COVID-19, with a survival rate of 70%.
eePrepared
Prepared
Prepared
Be Prepared
he
ethe
the
Society
Society
Take
Society
the
ofofCritical
of
Society
Critical
Critical
Care
of
Care
Care
Critical
Medicine’s
Medicine’s
Medicine’s
Care Medicine’s
online
online
online online
lal
cal
care
care
care
critical
fundamentals
fundamentals
fundamentals
care fundamentals
courses.
courses.
courses.
Purchase
Purchase
courses.
Purchase
aPurchase
aa a
directed
-directed
rected
self-directed
course
course
coursebybyby
visiting
course
visiting
visiting
sccm.org/fundamentals.
by
sccm.org/fundamentals.
sccm.org/fundamentals.
visiting sccm.org/fundamentals.
directed
cted
ectedcourse
Self-directed
course
course
highlights
highlights
highlights
course
include:
include:
include:
highlights include:
ntent
ontent
nt forfor
all
for
all
levels
• all
levels
Content
levels
of of
healthcare
of
healthcare
forhealthcare
all levels
professionals
professionals
of
professionals
healthcare professionals
ctive
ractive
teractive
learning
learning
•learning
Interactive
modules
modules
modules
learning
including
including
including
modules
lectures
lectures
lectures
including
developed
developed
developed
lectures
byby
critical
by
critical
developed
critical
care
care
care
experts
experts
byexperts
critical care experts
re-
ndand
and
posttests
posttests
posttests
• Pre-to to
assess
and
to
assess
assess
posttests
mastery
mastery
mastery
toofassess
of
educational
of
educational
educational
mastery
content
content
ofcontent
educational content
ME
E/CME
CME credit
credit
credit
• available
CE/CME
available
available credit available
EXPAND
EXPAND
EXPAND
YOUR
YOUR
YOUR
EXPAND YOUR
lf-Directed
irected
DirectedFundamental
Self-Directed
Fundamental
FundamentalCritical
Fundamental
Critical
Critical
Care
Care
Care
Support
Critical
Support
Support
Care Support CRITICAL
CRITICAL
CRITICAL
CARE
CARE
CARE
CRITICAL CARE
sches
es
critical
critical
critical
care
Teaches
care
care
knowledge
knowledge
knowledge
criticalincluding
care
including
including
knowledge
assessing
assessing
assessing
including
andand
and
managing
managing
assessing
managing
critically
critically
and
critically
managing
ill ill
ororill or critically ill or
® ® ®
KNOWLEDGE
KNOWLEDGE
KNOWLEDGE
®
FROM
KNOWLEDGE
FROM
FROM FROM
patients
dred
patients
patients
forinjured
for
the
for
thefirst
the
patients
first
first
2424 hours
24
hours
for
hours
the
of of
care
first
of
care
care
or
24or
until
hours
or
until
until
proper
proper
ofproper
care
consultation
consultation
orconsultation
until proper
cancancan
be
consultation
bearranged
bearranged
arranged
can be arranged YOUR
YOUR
YOUR
HOME
HOME
HOME YOUR HOME
OROROR
OFFICE
OFFICE
OFFICE OR OFFICE
lf-Directed
irected
DirectedFundamental
Self-Directed
Fundamental
FundamentalCritical
Fundamental
Critical
Critical
Care
Care
Care
Support:
Critical
Support:
Support:
Care
Obstetrics
Obstetrics
Obstetrics
Support: Obstetrics
specialized
sers
specialized
specialized
Offers
critical
critical
critical
specialized
care
care
care
education
education
education
critical
dedicated
care
dedicated
dedicated
education
to to
treating
to
treating
treating
dedicated
critically
critically
critically
toilltreating
ill
ororill or critically ill or
patients
dred
patients
patients
injured patients
Purchase
Purchase
Purchase
a aFundamentals
Fundamentals
aPurchase
Fundamentals
a Fundamentals
lf-Directed
irected
DirectedFundamental
Self-Directed
Fundamental
FundamentalDisaster
Fundamental
Disaster
Disaster
Management
Management
Management
Disaster Management Self-Directed
Self-Directed
Self-Directedcourse
Self-Directed
course
course
bybyvisiting
by
visiting
visiting
course by visiting
pares
res
s clinicians
clinicians
clinicians
Prepares
with
with
with
thethe
clinicians
knowledge
theknowledge
knowledge
with
and
and
theand
skills
knowledge
skills
skills
necessary
necessary
necessary
andtoskills
to
provide
to
provide
necessary
provide
critical
critical
critical
to
care
care
provide
care critical care
onse
esponse
ponseto to
large-scale
to
large-scale
inlarge-scale
responsedisasters
disasters
todisasters
large-scale disasters
sccm.org/fundamentals
sccm.org/fundamentals
sccm.org/fundamentals
sccm.org/fundamentals
ororcontacting
or
contacting
contactingSCCM
or
SCCM
contacting
SCCM
Customer
Customer
Customer
SCCM Customer
lf-Directed
irected
DirectedPediatric
Self-Directed
Pediatric
Pediatric
Fundamental
Fundamental
Fundamental
Pediatric Critical
Fundamental
Critical
Critical
Care
Care
Care
Support
Critical
Support
Support
Care Support Service
Service
Service
atat+1
at
+1847
+1
Service
847
847
827-6888.
827-6888.
827-6888.
at +1 847 827-6888.
pares
res
s healthcare
healthcare
healthcare
Prepares
professionals
professionals
professionals
healthcare to to
assess
professionals
to
assess
assess
and
andand
manage
manage
tomanage
assess
critically
critically
critically
and ill
manage
ill
ororillinjured
or
injured
critically
injured
pediatric
pediatric
pediatric
ill or injured pediatric
ents
ts
forfor
the
for
thefirst
the
patients
first
first
2424 hours
24
hours
for
hours
the
of of
care
first
of
care
care
or
24or
until
hours
or
until
until
proper
proper
ofproper
care
consultation
consultation
orconsultation
until proper
cancan
can
be
consultation
be arranged
bearranged
arranged
can be arranged
ociety
ety
Society
of of
Critical
Critical
of
© Critical
2021
Care
Care
Society
Care
Medicine
Medicine
Medicine
of Critical Care Medicine
of
ciety
y of
Critical
Critical
of Critical
The
Care
Care
Society
Care
Medicine
Medicine
Medicine
of Critical
andandSCCM
and
SCCM
Care
SCCM
are
Medicine
are
registered
are
registered
registered
and trademarks
SCCM
trademarks
trademarks
are registered
of of
thethe
ofSociety
the
Society
trademarks
Society
of of
Critical
Critical
of of
Critical
Care
theCare
Society
Care
Medicine
Medicine
Medicine
of Critical Care MedicineYou can also read