Treatment of heart failure across the spectrum of left ventricular ejection fraction and an update on cardiac amyloidosis and ischaemic ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
European Heart Journal (2022) 43, 351–354 ISSUE @ A GLANCE
https://doi.org/10.1093/eurheartj/ehab906
Treatment of heart failure across
the spectrum of left ventricular
ejection fraction and an update on
cardiac amyloidosis and ischaemic
Downloaded from https://academic.oup.com/eurheartj/article/43/5/351/6521629 by guest on 10 February 2022
cardiomyopathy
Filippo Crea1,2
1
Department of Cardiovascular Medicine, Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy; and 2Department of
Cardiovascular and Pulmonary Sciences, Catholic University of the Sacred Heart, Rome, Italy
With thanks to Amelia Meier-Batschelet, Johanna Huggler, and Martin Meyer for help with compilation of this article.
For the podcast associated with this article, please visit https://academic. cardiology. Of note, the practice of interventional cardiology took
oup.com/eurheartj/pages/Podcasts. place amidst successive waves of the COVID-19 pandemic, which
continues to be a major burden for all healthcare professionals
This issue opens with two Special Articles of the series the Year in around the globe. In this review, the authors revisit the develop
Cardiovascular Medicine. The first article is the ‘The year in car ments in percutaneous coronary intervention (PCI), structural
diovascular medicine 2021: heart failure and cardiomyop heart interventions, and adjunctive pharmacotherapy.
athies’ by Johann Bauersachs from the Medizinische Hochschule The issue continues with a focus on HF and cardiomyopathies.
Hannover, and colleagues.1 In 2021 the universal definition and Ischaemic cardiomyopathy (ICM) is the most frequent cause of
classification of heart failure (HF) was published that defines HF HFrEF; its management is complex and widely debated.3,4 In a
as a clinical syndrome with symptoms and/or signs caused by a car Viewpoint article entitled ‘Myocardial revascularization in
diac abnormality and corroborated by elevated natriuretic peptide ischaemic cardiomyopathy: routine practice vs. scientific
levels or objective evidence of cardiogenic congestion. This defin evidence’, Raffaele De Caterina from Pisa University Hospital
ition and the classification of HF with reduced (HFrEF), mildly re and University of Pisa in Italy, and colleagues indicate that patients
duced, and preserved ejection fraction (HFpEF) are consistent with extensive coronary artery disease and ICM have an unfavour
with the 2021 ESC Guidelines on HF. Among several other new able prognosis.5 Current ESC guidelines recommend myocardial
recommendations, these guidelines give a Class I indication for the revascularization in ICM patients with suitable coronary anatomy,
use of the sodium–glucose co-transporter 2 (SGLT2) inhibitors dapa using either coronary artery bypass graft (CABG) or PCI.
gliflozin and empagliflozin in HFrEF patients. As first evidence-based Real-world data indicate that PCI has become the revasculariza
treatment for HFpEF, in the EMPEROR-Preserved trial, empagliflozin tion strategy of choice in ICM, with usage rates now nearly three
reduced the composite endpoint of cardiovascular death and HF hos times higher than CABG. The authors summarize the scientific evi
pitalizations. Several reports in 2021 have provided novel and de dence for revascularization with either CABG or PCI in patients
tailed analyses of device and medical therapy in HF, especially with ICM, the guiding principles to support its continued use,
regarding sacubitril/valsartan, SGLT2 inhibitors, mineralocorticoid re and the disturbing discordance between current clinical practice
ceptor antagonists, ferric carboxymaltose, soluble guanylate cyclase and scientific evidence.
activators, and cardiac myosin activators. Transthyretin amyloidosis (ATTR amyloidosis) is a heteroge
The second article from this series is ‘The year in cardiovas neous disorder with cardiac, neurological, and mixed pheno
cular medicine 2021: interventional cardiology’ by Javier types.6–13 In a Clinical Research article entitled ‘Transthyretin
Escaned from the Hospital Clinico Universitario San Carlos in cardiac amyloidosis in continental Western Europe: an in
Madrid, Spain, and colleagues.2 Since last year’s report, the authors sight through the Transthyretin Amyloidosis Outcomes
have witnessed substantial progress in all aspects of interventional Survey (THAOS)’, Thibaud Damy from the GRC Amyloid
Published by Oxford University Press on behalf of European Society of Cardiology 2022
352 Issue @ a Glance
Research Institute in Créteil, France, and colleagues describe the The authors conclude that ATTR amyloidosis genotypes and
phenotypic and genotypic profile of this disease in continental phenotypes are highly heterogeneous in continental Western
Western Europe as it appears from the Transthyretin Europe. A geographic map of the different disease profiles and
Amyloidosis Survey (THAOS).14 THAOS is an ongoing, world awareness that a subset of subjects have a dominant cardiac phe
wide, longitudinal, observational survey established to study differ notype, mimicking hypertrophic cardiomyopathy, at presentation
ences in presentation, diagnosis, and natural history in ATTR can facilitate the clinical recognition of this underdiagnosed dis
amyloidosis subjects. At data cut-off, 1411 symptomatic subjects ease. This manuscript is accompanied by an Editorial by Enrico
from nine continental Western European countries were enrolled Ammirati from the Niguarda Hospital in Milan, Italy and Omar
in THAOS [1286 hereditary (ATTRm) amyloidosis; 125 wild-type AbouEzzeddine from the Mayo Clinic, Rochester, MN, USA.15
ATTR (ATTRwt) amyloidosis]. Genotypes and phenotypes varied The authors conclude that ATTR is a broad spectrum of diseases
notably by country. Four mutations (Val122Ile, Leu111Met, with diverse genotypes, heterogeneous phenotypes, and variable
Thr60Ala, and Ile68Leu) and ATTRwt were associated with a geographic distribution. Current registries under-represent pa
Downloaded from https://academic.oup.com/eurheartj/article/43/5/351/6521629 by guest on 10 February 2022
mainly cardiac phenotype showing symmetric left ventricular tients with ATTRwt and ATTRm with cardiac genotypes. The ad
(LV) hypertrophy, normal diastolic LV dimensions and volume, vent of non-invasive, scintigraphy-based diagnostic techniques has
and mildly depressed LV ejection fraction (LVEF). Morphological increased recognition of ATTR cardiomyopathy. Future registries
and functional abnormalities on echocardiogram were significantly ought to incorporate more patients with ATTR and track cardiac
more severe in subjects with cardiac, compared with a mixed phe and systemic biomarkers to improve phenotypic classification, dis
notype characterized by higher median interventricular septal ease staging, and risk stratification. Finally, in this exciting era of
thickness (18 vs. 16 mm; P = 0.0006) and greater prevalence of therapeutic advances, studying the impact of novel disease-
LVEF ,50% (38 vs. 17%; P = 0.0008). Subjects with cardiac muta modifying agents on clinical course and outcomes is crucial.
tions or ATTRwt (or cardiac or mixed phenotype) had a lower In another Clinical Research article entitled ‘Primary care
survival rate than subjects with other genotypes (or the neurolo heart failure service identifies a missed cohort of heart
gical phenotype) (P , 0.0001, for both). failure patients with reduced ejection fraction’, Matthew
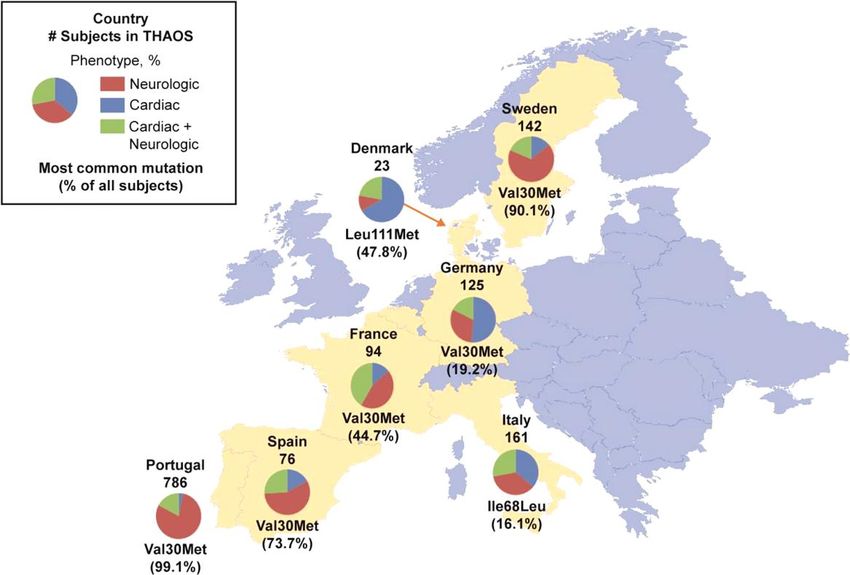
Figure 1 Subject phenotypes and the most common genotype in subjects enrolled in THAOS in continental Western Europe. Data are from
all European countries included in THAOS. Shown are: the total number of subjects from each country in THAOS, the proportions of each
phenotype, and the most common mutation in each country (with its percentage of all subjects in that country). Not shown are: Belgium, three
subjects with cardiac + neurological phenotype (genotypes: Val30Met, Glu54Leu, and Glu74Leu); and Cyprus, one subject with neurological
phenotype (genotype: Val30Met). Note that the most common form of ATTR amyloidosis in Germany and Italy was ATTRwt (41.6% and 34.2%
of all subjects, respectively).14Issue @ a Glance 353
Downloaded from https://academic.oup.com/eurheartj/article/43/5/351/6521629 by guest on 10 February 2022
Figure 2 Influence of ejection fraction on the effect of empagliflozin on time to cardiovascular death or hospitalization for heart failure.
Ejection fraction is analysed as a continuous variable, based on the assumption that the relationship is linear. Analysis of the influence of ejection
fraction using cubic splines yielded a pattern similar to that observed in our six subgroups, showing a consistent risk reduction in patients with
an ejection fraction ,65% and an attenuated effect at the highest ejection fractions. Shaded areas represent 95% confidence intervals.22
Kahn from the Liverpool Heart and Chest Hospital NHS care. Although no clinical outcomes were reported, it is not unrea
Foundation Trust in the UK, and colleagues explored whether a sonable to expect that this translated into improved outcomes.
missed cohort of patients in the community with HF and LV systo Medical records-based screening has the potential to identify pre
lic dysfunction (LVSD) could be identified and receive treatment viously unrecognized HF diagnoses and HF undertreatment.
optimization through a primary care HF (PCHF) service.16 Screening is widely accepted in other areas of medicine and should
A PCHF service is a partnership between Inspira Health, be further studied in HF.
National Health Service Cardiologists, and Medtronic. The SGLT2 inhibitors have emerged as a key treatment of HF.18–21 In
PCHF service uses retrospective clinical audit to identify patients a Clinical Research article entitled ‘Effect of empagliflozin in
requiring a prospective face-to-face consultation with a consultant patients with heart failure across the spectrum of left ven
cardiologist for clinical review of their HF management within pri tricular ejection fraction’, Javed Butler from the University of
mary care. The service is delivered via five phases: (i) interrogation Mississippi School of Medicine in Jackson, MS, USA, and colleagues
of general practitioner (GP) systems; (ii) clinical audit of medical assessed the influence of EF on the effect of the SGLT2 inhibitor
records; (iii) patient invitation; (iv) consultant reviews; and (v) empagliflozin on HF outcomes.22 A pooled analysis was performed
follow-up. A total of 78 GP practices (864 194 population) have on both the EMPEROR-Reduced and EMPEROR-Preserved trials
participated. The service found that within primary care, 27% of (9718 patients), and patients were grouped based on EF: ,25,
HF patients identified for a cardiologist consultation were eligible 25–34, 35–44, 45–54, 55–64, and ≥65%. Outcomes assessed in
for complex device therapy, 45% required optimization of medi cluded (i) time to first hospitalization for HF or cardiovascular
cines, and 47% of patients audited required diagnosis codes adding mortality; (ii) time to first HF hospitalization; (iii) total (first and re
to their GP record. current) hospitalizations for HF; and (iv) health status assessed by
The authors conclude that a PCHF service can identify a missed the Kansas City Cardiomyopathy Questionnaire (KCCQ). The risk
cohort of patients with HF and LVSD, enabling the optimization of of cardiovascular death and hospitalization for heart failure de
prognostic medication and an increase in device prescription. The clined progressively as EF increased from ,25% to ≥65%.
contribution is accompanied by an Editorial by Lars Lund from Empagliflozin reduced the risk of cardiovascular death or HF hos
the Karolinska Institutet in Stockholm, Sweden, and colleagues.17 pitalization, mainly by reducing HF hospitalizations. Empagliflozin
The authors conclude that the PCHF service resulted in an in reduced the risk of HF hospitalization by ≏30% in all EF subgroups,
crease by ≏40% of the number of patients receiving optimal with an attenuated effect in patients with an EF ≥65%. Hazard354 Issue @ a Glance
ratios were: EF ,25%, 0.73; EF 25–34%, 0.63; EF 35–44%, 0.72; EF 6. Rapezzi C, Aimo A, Pavasini R. Longitudinal strain in the management of cardiac
AL amyloidosis: do we need it? Eur Heart J 2022;43:342–344.
45–54%, 0.66; EF 55–64%, 0.70; and EF ≥65%, 1.05. Other HF out
7. Cohen OC, Ismael A, Pawarova B, Manwani R, Ravichandran S, Law S, et al.
comes, including KCCQ, showed a similar response pattern. Sex Longitudinal strain is an independent predictor of survival and response to ther
did not influence the responses to empagliflozin. apy in patients with systemic AL amyloidosis. Eur Heart J 2022;43:333–341.
The authors conclude that the magnitude of the effect of empa 8. Garcia-Pavia P, Rapezzi C, Adler Y, Arad M, Basso C, Brucato A, et al. Diagnosis
and treatment of cardiac amyloidosis: a position statement of the ESC Working
gliflozin on HF outcomes is clinically meaningful and similar in pa Group on Myocardial and Pericardial Diseases. Eur Heart J 2021;42:1554–1568.
tients with EF ,25% to ,65% but is attenuated in patients with an 9. Falk RH, Dorbala S. Transthyretin cardiac amyloidosis in patients with severe aor
EF ≥65%. The manuscript is accompanied by an Editorial by John tic stenosis. Eur Heart J 2020;41:2768–2770.
10. Rosenblum H, Burkhoff D, Maurer MS. Untangling the physiology of transthyretin
McMurray and Toru Kondo from the University of Glasgow in the
cardiac amyloidosis by leveraging echocardiographically derived pressure–vo
UK.23 The authors note that the two most novel aspects of the lume indices. Eur Heart J 2020;41:1448–1450.
new ESC guidelines on HF were the strong recommendation given 11. Chacko L, Martone R, Bandera F, Lane T, Martinez-Naharro A, Boldrini M, et al.
to SGLT2 inhibitors as a treatment for HFrEF (EF ≤40%) and the Echocardiographic phenotype and prognosis in transthyretin cardiac amyloidosis.
Eur Heart J 2020;41:1439–1447.
Downloaded from https://academic.oup.com/eurheartj/article/43/5/351/6521629 by guest on 10 February 2022
first ever recommendation of any therapy for the renamed 12. Emdin M, Aimo A, Rapezzi C, Fontana M, Perfetto F, Seferović PM, et al.
HFmrEF (EF .40% to ,50%). Use of all the major neurohumoral- Treatment of cardiac transthyretin amyloidosis: an update. Eur Heart J 2019;40:
modulating therapies was proposed in the latter patients, although 3699–3706.
13. van den Berg MP, Mulder BA, Klaassen SHC, Maass AH, van Veldhuisen DJ, van
the recommendation was much weaker than for patients with
der Meer P, et al. Heart failure with preserved ejection fraction, atrial fibrillation,
HFrEF because it was based on retrospective analyses of trials and the role of senile amyloidosis. Eur Heart J 2019;40:1287–1293.
which suggested benefit of these treatments in certain patients 14. Damy T, Kristen AV, Suhr OB, Maurer MS, Planté-Bordeneuve V, Yu CR, et al.
with an EF .40%, i.e. probably those with some degree of LV sys Transthyretin cardiac amyloidosis in continental Western Europe: an insight
through the Transthyretin Amyloidosis Outcomes Survey (THAOS). Eur Heart J
tolic dysfunction. The precise upper EF threshold above which 2022;43:391–400.
there is no benefit remains uncertain and a source of debate. 15. Ammirati E, AbouEzzeddine OF. Transthyretin amyloidosis in Western Europe: a
The issue is also complemented by two Discussion Forum con snapshot from the THAOS registry and a call for further perspectives. Eur Heart J
2022;43:401–404.
tributions. In a commentary entitled ‘Respectful language and
16. Kahn M, Grayson AD, Chaggar PS, Ng Kam Chuen MJ, Scott A, Hughes C, et al.
putting the person first with obesity’, Simar Singh Bajaj Primary care heart failure service identifies a missed cohort of heart failure pa
from Harvard University in Cambridge, MA, USA, and colleagues tients with reduced ejection fraction. Eur Heart J 2022;43:377–386.
comment on the recent publication ‘Obesity modifies the en 17. Lund LH, Hage C, Savarese G. Implementation science and potential for screening
in heart failure. Eur Heart J 2022;43:413–415.
ergetic phenotype of dilated cardiomyopathy’ by Jennifer 18. Piña IL. SGLT2 inhibitors: the story continues to unfold. Eur Heart J 2021;42:
J. Rayner from the University of Oxford in the UK.24,25 Rayner 4902–4094.
et al. respond in a separate comment.26 19. Packer M. Are the benefits of SGLT2 inhibitors in heart failure and a reduced ejec
tion fraction influenced by background therapy? Expectations and realities of a
The editors hope that this issue of the European Heart Journal will
new standard of care. Eur Heart J 2020;41:2393–2396.
be of interest to its readers. 20. Paneni F, Costantino S, Hamdani N. Regression of left ventricular hypertrophy
with SGLT2 inhibitors. Eur Heart J 2020;41:3433–3436.
References 21. Sattar N, Anker SD, Butler J, Verma S. Obesity, heart failure, and SGLT2 inhibi
tion: DECLARE-TIMI 58 provides insights. Eur Heart J 2022;43:ehab709.
1. Bauersachs J, de Boer RA, Lindenfeld J, Bozkurt B. The year in cardiovascular med
22. Butler J, Packer M, Filippatos G, Ferreira JP, Zeller C, Schnee J, et al. Effect of em
icine 2021: heart failure and cardiomyopathies. Eur Heart J 2022;43:367–376.
2. Escaned J, Jaffer FA, Mehilli J, Mehran R. The year in cardiovascular medicine 2021: pagliflozin in patients with heart failure across the spectrum of left ventricular
interventional cardiology. Eur Heart J 2022;43:377–386. ejection fraction. Eur Heart J 2022;43:416–426.
3. Pelosi F Jr. Defibrillator therapy for non-ischaemic cardiomyopathy: are sharks 23. Kondo T, McMurray JJV. Re-emergence of heart failure with a normal ejection
lurking beneath the rippling waters? Eur Heart J 2019;40:551–552. fraction? Eur Heart J 2022;43:427–429.
4. Gutman SJ, Costello BT, Papapostolou S, Voskoboinik A, Iles L, Ja J, et al. 24. Bajaj SS, Tu L, Stanford FC. Respectful language and putting the person first with
Reduction in mortality from implantable cardioverter-defibrillators in non- obesity. Eur Heart J 2022;43:430.
ischaemic cardiomyopathy patients is dependent on the presence of left ventricu 25. Rayner JJ, Peterzan MA, Clarke WT, Rodgers CT, Neubauer S, Rider OJ. Obesity
lar scar. Eur Heart J 2019;40:542–550. modifies the energetic phenotype of dilated cardiomyopathy. Eur Heart J 2022;43:
5. De Caterina R, Liga R, Boden WE. Myocardial revascularization in ischaemic car ehab663.
diomyopathy: routine practice vs. scientific evidence. Eur Heart J 2022;43: 26. Rayner JJ, Rider OJ. Investigating the disease is the key to the obesity stigma. Eur
387–390. Heart J 2022;43:431.You can also read