Diagnosing Pancreatic Cancer - Challenges and Developments - PCUK 15TH October 2018
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Diagnosing Pancreatic
Cancer – Challenges
and Developments
PCUK 15TH October 2018
Dr Andrew Millar
MDC Clinical Lead UCLH Cancer Alliance
Gastroenterologist and Hepatologist
North Middlesex University Hospital
Royal Free Hospital
The Problem of Cancer Diagnosis and
Survival in the UK
2
BENCHMARKING DATA HIGHLIGHTS A SURVIVAL GAP
Although an improving picture, cancer survival in the UK trails behind comparable countries
Source: International Cancer
Benchmarking Partnership M1 - 5
year survival, 1995-2007.
Published 2011
Providing increased impetus amongst professionals in the UK to improve early diagnosis
Slide courtesy of Sara Hiom – CRUK
UK HEALTH SYSTEM IS NOT SET UP FOR EARLY DIAGNOSIS
The UK, versus other comparable countries, has:
• Focus on Alarm Symptoms
• Less investigation of low risk symptoms
• Less access to diagnostics and specialists
Source: International Cancer Benchmarking
Partnership M3 - Survey 2012-2013. Published 2015
Amended slide courtesy of Sara Hiom – CRUK
Background
Current cancer pathways are unsustainable and not fit for purpose
Key findings of 2ww
referrals
NICE guidance (NG12)
2ww pathways - 3% cancer
conversion
Most cancers (>50%) are
not diagnosed on 2ww
pathway
A quarter (25%) diagnosed
on routine pathways
In the last 3 years 2ww referrals
have risen by 17% A fifth (21%) are diagnosed
via A&E
Source: Collated by Centre for Cancer Outcomes. In strictest confidence for NHS internal use only. CRUK website: 5
http://www.cancerresearchuk.org/health-professional/cancer-statistics/diagnosis-and-treatment#heading-Zero
Early Diagnosis of Pancreatic Cancer
The problem (opportunity) of symptoms
6
Hard for Patients Symptom appreciation - Hard to be ‘Clear on Cancer’ when the symptoms are so common (and GP access?) “Greater public and healthcare professional awareness of the combinations of subtle and intermittent symptoms, and their evolving nature, is needed to prompt timelier help-seeking and investigation among people with symptoms of pancreatic cancer” Mills K et al. BMJ Open 2017;7 7
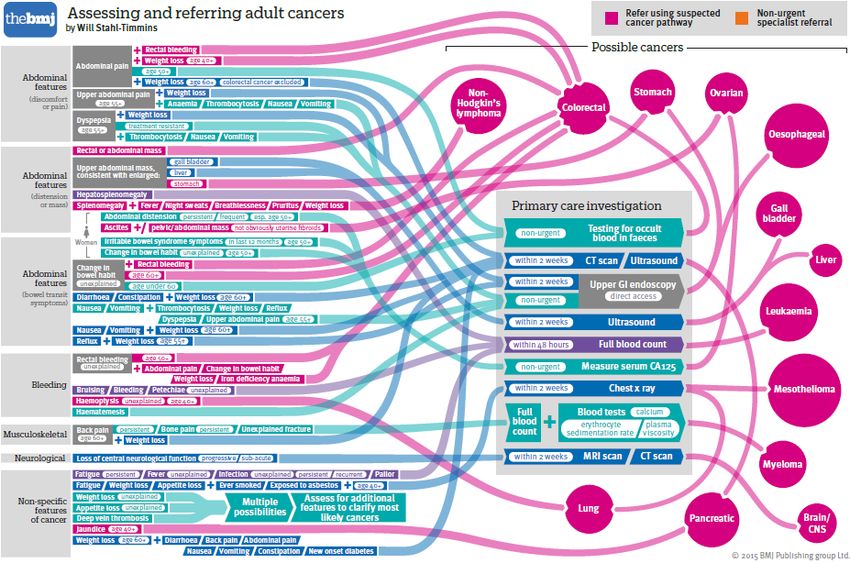
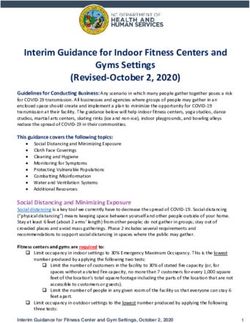
Hard for Doctors
The NG12 Symptom Based Infogram1
Assessing and referring adult cancers. Image from Suspect cancer (part 2- adults) BMJ 2015;350:h3044
Why is PDAC so difficult to diagnose in primary care? • >30,000,000 consultations for abdominal symptoms per year in the UK • Early symptoms non-specific • 0.02% are pancreatic cancer • GP access to CT scanning • No adequate diagnostic biomarkers • NG12 / 2WW guidance is better for specific symptoms

The Problem of Symptoms in Pancreatic Cancer • Non-specific symptoms – abdominal pain, weight loss, backache, fatigue, (NSCS) & new NIDDM • Symptom Study – 93% of patients had relevant symptoms up to 2 years before diagnosis1 • Delay is similar to other cancers with non-specific symptoms also diagnosed late2 • Patients often seen multiple times by GP – Av 3.23 • Consequence - Symptomatic PDAC usually stage 3-4 • How can we improve this? 1Keane MG, et al. BMJ Open 2014 2Dengsø KE et al J Neoplasm. 2017; 5: 2 3Lacey K et al Med J Aust 2016; 205 (2): 66-71 10
Diagnosis of Pancreatic Cancer
• Symptomatic – 95%
– Symptom Appraisal – patient understanding
– Help-seeking – patient attitude, accessibility
– Diagnostic – HCW attitude, availability of
tests, referral pathways, waiting times
• Asymptomatic – 5%
– Screening – identification of high risk people
– Surveillance – of identified lesions e.g. IPMN
11Symptomatic Cancer
Anderson Model of Patient Delay
Walter et al J Health Serv Res Policy Vol 17 No 2 April 2012
12Benefits of Early Diagnosis
• Increase survival by increasing resection rates
– currently 20% operable, 5% 5-year survival
• If we could detect earlier survival would improve
– ~30mm - survival 10-20%
–Key Points on Diagnosis
• CT scan before ERCP – latter with brushings
• If no diagnosis FDG-PET / EUS – latter with cytology
• CT or MRI for cysts - refer if jaundice/solid/dilated PD
• EUS for cysts with aspiration for Cytology and CEA
14Key points on Surveillance
• Surveillance for pancreatic cancer to people with:
– Hereditary pancreatitis and a PRSS1 mutation
– BRCA1, BRCA2, PALB2 or CDKN2A (p16) mutations and one or
more first-degree relatives with pancreatic cancer
– Peutz–Jeghers syndrome
– 2 or more first-degree relatives, across 2 or more generations
– Lynch syndrome (mismatch repair gene [MLH1, MSH2, MSH6 or
PMS2] mutations) and any first-degree relatives
• Surveillance by MRI / EUS / CT
15Current imaging diagnostic tests
• CT scan – misses 23% of small cancers1
• MRI – identifies 80% those not seen at CT2
• FDG-PET – best sensitivity (89%)
• EUS sensitive and allows needle aspiration but
limited availability
• None of these yet widely available in primary
care – increasing however
1Wong J.C et al Clin. Gastroenterol. Hepatol. 2008;6:1301–1308
2Kim J.H et al Radiology. 2010;257:87–96
16Biomarkers – active research area
17
Reproduced from Zhang X et al Am J Cancer Res 2018;8(3):332-353Multi-Disciplinary Diagnostic Centres
18Symptomatic Cancer
Anderson Model of Patient Delay
Walter et al J Health Serv Res Policy Vol 17 No 2 April 2012
19What are MDCs?
MDC pathway: avoiding the hospital pinball machine
2021
What are MDCs?
MDC pathway
1. Fast track diagnostic centre/clinic for suspected cancer
What is an
where existing 2WW pathway is unclear or not suitable
MDC?
2. MDC runs within a hospital and uses current hospital infrastructure
1. CT
2. Bloods
Main 3. Endoscopy
Diagnostic 4. Colonoscopy
tests 5. MRI
6. PET CT
7. ERCP
1. Named CNS contact from time referral is received
Benefits
2. Fast access to diagnostics
1. If shown to be beneficial will be rolled out nationally
Future
2. Opportunity to support more DIRECT and STRAIGHT TO TEST
22MDCs align with national and local strategy
Danish Model – more GP access to tests
Aligns with Aligns
Potential Area of benefit Rationale national with NCL
strategy? strategy?
benefits of MDCs
Diagnosis within •Rapid access to diagnostics
28 days •Improves patient experience
Improve
quality and
Aid treatment
within 62 days
•Earlier diagnosis in pathway Will
improve survival rates
outcomes
•Cancer diagnosis following ED poorer
Reduction in
A&E cancer
outcome, even when controlling for
other factors1
diagnosis
•Better use of hospital resources
Improve
patient
experience
Diagnosis
through
•Patients benefit from CNS support
appropriate •Better access to diagnostic tests and
setting specialist cancer and holistic support
Reduction in Reduction in •Reduce number of GP visits
cost number of
wasted •Reduce incorrect referrals Meets
needs of primary care
consultations
23
1 - Plaser TR et al 2013; Schneider C et al. 2013THERE ARE 10 MDCS ACROSS ENGLAND • A common dataset
agreed across the
projects
Airedale, Wharfdale & Leeds
Craven MDC site: St James • Comparator data for
MDC site: Airedale University Hospital
General Hospital (Specialist Cancer Centre) each project area; only
partial data and largely
retrospective audits
Greater Manchester
MDC sites: Manchester
University NHS
• National Cancer
Foundation Trust Diagnosis Audit used to
(Wythenshawe
Hospital) and The create a ‘proxy
Northern Care Alliance
(Royal Oldham
London comparator pathway’ for
MDC sites: North
Hospital) Middlesex University NSCS patient cohort
Hospital, University
College London Hospital • Collection of MDC data is
(Specialist Cancer
Centre), Southend ongoing (expect final
Oxford
MDC site: Oxford
University Hospital, cut-off for evaluation to
Queens (BHRUT) and the
University Hospital
Trust (Specialist Cancer
Royal Free Hospital be end July 2018)
Centre)
A national approach allows different NHS settings to be explored and creates a larger MDC
referral data set for analysisProject overview
North London MDC referral criteria and MDC sites
Who to refer
Current main indications
1. New unexplained
abdominal pain
North Middlesex
2. Unexplained weight loss
Royal Free
3. Painless jaundice Barts Health BHRUT
4. New and persistent
unexplained nausea / loss
of appetite
UCLH
5. GP has concern /gut feeling
of an underlying
gastrointestinal (GI) cancer
25Project overview
Case study
Patient referred in June 2017
1 Referral received
Day 0-1
2 Referral triaged by CNS
3 Patient seen in MDC Day 3
CT
Diagnostics
4 ERCP / bile duct brushing
Day 3-5
Upper GI MDT
4 Patient informed of diagnosis Day 9
Diagnosed
within 28 days:
5 Imaging sent to RLH for discussion
treated in 41
days
6 Patient seen by surgeon and informed of Day 9-41
care plan
7 Surgery
26MDC Performance Data
27NATIONAL FIGURES - CANCER DIAGNOSES BY MDC UNTIL END FEB
2018
MDC Number of Number of Conversion
cases cancers rate
Airedale 187 18 10
Greater Royal Oldham 119 17 14
Manchester
Wythenshawe 187 13 7
Leeds 326 27 8
London Queen (BHRUT) 119 8 7
North 103 6 6
Middlesex
Royal Free 8 - -
UCLH 281 10 4
Oxford 293 43 15
Total 1,623 142 9MDC outcomes
National figures - Diagnosis of MDC patients
Cancer Diagnosis Non-cancer Diagnosis
30 Broad Description N %
Diseases of the digestive system 166 39
Symptoms, signs and abnormal clinical and laboratory findings,
25 44 10
not elsewhere classified
Diseases of the respiratory system 42 10
Diseases of the genitourinary system 31 7
Percentage
20
Neoplasms (benign) 28 7
Diseases of the musculoskeletal system and connective tissue 20 5
15 Diseases of the circulatory system 19 5
Certain infectious and parasitic diseases 14 3
Endocrine, nutritional and metabolic diseases 14 3
10
Mental, Behavioural and Neurodevelopmental disorders 14 3
Diseases of the blood and blood-forming organs and certain
13 3
disorders involving the immune mechanism
5
Congenital malformations, deformations and chromosomal
6 1
abnormalities
0
Diseases of the nervous system 4 1
Diseases of the skin and subcutaneous tissue 2 0
Injury, poisoning and certain other consequences of external
2 0
causes
Factors influencing health status and contact with health services 2 0
Grand Total 421 100
29North London MDCs April 18- Oct 18
Referral numbers and reason
Number of patients referred between April 17 – Sept 18 Referral reason
400
350
60
300
50
250
40
200
30
150
No of patients
20
100
10
50
0
0
Dec-17
Apr-17
May-17
Mar-18
Apr-18
May-18
Jun-17
Jul-17
Oct-17
Aug-17
Jun-18
Nov-17
Jan-18
Aug-18
Sep-17
Feb-18
Jul-18
Sep-18
Ma Ma Ma
Apr Jun Jul- Aug Sep Oct Nov Dec Jan- Feb Apr Jun Jul- Aug Sep
y- r- y-
-17 -17 17 -17 -17 -17 -17 -17 18 -18 -18 -18 18 -18 -18
17 18 18
UCLH 14 12 22 19 24 25 24 35 31 36 39 26 42 45 51 40 43 37
UCLH NMUH BHRUT RFH
BHRUT 0 1 3 2 13 11 10 17 11 13 14 13 14 13 27 52 42 0
NorthMid 0 1 1 8 4 9 12 13 16 19 20 24 9 9 21 27 20 10
Royal Free 0 0 0 0 0 0 0 0 0 0 9 12 20 19 21 37 23 28 Referral numbers in August-
September are lower
E-referral’s has gone live
Source: UCLH, North Middlesex , Royal Free and BHRUT dataNorth London MDCs April 18- Oct 18
Diagnosis and cancer conversion rate
350
300
250
200
150
100
50
0
Cancers Non cancer All Test normal
North Mid 7 77 98
BHRUT 10 40 60
UCLH 28 287 96
Royal Free 5 48 49
North Mid BHRUT UCLH Royal Free
Cancer conversion rate
Site
Number of Cancer conversion Time to cancer Cancer conversion rate at ULCH is currently on 4.95 % this
referrals rate diagnosis (mean) may increase still awaiting outcomes for 2 more patients .
UCLH 565 4.95% 36.8 Time to cancer diagnosis very good with North Middlesex
North Mid 223 2.81% 25.5 currently averaging on 25.5 days.
BHRUT 256 3.90% 36.1 All sites need to improve in data entry of outcome status and
Royal Free 169 2.88% 42.6 date communication.
Source: UCLH, North Middlesex , Royal Free and BHRUT dataNorth London MDCs April 18- Oct 18
Types of Cancer
9
8
7
6
5
4
3 TOTAL
2 ULCH
1
0 BHRUT
NORTH MID
ROYAL FREE
Highest number are Pancreatic, Colon and Lung cancer with total of 8 (16%) each
Source: UCLH, North Middlesex , Royal Free and BHRUT data1 2 3 4
North London MDCs
Patient Experience
Patient experience
80% of patients are
90
extremely likely to
recommend the MDC
80 service to family and
70 friends
60 82.8 % felt they received
50 their first hospital
appointment as soon as
40
was necessary
30
89.3% felt their test results
20 were explained in a way
10 they could understand
0 78.6% felt they waited a
Extremely Likely Neither Don’t Not likely reasonable amount of time
likely likely or know
unlikely while attending clinics and
appointmentsMDC Challenges and Opportunities
Challenges Opportunities
• Creating the team – • Model of care clarified –
clinicians and CNS and to be enhanced
• Trust support - Clinic space • Strong CCG/GP support
and consultant time • 2WW pathway on ERS
• GP education • Pathway for rejected
• Integrating into CCG and referrals developing
Trust referral systems • Develop A&E pathway
• Excessive inappropriate • Is potential model for FDS
referrals – conversion rate • London Research Network
• Currently speeds diagnosis developing
but not improving stage
34So what do we need?
• Better awareness of the ‘pattern’ of cancer symptoms
• Manage population risk – obesity, smoking, alcohol (pancreatitis)
• Faster diagnostic pathways (MDCs)
• Identify high risk population and screening/surveillance methods
– Hereditary pancreatic cancer (5-10% of PC)
– IPMN surveillance – all need monitoring
– New diagnosis of Diabetes – 1% > 50 yrs in 3 years1
– Acute pancreatitis – 1.5-6.3% in 2 years 2, 3
– Chronic pancreatitis 1 and 4% risk of PD over 1 and 20 yrs4
– Other genetic syndromes – Lynch, Peutz-Jeghers
• Better biomarkers
1ChariS.T. et al Gastroenterology. 2005;129:504–511
2Kimura Y. et al. Intern. Med. 2015;54:2109–2114
3Munigala S. et al. Clin. Gastroenterol. Hepatol. 2014;12:1143–1150.
4Lowenfels A.B.et al International Pancreatitis Study Group. N. Engl. J. Med. 1993;328:1433–1437.
35The Future for Early Diagnosis of Pancreatic Cancer
• Patient awareness
• GP training and direct access to tests
• Blood / Urine biomarkers
• Rapid diagnostic pathways - MDCs
• Increase screening and surveillance
Thank youYou can also read