Summary of the CY 2022 Physician Fee Schedule Proposed Rule
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Summary of the CY 2022 Physician Fee Schedule Proposed Rule On July 13, 2021, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule that updates Medicare payment policies, reimbursement rates, and quality reporting for services furnished under the Calendar Year (CY) Medicare Physician Fee Schedule (PFS) on or after January 1, 2022. The rule will be published in the Federal Register on July 23, 2021. We will be working with you and your teams to develop comments on this proposed rule, which are due on September 13th. A broad fact sheet on the PFS proposed rule can be found on the CMS website here. A detailed fact sheet on changes specific to the Quality Payment Program can be found here. A press release on the proposed rule is located here. Below we provide highlights of the proposed rule policies impacting physicians and other clinicians that we believe have some relevance to plans and on which we will consider commenting. If there are other sections you believe we should consider for comment, please let us know. CY 2022 PFS Ratesetting and Conversion Factor The proposed CY 2022 PFS conversion factor is $33.58, a decrease of $1.31 from the CY 2021 PFS conversion factor of $34.89. This includes a reduction due to the expiration of the 3.75% payment increase provided for CY 2021 by the Consolidated Appropriations Act, 2021 (CAA). There is no inflationary update factor per Medicare Access and CHIP Reauthorization Act of 2015 (MACRA); updates will resume in CY 2026. Budget neutrality adjustments are applied to account for changes in relative value units (RVUs) as required by law when revisions to the RVUs cause expenditures for the year to change by more than $20 million. AHIP.ORG 1
Evaluation and Management (E/M) Visits
For CY 2022, CMS is making several proposals to account for recent changes to E/M visit codes, as
explained in the AMA CPT Codebook, which took effect January 1, 2021. CMS also clarifies and refines
policies that were reflected in certain manual provisions that were recently withdrawn. Specifically, CMS
proposes several refinements to the agency’s current policies for split (or shared) E/M visits, critical
care services, and services furnished by teaching physicians involving residents.
Split (or shared) E/M visits
CMS proposes a number of changes to its policies regarding split (or shared) E/M visits to address the
evolving role of non-physician practitioners (NPPs) as members of the medical team, and to clarify
conditions of payment that must be met to bill Medicare for these services. Specifically, CMS proposes
the following:
• Definition of split (or shared) E/M visits as E/M visits provided in the facility setting by a
physician and an NPP in the same group.
• The practitioner who provides the substantive portion of the visit (more than half of the total time
spent) would bill for the visit.
• Split (or shared) visits could be reported for new as well as established patients, and initial and
subsequent visits, as well as prolonged services.
• Requiring reporting of a modifier on the claim to help ensure program integrity.
• Documentation in the medical record that would identify the two individuals who performed the
visit. The individual providing the substantive portion must sign and date the medical record.
Critical Care Services
CMS proposes a number of changes to its policies related to critical care services. First, CMS
proposes to use American Medical Association (AMA) Current Procedural Terminology (CPT®)
prefatory language as the definition of critical care visits, including bundled services. Additionally, CMS
proposes to allow critical care services to be furnished concurrently to the same patient on the same
day by more than one practitioner representing more than one specialty, and that critical care services
can be furnished as split (or shared) visits. Additionally, CMS proposes that no other E/M visit can be
billed for the same patient on the same date as a critical care service when the services are furnished
by the same practitioner, or by practitioners in the same specialty and same group to account for
overlapping resource costs. Finally, CMS proposes that critical care visits cannot be reported during the
same time period as a procedure with a global surgical period.
Teaching Physician Services
The AMA CPT office/outpatient E/M visit coding framework that CMS finalized for CY 2021, under
which practitioners can select the office/outpatient E/M visit level to bill, was based either on use of the
total time personally spent by the reporting practitioner or medical decision making (MDM). Under the
agency’s existing regulations, if a resident participates in a service furnished in a teaching setting, a
teaching physician can bill for the service only if they are present for the key or critical portion of the
service. Under the so-called “primary care exception,” Medicare makes PFS payment in certain
teaching hospital primary care centers for certain services furnished by a resident without the physical
presence of a teaching physician.
AHIP.ORG 2CMS proposes to clarify that the time when the teaching physician was present can be included when
determining E/M visit level. Under the primary care exception specifically, only MDM would be used to
select the visit level to guard against the possibility of inappropriate coding that reflects residents’
inefficiencies rather than a measure of the time required to furnish the services.
Vaccine Administration Services Comment Solicitation
The proposed rule includes a comment solicitation around the costs involved in furnishing preventive
vaccines to inform the development of more accurate rates for these services. Specifically, CMS is
seeking information on:
• The different types of health care providers who administer vaccines and how that has changed
since the beginning of the pandemic.
• How the costs of furnishing flu, pneumococcal and hepatitis B vaccines compare to the cost of
furnishing COVID-19 vaccines.
• How the PHE may have impacted costs, including whether those costs will continue beyond the
PHE.
Additionally, CMS seeks input on (1) its policy implemented earlier this year to pay a $35 add-on
for each vaccine dose for certain vulnerable beneficiaries when they receive a COVID-19 vaccine at
home and what should qualify as a “home;” (2) whether CMS should treat monoclonal antibody
products the same way it treats other physician-administered drugs and biologicals under Medicare
Part B, meaning 95% of AWP in the physician office setting, and a reasonable cost in hospital
outpatient departments.
Telehealth
In this proposed rule, CMS has put forth several provisions to extend temporary coverage of some
telehealth services and make permanent coverage and payment for other services. The agency notes it
is evaluating whether or which services should be permanently added to the telehealth list following the
COVID-19 PHE. In the meantime, CMS proposes to allow certain services added to the Medicare
telehealth list to remain on the list until December 31, 2023.
Retention of Category 3 Telehealth Services
In the CY 2021 PFS Final Rule, CMS created a third temporary category of criteria for adding services
to the list of Medicare telehealth services. Category 3 describes services added to the Medicare
telehealth list during the public health emergency (PHE) for the COVID-19 pandemic (COVID-19 PHE)
that will remain on the list through the calendar year in which the PHE ends. In the CY 2021 PFS Final
Rule CMS added the following services to the Medicare telehealth list on a Category 3 basis,
establishing coverage and payment for those services through the end of the year in which the PHE
expires:
• Domiciliary, Rest Home, or Custodial Care services, Established patients (CPT codes 99336-
99337)
• Home Visits, Established Patient (CPT codes 99349-99350)
• Emergency Department Visits, Levels 1-5 (CPT codes 99281-99285)
AHIP.ORG 3• Nursing facilities discharge day management (CPT codes 99315-99316)
• Psychological and Neuropsychological Testing (CPT codes 96130-96133; CPT codes 96136-
96139)
• Therapy Services, Physical and Occupational Therapy, All levels (CPT codes 97161-97168;
CPT codes 97110, 97112, 97116, 97535, 97750, 97755, 97760, 97761, 92521-92524, 92507)
• Hospital discharge day management (CPT codes 99238-99239)
• Inpatient Neonatal and Pediatric Critical Care, Subsequent (CPT codes 99469, 99472, 99476)
• Continuing Neonatal Intensive Care Services (CPT codes 99478-99480)
• Critical Care Services (CPT codes 99291-99292)
• End-Stage Renal Disease Monthly Capitation Payment codes (CPT codes 90952, 90953,
90956, 90959, 90962)
• Subsequent Observation and Observation Discharge Day Management (CPT codes 99217;
CPT codes 99224-99226)
In this rule, CMS is proposing to retain all services added to the Medicare telehealth services list on a
Category 3 basis until the end of CY 2023.
Telehealth for mental health services
Section 123 of the CAA removed the geographic restrictions and added the home of the beneficiary as
a permissible originating site for telehealth services when used for the purposes of diagnosis,
evaluation, or treatment of a mental health disorder. However, the law also added a requirement for an
in-person, non-telehealth service with the physician or practitioner within six months prior to the initial
telehealth service, and thereafter, at intervals as specified by the Department of Health and Human
Services. This requirement would apply only to the mental health telehealth services made possible by
the CAA; that is, it would apply only to services delivered to patients in their homes (regardless of the
geographic location of the patient) and services delivered to patients in geographic locations beyond
those currently authorized for Medicare telehealth services.
In the CY2022 PFS proposed rule, CMS proposes changes to the current requirement for telehealth
visits to utilize an “interactive telecommunications systems,” defined as multimedia communications
equipment with audio and video equipment permitting two-way, real-time interactive communication
between the patient and distant site physician or practitioner. CMS proposes to allow the use of audio-
only communication technology when used for telehealth services for the diagnosis, evaluation, or
treatment of mental health disorders furnished to established patients in their homes when a beneficiary
is not capable of using, or does not consent to, the use of two-way, audio/video technology. CMS is
seeking comment on whether additional documentation should be required in the medical record to
support clinical appropriateness of the use of audio-only services, and whether audio-only services
should be precluded for some high-level services, such as Level 4 or 5 E/M visit codes. CMS also
seeks comments on what other guardrails should be considered when audio-only services are provided
for mental health care.
Opioid Treatment Program (OTP)
CMS proposes to allow OTPs to furnish counseling and therapy services via audio-only interaction
(such as telephone calls) after the conclusion of the COVID-19 PHE in cases where audio/video
AHIP.ORG 4communication is not available to the beneficiary, including circumstances in which the beneficiary is not capable of or does not consent to the use of devices that permit a two-way audio/video interaction, provided all other applicable requirements are met. CMS proposes to require that OTPs use a service- level modifier for audio-only services billed using the counseling and therapy add-on code and document in the medical record the rationale for a service being furnished using audio-only services, in order to facilitate program integrity activities. CMS also proposes several other modifications to regulations regarding the Part B OTP benefit. First, CMS proposes to adjust payments for take-home supplies of naloxone (including both the drug and associated services, finalized in the CY 2021 PFS final rule) for geographic and Medicare spending variation. In addition, CMS would create a new G-code describing a take-home supply of a new, higher dose naloxone product, and price the code using the same methodology used for existing codes in the benefit. Electronic Prescribing of Controlled Substances (ECPS) for Part D Drugs Section 2003 of the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities (SUPPORT) Act generally that prescriptions for controlled substances covered under a Medicare Part D prescription drug plan or Medicare Advantage Prescription Drug Plan (MA/PD) be transmitted by a health care practitioner electronically in accordance with an electronic prescription drug program, beginning January 1, 2021. Further, section 2003 of the SUPPORT Act provides CMS with the authority to, through rulemaking, enforce and specify appropriate penalties for noncompliance with the requirement for electronic prescribing of controlled substances (EPCS). CMS implemented Section 2003 of the SUPPORT Act through the CY 2021 PFS final rule and mandated electronic prescribing of Schedule II-V controlled substances under Medicare Part D beginning Jan. 1, 2021 and established January 1, 2022 as a compliance date for this requirement. However, given stakeholder input and the challenges create by the COVID-19 pandemic, CMS proposes to extend the compliance date for ECPS requirements until Jan. 1, 2023. CMS would further extend the compliance date for Part D controlled substance prescriptions written for beneficiaries in long-term care facilities until Jan. 1, 2025 due to the unique circumstances of these providers. In addition to revisions to the timing of these requirements, CMS also proposes that for prescribers to be considered compliant, they must prescribe at least 70% of their Part D controlled substance prescriptions electronically per calendar year. Proposed exceptions to this requirement would be for prescriptions issued where the prescriber and dispensing pharmacy are the same entity, prescribers who prescribe 100 or fewer Part D controlled substance prescriptions per year, prescribers who are prescribing during a recognized emergency (like a natural disaster or pandemic), and prescribers who request and receive a waiver from CMS due to extraordinary circumstances. CMS proposes that its compliance actions in CY 2023 would consist of sending letters to prescribers that the agency believes are violating the EPCS requirement. CMS also notes it will consider whether further compliance actions will be necessary in future rulemaking. AHIP.ORG 5
Therapy Services CMS is implementing the final part of section 53107 of the Bipartisan Budget Act of 2018, which requires CMS, through the use of new modifiers (CQ and CO), to identify and make payment at 85% of the otherwise applicable Part B payment amount for physical therapy and occupational therapy services furnished in whole or in part by physical therapist assistants (PTAs) and occupational therapy assistants (OTAs), for dates of service on and after January 1, 2022. For CY 2022 CMS proposes to revise the de minimis standard established to determine whether services are provided “in whole or in part” by PTAs or OTAs. Specifically, CMS proposes to revise the de minimis policy to allow a timed service to be billed without the CQ/CO modifier in cases when a PTA/OTA participates in providing care to a patient with a physical therapist or occupational therapist (PT/OT), but the PT/OT meets the Medicare billing requirements for the timed service without the minutes furnished by the PTA/OTA by providing more than the 15-minute midpoint (also known as the 8-minute rule). Physician Assistant (PA) Services Under current Medicare coverage policies, Pas may not bill Medicare directly for services furnished. CMS now proposes to implement provisions of the CAA starting January 1, 2022 to permit, Pas to bill Medicare directly for their services, incorporate with other Pas, and reassign payment to billing entities for their services. Beneficiary Coinsurance for Additional Procedures Furnished During the Same Clinical Encounter as a Colorectal Cancer Screening Colorectal cancer screenings do not entail beneficiary coinsurance, however, the addition of any procedure beyond the planned colorectal screening results in a beneficiary having to pay coinsurance. CMS proposes to implement special coinsurance rules for procedures that are planned as colorectal cancer screening tests but become diagnostic tests when the practitioner identifies the need for additional services (e.g., removal of polyps). CMS proposes to reduce the amount of coinsurance a beneficiary will pay for such services over time. CMS had previously finalized a proposal to increase the quality minimum performance standard to the 40th percentile in PY 2022. However, CMS proposes to delay this change until PY 2024 and instead freeze the quality performance standard at the 30th percentile MIPS quality performance category score for PY 2023. Quality Payment Program (QPP) Authorized by MACRA, the QPP is an incentive program that includes two participation tracks, the Merit-based Incentive Payment System (MIPS) and Advanced APMs. MIPS eligible clinicians are subject to a MIPS payment adjustment based on their performance in four performance categories: cost, quality, improvement activities, and Promoting Interoperability. If an eligible clinician participates in an Advanced APM and achieves Qualifying APM Participant (QP) status, they are excluded from the MIPS reporting requirements and payment adjustment. AHIP.ORG 6
MIPS Value Pathways (MVPs)
CMS proposes delaying MVP implementation until PY 2023. Through the CY 2020 PFS rulemaking
cycle, CMS created a new framework dubbed “MVPs” that connect measures and activities across the
four MIPS performance categories (Quality, Cost, Promoting Interoperability, and Improvement
Activities) that are relevant to a specialty, medical condition, or a particular population. The MVPs
would retain the full scope of Promoting Interoperability performance category requirements, as well as
population health claims-based measures as foundational elements, regardless of clinical focus.
Additionally, each MVP would include specific, clinically relevant measures and activities for the quality,
cost, and improvement activities performance categories. In the CY 2021 PFS final rule, CMS
established a set of criteria for use in the development and selection of MVPs. Specifically, CMS
finalized that it is not prescriptive on the number of quality measures that are included in an MVP.
In the CY 2022 PFS proposed rule, CMS proposes seven MVP candidate clinical topics and policies to
support implementation beginning in PY 2023. The agency believes delaying implementation beyond
the intended start date will provide clinicians the time needed to understand MVP requirements and
plan for any operational considerations. Specifically, CMS proposes following additions to the MVP
development criteria beginning with the 2022 performance year/2024 payment year:
• MVPs must include at least one outcome measure that is relevant to the MVP topic.
• Each MVP that is applicable to more than one clinician specialty should include at least one
outcome measure that is relevant to each clinician specialty included.
• In instances when outcome measures are not available, each MVP must include at least one
high priority measure that is relevant to the MVP topic.
• Allow the inclusion of outcomes-based administrative claims measures within the quality
component of an MVP.
• Each MVP must include at least one high priority measure that is relevant to each clinician
specialty included.
• To be included in an MVP, a qualified clinical data registry (QCDR) measure must be fully
tested.
CMS proposes to begin transitioning to MVPs in the 2023 MIPS performance year. CMS notes its intent
to gradually implement MVPs for more specialties and subspecialties that participate in the program.
The agency is requesting public comment on its aim to sunset traditional MIPS after the end of the
2027 performance and data submission periods. CMS is not proposing the timeframe in which MVP
reporting would no longer be voluntary and the future sunset of traditional MIPS at this time; any
proposal to sunset traditional MIPS would be made in future rulemaking.
The 7 proposed MVPs for the 2023 performance year align with the following clinical topics:
1. Rheumatology
2. Stroke Care and Prevention
3. Heart Disease
4. Chronic Disease Management
5. Emergency Medicine
6. Lower Extremity Joint Repair
7. Anesthesia
AHIP.ORG 7CMS proposes that MVP Participants would be required to report:
• Foundational layer (applicable to all MVPS):
o One population health measure (either Hospital-Wide, 30-day, All-Cause Unplanned
Readmission (HWR) Rate for the Merit-Based Incentive Payment System Program
(MIPS) Eligible Clinician Groups (finalized in CY 2021 final rule) or Clinician and
Clinician Group Risk-standardized Hospital Admission Rates for Patients with Multiple
Chronic Conditions (proposed).
o MVP Participants would report on the same Promoting Interoperability measures
required under traditional MIPS.
• Quality Performance Category:
o Four available quality measures one outcome measure (or a high-priority measure if an
outcome isn’t available or applicable).
• Improvement Activities Performance Category
o Participants would select one or two improvement activities, depending on how the
activities are weighted.
• Cost Performance Category
o CMS would calculate performance exclusively on the cost measures that are included in
the MVP using administrative claims data.
To allow more granular reporting from the MIPS program, CMS proposes to establish subgroup
reporting. Subgroup reporting would be voluntary for the 2023 and 2024 performance years. CMS
proposes that subgroups consist of “a subset of a group which contains at least one MIPS-eligible
clinician and is identified by a combination of the group Tax Identification Number (TIN), the subgroup
identifier, and each eligible clinician’s National Provider Identifier (NPI). In the initial years of subgroup
reporting, CMS proposes that it would be limited to clinicians reporting through MVPs or Alternative
Payment Model (APM) Performance Pathway (APP). Voluntary reporters, opt-in eligible clinicians, and
virtual groups would not be able to report to MIPS through an MVP for the 2023 performance year, due
to implementation challenges. However, CMS is requesting comment as to whether they should be
allowed to report MVPs in the future.
CMS proposes that the scoring for the MVPs would largely align with traditional MIPS. CMS also
proposes to provide comparative performance feedback within the annual performance feedback to
show the performance of like clinicians who report on the same MVP. CMS proposes to begin publicly
reporting subgroup-level performance information beginning with PY 2024 on the Care Compare tool
hosted by CMS.
APP
CMS proposes to allow MIPS eligible clinicians in MIPS APMs to report the APP as a subgroup,
meaning select clinicians within one TIN, beginning with the 2023 performance year. The definition of a
subgroup and eligibility to participate as a subgroup are the same for MVP and APP reporting.
AHIP.ORG 8Traditional MIPS
First, CMS proposes to expand the definition of a MIPS eligible clinician to include clinical social
workers and certified nurse mid-wives.
The Bipartisan Budget Act of 2018 requires a “gradual and incremental transition” for raising the
performance threshold during the first 5 years of the MIPS program. To address this requirement, CMS
proposes to establish the performance threshold using the mean final score from the 2017 performance
year/2019 MIPS payment year, which would result in a performance threshold of 75 points based on
historical performance data, which constitutes an increase of 15 points from the previous year.
For the 2022 performance year/2024 payment year, the performance category weights are: 30% for the
quality performance category (compared to 40% in 2021), 30% for the cost performance category
(compared to 20% in 2021), 15% for the improvement activities performance category, and 25% for the
Promoting Interoperability performance category, consistent with statutory requirements. CMS notes
the performance category weights are specified in statute, and the agency codified them in prior
rulemaking, and therefore they are not proposals available for comment.
For the quality performance category, CMS is making several proposals. First, the agency proposes
to update quality measure scoring to remove end-to-end electronic reporting and high-priority measure
bonus points as well as the 3-point floor for scoring measures (with some exceptions for small
practices). Next CMS proposes to use performance period benchmarks, or a different baseline period,
such as calendar year 2019, for scoring quality measures in the 2022 performance period as the
agency anticipates seeing fewer submissions for the 2020 performance period because of the
flexibilities offered due to the COVID-19 Public Health Emergency (PHE). Next the agency proposes to
extend the CMS Web Interface as a quality reporting option for registered groups, virtual groups, or
other APM Entities for the 2022 performance period. Additionally, CMS proposes to update the quality
measure inventory (a total of 195 proposed for the 2022 performance period). Finally, CMS proposes
to increase the data completeness requirement to 80% beginning with the 2023 performance period.
For the cost performance category, CMS proposes to add five newly developed episode-based cost
measures into the MIPS cost performance category beginning with the CY 2022 performance period:
• 2 procedural measures (melanoma resection, colon and rectal resection)
• 1 acute inpatient measure (sepsis)
• 2 chronic condition measures (diabetes, asthma/chronic obstructive pulmonary disease
[COPD]).
CMS is also seeking comment on the proposed process of cost measure development by stakeholders.
In the current measure development process, all cost measures are developed by CMS’s measure
development contractor.
For the improvement activities performance category, CMS proposes to update the improvement
activities inventory for the 2022 performance year, including adding new improvement activities about
health equity and standardizing language related to equity across the improvement activities inventory.
For the Promoting Interoperability performance category, CMS proposes to:
AHIP.ORG 9• Apply automatic reweighting to clinical social workers and small practices.
• Revise reporting requirements in the following ways:
o Revise reporting requirements for the Public Health and Clinical Data Exchange
objective to support public health agencies (PHAs) in future health threats and a long-
term COVID-19 recovery.
o Add a requirement in the Provide Patients Electronic Access to Their Health Information
measure that patients have access to their health information indefinitely, for encounters
on or after January 1, 2016.
o Require MIPS eligible clinicians to attest to conducting an annual assessment of the
High-Priority Guide of the Safety Assurance Factors for EHR Resilience Guides (SAFER
Guides) beginning with the CY 2022 performance period.
o Modify the Prevention of Information Blocking attestation statements to distinguish this
from separate information blocking policies under the Office of the National Coordinator
for Health Information Technology (ONC) requirements established in the 21st Century
Cures Act final rule.
CMS proposes to add affiliations for the following facility types on Care Compare:
• Long-Term Care Hospitals
• Inpatient Rehabilitation Facilities
• Inpatient Psychiatric Facilities Skilled Nursing Facilities
• Home Health Agencies
• Hospice
• End-Stage Renal Disease (ESRD) Facilities
CMS has also issued an RFI on utilization data. CMS is seeking information on how to make this
information more useful to consumers. Specifically, the agency is seeking information on types of and
number of conditions and procedures, data aggregation, information display, peer comparisons, and
claims lookback timeframe.
Medicare Shared Savings Program (MSSP)
In the 2021 final PFS, CMS finalized changes to quality and Merit-based Incentive Payment System
(MIPS) reporting for accountable care organizations (ACOs) in the MSSP. CMS now proposes to delay
certain aspects of previously finalized changes.
Specifically, CMS preciously finalized a new “a new Alternative Payment Model Performance Pathway
(APP)” where, ACOs must report clinical quality measure (CQM) using all-payer data rather than the
CMS Web Interface starting in PY 2022. CMS now proposes to extend the availability of the CMS Web
Interface collection type for two years, through PY 2023.
Specifically, CMS proposes that:
• For performance year 2022, ACOs would either report the 10 CMS Web Interface measures or
the 3 all-payer eCQMs/MIPS CQMs. Under the APP, all ACOs would administer the CAHPS for
MIPS Survey and be scored on 2 administrative claims-based measures (calculated by CMS).
• For performance year 2023, ACOs would either report the 10 CMS Web Interface measures
and at least one all-payer eCQM/MIPS CQM or the 3 all-payer eCQMs/MIPS CQMs. Under the
APP, all ACOs would continue to administer the CAHPS for MIPS Survey and be scored on 2
AHIP.ORG 10administrative claims-based measures (calculated by CMS). To transition ACOs to reporting all-
payer eCQM/MIPS CQM measures, the agency would only score the CMS Web Interface
measure set for an ACO that has also submitted at least one all-payer eCQM/MIPS CQM
measure.
CMS also proposes several other changes to various elements of the MSSP, including the
requirements around establishing repayment mechanisms, the MSSP application process, beneficiary
notification requirements, and the definition of primary care services that is used for beneficiary
assignment. In addition, CMS also seeks comment on the use of regional fee-for-service expenditures
in establishing, adjusting, updating and resetting the ACOs’ historical benchmarks.
Advancing to Digital Quality Measurement and the Use of Fast Healthcare
Interoperability Resources (FHIR) in Physician Quality Programs – Request
for Information
CMS reiterated its intention to transition fully to digital quality measurement in CMS quality reporting
and value-based purchasing programs by 2025. To support this transition, the agency is seeking
information on:
• Clarifying the definition of digital quality measures, including a potential definition for digital
measures.
• Using the Fast Healthcare Interoperability Resources (FHIR®) standard for eCQMs that are
currently in the various quality programs. This part of the RFI provides information on current
activities underway to align CMS eCQMs with the FHIR standard and support quality
measurement via application programming interfaces (APIs) and contrasts this approach to
current eCQM standards and practice.
• Standardizing data required for quality measures for collection via FHIR-based APIs.
• Leveraging technological opportunities to facilitate digital quality measurement.
• Better supporting data aggregation.
• Developing a common portfolio of measures for potential alignment across CMS regulated
programs, federal programs and agencies, and the private sector.
Closing the Health Equity Gap in CMS Clinician Quality Programs—
Request for Information (RFI)
CMS is seeking public comment on two potential future expansions of its work to address healthcare
disparities including: (1) future potential stratification of quality measure results by race and ethnicity,
and (2) improving demographic data collection. CMS is considering stratification of the
condition/procedure-specific readmission measures by race and ethnicity. To support such
stratification, CMS is seeking input on the potential future application of an algorithm to indirectly
estimate race and ethnicity to permit stratification of measures until more accurate forms of self-
identified demographic information are available.
CMS notes its interest in the collection and sharing of a standardized set of social, psychological, and
behavioral data by clinicians, including race and ethnicity, using electronic data definitions which permit
nationwide, interoperable health information exchange to enhance its equity reporting, To improve
AHIP.ORG 11demographic data collection CMS is soliciting comments on current data collection practices to capture demographic data elements (such as race, ethnicity, sex, sexual orientation and gender identity (SOGI), language preference, tribal membership, and disability status). Further, CMS is interested in potential challenges facing clinicians with collecting a minimum set of demographic data elements in alignment with national data collection standards (such as the standards finalized by the Affordable Care Act192) and standards for interoperable exchange (such as the United States Core Data for Interoperability). Medicare Diabetes Prevention Program Expanded Model (MDPP) CMS is proposing several changes to the MDPP that aim to boost supplier enrollment, with a goal of increasing beneficiary participation and access. CMS believes that these proposed changes would make it easier for local suppliers to participate in the model. CMS proposes to shorten the MDPP services period to one year by removing the Ongoing Maintenance sessions phase (months 13-24) of the MDPP set of services for beneficiaries starting MDPP on or after January 1, 2022. This proposal would make the MDPP services timeframe consistent with the Centers for Disease Control and Prevention (CDC) National DPP. The proposal would also redistribute some of the payments for Ongoing Maintenance sessions to Core and Core Maintenance Session performance payments when participants achieve the 5% target weight loss and for continuing attendance. CMS also proposes to waive the provider enrollment Medicare application fee beyond the PHE to increase supplier enrollment. Rural Health Clinics (RHCs) and Federally Qualified Health Centers (FQHCs) CMS proposes several provisions aimed at increasing the abilities of RHCs and FQHCs to furnish care to underserved Medicare beneficiaries. First, CMS proposes to allow Rural Health Clinics (RHCs) and Federally-Qualified Health Centers (FQHCs) to serve as distant site practitioners for mental health services delivered via telehealth and revise the current regulatory language for RHC or FQHC mental health visits to include visits furnished using interactive, real-time telecommunications technology. Under the proposal, these sites can receive payment for mental health telehealth visits in the same way they currently do when visits are in-person, including audio-only services when a patient is not capable of or does not consent to use video services. Next, CMS proposes to implement section 132 of the CAA, which makes FQHCs and RHCs eligible to receive payment for hospice attending physician services when provided by a FQHC/RHC physician, nurse practitioner, or physician assistant who is employed or working under contract for an FQHC or RHC, but is not employed by a hospice program, starting January 1, 2022. Finally, CMS proposes to allow RHCs and FQHCs to bill for Transitional Care Management and other care management services furnished for the same beneficiary during the same service period, provided all requirements for billing each code are met. Indian Health Services (IHS) Clinics CMS has received a request from the American Indian and Alaska Native community to amend its Medicare regulations to make all IHS- and tribally-operated outpatient facilities/clinics eligible for payment at the Medicare outpatient per visit /IHS all-inclusive rate (AIR), regardless of whether they were owned, operated, or leased by IHS. In addition, CMS notes it has been asked to consider certain AHIP.ORG 12
flexibilities regarding the cost reporting requirement for these types of facilities. Therefore, CMS soliciting comment on these topics that could be used to inform future payment policy decisions. Requiring Certain Manufacturers to Report Drug Pricing Information for Part B The CAA added a requirement for manufacturers that do not have a Medicaid Drug Rebate Agreement to report the average sales price (ASP). CMS uses the ASP to determine payment rates for drugs and biologicals that are separately reimbursed under Medicare Part B as Part B covers drugs that are administered in physicians’ offices and hospital outpatient departments. Previously, only drug manufacturers with Medicaid Drug Rebate Agreements were required to submit ASP data for their Part B products in order for their covered outpatient drugs to be payable under Part B. Manufacturers without such agreements had the option to voluntarily submit ASP data; however, after beginning January 1, 2022, the CAA requirements will be in effect and manufacturers of drugs or biologicals payable under Part B without a Medicaid Drug Rebate Agreement will need to report ASP data. CMS proposes to make regulatory changes to implement the new reporting requirements. Determination of ASP for Certain Self-administered Drug Products Section 405 of the CAA requires the Office of Inspector General (OIG) to conduct periodic studies on non-covered, self-administered versions of drugs or biologicals that are included in the calculation of payment under section 1847A of the Social Security Act. This provision permits CMS to apply a payment limit calculation methodology (the “lesser of” methodology) to applicable billing codes, if deemed appropriate. That is, the Medicare payment limit for the drug or biological billing code would be the lesser of: (1) the payment limit determined using the current methodology (where the calculation includes the ASPs of the self-administered versions), or (2) the payment limit calculated after excluding the non-covered, self-administered versions. CMS proposes the “lesser of” methodology for drug and biological products that may be identified by future OIG reports. Section 405 of the CAA also requires that beginning July 1, 2021, the ASP-based payment limit for billing codes representing Cimzia® (certolizumab pegol) and Orencia® (abatacept) as identified in a July 2020 OIG report adhere to the “lesser of” methodology. CMS has applied this methodology for these billing codes in the July 2021 ASP Drug Pricing files. Appropriate Use Criteria (AUC) Program The Protecting Access to Medicare Act (PAMA) of 2014 required CMS to establish a program to increase the rate of appropriate advanced diagnostic imaging services provided to Medicare beneficiaries. Under the AUC program, when a practitioner orders an advanced diagnostic imaging service for a Medicare beneficiary, the practitioner or staff acting under the practitioner’s direction will be required to consult a qualified Clinical Decision Support Mechanism (CDSM). CDSMs are electronic portals through which AUC are accessed. The CDSM provides a determination of whether the order adheres to AUC, or if the AUC consulted was not applicable (e.g., no AUC is available to address the patient’s clinical condition). In this rule, CMS proposes to delay the payment penalty phase of the AUC program from January 1, 2022 to either January 1, 2023, or the January 1 that follows the declared end of the PHE for COVID- AHIP.ORG 13
19. This flexible effective date is intended to consider the impact that the PHE for COVID-19 has had
and may continue to have on practitioners, providers, and beneficiaries.
Medicare Ground Ambulance Data Collection System
CMS proposes a series of changes to the Medicare Ground Ambulance Data Collection System
including:
• Changing the data collection period and data reporting period for selected ground ambulance
organizations in year three.
• Revising the timeline for when the payment reduction for failure to report will begin and when
the data will be publicly available.
• Revising the Medicare Ground Ambulance Data Collection Instrument. Through review of
questions and feedback that we received, we have identified some instances where changes
and clarifications to the instrument could improve clarity and be less burdensome to
respondents.
Clinical Laboratory Fee Schedule: Laboratory Specimen Collection and
Travel Allowance
The CLFS provides for a nominal fee for specimen collection for lab testing and a fee to cover
transportation and personnel expenses (generally referred to as a travel allowance) for trained
personnel to collect specimens from homebound patients and inpatients (not in a hospital). The travel
allowance is paid only when the nominal specimen collection fee is also payable.
During the COVID-19 PHE, CMS changed the Medicare payment rules to provide payment to
independent laboratories for specimen collection from beneficiaries who are homebound or inpatients
not in a hospital for COVID-19 testing under certain circumstances and increased payments from $3-5
to $23-25.
Although CMS expects the increased specimen collection fees will end with the PHE, it is seeking
comments on these policies for the future. Specifically, CMS requests comments regarding:
• the nominal specimen collection fees for trained personnel to collect specimens from
homebound patients and inpatients.
• the calculation of costs for transportation and personnel expenses for trained personnel to
collect specimens from such patients.
Medicare Provider Enrollment
CMS proposes several revisions to the provider enrollment regulations, including: expanding the
agency’s authority to deny or revoke a provider’s or supplier’s Medicare enrollment; establishing certain
rebuttal procedures for providers and suppliers whose Medicare billing privileges have been
deactivated; and exempting certain types of independent diagnostic testing facilities (IDTF) from
several IDTF supplier standards.
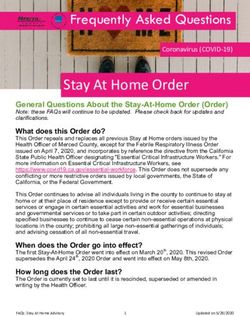
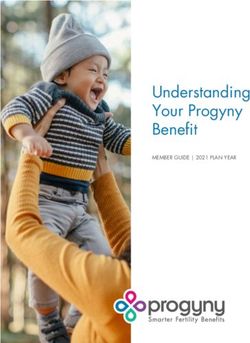
AHIP.ORG 14Rule Impact CMS notes the most widespread specialty impacts of the RVU changes are generally related to the changes to RVUs for specific services resulting from the misvalued code initiative, including RVUs for new and revised codes. Some specialties are anticipated to receive a relative increase in payments relative to other physician specialties, including portable x-ray, family practice, hand surgery, general practice, and endocrinology. These increases are primarily driven by the proposed update to clinical labor pricing, but also to the proposed increases in value for particular services in response to the recommendations from the American Medical Association (AMA)’s Relative Value Scale Update Committee (RUC), and CMS review and increased payments resulting from updates to supply and equipment pricing. Other specialties are anticipated to experience a decrease in payments relative to others, including interventional radiology, vascular surgery, radiation oncology, and oral/maxillofacial surgery. Similarly, these changes are largely a result of the redistributive effects of the proposed clinical labor pricing update, with additional impact based on the revaluation of individual procedures, and the continued phase-in supply and equipment pricing. The estimated impacts also reflect decreases due to continued implementation of previously finalized code-level reductions that are being phased in over several years. Table 123 below shows the payment impact of the policies contained in this proposed rule on PFS services, should CMS finalize this rule as proposed. To the extent that there are year-to-year changes in the volume and mix of services provided by practitioners, the actual impact on total Medicare revenues will be different from those shown in Table 123 (CY 2022 PFS Estimated Impact on Total Allowed Charges by Specialty). AHIP.ORG 15
AHIP.ORG 16
AHIP.ORG 17
You can also read