Rice bodies in the wrist - Oxford Academic Journals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Modern Rheumatology Case Reports, 00, 2021, 1–5
DOI: https://doi.org/10.1093/mrcr/rxab040
Advance access publication date: 7 October 2021
Case Report
Rice bodies in the wrist
Maurice Gillijns* and Wim Vandesande
Department of Orthopaedic Surgery, AZ St-Dimpna Geel, Geel, Belgium
Downloaded from https://academic.oup.com/mrcr/advance-article/doi/10.1093/mrcr/rxab040/6382445 by guest on 21 December 2021
*Correspondence: Maurice Gillijns; Maurice.gillijns@student.kuleuven.be; Department of Orthopaedic Surgery, AZ St-Dimpna Geel, Jokerstraat 12, Turnhout
2300, Belgium.
ABSTRACT
Rice bodies are a rare finding in medicine and offer a therapeutic challenge. As their occurrence varies over multiple rheumatic as well as
infectious diseases, multiple hypotheses have been made about their origin. While rice bodies are most frequently reported in the shoulder and
knee joints, flexor tendon synovitis with accompanying rice bodies is rarer. We report a case of extensive flexor tenosynovitis with rice bodies
in the wrist in a 90-year-old patient with seronegative rheumatoid arthritis. The patient reported a 5-month history of painful swelling of the right
wrist. Ultrasound showed pronounced swelling of the synovial tissue of the flexor tendons. Laboratory test were negative for rheumatology
tests with normal C-reactive protein and sedimentation rates. T2-weighted magnetic resonance imaging demonstrated an extensive synovitis
reaching from the distal forearm into the hand with inclusions, better known as rice bodies. Synovectomy including carpal tunnel release was
performed with dissection of the mass revealing an extensive synovitis with a multitude of rice bodies. Histopathology showed lymphohistiocytic
infiltrates consistent with rheumatoid nodules. After surgery, the patient regained full function of the wrist within 2 weeks without any pain or
remaining mass in the affected limb.
KEYWORDS: Rice bodies; MRI; flexor tenosynovitis; synovectomy; wrist
Introduction Initial differential diagnoses included ganglion, synovial
Rice bodies are a rare finding in medicine and remain to be a cyst, synovitis, and giant cell tumour. Other causes of wrist
challenge to provide adequate treatment. As their occurrence swelling like gout and abscess were possible, although less
probable due to the chronic nature of the swelling.
varies over multiple rheumatic as well as infectious diseases,
Laboratory tests including rheumatoid factors were per-
multiple hypotheses have been made about their origin [1–3].
formed. Results were normal except low haemoglobin
While rice bodies were at first most frequently reported in
correlating with underlying chronic renal insufficiency.
the shoulder and knee joints, flexor tendon synovitis with Rheumatoid factor as well as anti-citrullinated protein anti-
accompanying rice bodies is rarer [4–8]. We report a case body were negative. Uric acid was elevated, which could also
of extensive flexor tenosynovitis with rice bodies in the wrist be correlated with a history of chronic renal insufficiency
in a 90-year-old patient with seronegative rheumatoid arthri- (Table 1).
tis. We report clinical, radiological, and histopathological A magnetic resonance imaging (MRI) scan was performed
features as well as discuss current knowledge in literature. for further investigation. This showed a sharply defined fluid
collection surrounding the flexor tendons from the distal
diaphysis of the radius up to the distal diaphysis of the
Presentation of case metacarpals. This extensive synovitis measured almost 10 cm
A 90-year-old woman presented to the orthopaedic surgery in length and 5 cm in width (Figures 1–3). The fluid col-
department with a 5-month history of a painful right wrist lection was inhomogeneous with multiple sharply defined
with accompanying swelling. The patient reported no previ- hypointense noduli on T2-weighted images. These noduli are
ous injury to the right wrist; no swelling or pain was present in described in literature as rice bodies. Older erosive lesions in
the past. No signs of median nerve compression were withheld the carpal bones as well as the styloid process of the ulna cor-
at presentation. Physical examination of the right wrist and related with the age of the patient and not with the current
forearm revealed an extensive volar wrist swelling, extending pathology. The median nerve could not be distinguished. The
from the distal forearm up to the wrist. Tinel and Phalen tests overall conclusion of MRI scan was correlation with chronic
for median nerve compression were negative. arthritis of synovitis.
Doppler ultrasound was performed, which showed pro- The patient was referred to a rheumatology expert for
nounced swelling of the synovial tissue of the flexor digitorum further rheumatologic evaluation 7 months later. At this
tendons as well as the flexor pollicis longus tendon, but no time, the swelling was still present with lack of pain. The
conclusive diagnosis could be made. As a consequence of patient suffered nocturnal tingling sensations in the right
the volar swelling, possible median nerve compression was hand, correlating with median nerve compression due to the
withheld. mass in the volar wrist region. Diagnosis of seronegative
Received 21 May 2021; Accepted 4 October 2021
© Japan College of Rheumatology 2021. Published by Oxford University Press. All rights reserved.
For permissions, please e-mail: journals.permissions@oup.com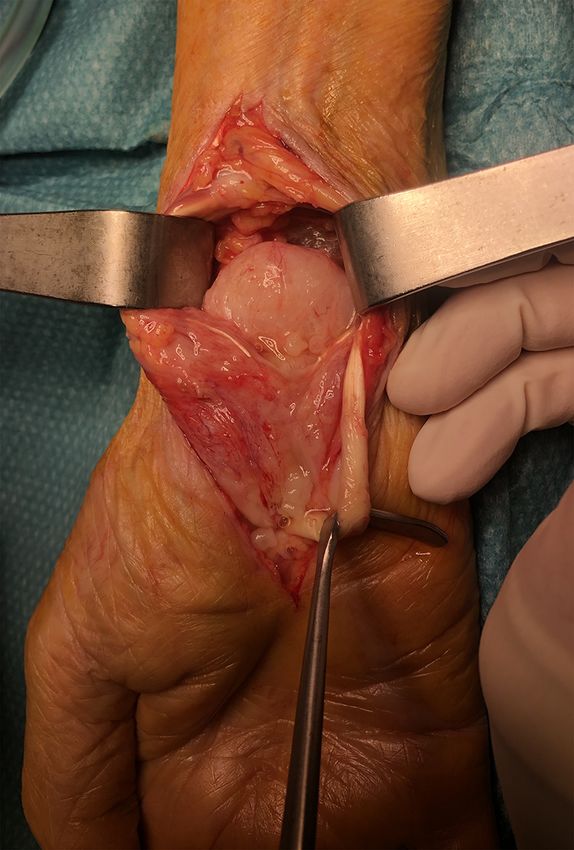
2 Gillijns and Vandesande Table 1. Laboratory results. Biomarker Value Reference value RF
Rice bodies in the wrist 3
Downloaded from https://academic.oup.com/mrcr/advance-article/doi/10.1093/mrcr/rxab040/6382445 by guest on 21 December 2021
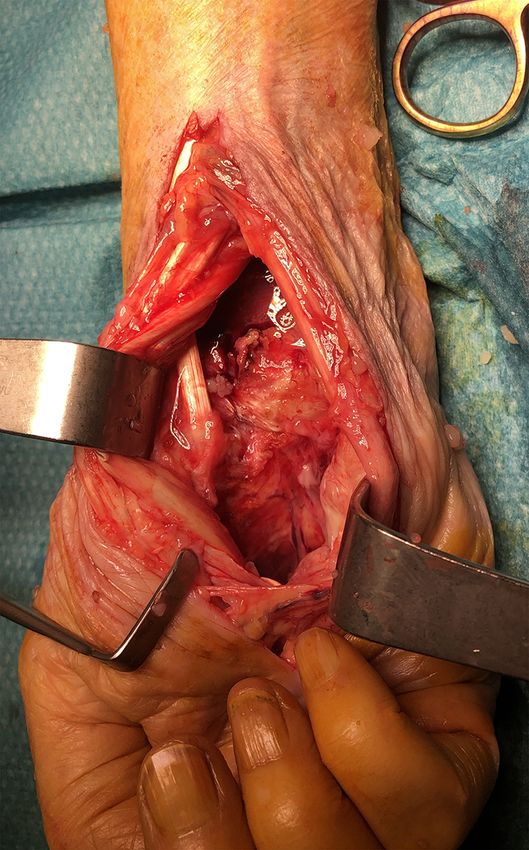
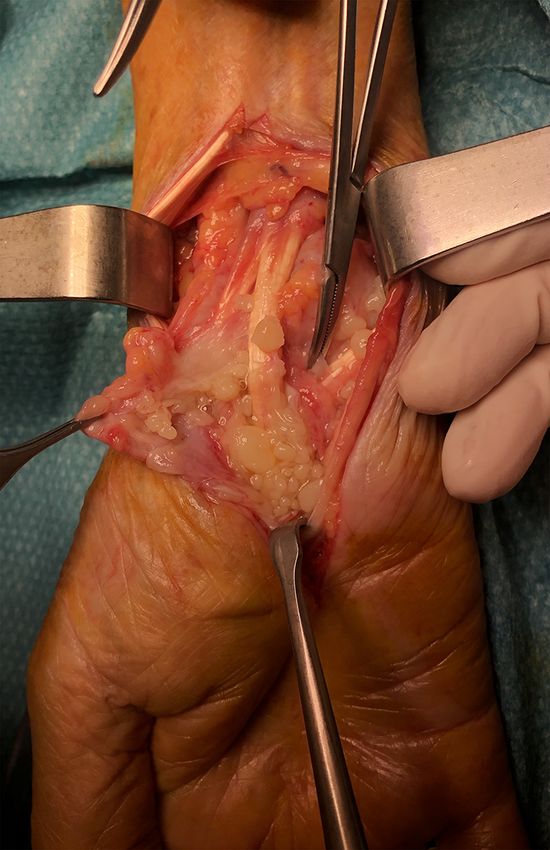
Figure 4. Dissection of the synovial mass from the flexor tendons Figure 5. Rice bodies escaping from the synovitis. Remark differences in
revealing extensive synovitis in the distal forearm. Rice bodies can be shape and volume of the nodules.
seen escaping from the synovitis.
giant cells were also found. No atypical cells were discovered while rice body synovitis of the wrist flexor tendons is
(Figures 7 and 8). uncommon [4–8].
Post-operative recovery was uneventful with limited The origin of rice bodies has been vastly discussed in
drainage fluid on Day 2 and normal primary healing of the the past. They are histologically defined as amorphous
wound with clinical evaluation on Day 2 after synovectomy. eosinophilic material, consisting mostly of fibrin, fibronectin,
Activation of wrist mobility was stimulated starting immedi- and collagen with accompanying mononuclear cells [1, 3].
ately post-operation; no immobilisation was advised. Nor- Multiple hypotheses have been formed in the past about the
mal painless range of motion was regained within 2 weeks cause of rice body formation. Some suggest degenerating
after surgery. One month after surgery, the patient was synovial villi, microinfarction of synovial tissue, subsequent
pain free with normal mobility of the wrist. Further follow- inflammation, proliferation, and secondary degeneration of
up was advised in case of recurrence of complaints or the synovium [2, 3].
swelling. The histological finding of a central area of fibrinoid
Diagnosis of seronegative synovitis with rice bodies was necrosis surrounded by a palisade layer of histiocytes and
maintained, correlating clinical symptoms, laboratory results, peripherally by a zone of loose connective tissue is called a
imaging, and histological tissue evaluation. ‘rheumatoid nodule’ and is almost specific for RA. These find-
ings of ‘rheumatoid nodules’ are similar to those described by
Iyenkar et al. [5], while in most cases a non-specific chronic
Discussion inflammation is reported [4, 7, 8].
Rice bodies have been first described in patients with tuber- While the patient reported with long-standing painful wrist
culous arthritis in 1895. Since then, rice bodies have swelling, our initial differential diagnosis included rheuma-
been correlated with a multitude of rheumatic and inflam- toid diseases like rheumatoid arthritis and gout, as well
matory diseases. Among these are rheumatoid arthritis, as a tumoural process. An important tumour to withhold
juvenile idiopathic arthritis, and systemic lupus erythe- in orthopaedic care is a giant cell tumour [9]. An MRI
matosus. Most common locations for rice bodies include and standard rheumatoid testing was performed for further
the subacromial bursa of the shoulder and the knee, evaluation.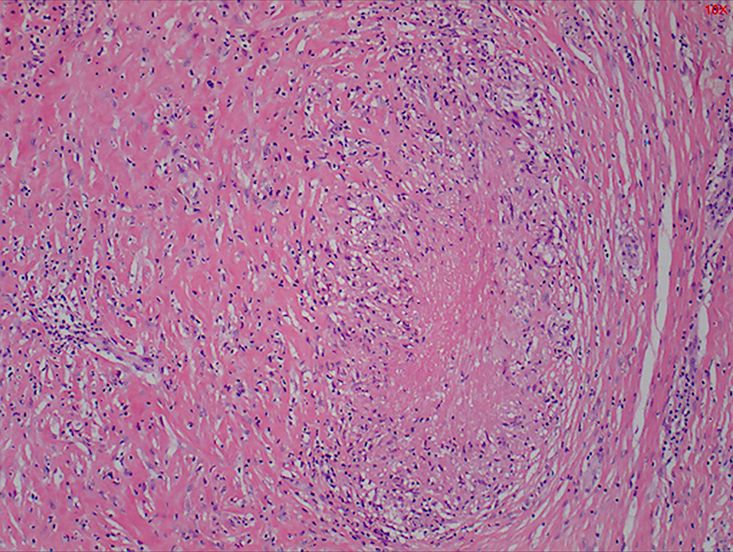
4 Gillijns and Vandesande
Downloaded from https://academic.oup.com/mrcr/advance-article/doi/10.1093/mrcr/rxab040/6382445 by guest on 21 December 2021
Figure 7. Rheumatoid nodule found in the peri-articular soft tissue,
consisting of a necrobiotic centre, surrounded by palisading histiocytes.
The adjacent tissue is fibrotic and contains a mild infiltrate of mainly
lymphocytes and few plasma cells.
Figure 6. Status after synovectomy and carpal tunnel release.
Biologic markers form an important factor in diagnosis Figure 8. Fibrinous deposits and formation of rice bodies on the synovial
of rheumatoid arthritis (RA). Rheumatic factor (RF) is an surface.
autoantibody found in 75% of RA patients, but is not specific
for RA. Anti-citrullinated peptide antibodies (ACPAs) can also
be found in 60–70% of RA patients but is highly specific for report a satisfactory aspirate in 86.6% of lesions of the hand
RA [10]. In this case no biologic marker for RA was found to and wrist, where FNAC is used in the initial diagnosis. The
be positive. This type of RA is known as seronegative RA. advantages of FNAC include the accessibility in primary diag-
While rice bodies have been seen in patients with RA, nostics as well as being a simple tool to provide adequate
occurring in multiple locations throughout the body, existence planning of treatment. In this case, FNAC could have pro-
of rice bodies in the wrist of seronegative patients is rare and vided an adequate option for diagnosis being less invasive and
only few reports exist to our knowledge [4–6, 8, 11]. easy to perform [15].
Superficial soft-tissue masses are ideal for initial ultrasound Popert et al. [3] suggest in their work that effective removal
evaluation [12]. The flexor muscles of the wrist form ideal by lavage and aspiration in itself proves to be an effective
landmarks for evaluating abnormalities in the wrist. Certain treatment and results in clinical improvement of the joint
features like dimension, vascularisation, internal abnormali- affected by rice body formation. Other treatment options
ties, and malignancy features can be assessed using ultrasound include urokinase and other fibrinolysis-promoting agents.
evaluation [12]. Although good superficial resolution can be While this approach can be easily performed in larger joints
obtained, difficulties in differentiating the nature of the mass like the knee and the shoulder, this can be difficult to per-
are likely to occur. Secondary MRI scanning is mandatory in form in the wrist. Albrecht et al. [2] proposed synovectomy
these circumstances because of high-contrast resolution and as an adequate treatment to prevent recurrence of rice body
higher specificity [13, 14]. formation. The risk of tendon rupture in flexor tenosynovitis
Further primary evaluation of wrist swelling is possible in the wrist makes surgery with synovectomy an appropriate
by fine needle aspiration cytology (FNAC). Goyal et al. [15] treatment option to provide the best outcome possible [16].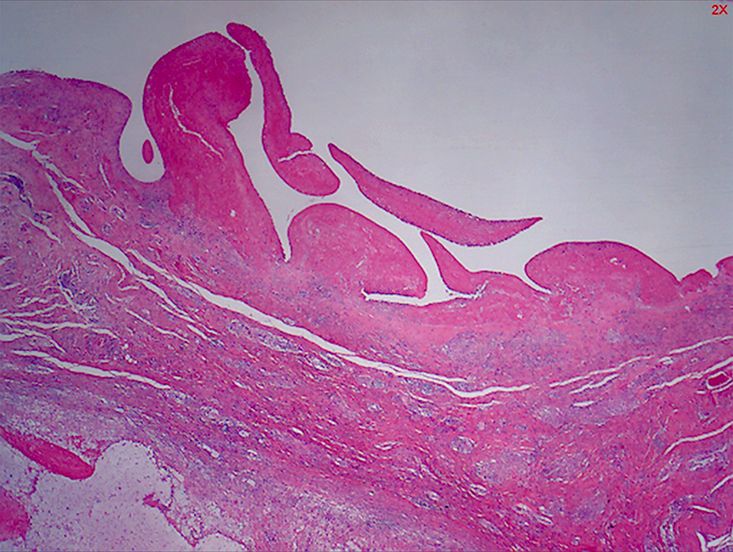
Rice bodies in the wrist 5
Surgery in the volar wrist should include dissection of wrist [4] Tyllianakis M, Kasimatis G, Athanaselis S et al. Rice-body forma-
swelling with synovectomy as well as release of the carpal tion and tenosynovitis of the wrist: a case report. J Orthop Surg
tunnel by an extended approach into the carpal tunnel. (Hong Kong) 2006;14:208–11.
Recurrence of rice body synovitis is assumed to be rare and [5] Iyengar K, Manickavasagar T, Nadkarni J et al. Bilateral recur-
rent wrist flexor tenosynovitis and rice body formation in a patient
has only been reported once in literature in a case of bilat-
with sero-negative rheumatoid arthritis: a case report and review
eral wrist flexor synovitis [5]. As no recurrence after 6 months
of literature. Int J Surg Case Rep 2011;2:208–11.
has been described, no further follow-up was indicated in this [6] Ergun T, Lakadamyali H, Aydin O. Multiple rice body forma-
case. tion accompanying the chronic nonspecific tenosynovitis of flexor
tendons of the wrist. Radiat Med 2008;26:545–8.
[7] Guo JJ, Wu K, Xu Y et al. Hundreds of rice bodies in the
Downloaded from https://academic.oup.com/mrcr/advance-article/doi/10.1093/mrcr/rxab040/6382445 by guest on 21 December 2021
Conflict of interest subacromial-subdeltoid bursa: report of two cases and literature
None declared. review. BMC Musculoskelet Disord 2020;21:539.
[8] Sugano I, Nagao T, Tajima Y et al. Variation among giant rice
bodies: report of four cases and their clinicopathological features.
Funding Skeletal Radiol 2000;29:525–9.
[9] Nahra ME, Bucchieri JS. Ganglion cysts and other tumor related
Nothing to disclose. conditions of the hand and wrist. Hand Clin 2004;20:249–60.
[10] Taylor P, Deleuran B. Biologic markers in the diagnosis and
assessment of rheumatoid arthritis. In: O’Dell J (ed.), UpToDate.
Patient consent Waltham, MA: UpToDate Inc., 2020. www.uptodate.com (21
February 2021, date last accessed).
Written informed consent and consent for publication were
[11] Nagasawa H, Okada K, Senma S et al. Tenosynovitis with rice
obtained from the patient. body formation in a non-tuberculosis patient: a case report. Ups J
Med Sci 2009;114:184–8.
[12] Catalano O, Varelli C, Sbordone C et al. A bump: what to do next?
References Ultrasound imaging of superficial soft-tissue palpable lesions. J
[1] Berg E, Wainwright R, Barton B et al. On the nature Ultrasound 2020;23:287–300.
of rheumatoid rice bodies: an immunologic, histochemical, [13] Narváez JA, Narváez J, Roca Y et al. MR imaging assess-
and electron microscope study. Arthritis Rheum 1977;20: ment of clinical problems in rheumatoid arthritis. Eur Radiol
1343–9. 2002;12:1819–28.
[2] Albrecht M, Marinetti GV, Jacox RF et al. A biochemical and elec- [14] Plotkin B, Sampath SC, Sampath SC et al. MR imaging and US of
tron microscopy study of rice bodies from rheumatoid patients. the wrist tendons. Radiographics 2016;36:1688–700.
Arthritis Rheum 1965;8:1053–63. [15] Goyal A, Pathak P, Sharma P et al. Role of FNAC in diagnosing
[3] Popert AJ, Scott DL, Wainwright AC et al. Frequency of occur- lesions of hand and wrist. Diagn Cytopathol 2018;46:853–8.
rence, mode of development, and significance of rice bodies in [16] Rizzo M, Cooney WP. Current concepts and treatment for the
rheumatoid joints. Ann Rheum Dis 1982;41:109–17. rheumatoid wrist. Hand Clin 2011;27:57–72.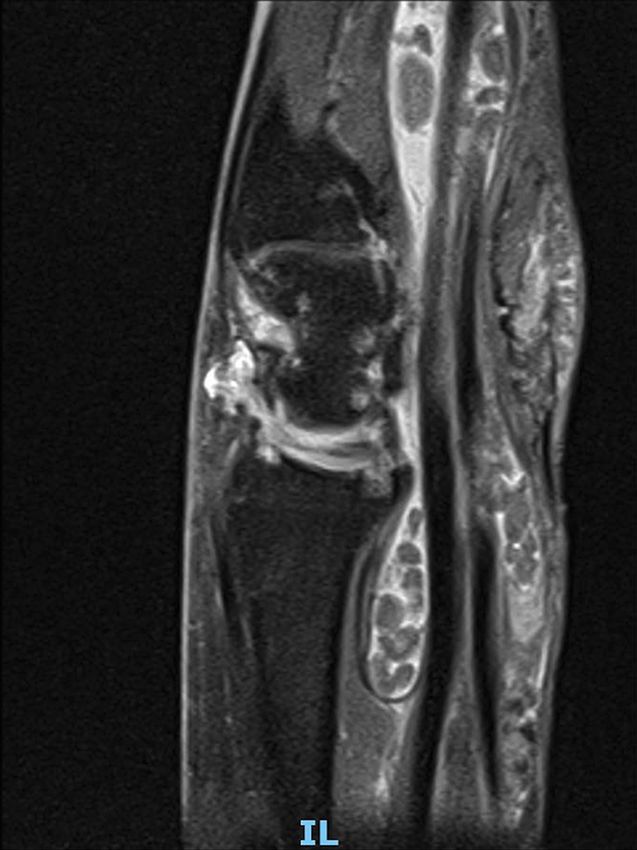

You can also read

















































