Isolated unilateral brachial plexus injury following carbon monoxide intoxication: a case report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Isolated unilateral brachial plexus injury following
carbon monoxide intoxication: a case report
Shu liu
Chongqing Medical University
Hou-chao Sun
Chongqing Medical University
Xu Yang
Chongqing General Hospital
Zhi-You Cai ( caizhiyou@ucas.ac.cn )
Chongqing Medical University
Case Report
Keywords: carbon monoxide intoxication, brachial plexus injury, peripheral neuropathy
Posted Date: January 3rd, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2364878/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 1/12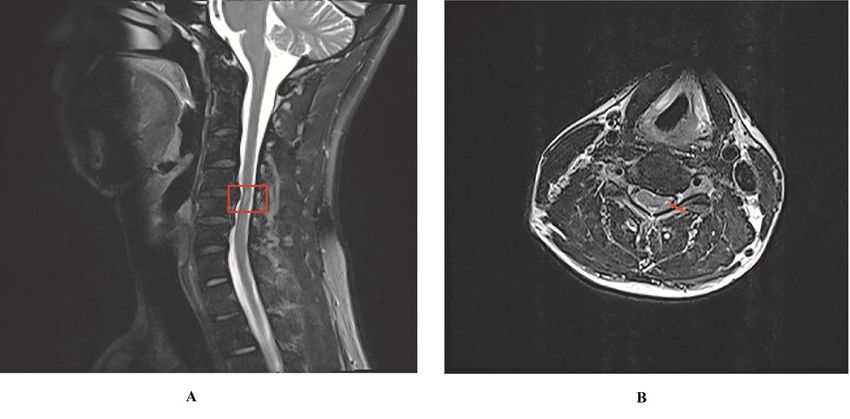
Abstract
Background
CO is an odorless, colorless gas that often still undetectable until exposure results in coma or death.
Carbon monoxide (CO) intoxication is a common fatal poisoning worldwide. The toxic effects of CO lead
to tissue hypoxia and produce systemic and neurological complications. Besides, some severe
neurological manifestations and delayed sequelae may occur after CO intoxication. However, peripheral
neuropathy following CO poisoning is relatively rare that usually occurs in young people. Beforehand,
only one case reported unilateralplexopathy following CO poisoning, which combined with
rhabdomyolysis and cognitive dysfunction.
Case presentation
A 31-year-old young man slept in his private car with closed doors and windows. His wife discovered him
in about 7 hours when he was in an unconscious state. He was diagnosed with acute carbon monoxide
poisoning. After about 12 hours in a coma, he returned to an alert state without conscious disorder.
However, he woke up with left upper arm weakness associated with limitation of movement of the left
upper limb. The electrophysiological conclusion was left incomplete total brachial plexopathy.
Conclusion
Ischemia of spinal cordcaused by CO intoxication may be a key mechanism in this case. Hyperbaric
oxygen therapy as soon as possible is necessary to prevent peripheral neuropathy after acute CO
intoxication. Besides, persisting in rehabilitation training might be important to treat peripheral
neuropathy after acute CO intoxication.
Background
Carbon monoxide (CO) intoxication is the most common fatal poisoning all over the world. Symptoms of
carbon monoxide poisoning can vary from a mild headache to critical illness. It can affect multiple
organs including brain, heart, lung, kidney, skeletal muscle and peripheral nerve. Most complications have
been widely described. However, few studies have reported peripheral neuropathy and
electrophysiological features[1]. We present a case of isolated unilateral brachial plexopathy following
CO poisoning.
Case Presentation
A 31-year-old young man slept in his private car with closed doors and windows at about 11 o’clock in
11th of February 2022. His wife discovered him in about 7 hours when he was in an unconscious state.
He was admitted to the hospital and diagnosed with acute carbon monoxide poisoning. His blood test
showed elevated carbon monoxide hemoglobin (16.2%), normal glucose, hepatic function and complete
Page 2/12blood count tests. On brain magnetic resonance imaging (MRI), punctate slightly hyperintense signal at
the bilateral basal ganglia was detected. After about 12 hours in a coma, he returned to an alert state
without conscious disorder. However, he woke up with left upper arm weakness associated with limitation
of movement of the left upper limb. Neurological examination showed the left arm paralysis (Manual
muscle tests revealed 1 medical research council (MRC) grade), distal vibratory, thermic and algic
hypoesthesia, disappeared deep tendinous reflect in left upper arm. Ultrasonic examination showed that
the left median and left radial nerves were swollen in the forearm and upper arm. A motor nerve
conduction study showed a normal motor conduction velocity (MCV) for left ulnar, median, and radial
nerves, and a decreased amplitude of compound muscle action potentials (CMAP) for left axillary and
musculocutaneous nerves. Besides, sensory conduction velocity (SCV) for left median nerve and ulnar
nerves are in the normal range (Table 1). Needle electromyography revealed abnormal spontaneous
activities including positive sharp wave and fibrillation potential in left deltoid, left biceps brachii, and left
triceps brachii (Table 2). The electrophysiological interpretation was left brachial plexopathy involve
upper and middle branches(severe upper branches abnormalities and moderate middle branches
abnormalities). The patient underwent rehabilitation training and about 80 sessions of hyperbaric oxygen
therapy. He readmitted to hospital due to check-up 70 days after CO intoxication. The limitation of
movement in his left upper limb is slightly improved(Manual muscle tests revealed 3 medical research
council (MRC) grade). There was existed sensation to pinprick and light touch in the left upper limb. In
addition, the patient remained no other sequelae. We found marked atrophy of left deltoid and biceps
(Fig. 1). Compared to admission, the re-examination of the cerebral magnetic resonance imaging (MRI)
showed no significant change. The sense nerve conduction study showed a decreased nerve conduction
velocity and amplitude for left radial nerves (Table 3). Motor nerve conduction was normal except for the
left axillary and musculocutaneous motor amplitude which were highly decreased (Table 4). The
electrophysiological conclusion for this admission was left incomplete total brachial plexopathy involved
axillary, musculocutaneous and radial nerves. It seems that the patient’s relevant examination results did
not change much compared with the first. However, we did a total spine magnetic resonance imaging
(MRI) for the man. Long strip T2 high signal was shown in the left part of the cervical medulla at the level
of the 4/5 intervertebral space (Fig. 2). During this hospitalization, the man continue to receive
rehabilitation training and hyperbaric oxygen therapy.
Page 3/12Table 1
Motor nerve conduction study and sensory nerve conduction study in the patient after carbon monoxide
intoxication
Nerve Dl Amp Dis Vel
mS mV mm m/s
MNCS
Axillaris left
Erb-Del. 8.85 1.19
Medianus left
Erb-Del. 3.67 12.5
Medianus left
Wrist-APB 3.27 20.1
Elb-APB 6.72 18.1 195 56.5
Elb-F 25.8 0.55
Musculocutaneous left
Erb-Biceps 8.41 0.29
Musculocutaneous right
Erb-Tricep 4.67 24.8
Radialis left
Erb-Tricep 4.45 19.7
Ulnaris left
Wrist-ADM 2.42 13.1
Elbow-ADM 5.33 12.9 195 67
Stim 1-F 21.1 2.3
Stim 2-F 20.3 2.7
SNCS
Medianus left
Wrist-DigⅡ 2.6 17.6 170 65.4
MNCS, motor nerve conduction study; Dl, distal latency; Amp, amplitude; Dis, distance; Vel, velocity;
Erb, elbow; Del, deltoid; APB, abductor pollicis brevis; ADM, abductor digiti minimi; Sti, stimulation;
SNCS, sensory nerve conduction study.
Page 4/12Nerve Dl Amp Dis Vel
mS mV mm m/s
Ulnaris left
Wrist-DigⅤ 1.96 46.9 120 61.2
MNCS, motor nerve conduction study; Dl, distal latency; Amp, amplitude; Dis, distance; Vel, velocity;
Erb, elbow; Del, deltoid; APB, abductor pollicis brevis; ADM, abductor digiti minimi; Sti, stimulation;
SNCS, sensory nerve conduction study.
Table 2
Electromyographic findings in the patient after carbon
monoxide intoxication
Spontaneous Activities
Muscle Explanation Fib PSW
Right Biceps Normal 0/10 0/10
Right Deltoid Normal 0/10 0/10
Right Vastus Normal 0/10 0/10
Left Vastus Normal 0/10 0/10
Left ADM Normal 0/10 0/10
Left Abd pollicis brevis Normal 0/10 0/10
Left Triceps 2/10 0/10
Left Biceps Loss of MU 6/10 6/10
Left Deltoid Loss of MU 6/10 6/10
Fib, fibrillation potential; PSW, positive sharp wave; ADM, abductor digiti minimi; Abd, abductor.
Page 5/12Table 3
Sensory nerve conduction study in the patient when readmission.
Nerve/Part Site Onset Lat Peak Lat Amp Distance Velocity
ms ms mm mm m/s
Left median nerve- Middle finger
Wtist DigⅢ 2.4 3.18 56.4 125 52
Left ulnar nerve- Little finger
Wrist DigⅤ 2.08 2.81 31.5 100 48
Left radial nerve- Anatomical snuff box(Forearm)
Forearm Wrist 2.19 2.92 14.0 95 43
Lat, latency; Dig, digiti; Amp, amplitude.
Page 6/12Table 4
Motor nerve conduction study in the patient when readmission.
Nerve/Part Muscle Latency Amplitude Distance Velocity
ms mV mm m/s
Left radial nerve- EIP
Forearm EIP 2.34 3.3
Spiral Gr EIP 3.7 3.6 80 59
Left median nerve- Abductor pollicis brevis
Wrist Abductor pollicis brevis 3.23 9.4
Elbow Abductor pollicis brevis 6.25 10.9 160 53
Left ulnar nerve- ADM
Wrist Abductor digiti minimi 2.66 10.9
Elbow Abductor digiti minimi 5.1 9.0 160 65
Left axillary nerve- Deltoid
Erb's Deltoid 2.92 8.9 190
Left musculocutaneous nerve- Biceps
Erb's Biceps 4.79 1.6 302
Right axillary nerve- Deltoid
Erb's Deltoid 3.44 28
Right musculocutaneous nerve- Biceps
Erb's Biceps 3.96 9.1
Right radial nerve- EIP
Forearm EIP 2.60 8.9
Spiral Gr EIP 4.01 9.2 95 68
EIP, extensor indicis proprius; Erb, elbow; ADM, abductor digiti minimi.
Discussion
Carbon monoxide (CO) has the toxic effects of tissue hypoxia and produces various systemic
complications. CO poisoning has previously been related to central nervous system, cardiovascular
system, respiratory system, hematological system, metabolic and endocrinological system,
musculoskeletal system and changes in perception of the visual and auditory systems, especially the
Page 7/12cardiovascular system and central nervous system such as amnesia, encephalopathy, dysarthria,
parkinsonism and peripheral neuropathy. Among them, little has been reported regarding peripheral
neuropathies.
To our knowledge, there was a large-scale clinical study about neuropathy after CO poisoning. Among
2759 patients with acute CO poisoning examined clinically between 1976 and 1982, peripheral
neuropathy was diagnosed in 23 subjects( 11 men and 12 women, mean age was 29.3) by
electrophysiological detection. Of all patients, 14 subjects had sensory symptoms, 8 subjects had mixed
symptoms and only one had isolated motor symptoms. All are involve in the lower extremity except 2
subjects. The study also show that peripheral neuropathy after CO poisoning commonly affected young
people and all recovered within 3–6 months[2]. Rahmani et al reported a 42-year-old man with reversible
bilateral brachial plexus injury after acute CO poisoning, who had good prognosis after hyperbaric oxygen
therapy[3]. Gi-Young Park et al reported unilateral brachial plexopathy with impaired cognitive function
after CO intoxication. Electrophysiological interpretation was left incomplete total brachial plexopathy
with axonal involvement. The 45-year-old patient had poor prognosis with no significant change of left
upper extremity weakness and impaired cognitive function when 11 months after CO intoxication[4].
Other articles have also reported peripheral neuropathy after
CO intoxication: Sciatic neuropathy and rhabdomyolysis, motor and sensory peripheral neuropathy,
unilateral diaphragmatic paralysis.
The precise pathogenesis of peripheral neuropathy following CO intoxication remains in doubt. However,
4 possible mechanisms may be responsible for this: hypoxia due to CO and subsequently ischemia, nerve
compression, cytotoxic effect of CO and petechial hemorrhages. CO causes hypoxia through the
formation of COHb and binding to heme-containing proteins, particularly cytochrome c oxidase and
myoglobin. In addition, CO binds to platelet heme protein, causing the release of NO. Increased NO
produces peroxynitrite (ONOO), which impairs mitochondrial function and worsens tissue hypoxia[5]. The
central nervous system are most vulnerable to the effects of ischaemia and hypoxia. The thoracic spinal
cord was feed by the radiculomedullary arteries, which originate from a few intercostal arteries (from the
subclavian artery and aorta), compromise of blood flow from these arteries potentially creates a great risk
of ischemia because of poor collateralization in the thoracic vascular region. Besides, The watershed
effect is common in the vascular system of the spinal cord. It occurs when 2 streams of blood flowing in
opposite directions meet. The watershed effect is at its maximum in the midthoracic area because the
distance between radicular arteries is the greatest[6]. In the case, we found that Long strip T2 high signal
was shown in the left part of the cervical medulla at the level of the 4/5 intervertebral space. Abnormal
signal intensity of the left cervical spinal cord is present at MRI at a level suggestive of a correlation with
the clinical symptoms and signs. At that level there is also a disk protrusion. However, it is clear that this
lumbar disk protrusion did not compress the spinal cord of patient, so it was not sufficient to cause
brachial plexus injury. The patient’s wife found him lying in the driver's seat with his head tilted to the left.
It is possible that it is a spondilogenic compression myelopathy (ischemic pathomechanism?) possibly
related to the position of the unconscious patient in the car. So we suspect that the ischemia of spinal
Page 8/12cord caused by CO intoxication may be a key mechanism of left brachial plexopathy. Besides, nerve
compression and cytotoxic effect of CO should also be considered. The young man in our case
experienced isolated unilateral brachial plexus injury following acute CO poisoning with incomplete
improvement after nearly 3 months, which is the second case on unilateral brachial plexopathy following
CO intoxication in literature so far. Ischemia of spinal cord caused by CO may be the main mechanism
about unilateral brachial plexopathy. Therefore, correct hypoxia caused by CO (hyperbaric oxygen and
normobaric 100% oxygen) as soon as possible is necessary to prevent peripheral neuropathy after acute
CO intoxication. In addition, persisting in rehabilitation training might be important to treat peripheral
neuropathy after acute CO intoxication.
Declarations
Competing interests The authors declare no competing interests.
Ethical approval and consent to participate The Institutional Review Board at Chongqing General Hospital
approved this case report.
Consent for publication Written informed consent for publication of this case report was obtained from
the patient.
Availability of data and materials The datasets used or analysed during the current study are available
from the corresponding author on reasonable request.
Funding This work was supported by the Construction Project of Capacity Improvement Plan for
Chongqing Municipal Health Commission affiliated unit (2019NLTS001)-ZS03174, operating grant to
Chongqing Key Laboratory of Neurodegenerative Diseases (1000013), Chongqing Talent Project
(2000062), Overseas Students entrepreneurial fund (2000079), and Plan for High-level Talent Introduction
(2000055).
Author Contributions Shu, Liu: Data Curation, Writing - Original Draft, Visualization. Hou-chao Sun: Writing
- Review & Editing. Xu Yang: Writing - Review & Editing. Zhi-you Cai: Writing - Review & Editing.
Acknowledgements This work was supported by the Construction Project of Capacity Improvement Plan
for Chongqing Municipal Health Commission affiliated unit (2019NLTS001)-ZS03174, operating grant to
Chongqing Key Laboratory of Neurodegenerative Diseases (1000013), Chongqing Talent Project
(2000062), Overseas Students entrepreneurial fund (2000079), and Plan for High-level Talent Introduction
(2000055).
References
1. García A, Maestro I. Reversible motor and sensory peripheral neuropathy in a patient following acute
carbon monoxide intoxication. Electromyogr Clin Neurophysiol. 2005;45 1:19–21.
Page 9/122. Choi IS. A clinical study of peripheral neuropathy in carbon monoxide intoxication. Yonsei Med J.
1982;23 2:174–7. doi:10.3349/ymj.1982.23.2.174.
3. Rahmani M, Belaidi H, Benabdeljlil M, Bouchhab W, El Jazouli N, El Brini A, et al. Bilateral brachial
plexus injury following acute carbon monoxide poisoning. BMC Pharmacol Toxicol. 2013;14:61.
doi:10.1186/2050-6511-14-61.
4. Park GY, Kwon DR, Jung WB. Unilateral brachial plexus injury following carbon monoxide
intoxication: A case report. Medicine. 2018;97 30:e11699. doi:10.1097/md.0000000000011699.
5. Chenoweth JA, Albertson TE, Greer MR. Carbon Monoxide Poisoning. Critical care clinics. 2021;37
3:657 – 72; doi: 10.1016/j.ccc.2021.03.010.
6. Martirosyan NL, Feuerstein JS, Theodore N, Cavalcanti DD, Spetzler RF, Preul MC. Blood supply and
vascular reactivity of the spinal cord under normal and pathological conditions. J Neurosurg Spine.
2011;15 3:238–51. doi:10.3171/2011.4.Spine10543.
Figures
Page 10/12Figure 1
The muscle profile of the patient
Page 11/12Figure 2
Total spine magnetic resonance image(MRI) revealed long strip T2 high signal in the left part of the
cervical medulla at the level of the 4/5 intervertebral space on sagittal position(a) and cross section(b).
Page 12/12You can also read

















































