RO Model - Process and Procedure - Anne Hubbard, ASTRO Director of Health Policy 703-839-7394
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

RO Model – Process and Procedure Anne Hubbard, ASTRO Director of Health Policy Anne.Hubbard@ASTRO.org 703-839-7394
Agenda • RO Model Participation Requirements & Exemptions • Model Episode Construct • Billing & Coding • Reconciliation and True Up • ASTRO Concerns

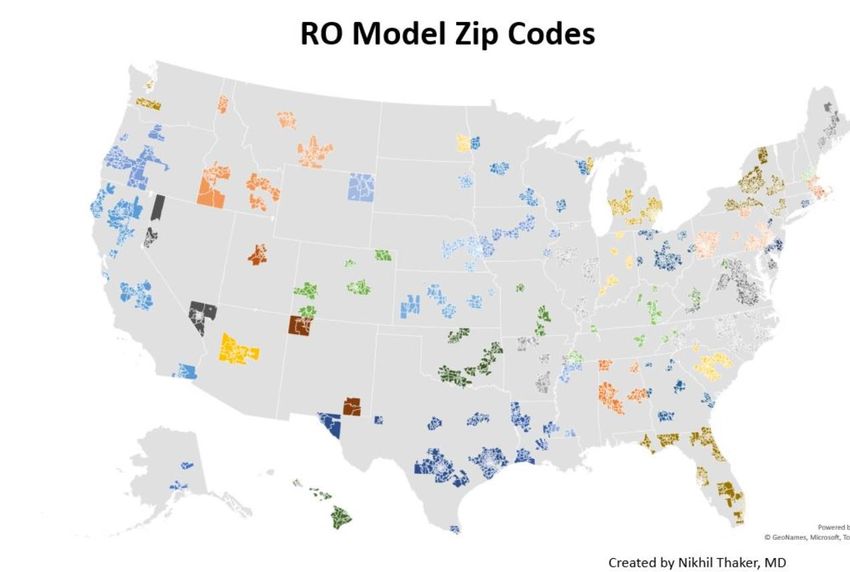
Mandatory participation • 30% of all RO episodes in eligible geographic areas will be included in the model. • $230 million in savings over 5 years (2021-2025) • Exemption for practices with fewer than 20 Medicare FFS episodes in prior year • 500 group practices • 450 hospital outpatient departments • 20% of participants are in rural zip codes

• Check RO Model Zip Code List:
https://innovation.cms.gov/innovation-
models/radiation-oncology-model
• RO Model ID
• CMS Help Desk – 1-844-711-2664, option 5
How do I • Provide your TIN or CCN number and name of
primary contact
know if I’m a • ROAP – Radiation Oncology Administrative
Portal (coming soon)
RO Model • Data including case mix and historical experience
Participant? • Performance reports
• Data Request Forms – claims, episode and
participant
• Attestation of CHERT and PSO
• Radiation Oncology Connect (coming soon)
• Document sharing and other resources.Exemptions
• Low-Volume Opt-Out
• 20 or fewer RT episodes across all CBSAs selected for participation
in the most recent year with available claims data
• CMS will notify practices that qualify for the opt-out 30-days prior
to the beginning of the performance year
• Practices that wish to opt-out must attest to their intention to opt-
out
• Centers in MD, VT, US Territories, ASCs, CAHS, PPS-Exempt Cancer
Hospitals and Penn Rural Health Model Participants are exemptRO Participants
• Professional Participant = PGPs, identified by a single TIN, that
deliver only the professional component of radiation therapy
services at either a freestanding or Hospital Outpatient Department
(HOPD)
• Technical Participant = HOPDs or freestanding center, identified by a
single CCN or TIN, which delivers only the technical component of
radiation therapy services.
• Dual Participant = A RO participant, identified by a single TIN, that
delivers both the professional and technical radiation therapy
services through a freestanding radiation therapy center.• Any Medicare FFS beneficiary receiving
radiation therapy for at least one identified
cancer type.
• Medicare FFS beneficiaries participating in
clinical trials for radiation therapy services,
excluding PBT trials
Medicare FFS • RO Participants must notify Medicare
beneficiaries that they are participating in the
Beneficiaries RO Model by providing a written notice.
• Beneficiaries have the right to refuse
sharing clinical data. In those cases the
participant must notify CMS.
• Medicare FFS beneficiaries are responsible for
20% of the cost of care• Anal Cancer • Lymphoma
• Bladder Cancer • Pancreatic Cancer
• Bone Metastases • Prostate Cancer
• Brain Metastases • Upper GI Cancer
Cancer •
•
Breast Cancer
Cervical Cancer
• Uterine Cancer
Types •
•
CNS Tumors
Colorectal Cancer
• Head and Neck Cancer
• Liver Cancer
• Lung CancerRO Model Services Include Treatment Planning through the Delivery of Treatment
Included Services & Modalities
Services Modalities
• Treatment planning • 3-D Conformal Radiotherapy
• Dose planning • IMRT
• Radiation physics and dosimetry • SRS
• Treatment devices • SBRT
• Special services • PBT
• Treatment delivery • IGRT
• Treatment management • BrachytherapyEpisode Length and Trigger
90-Day Episode of Care
28 Day Clean
Period
Episode begins Payment Trigger Criteria: 1) Initial Treatment Planning
when Treatment Service (77261-263) delivered by a Professional Participant
Planning (77261- or a Dual Participant and 2) at least one radiation
77263) is initiated. treatment delivery service delivered by a Technical
Participant or a Dual Participant within 28 days1. National Base Rates
2. Application of a Trend Factor
3. Geographic Adjustment
4. Case Mix, Historical Experience & Blend
Payment 5. Discount Factor
6. Withholds for Incorrect Payments and
Methodology Quality Measures Performance
7. Co-Insurance
8. Sequestration
How and when will I know
what my PC and TC Rates are?1. National Base Rates
2. Application of a Trend Factor
3. Geographic Adjustment
4. Case Mix, Historical Experience & Blend
Payment 5. Discount Factor
6. Withholds for Incorrect Payments and
Methodology Quality Measures Performance
7. Co-Insurance
8. Sequestration
Dec. 2020 for Case Mix, Historical
Experience Adjustment, and Trend
Factor• RO Model specific Cancer Type HCPCS
Billing Code
• Start of Episode – SOE – V1 modifier
and • End of Episode – EOE – V2 modifier
• Practices must still submit encounter
claims data for all radiation therapy
Coding services included on the RO Model HCPCS
list
• More to come in RO Model Billing GuideClaims Processing – Professional and Dual
Participants
• Start of Episode (SOE)
• Professional participants and Dual participants bill a new RO Model HCPCS
code and a V1 modifier that indicate treatment planning has taken place.
• The first half of the episode payment for the PC services is made through the
PFS.
• End of Episode (EOE)
• Professional participants and Dual participants bill the same RO Model HCPCS
code with a V2 modifier.
• The EOE claim may be submitted as early as day 28 of the 90-day episode.
• Any RT services delivered after the EOE is submitted during the 90-day period
will not be paid.
• Any RT services delivered after the 90-day episode, during the 28-day clean
period will be paid FFS.Claims Processing – Technical and Dual Participants
• Start of Episode (SOE)
• Technical and Dual participants that provide the technical
component of an episode will bill a new RO Model HCPCS code
with a V1 modifier for the first half of the episode payment.
• The Professional participant will provide the Technical participant
with a signed and dated prescription and the final treatment plan,
indicating that the PC component of the episode has been
initiated. The TC of the episode begins on or after the date that
the PC component is initiated.
• The submission and payment of TC claims is not dependent on the
submission of PC claims.
• The first half of the payment will be paid to HOPDs via the OPPS or
Freestanding Centers via the PFSClaims Processing – Technical and Dual Participants
• End of Episode (EOE)
• Technical and Dual participants that provide the technical
component of an episode will bill the same RO Model
HCPCS code with a V2 modifier for the second half of the
episode payment.
• The EOE claim may be submitted by the Technical
participant or Dual participant as early as day 28 of the 90-
day episode.
• Any RT services delivered after the EOE claim is submitted
during the 90-day period will not be paid.
• If the patient requires additional RT services after the 90-
day period, during the 28-day clean period, will be paid FFS.What if the Episode includes a Secondary Diagnosis? • If the episode includes services for multiple cancer types those services and costs are included in the episode payment rate. • If two or more claim lines fall within brain mets or bone mets or secondary malignancies the episode is set to the cancer type with the highest claim count. • If there are fewer than two claim lines for brain mets, bone mets or secondary malignancies, the episode is assigned to the cancer type with the highest claim count among all other cancer types.
How will services provided by multiple
physicians at multiple sites be addressed?
• Duplicate Services
• The PC component of RO Services are provided by more than one
Professional participant or Dual participant
• TC component of RO Services is provided by more than one Technical or
Dual Participant.
• Examples:
• EBRT and Brachytherapy
• Cervical cancer episode initiated by Dual Participant in community
clinic referred to physician at hospital for brachytherapy
• Prostate cancer episode initiated by Professional Participant for brachy
in hospital, referred to community clinic for EBRTCervical Episode
Cervical cancer episode initiated by Dual Participant in community clinic
referred to physician at hospital for brachytherapy
• Dual participant initiates the episode at the community clinic with
the combination treatment planning and EBRT delivery codes.
• The referral to the physician at the hospital for brachytherapy. The
hospital services will bill a modifier or condition code to indicate
that those services should be paid FFS.
• During the Incorrect Payment reconciliation period the FFS amounts
paid for the hospital-based brachytherapy services (both the PC and
the TC portion) will be taken from the 1% Incorrect Withhold
amount. CMS will not deduct more than the value of the episode.Prostate Episode
• Prostate cancer episode initiated by Professional participant for brachy in hospital,
referred to community clinic for EBRT
• The Professional participant and Technical participant trigger the episode with the
combination planning and treatment delivery codes associated with the delivery
of brachy therapy with the issuance of a SOE claim. They also submit an EOE
claim.
• The community-based clinic provides the EBRT uses a designated modifier or
condition code that indicated they should be paid FFS.
• During the Incorrect Payment reconciliation period the FFS amounts paid for the
EBRT services delivered by the community-based clinic will be taken from the 1%
incorrect withhold for the Professional participant and Technical participant. CMS
will not deduct more than the value of the episode.What about referrals to PPS Exempt facilities?
• PPS Exempt Cancer Hospitals are exempt from participating in the RO
Model.
• Services referred to a PPS Exempt facility will be paid FFS
• FFS payments made to PPS Exempt facilities will not be deducted
from RO Model participants during the Incorrect Payment
reconciliation period.Reconciliation and True Up Process
PY 2021
Quality
Reconciliation True-Up
Measures
Begins
Reported August 2023
8/1/2022
3/31/2022Stop Loss Policy RO participants with fewer than 60 episodes in the baseline period (2016-2018) do not have sufficient historical volume to calculate a reliable adjustment to their payment rates. - CMS applies a stop loss policy to prevent these practice from significant payment shifts. - CMS will use no-pay claims data to determine what these RO Participants would have been paid under FFS as compared to payments under the RO Model. - CMS will pay these participants retrospectively for losses in excess of 20% of what they would have been paid under FFS. These payments are determined during reconciliation.
Timely Error Notice and Reconsideration
• Limited to reconciliation process not the RO Model payment
methodology or AQS methodology
• Timely error notice must be submitted 45 days from
reconciliation report
• CMS has 30 days to respond
• Reconsideration Review must be submitted 10 days of Timely
Error response
• Official response issued 60 days post Reconsideration
Review submission• CMS is designated the RO Model as an Advanced
Advanced APM and MIPS APM
• The Agency limits the 5% bonus to the PC
APM and component only.
• Practices must meet Qualified Advanced APM
Thresholds to achieve Advanced APM QP status
MIPS • 50% of Medicare Part B payments
generated through participation in an
Advanced APM, OR
APM • 35% of Medicare patients received care
through an Advanced APM• Implementation Date Set for
January 1, 2021
• Mandatory for 30% of
Episodes (950 practices)
• Discount Factors set at
3.75% for PC and 4.75% for
TC
• Medicare FFS payment cuts
• 6% for PGPS
• 4.7% for HOPDsOur volume is still down from COVID, The combination of dramatic cuts in
both for the current time as well as for payments and the increased
the entire year. Revenues are way off… requirements of documentation and
Our centers were already talking about data entry for this mandatory
laying off or reducing staff. Jan 1 start program will break us. My staff and I
date is awfully ambitious considering are stretched to the limit. This has
the amount of training and been the worst year of my
documentation that we need to professional life. That the agency
implement to meet the programs would spring this on frontline
requirements. providers during a pandemic is just
Stories from --Massachusetts Radiation Oncologist
The proposed model is extremely
cruel. Practices will close. Patients
will be harmed.
--Virginia Radiation Oncologist
the front line complex and confusing. The amount of
time and training to ensure that we
have revenue personnel who are Our volume is down 35% year over
last and our supply expenses are up
trained to accurately comply with all of
these proposed changes will be 14% thanks to COVID-19.
extraordinary. The very burdensome Consequently, this seems like the
requirements of the APM, coupled with worst possible time to implement
the likelihood of having to operate a such a radical change. With the
simultaneous and parallel FFS challenges private practice’s are
operation with private payors, means already facing this could be disastrous
that we will likely need to hire a for the foreseeable future, and one
dedicated FTE to coordinate this that we may or may not be able to
transition. survive due to the inequity imposed.
--New Jersey Radiation Oncologist --Florida radonc practice
administratorCongress Must Act to Protect Patient Access to
Radiation Oncology and Drive Value-Based Care
1 2
Provide mandated participants Reduce the discount factor cuts to
more time to cope with the a level consistent with MACRA’s
pandemic and adopt the model. intent and other payment models.
• Delay implementation until July 1, 2021 • Decrease the professional and technical
and after the expiration of the PHE. discount factor payment cuts to 3%.Questions? Anne Hubbard, ASTRO Director of Health Policy Anne.Hubbard@ASTRO.org 703-839-7394
You can also read