FUTURESCAN Health Care Trends and Implications 2019-2024 - Northwell Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

FUTURESCAN
Health Care Trends and Implications
2019–2024
HEA LT H A DMINIST R AT IO N P R E SS
with support from CareTech Solutions
Futurescan 2019 COV.indd 1 12/31/18 3:10 PM
ABOUT FUTURESCAN 2019–2024
This is the latest in a series of publications for
health care leaders that the American Hospital
Association’s Society for Healthcare Strategy &
Market Development (SHSMD) in collaboration
with the American College of Healthcare Executives
(ACHE) has published annually since 1999.
In Futurescan 2019–2024, a panel of thought leaders
describe eight key trends affecting health care
organizations. Their expert insights are supported by
data from a survey of health care executives across
the country.
The Futurescan national survey, conducted in May
and June 2018, asked 1,452 hospital CEOs and leaders
from SHSMD’s membership their opinions about the
future trajectory of a variety of important issues. A
total of 180 responses were received, for a response
rate of 12.4 percent.
This publication is sold, or otherwise provided, with the understanding that SHSMD and ACHE are not engaged
in rendering professional services. If professional advice or other expert assistance is required, the services of a
competent professional should be sought. Opinions expressed in this publication are those of the guest authors
and do not represent the official positions of SHSMD, the American Hospital Association, ACHE, or Health
Administration Press.
© 2019 by the Society for Healthcare Strategy & Market Development of the American Hospital Association.
This book or parts thereof may not be reproduced in any form without written permission from SHSMD.
Printed in the United States of America.
ISBN: 978-0-87258-990-2
AHA order numbers: 127143 (single copy), 127144 (package of 15 copies)
ACHE order number: 2391
Society for Healthcare Strategy & Health Administration Press
Market Development A division of the Foundation of the
American Hospital Association American College of Healthcare Executives
155 North Wacker Drive, Suite 400 300 S. Riverside Plaza, Suite 1900
Chicago, IL 60606-1725 Chicago, IL 60606-16698
312.422.3888 312.424.2800
www.shsmd.org www.ache.org
Futurescan 2019 COV.indd 2 12/31/18 3:10 PM
FUTURESCAN
Health Care Trends and Implications
2019–2024
Introduction page 2
Leading Through Times of Change
by Ian Morrison, Ph.D.
1. Drug Crisis page 5
Agents of Change: How Hospitals and Health Systems Can Change
the Course of the Opioid Epidemic
by Michael Botticelli
2. Digital Health page 11
Flipping the Stack: Can New Technology Drive Health Care’s Future?
by Matthew Holt and Indu Subaiya, M.D.
3. Biotechnology page 17
Bioelectronic Medicine: Creating New Treatment Paradigms
by Chad Bouton
4. Value-Based Care page 21
Adopting the Attributes of High-Value Hospitals
by David S.P. Hopkins, Ph.D., Melora Simon, Thomas Wang, Ph.D.,
and Arnold Milstein, M.D.
5. Physician Aggregation page 26
Health Systems Partner to Grow Consumer-Driven Physician
Networks
by Amir Dan Rubin
6. Governance page 31
Reaching the Limits of the Governance Model
by James E. Orlikoff
7. Policy and Regulation page 36
The Future Role of States in Health Care Policy and Regulation
by Erin C. Fuse Brown, J.D.
8. Workforce page 41
Solutions to Workforce Shortages May Require Strategic Partners
by Susan Salka
Futurescan 2019 INT.indd 1 1/2/19 11:21 AM
INTRODUCTION
Leading Through Times of Change
by Ian Morrison, Ph.D.
A
s the nation’s medical system
goes through a period of
high uncertainty and disrup-
tion, Futurescan 2019–2024
brings together insightful experts and
thought leaders to prepare hospitals and
health systems for key trends that are
shaping the future of health care.
Drug Crisis
Michael Botticelli, director of the White
House Office of National Drug Control
Policy under the Obama administration,
is currently executive director of the
Grayken Center for Addiction at Boston
Medical Center.
In his article, Botticelli writes that
“the nation’s opioid epidemic is one
of the defining crises of our time and
requires a forceful response from every must be part of larger health care reform systems has revolutionized the business
sector. For hospitals and health systems, strategies, particularly those focused on sector, putting power and access into the
the epidemic forces an even stronger containing costs, improving medical hands of employees and customers and
sense of urgency given the magnitude outcomes, enhancing population health creating huge shifts in how transactions
of the problem and its intersection with and addressing social determinants of are done.” Holt and Subaiya observe
hospital services.” He says some hospi- health.” that health care organizations were
tals are successfully responding to the “latecomers to the enterprise technology
challenge through efforts such as the Digital Health game” and are now playing catch-up. As
following: Health care futurists Matthew Holt and technological advances accelerate, they
Indu Subaiya, M.D., focus on emerg- urge leaders to be prepared for the next
• Embracing nonopioid pain ing trends in digital health. Holt is the wave of change and its applications to
management practices. founder and publisher of The Health hospitals and health systems, including
• Enhancing the identification and Care Blog, cofounder of the Health 2.0 blockchain, artificial intelligence (AI),
treatment of patients with substance conference and a founding principal virtual reality and augmented reality.
use disorders (SUDs). of Health 2.0 Advisors. Subaiya is cur- Their article also takes us through the
• Incorporating SUD issues into payment rently executive vice president of Health likely focus of technology giants such as
and service delivery reform efforts. 2.0 and co-founder of Health 2.0: User Amazon, Apple and Alphabet/Google
Generated Healthcare. as they grow their presence and impact
Botticelli notes that “addressing They write, “The easy availability of in the field. Traditionally, the U.S. med-
the opioid crisis in the United States cloud- and mobile-based computing ical system has centered around care
About the Author Columbia, Canada. He is the author of sev-
Ian Morrison, Ph.D., is an author, consultant eral books, including the best-selling The
and futurist. He received an undergraduate Second Curve: Managing the Velocity of
degree from the University of Edinburgh, Change. Morrison is the former president of
Scotland; a graduate degree from the Uni- the Institute for the Future and a founding
versity of Newcastle upon Tyne, England; partner of Strategic Health Perspectives, a
and an interdisciplinary doctorate in urban forecasting service for clients in the health
studies from the University of British care industry.
2 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 2 1/2/19 11:21 AM
delivery, services and technology plat- on identifying hospitals that consistently that three-quarters of respondents are
forms, in that order. The authors invite provide high-value care—excellent qual- operating their network at a loss or are
us to “imagine inverting this triple-layer ity at a low cost. willing to do so to achieve broader stra-
stack and starting with technology plat- Their article highlights the results of tegic objectives.
forms.” In this scenario, trackers and AI the research, which revealed three sets of According to Rubin, health systems
systems would monitor and even suggest care delivery attributes that distinguish are pursuing these investments to attract
next steps to clinicians and patients to top-performing hospitals from their more covered lives to their networks;
improve the quality of care. peers: (1) thinking beyond the hospi- to deliver higher levels of service, access
Holt and Subaiya stress that it is tal stay, (2) cutting waste, not safety and value; and to prevent physicians
vital for health care leaders to under- and (3) engaging the frontline team and their patient bases from becoming
stand these technologies and trends in improving the cost-effectiveness of aligned with competing networks.
through learning and pilots and by needed care. One of the best ways to accomplish
engaging with clinical leaders in their The study found that hospitals are these goals, he says, is through part-
organizations. rapidly adopting these attributes in areas nerships, including affiliations, joint
where they have the greatest economic ventures, clinically integrated networks,
Biotechnology incentive, such as readmissions and epi- lease arrangements, management ser-
Chad Bouton is director of the Center for sodes of care. Stronger payer incentives vices offerings, cost-plus contracts,
Bioelectronic Medicine at the Feinstein will likely be necessary to increase adop- fee-for-service billing and capitated
Institute for Medical Research at North- tion of attributes that reduce hospital or accountable care organization–like
well Health and a renowned researcher occupancy. arrangements.
and developer of advanced biomedical
technology. Bouton explains in his arti-
cle how this exciting new field combines The articles by this year’s panel of experts
neuroscience, molecular biology and
bioengineering to tap into the nervous provide evidence-based insights designed
system to treat conditions involving
inflammation, such as Crohn’s dis- to help hospitals and health systems prepare
ease, lupus, rheumatoid arthritis and
paralysis.
for a range of strategic, market, policy, social,
He observes that while many of the economic and competitive challenges.
advances in bioelectronic medicine are
related to implantable devices, innova-
tions in wearable technology will also The authors conclude, “As payers Many providers, he adds, find that
play a major role in creating new ther- gradually increase rewards for yearlong these options can reduce capital burdens
apies and treatments. And he says dis- excellence in care delivery, hospital and and business risks because all partnering
coveries made in the lab are being made health system leaders will benefit from organizations commit resources and
possible by investors from industry who implementing best practices and bright management energy to the initiatives.
recognize bioelectronics as a growing spots in value-driven performance that
sector that will present alternatives to meet the needs of patients and health Governance
the biochemical therapies traditionally insurers alike.” James E. Orlikoff, president of Orlikoff
offered by Big Pharma to treat many & Associates Inc. and a renowned expert
diseases and conditions. Physician Aggregation on governance and the emerging health
In the future, Bouton believes this Amir Dan Rubin, president and CEO care environment, begins his article
branch of technology will continue to of One Medical, begins his article on by stating that the traditional gover-
expand, and we can expect rapid growth building physician networks through nance model “can no longer be taken
in the field that could greatly improve partnerships by emphasizing the rapid for granted” in “the rapidly changing
how we deliver care. pace at which health care organizations and radically challenging health care
are aligning with physicians. landscape.”
Value-Based Care He points out that in the latest He says hospital and health system
As part of their America’s Most Valuable Futurescan national survey of hospital boards are getting older: Since 2005, the
Care study, David S. P. Hopkins, Ph.D., and health system leaders, 76 percent of percentage of board members under the
Melora Simon, Thomas Wang, Ph.D., respondents say they are already growing age of 50 has declined. Furthermore,
and Arnold Milstein, M.D., of the their networks by more than 25 percent time demands on board members are
Clinical Excellence Research Center at or are likely to do so in the next five growing and are an increasing cause of
Stanford University have concentrated years. He says the survey also indicates complaint.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 3
Futurescan 2019 INT.indd 3 1/2/19 11:21 AM
Looking ahead, Orlikoff predicts states are stepping into the vacuum to take is driving problems related to hiring,
leaders can expect the following: action on a variety of health care concerns. retention, turnover, unit staffing and
She notes that the stakes are high scheduling, morale, quality of care and
• Recruiting and retaining qualified because rising medical expenses translate overtime costs. According to Salka,
board members will become more to increasing budgetary pressure for health care employment continues to
difficult. states, squeezing out other public priori- boom but still cannot keep pace with
• Effectively integrating members of the ties such as education and infrastructure. demand because of two leading drivers:
millennial generation and Generation X In response, states are focusing on three
into current governance models will be key issues: • An aging population that is
a growing problem. consuming more health care services.
• Leaders will experiment with new 1. Rising costs from consolidation. • The wave of retirements among baby
approaches to governance, with mixed 2. Drug price increases. boomer practitioners.
results. 3. Affordability for health care
consumers. To help resolve the crisis, she calls for
As the traditional model of gover- investment in modernizing the field’s
nance nears the end of its useful life, Fuse Brown concludes that the grow- human resources sector. Salka says pro-
Orlikoff says, “We must begin to con- ing role of states will mean more state- viders that use innovative best practices
ceptualize and then to experiment with by-state variation. Hospitals and health in recruitment and retention, coupled
new models that are relevant to a radi- systems will need to concentrate not with hiring outside health care staffing
cally different future.” just on health care policies at the federal experts when needed, is a formula for
level but also on a proliferation of state success in the escalating race for clinical
Policy and Regulation regulations that will affect their facilities, talent.
Erin C. Fuse Brown, J.D., an associate finances and delivery models.
professor of law and a faculty mem- Conclusion
ber of the Center for Law, Health and Workforce Futurescan once again identifies key
Society at the Georgia State University Susan Salka, president and CEO of AMN issues and emerging trends that demand
College of Law, provides an insightful Healthcare, leads the country’s largest an informed and planned response
perspective on the growing importance health care staffing and recruitment by health care leaders. The articles by
of the states’ role in establishing health company. In her article, Salka describes this year’s panel of experts provide
care policies and regulations. the industry’s unprecedented workforce evidence-based insights designed to help
Fuse Brown says that nearly a decade shortages across the country as one of the hospitals and health systems prepare
after the passage of the Affordable Care most critical issues facing hospitals and for a range of strategic, market, policy,
Act, political gridlock has made it diffi- health systems now and in the future. social, economic and competitive chal-
cult for the federal government to move She points out that the growing lenges and to guide them in taking the
forward with national reforms, while a deficit of qualified physicians, nurses actions required to be successful in the
renewed emphasis on state flexibility means and many other medical professionals ever-changing health care landscape.
4 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 4 1/2/19 11:21 AM
1 DRUG CRISIS
Agents of Change: How Hospitals and Health
Systems Can Change the Course of the Opioid
Epidemic
by Michael Botticelli
T
he nation’s opioid epidemic is
one of the defining crises of
our time and requires a force-
ful response from every sector.
For hospitals and health systems, the
epidemic forces an even stronger sense
of urgency given the magnitude of the
problem and its intersection with hos-
pital services. Our ability to address the
crisis depends to a large degree on how
well the health care field implements
evidence-based services, continues to
innovate and replicates emerging best
practices.
The stakes could not be higher. The
number of drug overdose deaths involv-
ing opioids has risen sharply since the
turn of the century, reaching more than
49,000 in 2017 (exhibit 1). The increase
in overdose deaths is a major contribu- from national survey information and outbreaks of HIV. In just over five years,
tor to the shocking decline in life expec- does not include homeless individuals or the number of new hepatitis C infec-
tancy in the United States over the past those who are currently incarcerated— tions reported to the Centers for Disease
two years (Xu et al. 2018). populations known to have high OUD Control and Prevention (CDC) has
In 2016, an estimated 2.1 million rates. nearly tripled, reaching a 15-year high
people aged 12 years or older met diag- In addition, needle sharing and the (CDC 2018).
nostic criteria for an opioid use disorder lack of access to sterile syringes associ- Another consequence has been a
(OUD) (SAMHSA 2017). This statistic ated with heroin and fentanyl use have marked increase in the number of preg-
may be a dramatic underestimation led to a dramatic increase in hepatitis nant women with an OUD. From 2004
because overall prevalence is derived C virus infections, as well as localized to 2014, the number of U.S. infants
About the Author
Michael Botticelli, one of the nation’s lead- Before joining ONDCP, he served as direc-
ing addiction experts, is executive director tor of the Bureau of Substance Abuse Ser-
of the Grayken Center for Addiction at vices at the Massachusetts Department of
Boston Medical Center. Previously, he was Public Health, where he expanded innova-
director of national drug control policy tive and nationally recognized prevention,
for the Obama administration. He joined intervention, treatment and recovery ser-
the White House Office of National Drug vices for Massachusetts. Botticelli holds a
Control Policy (ONDCP) as deputy direc- bachelor of arts degree from Siena College
tor in November 2012 and later served as and a master of education degree from St.
acting director. Botticelli has more than two Lawrence University. He is also in long-term
decades of experience supporting Ameri- recovery from a substance use disorder,
cans affected by substance use disorders. celebrating more than 28 years of recovery.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 5
Futurescan 2019 INT.indd 5 1/2/19 11:21 AM
FUTURESCAN SURVEY RESULTS
Drug Crisis
How likely is it that the following will happen by 2024?
Already Very Somewhat Somewhat Very
Happening Likely Likely Neutral Unlikely Unlikely
(%) (%) (%) (%) (%) (%)
30 28 24 12 4 3
Our organization will emphasize nonpharmacological pain management (e.g.,
acupuncture or cognitive behavioral therapy) to reduce opioid prescribing (e.g.,
number of prescriptions, duration or dosage) by physicians in our employment.
27 43 20 6 3 1
Our organization will expand the ability to diagnose patients who may have a
substance use disorder while integrating treatment into multiple health care
settings.
18 28 25 18 6 5
Our organization will integrate peers/recovery coaches into substance abuse and
treatment services or other services such as emergency departments.
13 24 28 21 8 6
Expansion of accountable care organizations will serve as a major driver for an
enhanced focus on substance use disorders among patient populations for our
organization.
16 30 28 17 6 3
Our organization will establish initiatives specifically to meet the needs of
employees or their family members addicted to opioids or other drugs.
Note: Percentages in each row may not sum exactly to 100 percent because of rounding.
What Health Care Executives Anticipate by 2024
• To decrease opioid prescribing by employed physicians, 58 percent of hospi-
tal and health system leaders either already are emphasizing nonpharmaco-
logical pain management alternatives or are very likely to do so.
• About two-thirds (65 percent) of respondents are at least somewhat confi-
dent that expansion of accountable care organizations will play a key role in
enhancing the focus on patient substance use disorders.
• Sixteen percent of leaders have established their own organizational initia-
tives to help employees or their family members addicted to opioids or other
drugs. Another 58 percent are somewhat or very likely to do so.
6 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 6 1/2/19 11:21 AM
Exhibit 1
Number of Deaths Involving Opioids
49,068
50,000 Total
Female 42,249
40,000 Male
30,000
20,000
10,000
0
14
15
na 16
10
11
12
13
02
03
04
05
06
07
08
09
7
01
20
20
20
20
io 20
20
20
20
20
20
20
20
20
20
20
l2
is
ov
Pr
Source: National Institute on Drug Abuse (2018).
—continued from pg. 5 in health care and criminal justice expenses, not
diagnosed with opioid withdrawal symptoms, to mention lost business productivity—nearly
known as neonatal abstinence syndrome, 2.8 percent of the gross domestic product.
increased 433 percent—from 1.5 to 8.0 per
1,000 hospital births (Patrick et al. 2015). How We Got Here
The emergence of inexpensive, highly potent The epidemic that now claims close to 140
synthetic drugs, such as fentanyl and its ana- lives a day grew out of a number of intersecting
logues, adds a heartbreaking level of severity dynamics. It took decades to develop, with
to opioid overdoses. From 2014 to 2016, the many historical factors combining to make con-
percentage of overdose deaths attributable to ditions ripe for this epidemic to flourish:
fentanyl increased from less than 20 percent to
almost 50 percent (CDC 2016). • A fragmented health care delivery system.
The impact of the opioid crisis on the health • An overreliance on arrest and incarceration at
care delivery system is staggering from both a both the policy and funding levels.
volume and a cost perspective. Hospitalizations • A lack of training among medical staff on
related to opioid misuse and dependence have substance use disorders (SUDs).
increased dramatically, with the rate of hospital • Inadequate reimbursement and insurance
inpatient stays per 100,000 population nearly coverage for SUD treatment.
doubling between 2000 and 2012. During • The pervasive stigma surrounding drug users.
that same period, opioid-related emergency
department (ED) visits increased by 99.4 per- As a result of these and other factors, only a
cent (Weiss et al. 2017). Because untreated very small percentage of those with an SUD
addiction is a major driver of overall medical receive care.
expenditures, hospitals and health systems have Historically, the country’s policies and
significant opportunities to identify and engage funding for dealing with the problem and its
people in treatment—not only to achieve better consequences focused heavily on reducing
outcomes for patients but also to reduce the global drug supply and on law enforcement at
large-scale financial burden. the federal, state and local levels. Until 2012,
The economic impact on our nation is public health approaches such as prevention,
also profound. A report by the White House’s early intervention and treatment were not high
Council of Economic Advisers (2017) has esti- priorities.
mated that opioid use in the United States is In addition, one of the early drivers of the
associated with more than $500 billion a year epidemic was the overprescribing of opioid
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 7
Futurescan 2019 INT.indd 7 1/2/19 11:21 AM
medications. According to the CDC, reported that they do not intervene OUD, hospitals have an opportunity
doctors wrote 72.4 opioid prescriptions when use of illicit drugs is detected. to make a major impact on reducing
per 100 persons in 2006. This rate Only 28.6 percent of family medicine morbidity and mortality related to the
increased 4.1 percent annually from residency programs have required addic- epidemic. The following examples illus-
2006 to 2008 and 1.1 percent annually tion medicine curricula (Friedmann, trate how some hospitals are responding
from 2008 to 2012. By that year, 259 McCullough and Saitz 2001). to the need.
million opioid prescriptions were writ- Until the Affordable Care Act and
ten in the United States—four times Medicaid expansion in some states Embracing nonopioid pain manage-
as many as in 1999. Although we have required an SUD treatment benefit, ment practices. Nora Volkow, MD,
seen an overall decrease since 2012, the lack of insurance was a major barrier director of the National Institute on
level of opioid prescribing still remains for many people seeking care. Com- Drug Abuse, has said that the overpre-
triple what it was in 1999 (Guy et al. pounding the problem, numerous scribing of opioids “started the fire.”
2017). public and commercial health plans had (Boston Medical Center 2018). It follows
From the beginning, one of the pri- implemented a variety of discriminatory that, to extinguish the fire, we must con-
mary obstacles in the path to stopping practices for SUD benefits that did not tinue to push for pain management strat-
the opioid epidemic has been the fact apply to other medical benefits. The egies that rely on nonopioid medications
that too few people with opioid addic- 2008 Mental Health Parity and Addic- and nonpharmacological approaches.
tion are receiving the help they need. tion Equity Act attempted to rectify These efforts go hand in hand with pre-
According to the National Survey on this inequity by requiring insurers to scription-monitoring programs for prob-
Drug Use and Health, only 10 to 14 offer mental health and SUD benefits lematic prescribing and reducing drug
percent of those with an SUD receive on a par with benefits for other medical diversion. Some states have laws that
treatment (SAMHSA 2017). Despite conditions. Despite enhanced regulatory limit doctors to prescribing a set course
the high prevalence of people with oversight and compliance efforts at both of opioids, but the hope is that the field
SUDs intersecting with the nation’s the state and federal levels, much work will take action ahead of the mandates to
health care delivery system, only 8 per- remains if we are to achieve full parity. adopt guidelines and standards that limit
cent of the referrals are coming from Doing so will significantly increase the prescriptions and promote alternative
health care settings. One major cause number of people who receive adequate pain management therapies.
of the low treatment rate is a lack of treatment. After researchers at Dartmouth-
clinical education in medical curricula Insurance carve-out arrangements Hitchcock in New Hampshire found
on the issue. A 2012 study on the gap for SUDs can also present a significant that surgical patients need only 43
between the science and the practice barrier to identification and treatment percent of the opioid pain medications
of addiction medicine found the topic because they segregate care delivery and they are generally prescribed, the hospi-
hardly mentioned in the board certifi- payment despite evidence that many tal introduced new guidelines to reduce
cation exam requirements of several key people with addictions have comorbid prescriptions and encourage over-the-
medical specialties (Center on Addiction medical conditions and are high utilizers counter alternatives. Results published
2012). of medical services. The situation con- in the journal Annals of Surgery reported
This lack of training created signif- tinues to drive episodic hospitalizations a 53 percent reduction in the number
icant missed opportunities to identify and other drains on the overall health of pills prescribed for five common out-
people with or at risk for SUDs. Similar care system. Yet, with separate payment patient procedures. Hospitals following
to chronic diseases such as diabetes, streams, carve-out carriers have little this example must provide access to
drug addiction can be linked to fam- incentive to promote ample treatment nonopioid medications and evidence-
ily history, detected early and treated options for SUDs. based, nonpharmacological pain man-
with evidence-based therapies. Yet, in agement services (Hill et al. 2018).
the mid- to late 2000s, as opioid abuse Changing History
increased, little detection or intervention The opioid crisis has reached a reckon- Enhancing patient identification and
occurred in hospitals and primary care ing point. We must assess and rapidly treatment initiation. Beyond prescrib-
settings. replicate what evidence suggests is work- ing limits and vigilant monitoring,
In a national survey of primary care ing. Ending the opioid epidemic will America’s Essential Hospitals notes that
providers and psychiatrists, 18 percent involve cumulative action on the part hospitals are uniquely positioned to
of physicians reported that they typically of multiple stakeholders, including the screen for and monitor opioid use by
offer no intervention to their alcoholic pharmaceutical industry, government, patients, offer transitional treatment and
patients—not even a referral—in part law enforcement sector and health care form multisector partnerships—all of
because of misplaced concern about delivery system. which can have a significant impact on
patients’ sensitivity to these issues. Given the burgeoning volume of identifying and initiating treatment for
Nearly the same proportion (15 percent) inpatients and outpatients with an patients with SUDs.
8 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 8 1/2/19 11:21 AMApproximately 15 percent of inpa- gone through the necessary training, For example, Rush University Med-
tients have an active SUD. Thus, hospi- and even fewer actually prescribe. ical Center in Chicago uses an online
tals have an opportunity to begin addic- Hospitals are also uniquely posi- tool called NowPow to connect people
tion treatment for those patients during tioned to build their own treatment who have chronic diseases with local
their stay. Best-practice approaches capacity in primary care settings. In resources that can help them better
include the Addiction Consult Service Massachusetts, a primary care office– manage their conditions. According to
program at Boston Medical Center, based opioid treatment program that Modern Healthcare, NowPow, which
which diagnoses and initiates care for
patients with SUDs and links them to
outpatient addiction treatment. This Ending the opioid epidemic will involve
program has proven effective at the
medical center in reducing subsequent cumulative action on the part of multiple
hospitalizations and ED visits among
that patient population (Trowbridge et stakeholders, including the pharmaceutical
al. 2017).
A recent Yale University study indi-
industry, government, law enforcement
cates that beginning treatment in EDs sector and health care delivery system.
is another practice that should be more
widely implemented in hospitals. The
research found that patients with OUDs emphasizes collaborative care was cre- grew out of a population health ini-
are more likely to receive addiction treat- ated and is widely used across the nation tiative led by the Lindau Lab at the
ment and reduce opioid use long-term if through the Community Health Center University of Chicago, can also measure
they start medication to reduce cravings Network. whether referrals were acted on and lets
in the ED (D’Onofrio et al. 2015). hospitals know how successful they were
Despite the evidence, this practice Incorporating SUD issues into pay- in assisting individuals with their needs
is far from standard. Even though find- ment and service delivery reform (Dickson 2018).
ings from a June 2018 study funded by efforts. Finally, addressing the opioid
the National Institute on Drug Abuse crisis in the United States must be part Conclusion
showed that opioid overdose deaths of larger health care reform strategies, From a historical perspective, the costs
decreased by 59 percent for those particularly those focused on containing and casualties of today’s opioid crisis
receiving methadone and 38 percent for costs, improving medical outcomes, might seem surreal to future genera-
those receiving buprenorphine in the 12 enhancing population health and tions. Hopefully, decades from now,
months following a nonfatal overdose, addressing social determinants of health. this public health emergency will have
fewer than one-third of patients were Research shows that 20 percent of the been addressed through medical break-
provided any medication for their OUD factors leading to premature death are throughs, health care innovations and
(Larochelle et al. 2018). Hospitals and related to social and environmental provider- and community-based interven-
health systems can help increase these issues, and 40 percent are related to tions. But for now, we remain far from
percentages by encouraging more phy- behaviors (Committee on Population et this goal, and the severity of the problem
sicians to obtain Drug Enforcement al. 2015). Acknowledging this fact, hos- warrants unprecedented action on the
Administration waivers to prescribe pitals and health systems are increasingly part of our hospitals, health systems
addiction medications. Currently, only supporting community-based outreach and all those who are best positioned to
3 percent of primary care doctors have programs and wellness initiatives. reverse and eliminate the epidemic.
References
Boston Medical Center. 2018. “Boston University and the Grayken Center Host National Conversation on
Research, Practice and the Opioid Epidemic.” Accessed December 17. www.bmc.org/node?page=15.
Center on Addiction. 2012. “Addiction Medicine: Closing the Gap Between Science and Practice.” Published June.
www.centeronaddiction.org/addiction-research/reports/addiction-medicine-closing-gap-between-science-
and-practice.
Centers for Disease Control and Prevention (CDC). 2018. “Surveillance for Viral Hepatitis—United States, 2016.”
Updated April 16. www.cdc.gov/hepatitis/statistics/2016surveillance/.
———. 2016. “Synthetic Opioid Overdose Data.” Updated December 16. www.cdc.gov/drugoverdose/data/
fentanyl.html.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 9
Futurescan 2019 INT.indd 9 1/2/19 11:21 AMCommittee on Population, Division of Behavioral and Social Sciences and Education, Board on Health Care
Services, National Research Council and Institute of Medicine. 2015. “Data from Major Studies of Premature
Mortality.” Published February 24. www.ncbi.nlm.nih.gov/books/NBK279981/.
Council of Economic Advisers. 2017. “The Underestimated Cost of the Opioid Crisis.” Published November. www.
whitehouse.gov/briefings-statements/cea-report-underestimated-cost-opioid-crisis/.
Dickson, V. 2018. “Mapping the Impact of Social Determinants of Health.” Modern Healthcare. Published March 31.
www.modernhealthcare.com/article/20180331/NEWS/180339986.
D’Onofrio, G., P.G. O’Connor, M.V. Pantalon, M.C. Chawarski, S.H. Busch, P.H. Owens, S.L. Bernstein and D.A. Fiel-
lin. 2015. “Emergency Department–Initiated Buprenorphine/Naloxone Treatment for Opioid Dependence: A
Randomized Clinical Trial.” Journal of the American Medical Association 313 (16): 1636–44.
Friedmann, P.D., D. McCullough and R. Saitz. 2001. “Screening and Intervention for Illicit Drug Abuse: A National
Survey of Primary Care Physicians and Psychiatrists.” Archives of Internal Medicine 161 (2): 248–51.
Guy, J.G., K. Zhang, M.K. Bohm, J. Losby, B. Lewis, R. Young, L.B. Murphy and D. Dowell. 2017. “Vital Signs: Changes
in Opioid Prescribing in the United States, 2006–2015.” Morbidity and Mortality Weekly Report 66 (26):
697–704.
Hill, M.V., R.S. Stucke, M.L. McMahon, J.L. Beeman and R.J. Barth Jr. 2018. “An Educational Intervention Decreases
Opioid Prescribing After General Surgical Operations.” Annals of Surgery 267 (3): 468–72.
Larochelle, M.R., D. Bernson, T. Land, T.J. Stopka, N. Wang, Z. Xuan, S.M. Bagley, J.M. Leibschutz and A.Y. Walley.
2018. “Medication for Opioid Use Disorder After Nonfatal Opioid Overdose and Association with Mortality:
A Cohort Study.” Annals of Internal Medicine 169 (3): 137–45.
National Institute on Drug Abuse. 2018. “Overdose Death Rates.” Revised August. www.drugabuse.gov/related-
topics/trends-statistics/overdose-death-rates.
Patrick, S.W., M.M. Davis, C.U. Lehmann and W.O. Cooper. 2015. “Increasing Incidence and Geographic Distri-
bution of Neonatal Abstinence Syndrome: United States, 2009 to 2012.” Journal of Perinatology 35 (8):
650–55.
Substance Abuse and Mental Health Services Administration (SAMHSA). 2017. “Results from the 2016 National
Survey on Drug Use and Health.” Published September 7. www.samhsa.gov/data/sites/default/files/NSDUH-
DetTabs-2016/NSDUH-DetTabs-2016.pdf.
Trowbridge, P., Z.M. Weinstein, T. Kerensky, P. Roy, D. Regan, J.H. Samet and A.Y. Walley. 2017. “Addiction Con-
sultation Services—Linking Hospitalized Patients to Outpatient Addiction Treatment.” Journal of Substance
Abuse Treatment 79: 1–5.
Weiss, A.J., A. Elixhauser, M.L. Barrett, C.A. Steiner, M.K. Bailey and L. O’Malley. 2017. “Opioid-Related Inpatient Stays
and Emergency Department Visits by State, 2009–2014.” Healthcare Cost and Utilization Project. Revised
January. www.hcup-us.ahrq.gov/reports/statbriefs/sb219-Opioid-Hospital-Stays-ED-Visits-by-State.jsp.
Xu, J., S.L. Murphy, K.D. Kochanek, B. Bastian and E. Arias. 2018. “Deaths: Final Data for 2016.” National Vital Sta-
tistics Reports 67 (5): 1–75.
10 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 10 1/2/19 11:21 AM2 DIGITAL HEALTH
Flipping the Stack: Can New Technology Drive
Health Care’s Future?
by Matthew Holt and Indu Subaiya, M.D.
T
he easy availability of cloud-
and mobile-based computing
systems has revolutionized the
business sector, putting power
and access into the hands of employees
and customers and creating huge shifts
in how transactions are done. Now the
companies with the highest market
value are both the drivers and the ben-
eficiaries of this transition—notably
Apple, Facebook, Amazon and Alphabet
(Google), as well as their international
rivals such as Samsung, Baidu, Tencent
and Alibaba.
Underpinning this transformation
has been a change from enterprise-
specific software to generic cloud-based
services—sometimes called SMAC
(social, mobile, analytics and cloud).
Applications for data storage, sales man- have flocked to these new platforms entertainment (Netflix), lodging
agement and email and the hardware using GSuite, Amazon Web Services, (Airbnb) and more.
they ran on were put into enterprises in Salesforce, Slack and countless others
the client-server era dominated by Intel (exhibit 1). Those technologies, in turn, What About Health Care
and Microsoft. These have now migrated have enabled the growth of completely Organizations?
to cloud-based, on-demand services, new types of businesses, transforming Hospitals and health systems were late-
and consumers and businesses alike sectors such as transportation (Uber), comers to the enterprise technology
About the Authors
Matthew Holt is a nationally recognized Indu Subaiya, M.D., is a visionary leader
health technology expert who is best known whose work builds community, creates
as the founder of The Health Care Blog and dialogue and inspires radical thinking about
cofounder of the Health 2.0 conference. The how health shapes lives. She cofounded and
Health Care Blog has been a leading source served as CEO of Health 2.0, the leading con-
of opinion, news and interviews about health ference and media platform that promotes
and health technology since 2003 and fea- and catalyzes new technologies in health
tures Holt’s “Health in 2 Point 00” videos with care. Health 2.0’s conference business was
Jessica DaMassa. Health 2.0 is the leading acquired by HIMSS in 2017, and Subaiya con-
conference series showcasing frontier tech- tinues to head the organization as executive
nologies in health care. Holt also works on vice president as it scouts new technologies
SMACK.health, advising a group of startups and builds initiatives to drive sustainable
navigating the health care world. Earlier in his change in today’s health care landscape. An
career, following graduate work at Stanford immigrant from India, Subaiya is a passionate
University, Holt worked for the renowned advocate for ending health care disparities
Institute for the Future and the Harris Insights and increasing diversity in the industry’s
& Analytics polling organization. leadership ranks.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 11
Futurescan 2019 INT.indd 11 1/2/19 11:21 AMFUTURESCAN SURVEY RESULTS
Digital Health
How likely is it that the following will happen by 2024?
Already Very Somewhat Somewhat Very
Happening Likely Likely Neutral Unlikely Unlikely
(%) (%) (%) (%) (%) (%)
8 29 24 25 3 1
Our organization will use the FHIR (Fast Healthcare Interoperability Resources)
standard to make accessing health care records easier for third-party
applications and organizations.
6 24 27 36 6 2
Our organization will change most data storage and transaction tools to
blockchain or other distributed computing technologies.
9 38 26 11 13 3
A major technology company, such as Google, Amazon or Apple, will emerge as
a significant developer of health care services that competes directly with our
organization’s services.
Note: Percentages in each row may not sum exactly to 100 percent because of rounding.
What Health Care Executives Anticipate by 2024
• Nearly half (47 percent) of hospital and health system leaders say a major
technology company either already has emerged as a competitor to their
organization’s health care services or is very likely to do so.
• Fifty-seven percent of respondents are at least somewhat likely to change
most of their organization’s data storage and transaction tools to blockchain
or other distributed computing technologies.
• Only 8 percent of leaders indicate that their organization uses the FHIR (Fast
Healthcare Interoperability Resources) standard to facilitate access to health
care records by third-party applications and organizations. However, another
53 percent say their organization is at least somewhat likely to do so.
12 FUTURESCAN 2019–2024
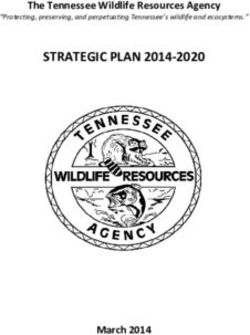
Futurescan 2019 INT.indd 12 1/2/19 11:21 AMExhibit 1
Growth in Use of Cloud Data Centers Versus Traditional Data Centers
Traditional Data Center (3% CAGR) 21% CAGR
600 Cloud Data Center (26% CAGR) 2015–2020
500 8%
92%
400
Installed
Workload 300
in Millions
200
25%
100 75%
0
2015 2016 2017 2018 2019 2020
Note: CAGR = compound annual growth rate.
Source: Cisco Global Cloud Index, 2015–2020.
—continued from pg. 11
and 24 percent reported they are somewhat
game, including to client-servers. In the 2000s likely. Our take is that these numbers understate
and 2010s, mostly in response to the HITECH FHIR’s impact. After all, this standard is already
(Health Information Technology for Economic being used by Apple to extract data for its health
and Clinical Health) Act, hospitals added elec- record from more than 100 top hospitals, and
tronic medical records (EMRs) to their other all major EMR vendors (and many major health
information systems. The majority of these systems) are developing a series of partnerships,
EMRs are client-server based and enterprise app stores and innovation programs to allow
specific. Even those that are cloud based tend those third-party application vendors easier
to be hosted in the private cloud environment access to users (e.g., clinicians, patients, adminis-
of vendors. However, the health care sector is trators). Also, many hospitals are contributing to
likely to transition to using the cloud as other the explosion in apps and services by encourag-
businesses have. Current technology vendors, ing their internal teams to create them.
including Epic and Cerner, are beginning to There is considerable debate among experts
open their systems and are moving their cli- regarding the near-term evolution of technology
ents to their private cloud, while another large in health care. Most hospitals have spent huge
vendor, Allscripts, has put most of its tech- amounts on EMR installations in recent years,
nology onto Microsoft’s public cloud (Azure). so they are unlikely to replace their incumbent
Meanwhile, all of the major EMR vendors have vendors. But although the transaction layer
adopted the FHIR (Fast Healthcare Interop- inside the current EMR may seem to be well
erability Resources) standard and SMART embedded in the system, new types of interface,
(Substitutable Medical Apps and Reusable storage and data analytics solutions are increas-
Technology)-on-FHIR protocols, which make ingly being trialed.
it much easier to transfer data between different The advent of FHIR and distributed storage
applications and to give users a choice of tools, certainly portends a future of decentralized data
many of which are hosted on the cloud. and services, with big implications for hospitals
How quickly is FHIR being adopted? In the and health systems that are trying to implement
Futurescan national survey, only 8 percent of physical and contractual controls over those areas.
health care executives said their organizations are
already using FHIR to make it easier for third- New Developments
party applications to access their data; 29 percent As the pace of technological advances contin-
indicated they are very likely to do so by 2024, ues to accelerate, health care leaders need to be
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 13
Futurescan 2019 INT.indd 13 1/2/19 11:21 AMVirtual reality and augmented reality.
While VR and AR are already changing
the worlds of gaming and entertain-
ment, it is more difficult to see where
these technologies fit in health care. So
far, VR is being experimented with in
pain management and mental health.
AR seems to be finding its niche in
remotely recording and supporting
patient–physician visits and overlaying
X-ray images on patients to aid in clini-
cal precision.
The AI, VR and AR revolution is
likely to make its biggest impact when
these trends are combined with the
underlying technologies of sensors, ana-
lytics and on-demand computing. The
early stages of this potential have been
dominated by consumer use of voice
prepared for the next wave of change In the latest Futurescan survey, 6 assistants and automatically controlled
and how it will affect their organizations percent of hospital and health system systems that respond to questions and
and the communities they serve. leaders said their organization has already commands. Some companies are already
At the forefront are blockchain, changed most of its data storage and putting voice assistants in hospital
artificial intelligence (AI), virtual reality transaction tools to blockchain or other rooms to replace nurse call systems.
(VR) and augmented reality (AR)—all distributed computing technologies. Soon, more of these communications
built on the expanding capabilities of Another 24 percent believe such a change will be automated, and the sensors will
cloud computing and driven by the bur- is very likely in the next five years. not only take instruction but also pas-
geoning internet of things (IoT). sively track patient activity in the hospi-
Artificial intelligence. The only thing tal or home and automatically respond.
Blockchain. Blockchain is a distributed generating more hype than blockchain
database technology in which every is AI. At its core, AI enables very quick The Role of the Tech Giants
transaction is recorded on every node in a computation of vast amounts of data, It has escaped few observers’ attention
network. It is, therefore, hard to hack or looks for patterns and makes suggestions that the companies with the most
alter. Blockchain also does more than just about them (e.g., symptom assessment advanced technology in AI, voice rec-
record transactions: It allows “smart con- in radiology) or, in some cases, acts on ognition, sensors and cloud computing
tracts” to be embedded in the blockchain them (e.g., self-driving cars, fully robotic are the same ones that have benefited
to enable permissions, grant access to surgery). Perhaps the most promising from the SMAC revolution. The health
data and perform transactions—all auto- area for AI in health care is in compu- tech press has been abuzz with articles
matically. Closely related is the concept tations that are just far too complicated attempting to read the tea leaves about
of “identity by consensus,” which enables for humans, such as identifying the fac- what Apple, Amazon and Alphabet
the authorization of identity from data tors behind cancer or managing complex (Google) will do in the health care sec-
gathered from multiple sources. drug regimens for safety and matching tor in the future (see sidebar).
Blockchain is still in its early days. them with genomes and phenotypes. The Futurescan survey asked exec-
One or two industry groups are form- AI is also being used for tasks such as utives whether they believe a major
ing in health care, including the Linux the following: technology company will emerge as a
Foundation’s Hyperledger Consortium significant developer of health care ser-
and Hashed Health. In a recent survey, • Predicting which patients are likely to vices that compete directly with hospitals
75 percent of health care executives contract a certain disease based on lab, and health systems. Only 9 percent of
described their understanding of block- medical and insurance claims data. respondents said this is already happen-
chain as “excellent,” while 39 percent • Personalizing drug regimens to lower ing (which might be a surprise to the
indicated that learning about blockchain patients’ risk for complex interactions tech giants), but another 38 percent
is one of their top five priorities. Eleven and to improve outcomes. indicated it is very likely to happen in
percent of respondents reported deploy- • Leveraging chatbot technology the next five years.
ing blockchain somewhere in their to analyze patient symptoms and Although it remains to be seen how
enterprise (Deloitte 2018). diagnose health problems. the tech giants’ health care strategies
14 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 14 1/2/19 11:21 AMwill unfold, clearly they have the talent, be the final step (or layer in the stack).
Sleuthing the Tech resources and funding to make a consid- In fact, almost any intervention could
Giants’ Potential erable impact in the field. In addition, be considered a failure of the system,
Health Care Moves other major players such as CVS/Aetna, or at least a correction of the autopilot
Walmart and UnitedHealth Group, to mode.
Apple seems focused on name a few, are not sitting still. All of What might this inverted stack
embedding sensors in them seem to be angling in on chronically look like? Imagine a combination of
its watch that can track ill consumers in the home—a patient home-delivered medications (PillPack),
bodily functions related population and location that health care IoT sensors recording a person’s vital
to diabetes, heart disease providers have traditionally struggled with. signs (Apple), technology-based ser-
and sleep. The company vices monitoring chronically ill patients
has also integrated the Inverting the Stack (Livongo), online physician care (Doc-
EMRs of more than 90 New market entrants can change health tors on Demand) or even acute, hospital-
hospitals to bring data care in several obvious scenarios, but the like care provided in the home (Med-
into its app store, and one in which they take a major role is ically Home). In this model, the tech
it is developing med- called “inverting the stack.” platform is the underlying system, with
ical clinics for its own Traditionally, the U.S. health care services and professionals at the top of
employees. system has been designed around care the stack. In our opinion, this scenario
delivery, services and technology plat- could soon become a reality that radi-
Amazon is clearly get- forms, in that order (exhibit 2). cally reduces doctor visits and hospital
ting into the hospital Imagine inverting this triple-layer admissions and improves patient care.
supplies business and stack and starting with technology
recently bought PillPack, platforms (exhibit 3). In this model, Implications for Health Care
a pharmacy specializ- sensors, trackers and AI systems and Leaders
ing in home delivery for processes would be in place monitoring, As the technology trends described in
customers on multiple measuring and suggesting next steps to this article progress, the key question
medications. It also has both providers and patients. Health care is how quickly and to what extent they
the biggest cloud ser- would shift from being an event-driven will transform health care. Here are a
vice, and Alexa, which is system to a consistent process. Normal few suggestions to help hospital and
already in 20 percent of patient behavior and activity would not health system executives better under-
U.S. households, cur- need a response, whereas exceptions and stand the transition and assess the rate
rently dominates the problems would require medical inter- of change:
voice assistant market. vention from a combination of human-
and machine-driven services. Health • Become familiar with the technologies.
Alphabet (Google) is
care delivery as we know it today would You will not fully understand VR by
concentrating on its
cloud service, which has Exhibit 2 Exhibit 3
more than 30 health
tech companies in its Traditional Health Care Model Tech Inverts the Stack
app store, and its Verily
unit, which specializes
in genomics and per-
sonalized medicine. In
addition, it has a $500 TECH PLATFORMS CARE DELIVERY
million joint venture
with Sanofi called
Onduo that is working SERVICE SERVICE
on high-tech solutions
for managing diabetes,
and it bought 10 per-
cent of Oscar Health, CARE DELIVERY TECH PLATFORMS
a technology-focused
health insurance
company.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 15
Futurescan 2019 INT.indd 15 1/2/19 11:21 AMreading about it. You might if you • Spend time with health tech startups at payment-for-value becomes ingrained
play a video game with your kids on conferences, participate in a health care in health care, the likelier it is that real
their new Oculus headset. incubator program and get to know changes in how chronically ill patients
• Talk to the clinicians who are using the tech-savvy doctors in your hospital. are monitored and managed will be
these new tools in your organization They will be pushing the boundaries implemented.
to get their feedback. Engage the end of technological innovation and know
users—your patients—about their what may be possible in the future. Taking these steps is a good way to
experiences in being treated with the • Pay attention to both leading-edge start preparing yourself for the next
technologies. Ask your researchers and payers (e.g., Oscar Health or any phase of health care’s digital revolution
analysts for data on the impact the employer who uses Grand Rounds) and determining what strategies may or
technologies are having on the cost and the Centers for Medicare may not make sense for your organiza-
and quality of care. & Medicaid Services. The more tion now and in the future.
Reference
Deloitte. 2018. “2018 Global Blockchain Survey.” Accessed September 20. www2.deloitte.com/us/en/pages/
consulting/articles/innovation-blockchain-survey.html.
16 FUTURESCAN 2019–2024
Futurescan 2019 INT.indd 16 1/2/19 11:21 AM3 BIOTECHNOLOGY
Bioelectronic Medicine: Creating New Treatment
Paradigms
by Chad Bouton
I
n the new era of medicine, technology
is woven into virtually every aspect of
patient care. Electronic health records
are being harnessed to identify ways to
improve care, with predictive algorithms
under development to warn providers
about possible health issues. Advances
in wearable devices help both patients
and medical professionals track vital
health information, while new laboratory
instrumentation and artificial intelli-
gence aid in applications ranging from
detecting infections to diagnosing cancer.
A rapidly growing field called bio-
electronic medicine uses technology to
modulate the nervous system to treat
disease and injury without the use of
pharmaceuticals. Initial clinical trial
results are positive and show the inno- aware of the field because research One of the initial discoveries was
vation is on its way to being a tangible related to bioelectronic medicine has the made in the late 1990s by Kevin J.
alternative to certain medications. While potential to attract additional outside Tracey, M.D., president and CEO of the
it is hard to predict what will happen investment from donors and industry. Feinstein Institute for Medical Research,
with this technology in the next few who found that the vagus nerve is
years, health care leaders should make it Harnessing the Nervous involved in controlling inflammation
a priority to stay abreast of new devel- System to Treat Disease (Tracey 2002). This revelation raised
opments because bioelectronics could and Injury hope that if we can interact with the
radically alter how physicians, hospitals, Before delving into what the future holds, nervous system, we may be able to treat
health systems and other providers let’s examine the foundation of bioelec- conditions involving inflammation, such
deliver care in the future. tronic medicine and some of its recent dis- as Crohn’s disease, lupus and rheuma-
Health care organizations that have coveries to understand how it differs from toid arthritis (RA). We may also be able
a research component should also be pharmaceutical research and development. to treat other conditions that involve
About the Author research in neurotechnology to treat paral-
Chad Bouton is the vice president of ysis and is developing new technologies to
advanced engineering and director of the accelerate the field of bioelectronic medi-
Center for Bioelectronic Medicine at the cine. His pioneering work, which allowed a
Feinstein Institute for Medical Research, the paralyzed person to regain movement using
research arm of Northwell Health in New a brain implant for the first time, has been
York. He formerly served as research leader featured on CBS’s 60 Minutes. Bouton holds
at Battelle Memorial Institute, the world’s more than 70 patents worldwide, and his
largest independent research and develop- technologies have received three R&D 100
ment (R&D) organization, where he spent 18 Awards. Bouton was recognized by the U.S.
years researching and developing biomed- Congress for his work in the medical device
ical technology. At the Feinstein Institute, field, and Battelle has named him a Distin-
Bouton is performing groundbreaking guished Inventor and an Inventor of the Year.
H E A LT H C A R E T R E N D S A N D I M P L I C A T I O N S 17
Futurescan 2019 INT.indd 17 1/2/19 11:21 AMYou can also read