Unprovoked Vestibular Burning in Late Estrogen-Deprived Menopause: A Case Series
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Unprovoked Vestibular Burning in
Late Estrogen-Deprived
Menopause: A Case Series
Martha F. Goetsch, MD, MPH
Department of ObGyn, Oregon Health & Science University, Portland, OR
h Abstract the vestibule are effective therapies, and physical therapy
Objective. This study aimed to document cases of se- can be important. With encouragement to avoid estrogen
vere menopausal vulvar burning localized to the vestibule. during menopause and with the increasing use of aroma-
Materials and Methods. Seven postmenopausal women tase inhibitors for breast cancer, menopausal unprovoked
presented to a vulvar clinic between 2007 and 2011 com- vestibulodynia may be increasing and can be challenging to
plaining of debilitating constant vulvar burning pain. They diagnose and treat. h
were treated according to the vulvar findings. Statistical
tools were descriptive.
Key Words: menopausal dyspareunia, vestibulodynia, vulvar
Results. The women’s ages ranged from 56 to 79 years
pain, vulvodynia, vulvovaginal atrophy
(mean age = 67 years). Pain had begun 1 to 4 years before
presentation (mean = 1.8 years) and was vestibular. Five
had contraindications to estrogen supplements. Only 1 pa-
C
tient was using estrogen; the mean number of years
hronic vulvar pain without a causative dermatologic
from menopause to onset of burning was16 years (range =
4Y27 years). Three patients developed pain during or or infectious explanation is termed vulvodynia and
after aromatase inhibitor therapy for breast cancer. Pelvic has been categorized as generalized or localized, pro-
floor myalgia was present in 3 patients. Of the patients, voked or unprovoked by the International Society for
3 improved on systemic estrogen, 3 improved using topi- Study of Vulvar Diseases [1]. Localized vulvodynia has
cal vestibular estrogen therapy, and 1 was managed with been described as a condition primarily in premenopausal
reassurance alone. Vestibulodynia regressed in those using
estrogen supplementation. One patient noted resolution
women, and it is typically painful with touch only, that is,
after localized removal of vestibular mucosa. provoked. The condition of generalized unprovoked
Conclusions. Severe unprovoked vestibulodynia can vulvodynia was described in perimenopausal and post-
present as unprovoked generalized pain in late menopause, menopausal women and was not linked to hormone
and topical lidocaine can aid the diagnosis. Constant pain status [2]. It is thought to be a centrally mediated neu-
can arise after years of only provoked pain or in association
ropathology without localized vulvar stigmata, whereas
with further lowering of estrogen from antiestrogen ther-
apy for breast cancer. Therapy to the vestibule can provide localized vestibulodynia has been found to have local
relief. Lidocaine and local application of estrogen cream to pathology in the form of neural hypertrophy with
lymphocyte and mast cell infiltrates on biopsy [3].
Clinically most generalized chronic vulvar burning is
present in both vulva and vestibule, whereas most pro-
Reprint requests to: Martha F. Goetsch MD, MPH, Oregon Health Sci-
ence University UNH 50, 3181 SW Sam Jackson Park Rd, Portland, OR 97239.
voked vulvodynia is localized to the vestibule and does
E-mail: goetsch@ohsu.edu not constantly burn.
The author has no conflicts of interest to declare.
This study was presented as a poster at the International Society for
The growing understanding of vulvodynia has evol-
Study of Vulvar Diseases conference in Paris, France, in September 2011. ved during a decade when national recommendations
regarding menopausal hormone therapy urge women to
Ó 2012, American Society for Colposcopy and Cervical Pathology
forgo hormone use or use the lowest doses for the shortest
Journal of Lower Genital Tract Disease, Volume 16, Number 4, 2012, 442Y446 time [4]. This case series presents 7 menopausal women
Copyright © 2012 American Society for Colposcopy and Cervical Pathology. Unauthorized reproduction of this article is prohibited.Vestibulodynia in late menopause & 443
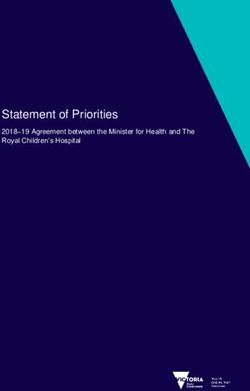
Table 1. Profiles of Women with Unprovoked Vestibulodynia
Contraindication
Patient no. to estrogen Symptoms Therapy
1 Breast cancer Constant burningVbecame suicidal Failed nortriptyline, pregabalin. Stopped aromatase inhibitor.
Used patch estrogen/progesterone. Tried PT.
2 None Annoying constant burning and Already used oral estrogen 1 mg. Insufficient help with oral
significant dyspareunia gabapentin. Trial of systemic and vestibular estrogen; later
had local mucosal resections.
3 Breast cancer BurningVhad to reduce sitting Topical estrogen to vestibule nightly, Y2 per week; later also
Later noted mons burning which gabapentin cream 6% to local area of mons daily
felt different
4 Thrombophilia BurningVcurtailed standingVlimited Lidocaine for symptom relief; estrogen cream to vestibule; PT
walking to 1 h
5 Breast cancer BurningVworrisome but tolerable Declined therapy
6 Severe cardiovascular disease Burning disturbed most days One course of topical estrogen to vestibule corrected
unprovoked pain. Topical doxepin 2% for labial pain/itching
7 None BurningVhad to stop sitting PT (limited)
Estradiol patch 0.05 mg
who were estrogen deplete and who developed significant usually every 3 to 6 hours. Local treatment was by
unprovoked vulvar pain. The locus was the vestibule, and regular applications of estrogen cream to the vestibule,
this was the focus of therapy. not the vagina. Estrogen therapy was either systemic
using estradiol patches or topical using estradiol cream
MATERIALS AND METHODS to the vestibule. For the latter, patients were instructed
Between 2007 and 2011, 7 menopausal women with to apply estrogen cream liberally to a cotton ball or
similar symptoms and histories were among those pre- small make-up pad and place it into the introitus at
senting to the author’s practice at the Oregon Health and bedtime nightly until they noted relief and then 2 or
Science University Program in Vulvar Health. Each 3 times per week for maintenance therapy. One patient
woman complained of noxious or debilitating constant who had unremitting localized tenderness was given an
vulvar burning pain. They were followed, and data were option of minor superficial surgery in the fashion pub-
tabulated from chart review with institutional review lished by the author [6]. Those who had muscle ten-
board approval (IRB #8288). The 7 patients were not derness were sent for physical therapy (PT). Statistical
the only menopausal women to present with these tools were descriptive.
complaints but were those noted by the author for later
review and comparison. Details of menopause, previous RESULTS
dyspareunia, estrogen status, and previous therapies At presentation, the mean age of the women was 67 years
were collected. Patients were examined in standard (range = 56Y79 years). The duration of pain had been
fashion with visual examination for atrophy and vulvar 1.8 years (range = 1Y4 years). The symptoms were
dermatoses. Examination of the vestibule was by cotton described as constant and burning in all 7 patients. Over
swab testing (using very light rolling touch) followed by time, pain had become exacerbated by sitting in 2 patients
local application of 4% aqueous lidocaine to the ves- and by standing in 1 patient, in whom increased pain
tibular mucosa, followed by a repeated swab test. The was also associated with urinary urgency. Pain resulted in
successful rapid temporary reversal of localized exqui- curtailment of usual ambulatory activities in 4 patients,
site tenderness by topical lidocaine is felt by the author 2 of whom had to reduce or stop sitting.
to discriminate between the peripheral localized nerve Mean years from menopause were 16 years (range =
hypertrophy of vestibulodynia and centrally mediated 4Y27 years). Only 1 patient was on estrogen, which
pain or referred pain [5]. Pelvic floor myalgia was was in the form of oral estradiol 1 mg. Of the 7 patients,
assessed by digital examination after the vestibule was 5 had contraindications to estrogen from previous breast
made comfortable with lidocaine. Patients were treated cancer (3 patients), severe coagulopathy with previous
according to the findings. Symptom relief was by fre- stroke (1 patient), and severe cardiovascular disease
quent self-applications of lidocaine aqueous 4%, gel (1 patient). Three patients had developed pain during or
2%, or ointment 5% to the vestibule for comfort, after therapy with an aromatase inhibitor for breast
Copyright © 2012 American Society for Colposcopy and Cervical Pathology. Unauthorized reproduction of this article is prohibited.444 & GOETSCH
cancer. One patient, who was the first patient to present, worsened again, however, and she resumed systemic
had had pain-free menopausal intimacy for 24 years estradiol. She continued having moderate vulvar pain,
with no hormone therapy, but she presented at age felt to be referred pelvic floor myalgia; she had limited
79 years after 1 year of aromatase inhibitor use with success with PT owing to limitations of home practice
debilitating constant vulvar burning, which made her owing to her age.
suicidal. Before the onset of unprovoked burning, 4 other The other 3 women with contraindications to estro-
patients had had years of dyspareunia necessitating gen elected local estrogen use, but it was not applied in
abstinence during menopause (range = 3Y20 years). The the vagina. Each used a poultice technique to apply
remaining 2 of 7 patients were not having coitus for other estradiol cream to the vestibule several nights per week.
reasons than vulvar pain. Although the patients perceived They were instructed to saturate estradiol cream into a
their pain as vulvar/vaginal, their physical findings all cotton ball, a small make-up pad, or a large cotton swab
had a vestibular locus, and application of topical lido- and place it in the vestibule while they slept or for
caine temporarily reduced their pain. All except for the 20 minutes per treatment. This therapy was successful in
patient on oral estrogen had visible changes of vaginal all cases, but it must be stated that it was hard for several
and vestibular atrophy. None had a vaginitis. Four patients women to locate the small area of allodynia. Pain was
(57%) had a secondary finding of pelvic floor muscle worst in either those longest in menopause or those who
tenderness. See Tables 1 and 2 for comparisons of symp- had used aromatase inhibitors to eliminate estrogen.
toms, therapy, and outcomes in the group. Treatment with oral neuromodulators had been unsuc-
Therapy focused on the vulvar vestibule in each case cessful in 2 women, 1 of whom then electing higher
and entailed comfort strategies of local topical lidocaine systemic estradiol therapy that helped but did not cor-
as well as therapy by addition of estrogen, which the rect the problem. She elected to have a localized super-
respective patients felt was reasonable despite their ficial vestibulectomy in the office, the equivalent of two
known risks. All but 2 patients had medical contra- 1- to 2-cm biopsy specimens removing a 2-mm thickness
indications to its use, but the degree of vulvar burning of affected mucosa around each Bartholin’s duct using
prompted 4 patients to use estrogen therapy, either local injected lidocaine 1% with epinephrine for anesthesia
or systemic, for the sake of quality of life. Patient 1, age and hemostasis. This was curative of her burning and
78 years, who had become suicidal, elected to dis- her dyspareunia, and she continued patch estrogen
continue the aromatase inhibitor and begin systemic therapy. Her surgical tissues showed hypertrophy of
patch estradiol with the agreement of her oncologist nerves identical to those noted in the premenopausal
after nortriptyline and pregabalin neuromodulators vestibulodynia tissues. In patient 6, the vestibulodynia
failed to help. Her vestibular examination became touch decreased from unprovoked to provoked, but because she
negative over time, and she was tried on tamoxifen as an was abstinent in her marriage for partner reasons, this was
alternative that might target breast receptors (estrogen a cure for her. However, once the vestibule was more
>) but not vulvar estrogen receptors. Her vestibulodynia comfortable, she reported annoying unilateral external
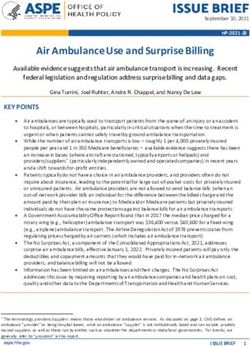
Table 2. Follow-Up and Final Outcomes
Patient
no. Length of follow-up, y Final outcome
1 1.7 Negative touch test results; intermittent pain from severe pelvic myalgia; continued patch
estradiol/norethindrone, nortriptyline; no breast cancer recurrence but developed lung cancer and died.
2 1.3 Complete correction of burning and dyspareunia after office mucosal vestibulectomy. Continues taking
estradiol/norethindrone patch.
3 3.3 Burning gone with maintenance 2 per week topical estradiol to vestibule. Corrected mons pain with topical
gabapentin 6% daily. Touch test result now negative in vestibule. Patient was very comfortable.
4 1.3 Comfortable on estradiol cream to vestibule 3 nights per week; uses topical lidocaine 5% as needed;
practices PT relaxation.
5 1 Did not wish to use estrogen due to breast cancer. Pain is minor, tolerable. She is celibate.
6 0.8 Topical estrogen course changed vestibulodynia from unprovoked to provoked (no symptoms). Noted
unilateral labial burning/itching, which responded well to topical doxepin 2% cream semiweekly
7 0.3 Did very limited PT due to cost; estradiol patch 0.05 mg helped other symptoms; burning unchanged;
able to have painless sex using lidocaine. One visit only with later telephone follow-up; then lost to
follow-up due to insurance issues and distance.
Copyright © 2012 American Society for Colposcopy and Cervical Pathology. Unauthorized reproduction of this article is prohibited.Vestibulodynia in late menopause & 445
burning, which was diagnosed as generalized vulvodynia, vulvodynia [12]. The use of the lidocaine test in this
and she was successfully treated with intermittent doses of cohort of women who had constant burning pain
topical doxepin cream. A second patient noted external allowed the vestibule, and therefore estrogen, to be
vulvar burning once the severe vestibular pain was cor- central to the therapeutic plan.
rected by vestibular estrogen; the use of daily topical A second issue raised by the study is that of the
gabapentin cream 6% was corrective. These 2 patients location and nature of vulvovaginal pain complaints
therefore had mixed localized and generalized vulvody- in menopausal women. The medical term has been
nia, each needing a different type of therapy. vulvovaginal atrophy and is known to improve with
estrogen therapy [13]. The term atrophy may not be
DISCUSSION appropriate for pain. Atrophy in other anatomic areas
This series describes the complaints and course of ther- is not a painful malady. Muscles that atrophy from
apy in 7 estrogen-deplete menopausal women who had disuse do not hurt. Moreover, not all menopausal
constant, and for most, debilitating vulvar burning pain. women with atrophy have complaints of pain, as was
It raises several issues, and it challenges some old the case with patient 1 who had no pain for 20 years of
assumptions. One issue is that of the nomenclature of untreated menopause until she underwent aromatase
vulvar pain and theories of etiology and treatment inhibitor therapy. It has been the author’s clinical
associated with that nomenclature. Another is the lan- experience that women with complaints of ‘‘vaginal
guage used in our field to describe menopausal vulvar dryness’’ actually have vestibular tenderness that
complaints, with atrophy reserved for the dyspareunia reverses with lidocaine and is consistent with the
from lack of estrogen and vulvodynia reserved for con- diagnosis of menopausal vestibulodynia. In mild cases,
stant pain. Atrophy is considered a vaginal pain com- vaginal estrogen therapy corrects the tenderness, but
plaint, and vulvodynia is considered an external vulvar for cases of severe allodynia, vaginal applications of
complaint. The third issue raised by this series is the estrogen are insufficient to correct the vestibule ten-
need to consider the use of local estrogen therapy in derness. Our group is writing up a study analyzing the
women with significant medical contraindications to surgical specimens from menopausal women who had
estrogen therapy. vestibulodynia despite estrogen therapy and who
Using standard International Society for Study of underwent successful vestibule surgery for their dys-
Vulvar Diseases nomenclature, the women in this series pareunia. It is our contention that the vulvar vestibule is
would seem to have presented with generalized vulvo- sensitive to withdrawal of estrogen in menopause and
dynia because of the unprovoked nature of the pain and develops the neuroinflammatory changes of vestibulo-
the ages of the women [2]. However, the examination of dynia alongside visual changes of atrophy and that the
the posterior vestibule, aided by the aqueous lidocaine vagina can develop marked atrophy but does not become
test, led to a more focused diagnosis. The vestibule tender to the same degree as the vestibule.
rather than the vulva became the target of therapy, and The 7 patients in this series each had a severe degree
the diagnosis shifted from generalized vulvodynia to of vestibulodynia causing spontaneous pain and dis-
localized but unprovoked vestibulodynia. In the author’s rupting activities of daily living. Five patients had
opinion, the rapid reversal of introital pain by lidocaine medical contraindications to estrogen therapy. Opting to
indicates a peripheral locus of pain consistent with ves- increase quality of life, 4 patients chose to take estrogen,
tibulodynia, an overgrowth of nerves with a well- and in 3 patients, this was administered using topical
described histologic appearance [7Y9]. Local peripheral estrogen cream to the vestibule. This is the first report of
excisional therapy is usually successful in correcting such therapy successfully targeting the vestibule rather
localized vestibulodynia but is considered an inap- than the vagina in correcting menopausal vulvar pain.
propriate therapy for centrally medicated pain [10, 11]. There are no data about absorption of estrogen from
The lidocaine test has been the author’s diagnostic the vestibule, but the assumption was made that because
mainstay for more than 20 years, but its efficacy rests on the surface area of the introitus is smaller than that of the
experiential evidence [5] because generalized vulvo- vagina, absorption would be very low. Absorption data
dynia is not considered to have identifying histologic are needed.
features to allow proof of distinguishing category. A This series presents women who either had pro-
consensus panel admonished the vulvar field to estab- longed absence of estrogen from years of menopause or
lish evidence-based definitions to clarify the types of were treated to lower circulating estrogen below usual
Copyright © 2012 American Society for Colposcopy and Cervical Pathology. Unauthorized reproduction of this article is prohibited.446 & GOETSCH
physiologic levels during menopause. Most menopau- 2. McKay M. Dysesthetic (‘‘essential’’) vulvodynia. Treat-
sal symptoms such as flushing and sweats fade rather ment with amitriptyline. J Repro Med 1993;38:9Y13.
than increase over time. This is not the case with dys- 3. Leclair C, Goetsch M, Korcheva V, Anderson R, Peters
pareunia, which has been noted to increase with longer D, Morgan T. Differences in primary compared with secondary
menopausal status [14]. The symptoms in this group had vestibulodynia by immunohistochemistry. Obstet Gynecol 2011;
117:1307Y13.
moved beyond pain with touch and had become constant
4. North American Menopause Society. Estrogen and
noxious or debilitating pain, which improved with
progestogen use in postmenopausal women: 2010 position
estrogen therapy. This may be a clinical variant of vesti-
statement of The North American Menopause Society.
bulodynia not described to date. The pain was so intense
Menopause 2010;17:242Y55.
that women found it hard to localize the discrete vestib-
5. Goetsch MF. Surgery combined with muscle therapy
ular area to treat. There were several examples of mis- for dyspareunia from vulvar vestibulitis: an observational
placed therapy, too external or too internal to the study. J Repro Med 2007;52:597Y603.
vestibule, requiring repeated office visits to instruct in 6. Goetsch M. Simplified surgical revision of the vulvar
technique and requiring a mirror for demonstration. The vestibule for vulvar vestibulitis. Am J Obstet Gynecol 1996;
oldest women had a harder time mastering topical 174:1701Y7.
applications of lidocaine or estrogen and home PT. 7. Weström L, Willen R. Vestibular nerve fiber prolifera-
Concomitant pelvic floor myalgia is a comorbidity com- tion in vulvar vestibulitis syndrome. Obstet Gynecol 1998;91:
monly seen with long-standing vestibulodynia, and in 572Y6.
some of these women, it was a second source of burning 8. Bohm-Starke N, Hilleges M, Falconer C, et al. Increased
pain and also needed directed therapy. intraepithelial innervation in women with vulvar vestibulitis
For approximately 8 years, since the publication of the syndrome. Gynecol Obstet Invest 1998;46:256Y60.
Women’s Health Initiative, various national organiza- 9. Goetsch MF, Morgan TK, Korchova VB, Li H, Peters
tions have urged that women minimize estrogen exposure D, Leclair CM. Histologic and receptor analysis of primary
and secondary vestibulodynia and controls: a prospective
during menopause [4]. In addition, there are 2.5 million
study. Am J Obstet Gynecol 2010;202:614.e1Y8.
US survivors of breast cancer for whom estrogen is con-
10. Tommola P, Unkila-Kallio L, Paavonen J. Surgical
traindicated [15]. This report of 7 women with burning
treatment of vulvar vestibulitis: a review. Acta Obstet Gynecol
vulvar pain after prolonged lack of estrogen raises the
Scand 2010;89:1385Y95.
possibility of an emerging menopausal problem of
11. Haefner H, Collins M, Davis G, Edwards L, Foster D,
unprovoked vestibulodynia. Some patients have found Hartmann E, et al. The vulvodynia guideline. J Lower Gen
their way to our specialized clinic after failing therapies Tract Dis 2005;9:40Y51.
advanced by specialists in pain management or urology, 12. Bachman G, Rosen R, Pinn V, Utian W, Ayers C,
and even gynecologists are not associating the long Basson R, et al. Vulvodynia: a state-of-the-art consensus on
estrogen deprivation with late onset of burning vulvar definitions, diagnosis and management. J Repro Med 2006;
pain. The condition is challenging to diagnose as well as 51:447Y56.
to treat but needs to be in the differential diagnosis of 13. ACOG Practice Bulletin No. 93: diagnosis and man-
burning vulvar pain in menopausal women. agement of vulvar skin disorders. Obstet Gynecol 2008;111:
1243Y53.
14. Kao A, Binik Y, Kapuschiinski A, Khalife S. Dyspar-
REFERENCES eunia in postmenopausal women: a critical review. Pain Res
1. Moyal-Barracco M, Lynch PJ. 2003 ISSVD terminology Manag 2008;13:243Y54.
and classification of vulvodynia a historical perspective. J 15. US breast cancer statistics, 2010. Available at: http://
Reprod Med 2004;49:772Y77. seer.cancer.gov/statfacts/html/breast.html. Accessed June 2012.
Copyright © 2012 American Society for Colposcopy and Cervical Pathology. Unauthorized reproduction of this article is prohibited.You can also read