The NSW approach to value based healthcare - George Leipnik Director, Strategy and System Priorities Strategic Reform and Planning Branch - ACT Health
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The NSW approach to value based healthcare George Leipnik Director, Strategy and System Priorities Strategic Reform and Planning Branch
Why do we need to adapt?
Healthcare worldwide There is increasing
is changing with rising demand and
health costs and complexity of
new technologies delivering care
The needs and
Patients are taking
expectations
a more active role in
of patients, carers,
their healthcare and
clinicians and
choices about what
communities
matters to them
continue to grow
NSW Health has developed a framework to support a shared understanding of value based healthcare
How do we frame the move to value based healthcare?
Building on the
good work already
occurring, aligned
narrative
Long-term
evolution, not a
Systematic measurement
discrete project
of outcomes
Maximise
outcomes from Re-prioritising
the patient
perspective
4
What distinguishes value based healthcare?
NSW Health’s approach to move towards value based healthcare

Integrated Care
LHDs implementing at least one evidence
based integrated care initiative from the ED to • Reducing ED attendance for
five options Community frequent users
Residential • Targeted support for
Body copy Residential Aged Care
Aged Care settings
Ideas
Scaled Vulnerable • Community support for
Ideas Initiatives Families
vulnerable parents and
children
Ideas Specialist • NSW Health outreach to
Care in Primary Care to enhance
Primary Care capability
Paediatrics • Reducing travel burden for
Network regional paediatric patients
Sensitive: NSW Cabinet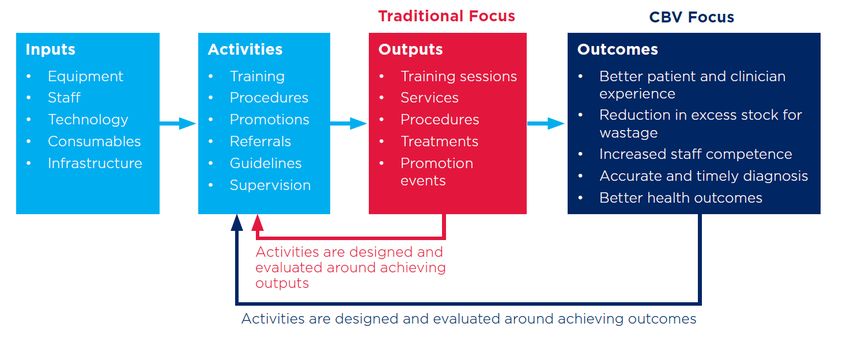
Collaborative
Horizon Commissioning
3: Collaborative Commissioning
Principles
1. Evidence based focus on regional 2. Collaboration to improve care 3. Joint accountability across 5. Sustainability through realignment of
4. Flexible purchasing arrangements existing resources
need and priorities for patients and outcomes for patients providers
20%
Local co-
commissioning
Local needs
Commissioning
Service delivery
LHD
PHN
Governance Partners Funding
PCCG Executive Provider agreement
PCCG Director of Operations Flexible provider
Partners funding
Service Providers Shared Benefits
8
Commissioning for Better Value
9
Leading Better Value Care
• Identifying and scaling evidence based initiatives to
improve outcomes across the quadruple aim
• Focuses on specific conditions or risk factors
• All local health districts working on the same initiatives
at the same time
• Strategy and system management from the Ministry
• Solution development and implementation support from
Pillars
• Flexible local implementation
• Consistent measurement, monitoring and evaluation
A structured statewide program for value based healthcare
10Tranche 1
clinical initiatives
Chronic Chronic Diabetes Diabetic
heart obstructive mellitus high risk
failure pulmonary foot services
disease
Renal Falls in Osteoarthritis Osteoporosis
supportive hospital chronic care re-fracture
care prevention
11Tranche 2
clinical initiatives
Hypofractionated Direct access
radiotherapy for colonoscopy
early stage
breast cancer
Hip
fracture
care
Chronic wound Bronchiolitis
management
12LBVC: Approach to measurement
Registry of
Patient Outcomes,
Economic Quarterly Activity Costing
reported Value & Evaluations
Assessment Monitoring Benefit Studies
measures Experience
(ROVE)
Economic
justification, Used in real- Assess actual Linked data Measure
cost avoided, Monitor and time and for Repurposing, service costs across journey impact
inform influence evaluation and inform for accurate is critical to across four
purchasing, change analysis purchasing funding understand dimensions
ensure value of value
sustainability
“The rigour of the program appeals to people. The
evidence of the data and models have reduced the
squeaky wheels. This makes LBVC look a bit different to
other programs or strategies that have come before”.
Executive Sponsor, LHDLBVC: Early results
► More than 100 health facilities now have a Leading Better
In 2019-20 compared to BAU:
Value care initiative in place
► Early data indicates that the initiatives are freeing up 390
capacity in hospitals – we are “bending the curve” fewer patients need joint
replacement operations
3,200
fewer patients with diabetes
need hospitalisation
for HRFS
1,200
fewer patients need
hospitalisation for refractureKey lessons to date
Feedback from our local health districts:
► Enabling environment from a structured state-wide program
has been well received
► Initiatives need authorised clinical consensus
► Executive and clinical leadership are critical success factors
► Different implementation approaches and models in rural
(allied, community and primary led) and metropolitan districts
(medical and specialist led)
► Change fatigue. Work required to implement is significant and some
see it as ‘additional’ or a short-term project
► Case for change provided through data was critical to minimising
resistance
► It takes time to build understanding and capability to repurpose
avoided costs
15More Information
For more information visit:
www.health.nsw.gov.au/value
16You can also read