Inside MedicalLiability - MPL Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

ILM Covers 4Q 2017 FINAL USE_Layout 1 10/27/17 11:41 AM Page 2
A PIAA PUBLICATION FOR THE MEDICAL PROFESSIONAL LIABILITY COMMUNITY
Inside Medical Liability
WWW.PIAA.US 2017 FOURTH QUARTER
Will
InsurTech
revolutionize
MPL?
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:02 PM Page 1
N
T.
Change your approach to record
retrieval and analysis with Ontellus.
Eight leading companies have merged to become Ontellus,
a revolutionary, nationwide online record retrieval partner
that empowers you to:
■ Accelerate cycle times ■ Focus on strategy
■ Improve outcomes ■ Achieve industry-leading,
SOC2 level security
Competitive advantage becomes yours through better-informed
decisions, faster turnaround and expedited case resolution.
Discover a whole new world of efficiency and data security at Ontellus.com.
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:02 PM Page 2
PERSPECTIVE
“ Rest assured, as we
approach 2018, PIAA is
working diligently to
P R E S I D E N T, B R I A N AT C H I N S O N
prepare for the future.
”
CHANGE AND DISRUPTION–
. RESPONDING TO A NEW ENVIRONMENT
T
hese are challenging—but in some respects, exhilarating— ance sector, relates the evolving saga of this growing niche market.
times for medical liability insurers and indemnifiers. The These developments have the potential to significantly change the
changing healthcare delivery system and liability environ- manner in which insurers cover risk and do business.
ment are creating uncertainty and the need for innovation Another feature in these pages discusses the complex issues at
like never before. Each organization must ensure it has optimal func- stake in dental imaging, and in particular those that involve the stan-
tionality today in its claims handling, underwriting, technology, and dard of care in a dental professional liability case. While this stan-
other key operations, knowing full well that external circumstances dard, like so much in healthcare, may be evolving, the author provides
may compel a new approach tomorrow. important guidance to help insurers and indemnifiers
The products and services these companies offer consider this critical component of any claim.
may need to evolve as well. This requires regularly You will also learn in this issue how one PIAA
updated information regarding customers’ preferences member, KaMMCO, offers a prime example of how to
and needs for their liability protections and risk take the initiative and embrace the changes in the
management. healthcare delivery system and the growing need for
Fortunately, there are opportunities for like-mind- more and better data. KaMMCO Health Solutions strat-
ed organizations to explore these issues, such as the egy is to innovate in the field of healthcare informatics
recently concluded PIAA International Conference in and quality reporting—and their experiences are prov-
London that focused on the theme of “Change and ing to be both fascinating and inspiring.
Disruption.” Attendees from 24 countries around the Finally, this issue features an analysis of recent
world heard that change and disruption are not unique to one loca- MPL claims. The data used in this analysis is derived from the 2016
tion; they are everywhere. The issues for insurers and indemnifiers PIAA Closed Claim Comparative, which summarizes data submitted
across the globe have become similar. We have found that what is by participating members in conjunction with PIAA’s Data Sharing
happening in one part of the world may well have already occurred Project. In addition to other key findings, the article identifies two
somewhere else—or may happen very soon. Consequently, the shar- salient trends: both the proportion of large claims and the cost per
ing of information and experiences among participants is among the large claim are increasing. The impact of these developments could
best ways for companies to learn and adapt in order to prosper. well be increases in premiums, as needed to cover the rising costs.
This issue of Inside Medical Liability focuses on a number of As this year draws to a close, we can look back on 2017 as a
topics that illustrate the power of change and disruption, and the year whose theme was “change and disruption” in the U. S. and
imaginative and successful ways that PIAA members and others have around the world. The worlds of healthcare and medical profession-
been responding to challenges and embracing change. al liability are exciting and challenging. Rest assured, as we
The cover story of this issue, about the rapidly evolving dynam- approach 2018, PIAA is working diligently to prepare for the future
ic of InsurTech products—innovations, business models, and apps and to help ensure that our members are well positioned for the
being created to revolutionize traditional business—for the insur- challenges ahead.
I N S I D E M E D I C A L L I A B I L I T Y 1 F O U R T H Q U A R T E R 2 0 1 7
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:02 PM Page 3
Inside Medical Liability
A PIAA PUBLICATION FOR
THE MEDICAL PROFESSIONAL
LIABILITY COMMUNITY
2017 FOURTH QUARTER
contents
22 33
Up
1
4
8
11
Front
Perspective
Events & Calendar
Observer
PIAA DSP Data Snapshot
Departments
12 Tech Talk
Planning for Data Conversions
By Martin Lippiett
17 Legislative Update
20 Case and Comment
When Do Claims Expire?
By Sarah Morse
46 International Perspective
Addressing Unsafe Rotas
29 36 By Liz Price
49 Interview with…
Pascale Carayon, PhD
54 As I See It
Carole Hemmelgarn
Features 57 By the Numbers
22 Cover story: InsurTech—Catching the Next Wave Has Fortune Turned Its Back on
MPL Insurers?
By Dr. Dietmar Kottmann and Dr. Nikolai Doerdrechter By Stephen J. Koca and Richard B. Lord
29 Feature: Dental Imaging and the Standard of Care 61 The Asset Side
The Shifting Sands of Central Bank
By Craig Fontaine Monetary Policy
By Peter Cramer, CFA
33 Feature: Evolution of a PIAA Company
64 Last Word
By Kurt Scott
36 Feature: Short-Duration Contracts—Loss Disclosures
By Magali Welch, Katie Glover, and Steve Merz
40 Feature: Will Severity Increases Finally Drive Premiums Higher?
By Timothy C. Mosler
“But behind the bright and shiny digital future, there are some lingering
questions for the industry. When it comes to MPL cover, how far is too far in the
individualization and real-time adaptation of policies?”
—Cover story
I N S I D E M E D I C A L L I A B I L I T Y 2 F O U R T H Q U A R T E R 2 0 1 7
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:02 PM Page 4
CHANGE IS COMING
D O YO U H AV E T H E R I G H T TO O L S TO
S U C C E S S F U L LY M A K E T H E L E A P ?
Delphi Medical Professional Liability provides insurance carriers
with the most advanced software solutions available today giving
them the power to:
• Significantly improve operational efficiencies
• Enhance levels of customer service
• A c h i e v e e n d - t o - e n d p r o c e s s i n g f o r t h e e n t i r e p o l i c y, c l a i m s , a n d f i n a n c i a l l i f e c y c l e
• A c h i e v e r e a l - t i m e a u t o m a t i o n , v i s i b i l i t y, a n d c o n t r o l o v e r o p e r a t i o n a l p r o c e s s e s
• Collaborate across the organization by providing timely and accurate information
W h a t ’s i n i t f o r y o u ?
• The flexibility to more quickly respond to changing market conditions
• The ability to link your business more directly to your customers’ needs
• A system platform built on modern technology and open architecture
providing the optimal environment for acquisition integration
L e t D e l p h i Te c h n o l o g y s h o w y o u h o w w e c a n t r a n s f o r m y o u r
critical business challenges into measurable business results.
F o r m o r e i n f o r m a t i o n , c o n t a c t u s a t D e l p h i - Te c h . c o m .
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:02 PM Page 5
COMING ATTRACTIONS
EVENTS & CALENDAR
■ 2018 Board Governance ■ 2018 Dental Workshop
Roundtable An Actuarial Look at Loss,
The Role of the Board in Mergers Premium, Expense, and Other Data
and Acquisitions Trends in Dentistry/Oral Surgery
When a company becomes involved in the In this session, Susan J. Forray, FCAS, MAAA,
mergers and acquisitions (M&A) market, its Principal and Consulting Actuary,
board of directors faces a unique set of chal- Milliman, will provide an overview of the
lenges and considerations through every stage of dental professional liability insurance market-
a potential transaction—from inception and place, as seen through the eyes of an industry
evaluation to execution and through integration. actuary. She will use data compiled from PIAA
What can board members do to ensure their carriers as the basis for an analysis and discus-
role in the deal process is optimized? And how can boards add value to sion of claims trends, including both frequency and severity.
minimize a deal’s risk? In this session, Victor Lopez-Balboa, Vice Ms.Forray will also provide key comparisons of loss experience
Chairman of the Global Financial Institutions Group and Global between dental and other medical professional liability coverages. In
Co-Head of Insurance, Goldman Sachs, will discuss why and how addition, other key data trends in dentistry/oral surgery will be
deals take place, and the different cycles that impact M&A activity. He discussed, including premiums and expenses.
will provide an overview of what is important to know, as a board
member, when it comes to M&A, and share a case study about a recent
deal that took place in the insurance sector. In addition, he will provide
key information on critical board responsibilities, how to evaluate M&A
opportunities, and the crucial questions directors need to ask, as a
board member, when it comes to M&A activity.
April 11-13, 2018 July 25-27, 2018 October 11-12, 2018
Marketing Workshop Underwriting Workshop Corporate Counsel
Loews Santa Monica Beach Hotel Westin Portland Harborview Workshop
Santa Monica, CA Portland, ME Portland Regency Hotel
Portland, ME
April 11-13, 2018 September 12-14, 2018
Dental Workshop Claims and Risk
Loews Santa Monica Beach Hotel Management/Patient Safety Future PIAA Medical
Santa Monica, CA Workshop Liability Conferences
March 14-17, 2018 Swissotel Chicago, Chicago, IL
May 16, 2018 May 15-17, 2019
CEO/COO Meeting Leadership Camp September 26-28, 2018 Marriott Portland Waterfront
Hyatt Regency at Gainey Ranch Waldorf Astoria/Hilton Bonnet Creek Technology, Human Portland, OR
Scottsdale, AZ Orlando, FL Resources, and Finance
(THRF) Workshop May 6-8, 2020
March 15-17, 2018 May 16-18, 2018 Omni Shoreham Hotel
Board Governance Grand Hyatt Washington
Medical Liability Washington, D.C.
Roundtable Washington, D.C.
Conference
Hyatt Regency at Gainey Ranch Waldorf Astoria/Hilton Bonnet Creek
Scottsdale, AZ Orlando, FL
I N S I D E M E D I C A L L I A B I L I T Y 4 F O U R T H Q U A R T E R 2 0 1 7
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 6
I WON’T STEAL
YOUR DATA.
Ransomware is rampant, affecting businesses in every
industry. And cyber criminals are increasingly targeting
small-to-midsize businesses as they know that many
lack the privacy controls and IT support of larger
organizations.
While state-of-the-art cyber insurance is an essential
component of your clients’ data security strategy, a
strong policy is only part of the solution. Cyber Liability
coverage from NAS Insurance includes expert pre and
post-breach services to help them prepare for, and
defend against, the criminals seeking to hold their
business hostage.
Visit the cyber experts at nasinsurance.com/cyber
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 7
Aon Benfield
The
POWER
PARTNERSHIP
of
When you seek new paths to success, you need a partner
that has a firm grasp of your business. At Aon Benfield, we
build the close relationships required to propel your firm
forward and gain a foothold in profitable environments.
Find out more at aonbenfield.com.
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 8
A
Achieve
chieve h
healthy
ealth
hy an
and
d
sust
sustainable
ainable gr
growth
owth
Medical Pr Professional
ofessional Liability insur
insurers
ers oper
operate
ate in a challenging en
environment
vironment wit
with
h
rrising
ising litig
litigation,
ation, managing capit
capital,
al, and g
growing
rowing ttheir ness. Aon Benfield’s
heir business. Benfield’’s
Healt hcare team
Healthcare team has the
the experience
experience and resources
resources to
to help our clients achieve
achieve
new and pr
new ofitable g
profitable rowth in evolving
growth evolving areas.
areas.
To lear
To learnn more, cont
more, act Da
contact vid Sulliv
David an at da
Sullivan vid.sullivan@aonbenfield.com
david.sullivan@aonbenfield.com
or visit aonbenfield.com.
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 9
NOTABLE NEWS AND TRENDS
OBSERVER
‘It’s All in How You Define It,’
Pennsylvania-Style
L
ike so many states, Pennsylvania is between a rock and a hard
place, budget-wise. But Democratic Pennsylvania Governor
Tom Wolf has said he’s optimistic that the Republican-con-
trolled legislature can produce a deal to patch a projected
$2.2 billion budget gap.
Wolf said he’s cutting “over $2 billion to streamline govern-
ment.” This includes hundreds of millions of dollars in “cost avoid-
ances” that might have materialized anyway, such as hundreds of
millions of dollars in transfers from a workers’ compensation fund
and a nonprofit organization created by state law in 2002 to offer
MPL insurance (this is the Medical Care Availability and Reduction of
Error Fund, otherwise known as “MCARE”). MCARE, controversial
from the get-go, has been providing a reliable stream of news for
years now. But every two years, the Pennsylvania Department of Especially toothsome in all this, though, is Governor Wolf’s
Insurance is required to reassess the need for it, as Pennsylvania euphemism for “tax increases”— the term “recurring revenue” is the
law mandates that the fund be closed at some point in the future, preferred usage; this refers to “a new source of money that provides
when market conditions permit. The news floodgate could close a reliable cash infusion every year”—in other words, tax increases.
at any moment. Source: The (Harrisburg) Sentinel, September 19, 2017
Remedies for Dull Lawyer Videos
Learn from the Texas Law Hawk!
F
or several years now, lawyers on the law firm’s practice page and cre-
have been bombarded by legal- ating separate versions for Facebook.
marketing companies assuring But obviously, that doesn’t solve the
them that video is the next big dullness problem.
thing. And yet, video hasn’t really yield- The best answer may be to crank
ed results for most lawyers. Even one of up the volume, and the hysteria, some-
the pioneers of the lawyer video, New what like Crazy Eddie with his famous
York MPL attorney Gerry Oginski, with “blow-outs” commercials for audio
his extensive video library, typically stereos, in the heady days of the 1980s.
attracts hundreds, rather than thou- For MPL, the current exemplar of this
sands, of viewers. tactic is Bryan Wilson, the self-
But maybe lawyers can maximize proclaimed “Texas Law Hawk.”
L AW HAWK viewership of videos, by posting items
like explanation videos (more popular
Visit YouTube to get a taste of
Wilson’s dynamic.
BRYAN E. WILSON ★ ATTORNEY AT LAW
than commercials), or putting videos Source: Above the Law, September 2017
I N S I D E M E D I C A L L I A B I L I T Y 8 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 10
Who(m) Do You Trust?
A credit-rating enterprise, Experian, is offering patient identifiers
T
he idea of unique patient identifiers is not new. But cred- claims that
it-rating firm Experian says it’s ready to take it beyond combination
just the idea phase. It’s offering to fix a years-long makes the
patient-safety problem by leveraging its expertise from match more
the financial sector. accurate than
Dan Johnson, Vice President of Strategy for Experian Health, deterministic matching.
notes, “If the payer uses the same unique identifier to identify Experian has worked with Congress on the Ensuring Patient
Dan Johnson, and a hospital is sending them a claim, it ensures Access to Healthcare Records Act, which removes the business
the accurate linking of the correct patient across enterprises.” associate status from clearinghouses, thereby allowing them to
Johnson said Experian’s wealth of credit bureau data makes use protected health information under HIPAA.
it the perfect private-sector innovator for patient IDs. “The credit To which we, with all due respect, would like to respond
bureau is really good at matching identity,” he said. The compa- with one rather troubling word about the putative safety of the
ny’s Universal Identity Manager, first released in 2016, relies on a Experian identifier system: Equifax.
combination of probabilistic and referential matching. Experian Source: Modern Healthcare, September 8, 2017
They’ve Already Got Room Service
Should hospitals be more like hotels?
A
ccording to Horst Schultze, a staff reasonable target.
writer at Medical Economics, “to Here’s what healthcare pro-
build trust with patients, physicians fessionals should be taking careful
need to take a page out of the hos- note of, Schultze says: “Ritz-Carlton
pitality industry’s playbook and do three things.” employees never greet guests with
First, Schultze says, doctors need to priori- ‘hi.’ Within nine feet of a guest
tize customer service and the patient experi- approaching, they smile, look the
ence. Like all customers, patients have some guest in the eye, and say, ‘good
fundamental expectations: Customers expect afternoon, Mr. Smith.’ This is not
the product to be free of defects. They expect only welcoming; it shows all guests they are Good medicine requires more physician face-
timeliness. And they expect their interaction to individually respected and valued. This warmth time with patients.”
be pleasant. Indeed, a satisfied customer, says permeates all interactions.” But just like every other hypothesis, we
Schultze, is one who walks away from an inter- Schultze asserts, “For doctors, that’s the say this one needs proof. And by the gold stan-
action that meets these expectations. But a key. The skills of diagnosing symptoms and dard: a randomized, double-blind study.
loyal customer is one who walks away from an offering treatments are not enough. Doctors Incoming patients enrolled in this (proposed) in-
interaction that exceeds these expectations, should also make patients feel cared for, which depth research would be randomly assigned to
because “their interaction was not just nice, it would make diagnosis and treatment easier.” a (group one) silver-tongued former employee of
was caring.” And, flying in the face of the notoriously New York’s Waldorf-Astoria hotel (MD degree
Schultze points out that (and this is not tight confines of what’s allowed by most health via an online med school) or (group two) a tire-
exactly news to most of us) “first impressions insurance policies, there’s this, “That’s why it’s somely nasty House, MD, clone.
matter.” After that, the benchmark for compar- unconscionable that the average time primary Clearly, this rigorous-type project
isons is set vertiginously high: It’s the Ritz- care doctors spend face-to-face with patients is deserves funding. Perhaps Ritz-Carlton has a
Carlton that’s invoked. Something like a 21 minutes annually. How can patients trust foundation?
Marriott, for example, might have made a more someone they only see for a few minutes? Source: Medical Economics, September 11, 2017
I N S I D E M E D I C A L L I A B I L I T Y 9 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 11
That flash of brilliance you see?
It’s doctors and health care
innovators uniting as a
powerful source for good.
Here, the dream
eam of healing the sick is as pure
pur as it ever was. Here,
e, the champions of the healers know they
they, too,
have a champion. Constellation is a growing
growing partnership of mutual liability insur
insurers
ers and health service companies.
ogether w
To
Together we’re stronger.. And together we’re
we’re embarking on a mission to change the futur
future of health care.
e about our vision, visit Constellatio
To learn more ellationMutual.com.IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 12
FORESIGHT
PIAA DSP
PIAA DATA SHARING PROJECT
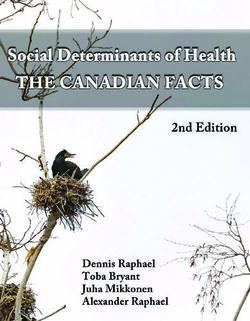
CARDIOVASCULAR DISEASE
In the PIAA Data Sharing Project, cardiovascular disease continues to be cited frequently among
patient outcomes leading to a claim or lawsuit. Approximately 7,000 claims and lawsuits closed
between 2011 and 2015 were identified, of which 26% paid $416 million in total indemnity, with
an average indemnity payment of $391,059.
For more detailed information, see the PIAA MPL Specialty Specific Series reports or contact P. Divya Parikh at dparikh@piaa.us.
© 2017 PIAA. All rights reserved. This page may not be reproduced or distributed without express written consent from PIAA.
I N S I D E M E D I C A L L I A B I L I T Y 11 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 13
TECH TALK
With the best of
intentions, some
BY MARTIN LIPPIETT
changes to the new
Planning for Data system will likely
occur throughout
Conversions
the life of the
project.
possible, and it will usually be on
the critical path of procedures
needed prior to going live with
the new system.
The plan should be realistic
about access to information on
the source of the data: Is it well
documented (it rarely is) and, if
not, are IT staff available to help
out with understanding the con-
tents and functionality of the
legacy system?
For initiation of the work,
the target software must be in a
fixed state. If the new system is
being designed or customized,
the conversion cannot be started
fully, because the work being
done makes the destination of
W
the data a moving target. With
hen an insurance company the old system may be looser, and the entity the best of intentions, some changes to the new
sets about the implementation relationship definitions in the new system may system will likely occur throughout the life of
of a new enterprise software not be compatible with those in the older lega- the project; the project plan should address
application, the question of cy application. But to the business users, how they will be coordinated with the
how to approach the transfer of data from the the data stored in the legacy system remains conversion.
old to the new software arises. In fact, a “data critical to their business functions and The method of balancing and validating
conversion” has to be planned as a separate decision-making. the conversion should be documented. In
and parallel exercise to the implementation of The planning process will need to identify, effect, this is a test plan. A common issue
the new software. among other things, the staffing requirements, occurs when reports from the legacy system
Data conversions are often the most com- the hardware and software that will be used, are used to balance against the new system;
plex and expensive components of a new sys- the test plan and test criteria, risk factors, and but they have filtering or other calculations
tem project, and almost without exception the change control. embedded in them, which means that they are
most risky and unpredictable task. The data not a 100% accurate representation of the
structure and complexity of the legacy system Steps in the process database.
are likely quite different from the new applica- It should be assumed that the process will be Is the data to be converted at a specified
tion being implemented, the type of database iterative, with each conversion revealing prob- point in time, so that the new software can be
may be different, the data integrity checks in lems and issues that must be dealt with before the system of record from that point forward?
another pass is made. For that reason—and This is the preferable way to do it—phasing
Martin Lippiett is Vice President of Business because every conversion has unknowns in the conversion is itself more complex, and
Consulting, Delphi Technology, Inc. it—the conversion should begin as early as requires that the company work with and
I N S I D E M E D I C A L L I A B I L I T Y 12 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 14
merge data from two systems until the process ■ Data is in the legacy system, but there is when the conversion is run.
is completed—not an ideal situation. no place for it in the new system. Perhaps the most critical decision con-
The plan must consider the various ■ Data is needed in the new system but is cerns which of the data should be converted,
dependencies within the insurance business. not available in the legacy database. Can the and this is where the business users’ opinion
Claims are events that happen under a policy, data be derived, or must it be entered? becomes important. Just because the data
so the policy conversion should be done before ■ The “same” data is present in more than exists doesn’t mean that it should be moved to
the data pertaining to claims. Name-and- one place in the legacy system. Which should the new system. There is a belief that if you
address records will be needed for creating be used? can convert one year of data, you can convert
policies, so they should be completed before ■ The usage and code structure of a particu- 20—the only difference is machine time. This
the policy conversion. If there is more than lar field is different in each system; for exam- is a fallacy; the more data there are and the
one source for the data, that adds complexity to ple, the legacy system may employ 80 codes for older it is, the greater the likelihood of anom-
the mapping and converting process, and it the various specialties, but the new system alies and errors that can bog down the process.
also has a bearing on dependencies. And if uses 120. In thinking about what to convert, consider the
there are plans to make other infrastructure These and many more questions will arise following questions:
changes (e.g., new hardware, new operating that cannot be answered by IT. Then, once the
system, or a new database) during the time question has been answered, the next decision ■ Is the legacy data consistent, going back
window of the conversion, the chain of will be about how to correct the data. There are through the years? If, for example, a prior con-
dependencies can become even more complex, generally two options: make corrections in the version was done 10 years ago, is the data prior
and also a risk factor. legacy system if that is possible (this is the pre- to that point in the same format and quality as
The user should be consulted throughout ferred approach), or do it in an outside source. the data after it?
the conversion project, for testing and for deal- An “outside source” might be an Excel spread- ■ What is the business- and regulatory-
ing with questions as they arise. As data is sheet generated by IT wherein the anomalous based- need to retain the data? Paid receiv-
mapped from the legacy system to the new records are listed with enough information that ables have very little value after the few
software, many decisions will be needed to they can be identified and with sufficient space months, when they may be required to support
address what should be done in the event of to enter the required data. These spreadsheets an inquiry. Perhaps the company had a line of
scenarios like these: are then merged with the other incoming data business that was discontinued some years
MPL Expert Over 5,000 attorneys, paralegals, and
claims professionals accessed the
EWD in 2016
Witness Database
The MPL Industry’s First Choice for Their Defense
Attorneys Examination of Plaintiff Experts
Features include:
• Testimony on over 4,000 experts
• Over 7,000 transcripts
• Not just a transcript repository but focused analysis on the experts past testimony
• Analytics reports of the expert’s testimony “opinion” across all transcripts to
compare past testimony to the case you are working on right now
• Online access for all authorized users
• Order as many transcripts as needed at no additional cost
• Flat monthly fee which covers all of your defense attorneys, paralegals, and claims
professionals for access to the database
What participating members have said:
• Paralegal – “It was wonderful and so easy to use. Thanks for the help.”
• SVP Claims – “This is well on its way to becoming the premier medical malpractice
defense expert witness database in the world.”
• Attorney – “Thank you so much. I really appreciate your help.”
• Paralegal – “Wow, thank you.”
For an online Internet demo which takes only 30 minutes,
contact dcostello@secondchair.com or call 239 410 5797
I N S I D E M E D I C A L L I A B I L I T Y 13 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 15
TECH TALK
Just because
ago. Is that data needed? the data
■ How far into the future do policy records exists doesn’t
need to be preserved to support late-reported
claims and other transactions? And is there a mean that it
way to add policy data for the rare late claim should be
that may come in instances when there is no
converted policy for it?
moved to the
■ Does the business require separate records new system.
for each and every claim payment and reserve
transaction, or can they be aggregated by
month, by quarter, or by year—depending on Migration occurs at a point in time when weeks; that underscores the need for a thor-
what reporting needs they have to support? all of the testing has been completed and the ough job of data mapping and cleansing, and
■ Is there a data warehouse that can be used conversion process is deemed ready for placing making a committed go/no-go decision when
to preserve some of the legacy data for which the the data into production. If the volume of data the conversion is done. It is also recommended
business cycle has been completed and is unlike- makes it possible, the ideal would be to freeze that a test migration be done beforehand to
ly to be needed for a transaction or an inquiry? input to the legacy system, say, on the Friday check everything as if it were being done for
If the data needed for reporting only can be evening of a three-day weekend, run the con- go-live, and also to get an idea of the timing of
warehoused, that generally is a simpler process versions, and balance the data in time for the the conversion process. And even with a well-
than converting it for doing a transaction. return to work. If this cannot be done, and the done conversion, it should not be surprising if
■ Is it more cost-effective to “convert” some legacy system must still be used, the data some data cleanups are needed during the first
data by manual entry? For example, for rate entered into it since the point of the conversion few months of using the new system.
tables or name-and-address records for some will need to be recorded and then reentered in
entities, it may be cheaper to manually enter the new system—a risky process. Few compa-
nies can revert to the old system after the con- For related information, see
the data than to write software for what is a
www.Delphi-Tech.com.
relatively small volume of records. verted data has been in production for days or
SOLUTIONS TO MEET YOUR NEEDS
SOLUTIO
US Premium Finance
hospitals of all sizes,
just your premium fin
We are committed t
• Increased flexi
your clients alm
credit cards, AC
• Hard cost elim
and collecting p
related issues re
• Competitive ra
Paul Lunney
Lunney,
y, SVP Director
Dire of Programs and National Accounts
PLunney@USPremiumFinance.com
PLunney@USPr emiumF | 215.498.2888
William J. V
Villari,
illari, Pr
President
BVillari@USPremiumFinance.com
BVillari@USPremiumFin
esi
| 678.985.5960
US PREMIUM
F I N A N C E
®
I N S I D E M E D I C A L L I A B I L I T Y 14 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 16
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 17
MARKET
LEADING
EXPERTISE
At JLT Re, our trusted team combines
market leading expertise and proprietary
analytical tools with the freedom to
challenge conventions. We create new
insights and explore innovative capital
solutions tailored to meet client needs.
UK & Europe • North America •$VLD3DFLĠF• Middle East • Africa
www.jltre.comIML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 18
LEGISLATIVE UPDATE
BY MICHAEL C. STINSON
PIAA Public Policy:
It’s Not All about Congress
A
t times, it must seem to some PIAA
members that the Association's
advocacy activities focus exclusively
on Congress. After all, as I noted in
a previous article about our Government
Relations Survey (“Helping PIAA to Help You:
The Biannual Government Relations Survey,”
Inside Medical Liability, Second Quarter 2017,
page 25), that's the number-one thing our
members say they expect from our public
policy efforts—to interact with Congress. As
a result, we are your eyes and ears on Capitol
Hill, with a full-time focus on making sure
that federal policies benefit your company, or
at the very least, don’t harm it. “Full-time, ”
however, doesn’t mean exclusive, and so we
work on many issues that are outside of the
congressional purview.
discussed. Through our newsletters and con- and revising the briefs to strengthen their
State legislation ference calls, we provide updates on hearings legal arguments, to simply providing a
Recently, PIAA has substantially increased its held on specific legislation, committee activi- national presence on a critical liability issue.
state legislative activity, recognizing that state ties, and votes. We also compile annual lists Once decisions are handed down, we review
legislatures play a more significant role in of relevant state legislation that has been and analyze the opinions, to help you deter-
insurance issues than Congress. One enacted, to help you keep up with what is mine how best to defend similar cases,
approach we take is to track and report on happening in other states. should they arise in the state(s) where you
legislative initiatives that could have implica- Once bills become law, however, we also do business.
tions beyond the state in which they are being track state judicial activities, to monitor the Beyond analysis, we also provide more
status of state tort reforms and other medical direct support, when requested, on behalf of
Michael C. Stinson is professional liability (MPL) related statutes. individual states’ legislative advocacy efforts.
Vice President of When invited by a member company, we also In recent years, we’ve coordinated with PIAA
Government Relations participate in amicus briefs. PIAA engage- members’ efforts to defeat no-fault-style leg-
and Public Policy at ment ranges from providing data to support islation, provided data to help enact damage
PIAA; mstinson@piaa.us. arguments made in the brief, to reviewing caps and other tort reforms, and created
I N S I D E M E D I C A L L I A B I L I T Y 17 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 19
LEGISLATIVE UPDATE
model legislation (most recently, to promote of our industry are protected.
“apology” protections and support prohibi- While the Federal The National Practitioner Data Bank
tions on “phantom damage” collections) to (NPDB) has long been a concern to many
provide a starting point for those looking to Insurance Office does not PIAA members, and thus PIAA has main-
enact new MPL laws in their state(s). tained close ties to the NPDB leadership. For
have any regulatory many years, PIAA served on the NPDB’s
NAIC/state regulation authority, it has been board (until the board was disbanded in favor
As any insurer knows, however, states’ regula- of a less formal, open communication process
tors can have a greater impact than their leg- charged with monitoring for NPDB stakeholders). Since then, PIAA has
islatures on MPL companies. PIAA regularly stayed in regular contact with NPDB—sub-
the insurance sector. As
engages with the National Association of mitting formal comments on proposed rule
Insurance Commissioners (NAIC) to stay on such, PIAA monitors the changes, inviting NPDB leaders to speak at
top of all the latest developments in the insur- workshops, and arranging meetings between
ance regulatory world. Some of this engage- agency and cultivates ties PIAA members and the NPDB hierarchy.
ment involves having a presence at NAIC to its staff to ensure that Other agencies have, only more recently,
meetings; monitoring committees, working begun work on issues relevant to PIAA mem-
groups, and task forces; and interacting regu- the inevitable mission bers, and PIAA has responded by engaging
larly with regulators and their staffs. them directly. The Agency for Healthcare
At other times, however, it’s critical for
creep will not encroach Research and Quality (AHRQ) was in the
PIAA to go deeper. One recent example of onto MPL issues. process of developing a Communication and
this is the NAIC’s MPL Working Group. Optimal Resolution (CANDOR) program to
As of late, the MPL Working Group has address MPL claims when PIAA intervened to
focused on state closed-claim reporting with the working group to develop a survey of address a number of concerns. Among PIAA’s
requirements. PIAA has utilized its expertise states with reporting requirements. We are recommendations were these: that insurers
in claims reporting (thanks to the PIAA Data hopeful that the results will help regulators should always be consulted when such a pro-
Sharing Project) to help advise the working gain a better understanding of whether or not gram is developed and/or implemented, and
group on key areas that need to be considered these reporting requirements actually result that flexibility was a key requisite to accom-
when addressing this issue. We’ve stressed in useful information for the states. modate local and regional differences in the
We also help address state-specific regu- delivery of healthcare. The final “tool kit” for
latory matters. Earlier this year, the Virginia such programs, as released by AHRQ, includ-
PIAA engagement ranges State Corporation Commission issued pro- ed those important concepts.
posed new rules regarding unfair claims-set- While the Federal Insurance Office does
from providing data to tlement practices. While the impetus for the not have any regulatory authority, it has been
change was allegedly to align the rules more charged with monitoring the insurance sector.
support arguments made closely with NAIC model acts, in reality, the As such, PIAA monitors the agency and
new proposal deviated from the models in cultivates ties to its staff to ensure that the
in the brief, to reviewing
numerous ways. Working with some of our inevitable mission creep will not encroach
and revising the briefs to companies in the state, we developed a set of onto MPL issues.
recommended changes to the proposed rules.
strengthen their legal In the end, the commission accepted several Conclusion
of our recommendations, thus changing Government relations extends well beyond
arguments, to simply pro- requirements for occurrence policies, provid- Congress; it encompasses the entire gamut of
viding a national presence ing more time to respond to a claim, and loos- governmental entities. For this reason, PIAA
ening the requirements for explaining a remains committed to interacting with gov-
on a critical liability issue. claim denial. ernmental organizations in all varieties and at
all levels of government. If there’s an aspect of
Federal regulations government that could affect your business,
that, before taking any action, the NAIC needs While the federal government doesn’t directly we are committed to addressing it, whether
to have a thorough understanding of what regulate the insurance industry, it can have a that means acting on your behalf directly, or
states are already doing in this regard, and significant impact on those providing MPL supporting your own strategic public policy
Superintendent Franchini of New Mexico (the coverage. Because of this, PIAA engages fed- initiatives. PIAA’s Government Relations
working group chair) has agreed. eral agencies in a variety of ways to ensure objectives are designed to reflect your needs,
With that in mind, we’ve worked closely that your voice is heard, and that the interests and we look forward to doing that.
I N S I D E M E D I C A L L I A B I L I T Y 18 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 20
IML 4Q 2017 FRONT _Layout 1 10/27/17 12:03 PM Page 21
CASE AND COMMENT
BY SARAH MORSE
When Do Claims Expire?
D
espite your policyholders’ best efforts
to provide conscientious care, they
may at some point find themselves
the defendant in a lawsuit. Even if
they have been involved in litigation before,
they will likely have many questions for their
attorney. One of the first they should ask, and
one of the first elements of a case every lawyer
will evaluate, is, “Has the statute of limitations
expired?”
Statutes of limitations are passed by legis-
latures and are written laws that establish a
time limit for a claimant to file a civil lawsuit. If
a claimant does not file suit before the expira-
tion of that time limit, he will be barred from
bringing the claim. The time limit for filing suit
depends upon: (1) the nature of the claim, and
(2) the date when the claim accrued, or came
into existence. The nature of a claim is impor-
tant because there are different time limitations the rendering or failure to render professional arises, or, in other words, on the date a
for different types of claims. The person bring- services by a health care provider” must be claimant sustains an injury, when the
ing suit, however, is not allowed to frame a per- brought within two years. (K.S.A. 60-514(c)) claimant learns of the injury, or when a
sonal injury claim as a contract claim merely to In Minnesota, however, a claim must be claimant should have discovered the injury.
avoid the time limitation. brought within four years. (M.S.A. § (See, for example, K.S.A. 60-513(c) (statute of
In the context of medical professional 541.076(b)) Some jurisdictions also have sep- limitations commences when “the fact of
liability (MPL), arate deadlines for filing wrongful death injury becomes reasonably ascertainable to
claims are frequently claims. In Maine, for example, a claim for the injured party.”); Fla. Stat. Ann. § 95.11
brought under theo- wrongful death must be brought within two (action must be commenced “within two
ries of medical negli- years, whereas claimants have three years to years from the time the incident. . .should
gence or wrongful make a claim for MPL, or professional negli- have been discovered with the exercise of
death. Statutes of gence. (Me. Rev. Stat. tit. 18-A, § 2-804 cf. Me. due diligence.”)
limitations for med- Rev. Stat. tit. 24, § 2902)
ical negligence and Determining the second element of the Exceptions—longer
Sarah Morse is wrongful death vary statute of limitations—the date when the time limits
with Goodell, by jurisdiction. For claim accrued—is not always a straightfor- There are circumstances, however, where the
Stratton, Edmonds example, in Kansas, a ward exercise. A cause of action accrues as statute of limitations time period may be
& Palmer, LLP. case “arising out of soon as the right to maintain a legal action tolled, or held in abeyance, meaning that a
I N S I D E M E D I C A L L I A B I L I T Y 20 F O U R T H Q U A R T E R 2 0 1 7IML 4Q 2017 FRONT _Layout 1 10/27/17 12:04 PM Page 22
plaintiff may file suit outside of the initial gence should have known, or received notice plaintiff filed suit contending that a doctor
deadline discussed above. There are three in writing of the existence of the injury or failed to diagnose her scoliosis at age 3, her
major instances where the statute of limita- death for which damages are sought in the case was dismissed pursuant to the statute of
tions may be tolled. action, whichever of such date occurs first, repose. (Bonin v. Vannaman, 261 Kan. 199,
First, the time limit for minors to file but in no event shall such action be brought 929 P.2d 754 (1996)).
suit is typically extended. If a claimant is a more than 4 years after the date on which Unfortunately, it is not always a straight-
minor when the injury occurs, he is typically occurred the act or omission or occurrence forward exercise to figure out when the
allowed to bring suit within some specified alleged in such action to have been the cause of statute of limitations will expire in any partic-
period of time after reaching the age of such injury or death. (735 Ill. Comp. Stat. Ann. ular situation. If healthcare professionals
majority. Second, fraudulent actions taken to 5/13-212) practice in a state that has a statute of repose,
deceive the patient from discovering the they may have some peace of mind to know
physician’s malpractice may also result in a Similarly, although Georgia’s MPL statute of that there is indeed a final end date after
tolling of the statute of limitations so the limitations is two years “after the date on which a claim may not be brought. If they
action does not accrue until the patient dis- which an injury or death arising from a negli- have questions about their state’s laws with
covers the fraud. Finally, if the statute begins gent or wrongful act or omission occurred,” it regard to statutes of limitation, they should
to run when the injury is reasonably ascer- is also true that, “in no event may an action contact their MPL insurer’s risk
tainable, it does not necessarily mean actual for medical malpractice be brought more manager or attorney to find out what the
knowledge of injury, but, rather, can mean than five years after the date on which the state’s limitations are.
when the claimant has the obligation to rea- negligent or wrongful act or omission Even if they know their state’s limita-
sonably investigate available sources to dis- occurred.” Ga. Code Ann. § 9-3-71. tions, physicians should always contact their
cover an injury. Unsurprisingly, there may For an MPL cause of action, the statute risk manager or insurer as soon as possible if
well be conflicting evidence as to when the of repose begins to run from the time the sued; they shouldn’t rely upon their own cal-
fact of injury became reasonably ascertaina- adverse event occurs, regardless of the negli- culations. An attorney will undoubtedly eval-
ble. In some instances, if there is conflicting gent doctor’s continued treatment of the uate whether the statute of limitations has
evidence about when the injury was ascer- patient. For example, although minors are expired, but will only have a short window
tainable, the question is submitted to a jury allowed to bring a cause of action for MPL of time for filing an answer to the petition
to determine when the cause of action within a certain time after reaching the age of and raising the issue on the healthcare
accrued. majority, the statute of repose bars an action professional’s behalf.
Healthcare professionals may feel that for MPL by or on behalf of a minor that is
with all of these exceptions, particularly with commenced more than eight years after the
the knowledge aspect, there is potentially no time of the act giving rise to the cause of For related information, see
www.gseplaw.com.
end to when a claimant may bring suit. Some action. Thus, in a case where an 18-year-old
legislatures have addressed this uncertainty
through laws known as “statutes of repose.” A
statute of repose is not related to the accrual
outtakes
of (knowledge of) a cause of action. Instead, a Value of Patient-Reported Outcomes
statute of repose bars a litigant from bringing
A
“
suit a fixed number of years after a particular s comfort
action by the defendant, even if the time with
period ends before the plaintiff has actually patient-
suffered any injury or knows about the
reported out-
claim.
For example, Illinois’ statute of repose comes (PROs)
reads: has grown, feed-
back has
[N]o action for damages for injury or death increasingly underscored that clinicians find collecting PROs
against any physician, dentist, registered
to be beneficial rather than burdensome. Evidence from
nurse or hospital duly licensed under the laws
of this State, whether based upon tort, or experienced users suggests PRO collection is not only feasi-
breach of contract, or otherwise, arising out of ble and good for clinical care but also may enhance physician
patient care shall be brought more than 2 satisfaction and prevent burnout.”
years after the date on which the claimant — New England Journal of Medicine, October 5, 2017
knew, or through the use of reasonable dili-
I N S I D E M E D I C A L L I A B I L I T Y 21 F O U R T H Q U A R T E R 2 0 1 7ILM 4Q 2017 Features _Layout 1 10/27/17 1:00 PM Page 1
C O V E R S T O R Y
BY DR. DIETMAR
KOT T M A N N A N D
DR . N I KOL A I
DOERDRECHTER
InsurTech–
Catching the
Next Wave
As insurers, we are no strangers to a
tightly competitive marketplace. But the
upside to intense competition is that, in
many instances, it motivates a culture
of innovation, as players scramble to
turn fresh thinking into ways they can
improve their business models.
N
owadays, a great deal of business transformation is fueled try merely experiencing a bump in the road? And if InsurTech players are
by technology advancements, known in our sector as going through a major shakeout, surely more successful new models are
“InsurTech.” This is the term used to describe the blending waiting in the wings? For medical professional liability (MPL) profession-
of new and multi-faceted digital technology with the insur- als, there are several clues that could help them stay ahead of the curve.
ance industry. At first glance, there is a myriad of InsurTech players, clambering
As expected, there has been a considerable buzz about InsurTech for market share and boasting of an enormous array of products and
among founders, investors, and incumbents. After a slower start, as services. This can be daunting for insurance professionals and their
compared with other industries, the InsurTech sector has seen some customers as well. To address this, in 2017 Oliver Wyman published a
serious investment since 2014, both financial and strategic. 2015 was report, “InsurTech Caught on the Radar: Hype or the Next Frontier?” in
the year of peak investment volumes and jaw-dropping “Z” mega-deals partnership with InsurTech investor Policen-Direkt.
(namely, ZhongAn and Zenefits), with deal numbers still rising well We took a structured and logical approach to assessing the global
into 2016 and 2017. InsurTech landscape, identifying a number of emerging industry pat-
Yet, there are distinct signs of the end of the honeymoon period, terns. This was achieved by painstakingly gathering data from more
with cracks starting to show. This year, several InsurTech players have fall- than 1,000 InsurTechs and other relevant players, such as FinTechs,
en short of their original plans, and others have found themselves strug- that are currently active within the insurance space. Some of our key
gling to gain traction. Is this the end of InsurTech hype—or is the indus- findings could offer some valuable insights for MPL practitioners.
Dr. Dietmar Kottmann is a Partner, Oliver Wyman, and Dr. Understanding the InsurTech universe
Nikolai Doerdrechter is Managing Director of Policen Direkt. Within the fast-moving world of InsurTech, there is no magic formula
I N S I D E M E D I C A L L I A B I L I T Y 22 F O U R T H Q U A R T E R 2 0 1 7ILM 4Q 2017 Features _Layout 1 10/27/17 1:00 PM Page 2
that will guarantee survival or success. The first wave of InsurTechs gen- Segment 3—“Operations.” In this segment, we looked at how players
erated a lot of activity, but little real disruption. This initial wave now have developed innovative offerings to operate insurance-based products
appears to be coming to an end. and services, covering new ways to enable and run insurance businesses.
We now anticipate a second wave of InsurTechs, which are savvier, Here we broke our findings down into five business model categories.
more creative, and no doubt more ambitious. They have the potential to Covering approximately 40% of InsurTech players in our database,
truly change the way insurers cover risk. The question is: how will the the activity level and strategic assessment of the companies in the
insurance industry respond? In our report we mapped players’ activity, Operations space are relatively well matched. Digital Sales Enablers
and organized them into 19 business model categories, within three appears to be the most overcrowded category in this segment. In con-
segments: Proposition, Distribution, and Operations. trast, the category “Underwriting” has more white space, and, therefore,
far less competition.
Segment One—“Proposition.” Today, as never before, organizations
are developing innovative offerings of insurance-based products and Movements in the InsurTech universe
services. Table 1 shows six business-model categories, and examples of InsurTech has fueled widespread change across the entire insurance
players that use these models. industry, but if you look at the results in context, some interesting pat-
When we crunched the numbers in our database, we found that terns emerge. In the overcrowded areas, one common factor is that
about a fifth of the total field of players are active within this segment. these resemble digital models that have worked in other industries.
Comparing activity level with strategic assessment, two categories Examples include e-commerce (intercepting customer searches),
(Situational and Community Based) appear to be overcrowded. launching digital versions of existing businesses, cutting large tradition-
Here, we expect to see a shakeout of players, possibly including the al businesses into digital pieces, or using digital communities.
demise of some well-known names. This represents the end of the These models clearly have their limitations for insurance, as insur-
first wave. ance typically offers low-interest products. Hence, business models that
Conversely, in the other three categories, From Insured to require active engagement from customers—known as “pull”—will
Protected, Risk Partner, and Digital Risk, we see a lot of white space experience challenges. This is a core problem for many of the models
remaining. This offers ideal ground for the new and ambitious con- copied from other industries, as they only work in the areas with active
tenders from the second InsurTech wave to gain traction. pull. Auto insurance is a good example of this.
Some similarities can also be seen in the areas with “white space,” i.e.,
Segment Two—“Distribution.” Reinventing how insurance-based room for growth. Here, they benefit from one of the most basic develop-
products and services are sold in the future will no doubt impact the ments associated with the digital revolution, namely, the evolution of suc-
bottom line. In this segment, we examined those business models that cessful business models from offering a product, to providing a function,
are taking advantage of new ways to sell products and services to con- and one step further to solving a real need. Take life insurance, for example.
sumers. Here we identified eight business model categories. While most of us are worried about risks in life, many people have a nag-
Players within the Distribution segment account for approximately ging doubt about whether these insurance products will really deliver what
40% of all the InsurTechs listed on our global database. Here, two cate- they need, in times of loss. Closing that gap in perception is a major preoc-
gories (Price Comparison Websites and Business to Consumer Online cupation for the second wave of enterprising models, which are now emerg-
Brokers/Value Comparison Websites) appear to be overcrowded. Again, ing. Their primary focus will be uncovering new ways to engage with their
we anticipate that a number of players will drop off the radar, as part of clients, thus evolving away from merely offering the classic insurance
a shakeout. In three categories (Affiliate Integration, Corporate “product.” Up to now, such high-engagement models have tended to be very
Platform, and Financial Partner), we believe there is still ample white employee intensive and hence very costly. Consequently, they were only
space; in other words, growth potential. available at the high end of the market. Through digitalization, these could
be opened up to the
mass market. Figure 1
Table 1. Business Models: Proposition shows some examples.
Current Strategic
Risk Model Tagline Example
Low Cost “We are the price leader for our target Microinsure; BIMA
Activity Level Assessment
What does
customers” this mean for
Situational “We provide instantaneous short-term Cuvva, MPL?
cover for your current needs” insuremyrentalcar.com
Community “We use community mechanisms to Teambrella, Banmahz, As a market sector, it is
Based lower the cost of sales or risk” Baobaoji well understood that
From Insured to “We not only insure you but also protect Oscar, Biovotion, eKincare
Protected you”
MPL is a type of insur-
Risk Partner “We not only provide insurance products, Getsurance, TikkR ance cover, with higher
but ensure you have exactly the right than average levels of
cover for your individual situation”
Digital Risk “We cover risks that come with digital Assurely, Cloudsurance customer engagement,
technology or digitally enabled models” as compared with
I N S I D E M E D I C A L L I A B I L I T Y 23 F O U R T H Q U A R T E R 2 0 1 7You can also read