Technical and pictorial file presentation - q-fin.de
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Technical and pictorial file
presentation
Table of content
Executive summary 3
I Introduction 3
II The way forward 3
III Background information 4
IV Major areas of intervention 4
Target group 4
V Vision and mission 6
Values 6
VI Objectives 7
VII Strategy 7
VIII Human Resources 8
IX Geografical location 8
X Modernisation of the centre 9
X. A Health care facilities 9
X .B Occupational therapy and income generating facilities 12
X. C Support facilities 12
X. D Preparation of traditional medicine 15
XI Function of the centre 16
XII Statistics in mental health (traditional and modern) 16
XII. A Frequencyof hospitalisation 16
XII. B Frequency of external consultation 16
XII. C Prevelance of mental illnesses in BIMEHC 17
XII. D Most prescribed psychiatric medication 17
XIII Partner organisations 17
XIV Conclusion and perspectives 18
Contact details 19
annex WHO: Seven good reasons for integrating mental health into primary care 20
BIMEHC 2
Summary Cameroon has just few government run mental health care facilities. Babungo Integrated Mental Health Care (BIMEHC) is a traditional/modern mental and primary health care facility in the Ngoketunjia Division in the North West Region. The variety of care, therapies and income generating activities as well as the comfortable, hygienic housing facilities offers a unique and therapeutic setting to treat people with mental disorders and basic health problems. BIMEHC has the facilities and capacity to function as a training center for community based integrated health care. Collaboration with the government would serve the disadvantaged people, staffs in training (both medical and paramedical) and the promotion of mental health enormously. BIMEHC can help to realise the goals that are mentioned in the Strategic Planning of the Ministry of Public Health 2001-2015. I-Introduction Cameroon has few government run mental health facilities to care for psychiatric patients (Hôpital Jamot Yaoundé and Laquintinie in Douala), where the few psychiatrists are working. In nearly all the regions, the mental health units in the Regional Hospitals are not functional due to a lack of specialised staff. Traditional practitioners try to fill the gap and are treating mental health patients; often to no avail. The lack of sufficient mental health facilities in Cameroon in general and the North West Region more specific justifies a setup like Babungo Integrated Health Care (BIMEHC). It is a reality that Cameroon’s population values/frequents visits to traditional healers The integrated combination of traditional and modern psychiatric care and basic health care in BIMEHC fills the gap that is tangible in Cameroonian communities. WHO states that integrated care helps to reduce the stigma associated with seeking help from stand-alone mental health services. An integrated service encourages the early identification and treatment of such disorders and thus reduces disability. Among other possible benefits are the provisions of care in the community and opportunities for community involvement in care ¹ ¹The mental health context. Geneva, World Health Organization, 2003 (Mental Health Policy and Service Guidance Package). II- The way forward There is a necessity to reinforce and reorganize the national system of mental health. Building new hospitals in other parts of the country would imply huge budgets. More efficient is exploiting the existing means and improve them systematically. BIMEHC has a proven record of being successful in integrating mental and basic health care in the community and can therefore serve as an example for future projects. BIMEHC 3

III- Background information
The founder of BIMEHC, Pa Mathias TUMENTA (1935-2009), started in 1959
treating his first patients traditionally.
In 1989, he was granted an official recognition from the government as a traditional
healer.
In 2001, Charity Health Foundation (registration number LT/GP/30/01/3399) took the
traditional home as an annex to carry out primary health care with modern
medication.
In June 2003, a Dutch VSO (Voluntary Services Overseas) volunteer took up a
placement, which was succeeded by a Kenyan VSO volunteer in September 2006,
Currently the Dutch VSO volunteer and a UK VSO volunteer are working in BIMEHC.
The home was registered as a Common Initiative Group in May 2004 with
registration number NW 30/04/8492 with the name Babungo Integrated Health Care
(BIHC).
Since the end of 2003 BIMEHC has developed itself enormously. Through national
and international assistance; the infrastructure improved drastically.
Papa Matthias Tumenta Wambo (1935-2009) founded a
traditional psychiatric home in the early sixties. In 2004 BIMEHC
was registered as a CIG.
Tweke John Tumenta
General Manager BIMEHC
(community nurse and traditional
healer)
IV-The major areas of intervention:
modern and traditional mental health care
primary health care
health education
support programme for People Living With HIV & AIDS (PLWHA)
Activities are expanded to cover other areas such as Human Rights and advocacy for
underprivileged groups, income generating activities, capacity building workshops,
watershed protection, sustainable agriculture, entrepreneurship, education and livelihoods.
Target group
• People with a mental health problem
• People in need for primary health care
• People living with HIV&AIDS
• Vulnerable children and orphans
BIMEHC 4
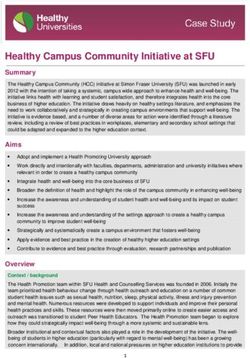
BIMEHC before
2004
Psychiatric wards
Patients shared rooms, slept on broken bamboo beds with grass matresses and
cooked inside the rooms
bathroom
and
toilets
BIMEHC 5
Primary Health Care
Consultation room Pharmacy and dressing room
Wards
V- Vision and mission.
Vision: A society in which, all persons, especially the underprivileged, are accepted and
have access to basic health care, economic resources and social facilities enabling them to
live a satisfying life.
Mission: To contribute to this vision we engage in domains such as the provision of mental
and primary health care for the poor; empowerment of underprivileged groups, sensitisation
of communities, promotion of sustainable agriculture and income generating activities. We
establish this through health care services, training, research, public - private partnerships
and international relations.
BIMEHC recognizes that its vision and mission can only be successfully achieved with a
qualified, devoted and experienced staff working on issues developed with the active
participation of the beneficiaries.
Values
Respect for fundamental human rights
Assurance of equal opportunity for all persons irrespective of ethnicity, religion, age
or gender
Professional integrity, transparency and accountability
Teamwork and collaboration
BIMEHC 6
VI- Objectives
Main objective:
to promote and provide traditional and modern mental and primary health care for
disadvantaged groups in Cameroon.
Specific objectives:
To promote access to mental and primary health care for disadvantaged groups
To holistically assist and care for people with mental health and primary health care
problems and their families by the use of traditional and conventional medicine and
approach.
To assist and equip people with mental health problems and HIV&AIDS with skills
and knowledge to facilitate their reinsertion and reintegration in society
To support income generating activities for these underprivileged groups
To promote food security and sustainable agriculture
To support education of the children from the underprivileged homes with focus on
the girl child
To advocate for mental health and the prevention of HIV&AIDS
To enhance the protection of the medicinal garden and the natural resources
To collaborate with the Faculty of Medicine and Biomedical Sciences, the Training
school for psychiatric nurses in Yaoundé and other mental health training institutions.
To expand the frontiers as training, research and resource centre to the public and
other mental health associations.
To build the capacity of the association’s staff
To support education of the children from the underprivileged homes with focus on
the girl child
VII-Strategy
Globally, BIMEHC’s strategy focuses on a combination of local and external resources to
enable local people, especially the poor and underprivileged to improve their own conditions
of life. Gender is mainstreamed in all its endeavours.
Essentially its strategy includes:
The setting up and maintenance of basic health care facilities (mental and primary
health care)
Capacity building of the staff
Target group involvement at all levels of the project cycle
Seed centre, processing and demonstration units (piggery, poultry and gardening)
Training, demonstrations and follow up
Human rights and Advocacy
Networking and maintaining collaborative partnerships with local and international
partners
Fundraising
BIMEHC 7
VIII- Human resources
1 General Manager
2 SR nurses (1 is a volunteer)
1 Laboratory technician
1 General Practioner (once a week)
1 Psychiatrist (monthly consultation)
1 Herbal/Convential pharmacist
1 Administrator
1 Project coordinator (medicial antropologist/sociologist)
1 Herbalist
3 Support staff
1 hotel/catering staff
2 International volunteers (psychiatric nurse/sociotherapist and management
specialist)
IX- Geographical location
The centre lies on a surface of 5 hectares on the foot of a mountain offering a
panoramic view of mountain chains with a waterfall, a panoramic view of rice field
cultivation of Ndop.
The centre is crossed by two rivers producing a sonore and beautiful atmosphere of
water clapotis.
All along the year, the climate is cold and a bit humid offering an ideal setup for the
recovery and rest of mental patients and people tired by their activities.
The presence of many bird species offers a musical boom during the first hours of the
morning.
Centre isolated (at 10 km from Ndop on the ring road towards Kumbo), away from
sound pollution and which offers a calm surrounding, appeasing, restfully and
therapeutic.
BIMEHC 8
The new Primary Health Care facility
X - Modernisation of the centre
Plurality of availability of care, health democracy of care in BIMEHC: an answer to
medical nomadic health seeking behaviour.
A. Health care facilities:
Construction of modern buildings since 2005:
pro-pharmacy
laboratory and examination room
consultation room both in and outpatients
maternity room
treatment room
duty room
store rooms
54 beds for psychiatric patients
32 beds for the section of PHC
psychotherapy hall for individual, couple and family therapy herbal pharmacy (drying,
preparation and store rooms)
BIMEHC 9
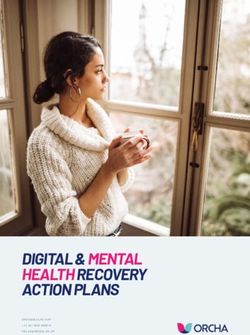
Psychiatric wards: each room has two beds
for the patient and the carer
Propharmacy
Laboratory
BIMEHC
BIMEHC 10Consultation rooms and duty room
Every room has 2 beds, one for the
patient and one for the carer. It is
not allowed to cook inside.
BIMEHC 11B. Occupational therapy and income generating facilities:
Multidisciplinary hall (occupational therapy, sanitary and health education, seminars,
conferences, formation of staff, leisure activities, church)
restaurant for patients, carers, staff and visitors
piggery house
poultry house
grinding mill and feed store house
field for outdoor games and sport
medicinal plants and vegetable garden
C. Support facilities
7 lodging houses for personnel
4 guesthouses (28 beds for passerby tourists, visitors and international volunteers)
restaurant for patients, carers, staff and visitors
administrative block (3 rooms)
souvenir shop with creative works from (ex)patients
8 toilet/bathroom blocks
indoor and outdoor kitchen
primary school
solar energy installation for the health care centre, staff quarter and guesthouses
(also to assure cold chain for vaccines)
Community hall
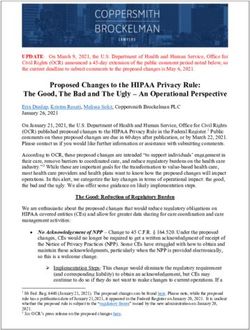
BIMEHC 12Community hall is being
used for health education,
workshops and leisure
activities.
Administrative block and
psychotherapy room
BIMEHC 13Patients and carers have the choice to
use the canteen or cook for themselves
in the indoor or outdoor kitchen.
Piggery and
poultry
Income generating
activities are also
used as
occupational
therapy
BIMEHC 14D. Preparation of traditional medicine
• Garden of psychotropic medicinal
plants at the premises of BIMEHC.
• Drying and storage of medicinal
plants in shaded room
Daily fresh preparation of concoctions and
storage in the refrigerator
Games and sports
BIMEHC 15Guesthouses and international volunteer lodging facilities
XI- Function of the centre
mental health care
preventive and curative care
rehabilitation and reinsertion
community based care
psychotherapy and conflict resolution
referral system and contra referral
vaccination programme
health education
programme of telemedicine (tele-psychiatry)
HIV&AIDS support group
microfinance activities for disadvantaged groups
XII- Statistics in mental health (traditional and modern)
A. Frequency of hospitalisation:
one week observation and diagnostics
stabilising patients with traditional and modern medication
average hospitalisation is about 3 to 6 months
monthly follow up after discharge
average of 20 psychiatric inpatients
B. Frequency of external consultation
average of 450 patients per year
BIMEHC 16C. Prevalence mental illnesses in BIMEHC
Depression
Schizophrenia
Bipolar disorder
Acute psychosis
Toxicomania
Obsessive compulsive disorder
Phobia
Hysteria
Post natal depression
Epilepsy
Dementia
D. Most prescribed psychiatric medication:
Antipsychotics:
Largactil® (Chlorpromazine)
Modecate® (Fluphenazine deconoate)
Haldol® (Haloperidol)
Risperdal® (Risperidon)
Mood stabilizers:
Tegretol® (Carbamazepine)
Depakine
Benzodiazepines:
Temesta® (Lorazepam)
Valium® (Diazepam)
Tranxene® (clorazapinezuur)
Antidepressants:
Anafranil® (Clomipraminehydrochloride)
Prozac® (Fluoxetine)
Corrector:
Artane® (Trihexyfenidyl)
Akineton® (Biperideen)
XIII- Partner organisations
National:
Habitat for Humanity Cameroon
Soeur Hospitalier du Sacré Coeur de Jésus, Benoît Menni
PRTC Fonta
Development for Humanity Cameroon
Government units (Ndop district hospital)
Care Help Cameroon
International:
Babungo Foundation (Netherlands)
Voluntary Services Overseas (VSO)
BIMEHC 17XIV- Conclusion and perspectives
Care : community based mental and primary health care
Training: Practical formation, academic stage, research and impregnation stages:
practical internships for students in medicine and psychiatry. Internships for
paramedical students: psychology, sociology, psychiatric nurses and state registered
nurses.
Research: Operational research in mental health (DPS, DLM, DRO)
International partnership: Tele-psychiatry (Switzerland, the Netherlands).
Advocacy: contribution to the promotion of mental health.
Intersectional collaboration: health-social welfare-agriculture-economy-education
BIMEHC 18Contact details
General Manager: Tweke John Tumenta
Address: Babungo Integrated Mental Health Care (BIMEHC)
Mbenjeh Babungo
P.O. Box 6 Ndop
Babessi subdivision
North West Region, Cameroon
Telephone: (+237) 79834047 / 98328062
Email: bihcare@yahoo.com
johntumenta@yahoo.com
Website: www.babungo.org
Registration number: BIHC: NW/GP/30/04/8492
BIMEHC 19ANNEX Seven good reasons for integrating mental health into primary care² 1. The burden of mental disorders is great. Mental disorders are prevalent in all societies. They create a substantial personal burden for affected individuals and their families, and they produce significant economic and social hardships that affect society as a whole. 2. Mental and physical health problems are interwoven. Many people suffer from both physical and mental health problems. Integrated primary care services help ensure that people are treated in a holistic manner, meeting the mental health needs of people with physical disorders, as well as the physical health needs of people with mental disorders. 3. The treatment gap for mental disorders is enormous. In all countries, there is a significant gap between the prevalence of mental disorders, on one hand, and the number of people receiving treatment and care, on the other hand. Primary care for mental health helps close this gap. 4. Primary care for mental health enhances access. When mental health is integrated into primary care, people can access mental health services closer to their homes, thus keeping their families together and maintaining their daily activities. Primary care for mental health also facilitates community outreach and mental health promotion, as well as long-term monitoring and management of affected individuals. 5. Primary care for mental health promotes respect of human rights. Mental health services delivered in primary care minimize stigma and discrimination. They also remove the risk of human rights violations that can occur in psychiatric hospitals. 6. Primary care for mental health is affordable and cost effective. Primary care services for mental health are less expensive than psychiatric hospitals, for patients, communities and governments alike. In addition, patients and families avoid indirect costs associated with seeking specialist care in distant locations. Treatment of common mental disorders is cost effective, and investments by governments can bring important benefits. 7. Primary care for mental health generates good health outcomes. The majority of people with mental disorders treated in primary care have good outcomes, particularly when linked to a network of services at secondary level and in the community. ² Integrating mental health into primary care, a global perspective. Geneva, World Health Organization & World Organization of Family Doctors, 2008 BIMEHC 20
You can also read