Oral Hygiene Recommendations In The Age of Dr. Google: An Evidence-Based Approach for Dental Professionals - A peer-reviewed article written by ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

EARN This course was
3CREDITS
CE written for
dentists,
dental hygienists,
and dental assistants.
© One Photo | Dreamstime.com
Oral Hygiene Recommendations
In The Age of Dr. Google:
An Evidence-Based Approach
for Dental Professionals
A peer-reviewed article written by Maria L. Geisinger, DDS, MS
PUBLICATION DATE: MARCH 2021
EXPIRATION DATE: FEBRUARY 2024
SUPPLEMENT TO
ENDEAVOR PUBLICATIONS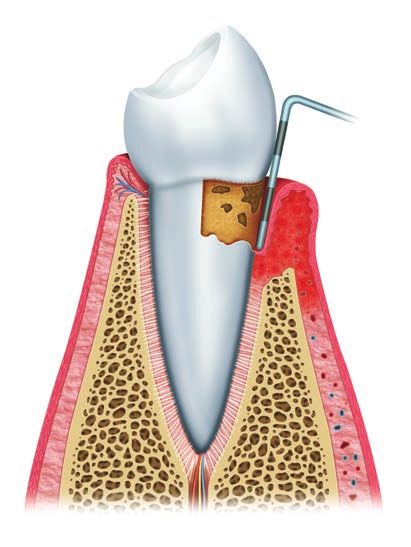
EARN
3CREDITS
CE
Oral hygiene recommendations This continuing education (CE) activity was developed by
Endeavor Business Media with no commercial support.
in the age of Dr. Google: An
This course was written for dentists, dental hygienists, and
dental assistants, from novice to skilled.
Educational methods: This course is a self-instructional
evidence-based approach for journal and web activity.
Provider disclosure: Endeavor Business Media neither has a
dental professionals
leadership position nor a commercial interest in any products
or services discussed or shared in this educational activity. No
manufacturer or third party had any input in the development of
the course content.
Requirements for successful completion: To obtain
ABSTRACT three (3) CE credits for this educational activity, you must pay
the required fee, review the material, complete the course
From charcoal toothpaste to oil pulling to “Flossgate,” recent controversies evaluation, and obtain an exam score of 70% or higher.
regarding ideal oral hygiene in the lay media have left many of our patients CE planner disclosure: Laura Winfield, Endeavor Business
Media dental group CE coordinator, neither has a leadership nor
with questions about the best way to take care of their teeth at home. While commercial interest with the products or services discussed
in this educational activity. Ms. Winfield can be reached at
dental associations, the National Institutes of Health (NIH), the Centers for lwinfield@endeavorb2b.com.
Disease Control and Prevention (CDC), and the United States Surgeon Gen- Educational disclaimer: Completing a single continuing
education course does not provide enough information to result
eral agree on the importance of proper self-delivered oral hygiene,1-3 there in the participant being an expert in the field related to the
continues to be confusion in the lay media and the public with regard to course topic. It is a combination of many educational courses
and clinical experience that allows the participant to develop
the role of patient-administered oral hygiene for the prevention of oral dis- skills and expertise.
eases. Current recommendations include brushing for two minutes twice Image authenticity statement: The images in this
educational activity have not been altered.
daily and cleaning between teeth to maintain a healthy mouth and smile.4 Scientific integrity statement: Information shared in this
Furthermore, customization of oral hygiene recommendations for patients CE course is developed from clinical research and represents
the most current information available from evidence-based
based upon their risk profiles allows for optimal outcomes for disease pre- dentistry.
vention. It is well established that there are over 700 identified species of bac- Known benefits and limitations of the data: The
information presented in this educational activity is derived
teria and up to 1,500 putative pathologic microorganisms5-7 found in dental from the data and information contained in the reference
section.
plaque biofilms. Many of these organisms as well as other factors, including
Registration: The cost of this CE course is $59 for three (3)
bacterial nutrients, food debris, molecules that facilitate bacterial adhesion CE credits.
and invasion and other extrinsic factors in the environment, and the body’s Cancellation and refund policy: Any participant who is not
100% satisfied with this course can request a full refund by
own immune response, contribute to diseases of the teeth and gingival tis- contacting Endeavor Business Media in writing.
sues. This course will review current recommendations for oral home care, Provider information:
Dental Board of California: Provider RP5933. Course
discuss strategies to deliver person-centered oral hygiene instructions for registration number CA code: 03-5933-21000. Expires
patients based upon risks for oral diseases, and review the current evidence 7/31/2022. “This course meets the Dental Board of California’s
requirements for three (3) units of continuing education.”
regarding oral hygiene practices and/or products.
Endeavor Business Media
is a nationally approved PACE program provider
EDUCATIONAL OBJECTIVES for FAGD/MAGD credit.
1. Understand the risks and benefits of controversial oral hygiene practices Approval does not imply acceptance by any
regulatory authority or AGD endorsement.
and/or products 11/1/2019 to 10/31/2022.
Provider ID# 320452
2. List the optimal strategies and rationale for oral hygiene, including tooth- AGD code: 490
brushing, interdental cleaning, and use of dentifrices and mouth rinses
3. Develop home-care recommendations that focus on evidence-based
strategies for oral health and emphasize individualized patient care rec-
ommendations based upon patient needs Endeavor Business Media is designated as an approved Provider by the American Academy of
4. Discuss the importance of preventive strategies for oral diseases, includ- Dental Hygiene, Inc. #AADHPNW (January 1, 2021-December 31, 2022). Approval does not imply
acceptance by a state or provincial Board of Dentistry. Licensee should maintain this document in
ing maintaining good oral hygiene in order to promote oral and overall the event of an audit.
well-being with a wide range of patients and interdisciplinary colleagues
Endeavor Business Media is an ADA CERP–recognized provider.
ADA CERP is a service of the American Dental Association to assist dental professionals in
identifying quality providers of dental continuing education. ADA CERP does not approve or
endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards
of dentistry.
Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at
ada.org/goto/cerp.
Go online to take this course.
DentalAcademyofCE.com
QU I CK AC C E S S C O D E 21000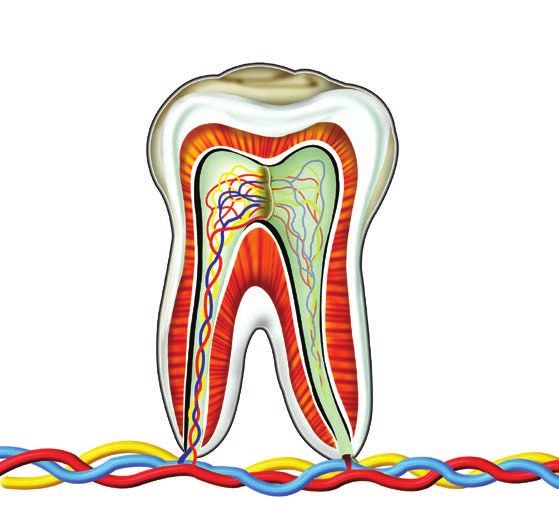
D ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
INTRODUCTION of such practices and products to stan- EPIDEMIOLOGY AND ETIOLOGY OF
Dysbiotic dental plaque biofilm is the pri- dard oral hygiene measures is imperative. CARIES AND PERIODONTAL DISEASE
mary etiology for both dental caries and peri- This was brought into particularly sharp Caries: Dental caries, or tooth decay,
odontal disease, the two most prevalent oral focus in August 2016 when the US govern- results from the breakdown of the hard
diseases.8 To maximize benefits of dental care ment released a statement discussing the tissues of the tooth (enamel, dentin, and
and maintain treatment results, patients are omission of oral hygiene recommendations cementum) due primarily to the acid by-
integral copractitioners with their oral health in the 2015-2020 Dietary Guidelines for products of bacterial metabolism of car-
providers. The sustained daily maintenance America (DGA).13 For the first time since bohydrates. Bacteria use simple sugars
of oral hygiene is critical to the success of pro- 1979, the DGA omitted recommendations as a food source and produce metabolic
fessional oral health interventions. Unfortu- for: 1) consumption of fluoridated water, acids as a part of the process to break down
nately, patient levels of home care are variable 2) reduction of sugary food and beverage those sugars.16,17 Conditions and medica-
and often suboptimal. Despite recommen- consumption, and 3) toothbrushing and tions that affect salivary flow, poor tooth
dations from the American Dental Associ- flossing as effective methods to reduce cleaning, dietary sugar and acid content,
ation (ADA) that individuals brush for two the risk of dental caries. Furthermore, the and fluoride availability can all affect the
minutes twice daily,9 the average total daily government statement indicated that the rate of caries.12
toothbrushing time ranges between 45-70 flossing recommendation was excluded O ral hard ti ssu es undergo
seconds.10 Similarly, patient compliance with due to a lack of definitive scientific evi- remodeling through a demineralization-
regular and sustained daily use of dental floss dence stating flossing prevents dental car- remineralization process.18 As pH within
for interdental cleaning has been estimated ies.14 The 2016 report cited a meta-analysis the oral cavity drops, demineralization
to be as low as 2%.11 Patients also report low that found that data supports interden- occurs, and as the pH increases,
levels of satisfaction with flossing, with more tal cleaning for the prevention and treat- remineralization of those tissues is seen.
than 35% of respondents to an American ment of gingivitis, but additional studies The net resultant mineral exchange is a
Academy of Periodontology (AAP) survey are needed to evaluate the role of inter- determinant of caries development and
stating that they would rather perform an dental cleaning in the prevention of den- progression.19 Dentistry has been focused
unpleasant task, such as filing a tax return tal caries and periodontitis.15 In response on prevention strategies to reduce caries
or cleaning toilets, than floss.12 to the media coverage of this report and rates for public health benefit. Water
Given the lack of enthusiasm for oral overall consumer interest in more natural fluoridation has proven to be one of the
hygiene measures,12 interest in alterna- or homeopathic therapies, dental practi- most cost-effective methods for reducing
tive methods of tooth cleaning and novel tioners and dental patients have demon- overall caries rates in the population,
oral hygiene products continues to grow. strated an increased interest in alternative with every $1 spent on water fluoridation
Thus, establishing comparative efficacy therapies and products. returning $5-$32 in decreased health-care
The return on investment for
Dental emergencies cause 2 million water fluoridation is estimated
emergency room visits annually to be between $5 and $32
for every $1 spent
It is anticipated that
Medicaid expenditures for The average cost of
preventable dental disease will be oral hygiene aids
$ 21 million in 2020 per person per year is $9
FIGURE 1: Caries impact in the United States
DentalAcademyOfCE.com 3D ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
costs within the community.20 However, and, in most cases, the severity is related to development and progression.35 Plaque
fluoridation remains insufficient to fully the amount and type of bacteria present on control is critically important to pre-
control dental caries, particularly in the tooth and soft tissue surfaces throughout vent and treat gingivitis prior to develop-
absence of regular, effective oral hygiene. the mouth and may be influenced by ment of periodontitis36 and maintenance
Dental caries is a highly prevalent dis- individual patient susceptibility to of periodontal health after arresting
ease in both children and adults, despite disease.24,25 The percentage of adults periodontitis.37,38
declining rates of both treated and without attachment loss who have
untreated caries since the 1970s. Nearly gingivitis is 93.9%.26 Removal of dental ORAL HEALTH AND HYGIENE AS
19% of US children ages 5-19 and almost plaque biofilm and local etiologic factors PERSON-CENTERED CARE
32% of US adults ages 20-44 have untreated is the definitive treatment for gingivitis Personalized assessments for car-
caries.21 Caries and subsequent edentulism and reduces local and systemic levels of ies and periodontal disease risk: Risk
negatively affect patients’ quality of life.22 inflammatory markers in such patients.7,27 assessment to predict future risk of disease
Nearly 51 million school hours are lost each Untreated gingivitis may progress to allows for more targeted interventions to
year to dental-related illnesses.23 Employed periodontitis. Periodontitis is a chronic prevent or control caries and periodon-
adults also lose 164 million work hours disease of the hard and soft tissues sup- tal diseases. Risk factors for both diseases
each year to dental disease.23 The emo- porting the teeth initiated by dysbiotic may be anatomical/physical, biochemi-
tional, financial, and educational impact bacterial plaque biofilm, which initiates cal, demographic, or lifestyle determinants
of caries is critically important and proper host immuno-inflammatory responses that that contribute to the development and
oral hygiene and home care are vital to the cause progressive destruction of the peri- progression of disease. A comprehensive
management and prevention of dental car- odontal ligament and alveolar bone.28-33 evaluation should include a history of oral
ies ( figure 1). Periodontitis typically has a slow to mod- diseases as well as an assessment of risk
Periodontal diseases: Periodontal erate rate of disease progression, but epi- factors associated with both caries and
diseases include inflammatory and tissue- sodes of accelerated attachment loss may periodontal disease (tables 1 and 2).
destructive diseases of the supporting be associated with local and/or systemic Behavioral modification: Motivat-
structures around the teeth, comprised factors.30,31 Destructive periodontitis has ing and educating patients to adequately
of the gingival tissues, periodontal been found to affect approximately 42% perform oral hygiene measures can be a
ligament, alveolar bone, and cementum. of US adults ( figure 2).1 Of those individu- clinical challenge. Patients may underesti-
All individuals are susceptible to gingivitis als, 7.8% have severe periodontitis.34 Ciga- mate brushing time12 and fail to adequately
and will develop gingivitis within 21 days rette smoking and uncontrolled or poorly remove microbial biofilm despite dem-
if no oral hygiene measures are instituted. controlled diabetes mellitus have been onstration of optimal methods.13 Patients
Gingivitis is caused by bacterial plaque shown to be risk factors for periodontitis report that their rationale for perform-
ing oral hygiene focuses on social/esthetic
factors, including fresh breath and attrac-
tive smile, and, lastly, to avoid disease.14
Improving patients’ understanding of the
importance of plaque control for treat-
ment of both caries and periodontal dis-
ease is critical to establishing new routines.
Oral hygiene interventions also require
reinforcement over time. Patients’ effec-
tiveness and compliance for oral hygiene
has been shown to decrease after three to
six months.17 It is of utmost importance
to personalize oral care instructions for
patients. Individualized techniques have
93.9% of individuals without
attachment loss have gingivitis. proven effective in improving oral hygiene
levels,14,18 and motivational interviewing
may be one technique to allow for patient
self-efficacy and improve awareness of
the importance of plaque control to oral
health.19,39 A single session of motivational
42.5% of US adults have periodontitis. interviewing to improve oral home care has
been shown to improve gingival bleeding
FIGURE 2: Periodontal disease prevalence in the United States scores and plaque index.20
4 DentalAcademyOfCE.comD ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
TABLE 1: Caries risk assessment—considerations TABLE 2: Periodontal risk assessment— toothbrushing in the short (0-3 months)
and screening considerations and screening and long (> 6 months) terms.46 Powered
Anatomical and intraoral risk factors History of past disease progression toothbrushing is effective and safe for oral
• Active and/or new carious lesions? • History of previous attachment soft tissues while providing a statistical
• History of previous carious lesions loss over the past five years? benefit in both plaque and gingival indi-
in the last three years? • Overall bone loss/age?
• Recurrent caries around • Biofilm deposits as compared
ces.46,47 While the clinical implications of
existing restorations? to disease progression? these reductions is unknown, it should
• Deep pits and fissures? be noted that the recommendation of a
• Enamel hypomineralization? Tobacco/nicotine consumption
• Exposed radicular surfaces? powered toothbrush may improve plaque
• Pack-year tobacco consumption?
• Plaque-retentive intraoral surfaces? • History of tobacco use (time removal in patients who struggle to achieve
• Orthodontic treatment or use of since cessation)?
other intraoral fixed appliances? adequate levels of oral hygiene or who have
• Alternative nicotine consumption (use of
Oral hygiene practices and fluoride electronic nicotine delivery devices [ENDs])? an increased susceptibility to periodontal
exposure Diabetes mellitus/glycemic control
diseases or high caries rates.46,47 Accep-
• Plaque present? tance of powered toothbrushes among
• Current HbA1c levels?
• Current understanding of plaque
• History of HbA1c over time?
patients of all ages has been reported to
control and the patient’s motivation?
• Brushes with fluoridated toothpaste daily? • History of diabetic complications? be high41,48 and may be of particular ben-
• Drinks city-added or naturally • Additional risk factors (use of corticosteroids, efit in individuals who demonstrate dif-
occurring fluoridated water? metabolic syndrome, obesity, etc.)?
ficulty in motivation or execution of oral
Dietary analysis Microbial pathogenicity
hygiene measures.
• Bacterial biofilm composition and
• Carbohydrate intake, including frequency intraoral bacterial count?
(consumption of sugar-sweetened • Presence of “red complex” bacteria? FLOSSING
beverages, e.g., soda, fruit drinks, • High quantities of bacterial
energy drinks, and sports drinks)? Dental floss is the most widely recom-
plaque biofilm deposits?
• Multiple between-meal • Inability to perform adequate mended tool for removing dental plaque
carbohydrates/day ingested? oral hygiene measures? from proximal tooth surfaces.49 In 2016 a
Microbial and salivary factors Immunological deficits controversy erupted in lay media when an
• Bacterial biofilm composition and intraoral • Neutrophil chemotactic deficiencies? article published in the New York Times
bacterial count (saliva testing)? • Existing immunodeficiency diseases?
• Xerostomia? suggested that flossing may not be ben-
• Preexisting autoimmune diseases?
• Prescription drugs affecting eficial to oral health.50 Within the dental
salivary rate and/or quality? Familial/genetic risk factors
• Decreased salivary buffering capacity?
community, this controversy was referred
• Familial history of periodontal disease? to as “Flossgate” and reflected a discon-
Familial/genetic risk factors • Familial history of early tooth loss?
• Inherited anatomical considerations? nect between the scientific understand-
• Family caries history?
• Inherited anatomical considerations? Social/psychological risk factors ing of the benefits of interdental cleaning
Social/psychological risk factors • Low socioeconomic status?
and the lack of longitudinal controlled tri-
• Dental anxiety? als that might demonstrate differences in
• Dental anxiety? • Limited access to dental care
• Limited access to dental care caries rates. Regular flossing as an adjunct
or oral hygiene materials?
or oral hygiene materials? to toothbrushing has been demonstrated
Other systemic risk factors
Systemic or medical risk factors to decrease plaque levels interproximally
• Pregnant individuals? and to decrease gingival inflammation over
• Chronic systemic diseases? • Patients with systemic diseases
• Medically or physically challenged? associated with periodontal diseases? toothbrushing alone.40 Furthermore, indi-
• Mental or physical disabilities that prevent viduals who floss demonstrate lower lev-
adequate delivery of oral hygiene?
TOOTHBRUSHING els of caries and gingival inflammation in
Toothbrushing with both manual and observational studies.51 In a matched twin
power brushes has been shown to be Similarly, high amounts of force are not cohort, the addition of flossing to tooth-
effective in the removal of plaque on tooth necessary for adequate plaque removal and brushing alone decreased visible plaque,
surfaces.40,41 Time spent toothbrushing is can cause trauma to hard and soft tissues gingival bleeding, and altered the subgin-
associated with a significantly greater in the mouth.45 It is important to counsel gival flora to reduce the proportions and
amount of plaque removal up to approxi- patients to replace toothbrushes regularly amounts of bacterial species associated
mately two minutes, or 30 seconds per since bristle wear after nine weeks of nor- with periodontal disease and dental car-
quadrant.42 Softer toothbrush bristles are mal use can affect the efficacy of plaque ies, including T. denticola, P. gingivalis,
associated with superior plaque removal removal.43 T. forsythia, P. intermedia, A. actinomy-
subgingivally and interproximally due Powered toothbrushes: In a meta- cetemcomitans, and S. mutans.52,53 While
to their increased flexibility and result analysis of current evidence, powered current randomized controlled trials do
in less gingival recession and abrasion toothbrushes were found to reduce not have large enough samples over suf-
to oral soft tissues than hard bristles.43,44 plaque and gingivitis more than manual ficient time to demonstrate lower caries
DentalAcademyOfCE.com 5D ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
rates in patients who perform brush- fill, than floss does for comfortable use.58 It has been concluded to be safe in concen-
ing and flossing compared to brushing Triangular wooden tips inserted in trations less than 1% for topical applica-
alone, decreased plaque scores are asso- interproximal areas, while better accepted tion, but even those low concentrations
ciated with decreased decayed, missing, by patients than flossing, demonstrate may cause mucosal sloughing.71
and treated (DMT) scores in adults and no overall reduction in plaque or gingival While no commercially available denti-
children.15,54,55 index, but do demonstrate a reduction in frices in the US contain the FDA-approved
Flossing is economical, effective when bleeding on probing (BOP) that is similar antigingivitis agent triclosan, it has been
performed correctly, and aids in removal to that seen with flossing.65 used in dentifrices in the past due to its
of plaque and food debris interproximally. Powered flossers have been shown to ability to reduce gingival inflammation.72
But challenges to implementation do exist. result in a reduction in interdental plaque The CDC has noted that triclosan was
Flossing may not be optimally effective in deposits and gingival bleeding when com- present in the urine of nearly 75% of the
areas with anatomical variations. Addition- pared to toothbrushing alone.62,63.66 The individuals over six years old tested in the
ally, adequate flossing habits are difficult magnitude of this reduction is variable National Health and Nutrition Examina-
to establish. It is reported that only 8% of and dependent upon the type and design tion Study (NHANES) from 2003-2004.71
teenagers floss daily and the number of all of powered flosser.62 These devices may be While laboratory animal studies have dem-
individuals who floss daily may be as low especially beneficial in individuals with onstrated varied results,73 evidence of thy-
as 2%.12,56-58 Increasing patients’ willingness dexterity issues. Implants present with dif- roid disruption, carcinogenic potential,
to floss and their ability to sustain habits ferences in cross-section and emergence and allergic reactions have been seen in
over time may depend upon the behav- profile when compared to natural teeth; animal testing. However, the Environmen-
ior modification techniques employed by therefore, patients with implants may ben- tal Protection Agency’s Cancer Assessment
the dental health-care professional, and efit from the use of a powered flosser, but Review Committee (CARC) has classified
we should be willing to recommend other the angle of the floss jet should be perpen- the carcinogenic potential of triclosan as
interdental cleaning techniques if adher- dicular to the implant fixture to protect the “not likely to be carcinogenic to humans”
ence is suboptimal. implant/soft-tissue seal.67 based upon the current evidence.73 Never-
theless, in 2016 the FDA issued a final rule
OTHER INTERDENTAL CLEANING DENTIFRICES that banned triclosan from many com-
METHODS Established products: The use of adjunc- mon over-the-counter (OTC) antiseptic
In patients for whom flossing results in tive chemotherapeutics delivered in den- agents, but allowed for its continued use
inadequate plaque removal or those who tifrices may offer some additional benefit in dentifrices and other products for anti-
cannot adhere to a flossing regimen, addi- over toothbrushing without such prod- gingivitis uses.74
tional interdental cleaning aids may be ucts. Fluoride-containing dentifrices have Emerging technologies: Emerging
preferable.58 Interdental brushes remove well-established effectiveness in reducing research has also shown dentifrices con-
more plaque interproximally when com- caries rates. Dentifrices with stannous flu- taining statin medications may reduce
pared to floss and have demonstrated sim- oride have antimicrobial properties that gingivitis through anti-inflammatory
ilar reductions in interproximal probing may reduce gingival inflammation.68 Many mechanisms.75 Edathamil has shown
depths and gingival bleeding.59-61 Interden- dentifrices contain pyrophosphates, which promise in reducing gingivitis levels by
tal brushes can be particularly helpful in interfere with crystal formation of calcu- chelation of cations that prevent the asso-
areas of concavities and root anomalies. In lus and may reduce supragingival calculus ciation of bacteria with the dental pellicle
patients who demonstrate gingival reces- formation by more than 30%.24 The effect early in bacterial plaque biofilm forma-
sion or those with previously treated peri- of pyrophosphate on subgingival calculus, tion.76 Dentifrices containing propolis, aloe
odontal disease, interdental brushes have however, is neglibile.69 vera, and miswak have all been reported to
been shown to be more effective than floss Dentifrices provide established ben- reduce gingivitis and/or have bactericidal
overall.62, 63 In adult patients who have ade- efits, but side effects may occur in some effects on cariogenic and periopathogenic
quate interdental space to use interdental patients, causing them to discontinue bacteria, but larger randomized trials are
brushes, plaque removal was greater with use. Dentifrices containing stannous flu- necessary to fully explore safety and effi-
toothbrushing and adjunctive use of inter- oride may result in temporary staining cacy of these products.77-80
dental brushes than with toothbrushing of teeth, although formulations that sta- Activated charcoal dentifrice is widely
alone, toothbrushing with floss, and tooth- bilize the stannous fluoride may dem- available commercially. While homeo-
brushing with interdental wooden sticks.64 onstrate reduced staining and lead to pathic medicine and dentistry have used
Furthermore, patients have been shown better long-term adherence to prescribed charcoal-based preparations since the
to prefer the use of interdental brushes use.70 Additionally, the surfactant sodium period of Ancient Greece, there are lim-
over flossing.61,63,64 Nevertheless, they may hexametaphosphate has been shown in ited current data to support the efficacy
not be correct for all sites as they require high doses to result in growth retardation of charcoal-containing dentifrice for caries
more interdental space, and less papillary and kidney swelling in laboratory animals. and gingivitis prevention.81 Furthermore,
6 DentalAcademyOfCE.comD ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
charcoal may alter or inactivate fluoride is considered to have a broad spectrum dietary supplements may improve oral
in dentifrice, and the abrasiveness of such of antimicrobial action, showing efficacy health outcomes in some patients. Further-
charcoal-containing dentifrices may pro- against gram‐positive and gram‐negative more, the use of anti-inflammatory com-
duce abrasion of enamel and dentin.81 bacteria, bacteria spores, fungi, protozoa, pounds to reduce gingival inflammation
and several viruses, and has been proposed may also prove to have adjunctive effects
MOUTH RINSES as a preprocedural rinse or as a prophylac- for patients at higher risk for periodontal
Established products: Mouth rinses con- tic measure against respiratory infections.91 diseases.94 Many of these ingredients have
taining antimicrobial substances, includ- Further research on the potential risks and also been proposed to be added to oral
ing cetyl pyridium chloride (CPC), essential benefits of long-term povidone-iodine use health-care home products, such as mouth
oils, and other antimicrobial ingredients, for maintenance of oral health is needed. rinses and dentifrices. Further research is
have been shown to be effective adjuncts to needed to determine their efficacy in stan-
adequate levels of brushing and interdental ADJUNCTIVE ORAL dardized clinical environments.
cleaning in reducing plaque and gingival HYGIENE ACTIVITIES
inflammation.82-85 Establishment of ade- Oil pulling: In oil pulling, one to two table- STANDARDS OF CARE FOR ORAL
quate levels of mechanical oral hygiene in spoons of oil are swished in the mouth for HYGIENE AND ORAL HYGIENE
addition to the use of mouth rinses should about 20 minutes, twice daily. It has been INSTRUCTION
be a goal of therapy. Bisbiguanide antisep- postulated that coating intraoral struc- Current oral hygiene
tics (including chlorhexidine gluconate) tures with lipids may alter the composition recommendations: Dental professional
have been shown to have antimicrobial and and ultrastructure of the dental pellicle and advocacy groups are united in
substantive effects.86 However, long-term and subsequent biofilm adherence.92 Addi- reinforcing the importance of regular
use is associated with several untoward tionally, it has been suggested that lipid and effective oral hygiene practices.1-4 It
side effects, including alterations in taste presence at tooth surfaces may convey has been stated that “the most important
and tooth staining, which make compli- resistance to acid erosion of hard tissues, behavioral factor, affecting both dental
ance with use challenging when consid- and anti-inflammatory effects of some lip- caries and periodontal diseases, is
ered a long-term treatment. Additionally, ids on oral soft tissues were described.92 routinely performed oral hygiene with
there is emerging evidence that beneficial However, much of this data is preclinical fluoride” and that “management of both
oral microflora may be affected by the long- and there is only limited evidence for the dental caries and gingivitis relies heavily
term use of broad-spectrum anti-infective therapeutic benefits of oil pulling. Current on efficient self-performed oral hygiene,
oral mouth rinses, such as chlorhexidine, published literature has not fully assessed that is toothbrushing with a fluoride-
and we do not yet know the effects of sig- the lipid composition of saliva and pelli- containing toothpaste and interdental
nificant alteration in the overall oral micro- cle after oil pulling nor the interactions of cleaning.”95 Emphasis on oral hygiene as
biome.87 Chlorhexidine mouth rinse has lipids with biofilm formation and matura- primary prevention of oral diseases and
also been shown to have cytotoxic effects tion.92 Long-term, randomized, controlled maintenance of health is tantamount for
on gingival fibroblasts in vitro, which may trials are needed to determine the poten- public health and individual patient care.
alter cell turnover and tissue repair.88 tial benefits of this practice.
Emerging technologies: Novel mouth It should be noted that oil pulling CONCLUSION
rinses, including those containing propo- may not be without risk. Kuroyama et al. As dental health-care professionals, it is
lis, oxygenating agents, amine alcohols, reported two cases of exogenous lipid imperative that we are able to adequately
metal ions, triclosan, and salicylamide, pneumonia associated with use of edi- interpret the scientific literature in a man-
have evidence to indicate their antimicro- ble oils in oil pulling for oral hygiene pur- ner that allows our patients to understand
bial properties.77,89 Further clinical trials are poses.93 The symptoms of exogenous lipid and implement the best practices for their
necessary to identify their utility and/or pneumonia are fever, weight loss, cough, oral health. While splashy headlines associ-
safety in clinical practice. There has also dyspnea, chest pain, and hemoptysis. Forty ated with novel approaches and oral health
been considerable recent interest in the percent of patients had mild or no symp- controversies such as “Flossgate” may be
biocidal efficacy of hydrogen peroxide and toms.93 Severe pneumonia with acute eye-catching to our patients, the underly-
povidone-iodine-containing mouth rinses. symptoms can be fatal to the patient.93 ing science is less titillating. Caries and
Hydrogen peroxide is generally consid- Dietary supplements: Bee products, periodontal disease are prevalent, serious
ered safe and in vitro studies have shown including honey, wax, and propolis; lico- diseases that represent a huge burden to
the hydroxyl radical and other oxygen- rice root (glycyrrhizin); and polyphenols the health and well-being of the population
ated species can act as potent oxidizing from green tea, berries, and wine have been as well as a cost burden on society. While
agents, reacting with lipids, proteins, and touted to have properties that may be anti- professional dental prophylaxis has been
nucleic acids,90 but further research needs cariogenic and bacteriostatic, which might shown to improve plaque levels and gingi-
to be performed on the in vivo efficacy affect dental plaque biofilm.94 While data vitis in the short term, these improvements
of specific formulations. Povidone‐iodine are still emerging, the adjunctive use of cannot be maintained without subsequent
DentalAcademyOfCE.com 7D ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
Toothbrushing Interdental cleaning Dentifrices Mouth rinses
• Brush for two minutes • Floss is cost-effective • Fluoride dentifrices have • Use of mouth rinses as
• Brush at least twice a day but may be less demonstrated significant an adjunct to oral hygiene
• Use a soft toothbrush accepted by patients reduction in caries rates may improve gingival
• Use a powered toothbrush • Interdental brushes • Anti-gingivitis agents index and caries rate
if compliance is poor demonstrate increased should be considered • Personalization of oral
plaque removal for patients at high risk hygiene recommendations
for periodontal disease improves overall outcomes
FIGURE 3: Oral hygiene recommendations and personalized dental care
optimization of home care by the patients 7. Mombelli A. Microbial colonization of the 19. Ten Cate JM. In vitro studies on the effects of
periodontal pocket and its significance fluoride on de- and remineralization. J Dent Res.
themselves ( figure 3). for periodontal therapy. Periodontol 2000. 1990;69(2 Suppl):614-619.
Clinical recommendations: Both 2018;76(1):85-96. 20. Griffin SO, Jones K, Tomar SL. An economic
dental caries and periodontal disease are 8. Meyle J, Chapple I. Molecular aspects of the evaluation of community water fluoridation. J
pathogenesis of periodontitis. Periodontol 2000. Public Health Dent. 2001;61(2):78-86.
largely preventable diseases. Proper evalu-
2015;69(1):7-17. 21. Segura A, Boulter S, Clark M, et al. Maintaining
ation and diagnosis of patients and moti- 9. American Dental Association Statement on and improving the oral health of young children.
vation to perform adequate oral hygiene Regular Brushing and Flossing to Help Prevent Pediatrics. 2014;134(6):1224-1229.
Oral Infections. August 22, 2013. Accessed June 22. Watt RG, Listl S, Peres MA, Heilmann A, eds.
and limit sugar intake are critical to their
9, 2020. https://www.ada.org/en/press-room/ Social inequalities in oral health: from evidence
prevention and management. news-releases/2013-archive/august/american- to action. London: International Centre for Oral
Regular patient-centered risk- dental-association-statement-on-regular- Health Inequalities Research & Policy. 2015.
assessment and oral health and hygiene brushing-and-flossing-to-help-prevent-oral 23. Yeh D-Y, Kuo H-C, Yang Y-H, Ho P-S. The
10. Nyvad B, Crielaard W, Mira A, et al. Dental responsiveness of patients’ quality of life to
recommendations should be implemented. caries from a molecular microbiological dental caries treatment—a prospective study.
Oral hygiene education should be rein- perspective. Caries Res. 2013;47(2):89-102. PLoS One. 2016;11(10):e0164707.
forced at regular dental visits and use prac- 11. Kaiser M. How long does the average person 24. Kornman KS, Page RC, Tonetti MS.
brush? Dentistry IQ. Academy of General The host response to the microbial
tical, accessible approaches to allow for Dentistry. September 30, 2014. Accessed April challenge in periodontitis: assembling the
optimal clinical outcomes. 17, 2020. www.dentistryiq.com/articles/2014/09/ players. Periodontol 2000. 1997;(14):33-53.
how-long-does-the-average-person-brush.html 25. Chapple ILC, Van der Weijden F, Doerfer C, et al.
12. Bader HI. Floss or die: implications for dental Primary prevention of periodontitis: managing
REFERENCES professionals. Dent Today. 1998;17(7):76-78, gingivitis. J Clin Periodontol. 2015:42(Suppl
1. National Institute of Dental and Craniofacial
80-82. 16):S71-S76.
Research. Strategic Plan. Mission Statement.
13. 2015-2020 Dietary Guidelines for Americans. 26. Li Y, Lee S, Hujoel P, et al. Prevalence and severity
NIDCR. Accessed June 9, 2020. https://www.nidcr.
Health. Accessed August 7, 2017. https://health. of gingivitis in American adults. Am J Dent.
nih.gov/about-us/strategic-plan/nidcr-mission
gov/dietaryguidelines/2015/ 2010;23(1):9-13.
2. Oral Health Tips. What Can Adults Do to Maintain
14. Saint Louis C. Feeling guilty about not flossing? 27. Löe H. The gingival index, the plaque
Good Oral Health? Centers for Disease Control
Maybe there’s no need. New York Times. August index and the retention index systems. J
and Prevention. Accessed June 9, 2020. https://
2, 2016. Accessed April 17, 2020. https://www. Periodontol. 1967;38(6):610-616.
www.cdc.gov/oralhealth/basics/adult-oral-health/
nytimes.com/2016/08/03/health/flossing-teeth- 28. 2000 Surgeon General’s Report on Oral Health
tips.html
cavities.html in America. National Institute of Dental and
3. Oral Health Objectives for Healthy People 2020.
15. Sambunjak D, Nickerson JW, Poklepovic T, et al. Craniofacial Research. Last reviewed January
Healthy People. Accessed June 9, 2020. https://
Flossing for the management of periodontal 2019. Accessed April 17, 2020. https://www.nidcr.
www.healthypeople.gov/2020/topics-objectives/
diseases and dental caries in adults. Cochrane nih.gov/DataStatistics/SurgeonGeneral/Report/
topic/oral-health/objectives
Database Syst Rev. 2011;(12):CD008829. ExecutiveSummary.htm
4. Brushing your teeth. Mouth Healthy. Accessed
16. Gumpert K. One-fourth of Americans lie to 29. Flemmig TF. Periodontitis. Ann Periodontol.
April 17, 2020. https://www.mouthhealthy.org/en/
dentists about flossing: Survey. Reuters. June 1999;4(1):32-38.
az-topics/b/brushing-your-teeth
23, 2015. Accessed June 9, 2020. https://www. 30. Page RC, Schroeder HE. Pathogenesis of
5. Cho I, Blaser MJ. The human microbiome: at the
reuters.com/article/us-usa-healthcare-flossing/ inflammatory periodontal disease. A summary of
interface of health and disease. Nat Rev Genet.
one-fourth-of-americans-lie-to-dentists-about- current work. Lab Invest. 1976;34(3):235-249.
2012;13(4):260-270.
flossing-survey-idUSKBN0P32BJ20150623 31. Löe H, Anerud A, Boysen H, Morrison E. Natural
6. Lourenço TGB, Heller D, da Silva-Boghossian CM,
17. Southam JD, Soames JV. Dental caries. In: Oral history of periodontal disease in man. Rapid,
et al. Microbial signature profiles of periodontally
Pathology. Oxford University Press; 1993: ch. 2. moderate and no loss of attachment in Sri
healthy and diseased patients. J Clin Periodontol.
18. 48th ORCA Congress. Caries Res. 2001;35(4):265- Lankan laborers 14 to 16 years of age. J Clin
2014;41(11):1027-1036.
316. doi:10.1159/000047468 Periodontol. 1986;13(5):431-440.
8 DentalAcademyOfCE.comD ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
32. Socransky SS, Haffajee AD, Goodson JM, Lindhe 2, 2016. Accessed June 9, 2020. https://www. implications. J Periodontol. 2013;84(4):436-443.
J. New concepts of destructive periodontal nytimes.com/2016/08/03/health/flossing-teeth- 67. Paraskevas S, Van der Weijden GA. A review of
disease. J Clin Periodontol. 1984;11(1):21-32. cavities.html the effects of stannous fluoride on gingivitis. J
33. Jeffcoat MK, Reddy MS. Progression of probing 51. Kressin NR, Boehmer U, Nunn ME, Spiro A 3rd. Clin Periodontol. 2006;33(1):1-13.
attachment loss in adult periodontitis. J Increased preventive practices lead to greater 68. Kazmierczak M, Mather M, Ciancio S, et al. A
Periodontol. 1991;62(3):185-189. tooth retention. J Dent Res. 2003;82(3):223-227. clinical evaluation of anticalculus dentifrices. J
34. Eke PI, Dye BA, Wei L, et al. Prevalence of 52. Biesbrock A, Corby PMA, Bartizek R, et Clin Prev Dent. 1990;12(1):13-17.
periodontitis in adults in the United States: 2009 al. Assessment of treatment responses 69. Oral health care drug products for over-
and 2010. J Dent Res. 2012;91(10):914-920. to dental flossing in twins. J Periodontol. the-counter human use; Antigingivitis/
35. Eke PI, Dye BA, Wei L, et al. Update on 2006;77(8):1386-1391. antiplaque drug products; Establishment
prevalence of periodontitis in adults in 53. Corby PMA, Biesbrock A, Bartizek R, et al. of a monograph; Proposed rules. Food and
the United States: NHANES 2009 to 2012. J Treatment outcomes of dental flossing in Drug Administration. May 29, 2003. Accessed
Periodontol. 2015;86(5):611-622. twins: molecular analysis of the interproximal April 17, 2020. www.fda.gov/downloads/
36. Tonetti MS, Eickholtz P, Loos BG, et al. Principles microflora. J Periodontol. 2008;79(8):1426-1433. Drugs/DevelopmentApprovalProcess/
in prevention of periodontal diseases: Consensus 54. Axelsson P, Nyström B, Lindhe J. The long-term DevelopmentResources/Over-the-
report of Group 1 of the 11th European Workshop effect of a plaque control program on tooth CounterOTCDrugs/StatusofOTCRulemakings/
on Periodontology on Effective Prevention of mortality, caries and periodontal disease in ucm096081.pdf
Periodontal and Peri-Implant Diseases. J Clin adults. Results after 30 years of maintenance. J 70. Lanigan RS. Final report on the safety
Periodontol. 2015;42(Suppl 16):S5-S11. Clin Periodontol. 2004;31(9):749-757. assessment of sodium metaphosphate,
37. Lang NP, Bartold PM. Periodontal health. J 55. Hellstrom MK, Ramberg P, Krok L, et al. The sodium trimetaphosphate, and sodium
Periodontol. 2018;89(Suppl 1):S9-S16. effects of supragingival plaque control on hexametaphosphate. Int J Toxicol. 2001;20(Suppl
38. Chapple ILC, Mealey BL, Van Dyke TE, et al. subgingival microflora in human periodontitis. J 3):75-89.
Periodontal health and gingival diseases Clin Periodontol. 1996;23:934. 71. Triclosan factsheet. Centers for Disease
and conditions on an intact and a reduced 56. Macgregor ID, Balding JW, Regis S. Flossing Control and Prevention. Last reviewed April 7,
periodontium: Consensus report of workgroup 1 behaviour in English adolescents. J Clin 2017. Accessed April 17, 2020. www.cdc.gov/
of the 2017 World Workshop on the Classification Periodontol. 1998;25:291. biomonitoring/Triclosan_FactSheet.html
of Periodontal and Peri-Implant Diseases 57. Kinane DF. The role of interdental cleaning in 72. Triclosan: Report of the Cancer Assessment
and Conditions. J Periodontol. 2018;89(Suppl effective plaque control: need for interdental Review Committee. EPA. January 4, 2008. .
1):S74-S84. cleaning in primary and secondary prevention. Accessed April 17, 2020. www3.epa.gov/
39. Neel EA, Aljabo A, Strange A, et al. In: Lang NP, Ättstrom R, Löe H. Proceedings of pesticides/chem_search/cleared_reviews/
Demineralization–remineralization the European workshop on mechanical plaque csr_PC-054901_4-Jan-08_a.pdf
dynamics in teeth and bone. Int J Nanomed. control: status of the art and science of dental 73. Safety and effectiveness of consumer
2016;11:4743-4763. plaque control, Berne, Switzerland, May 9-12, antiseptics; Topical antimicrobial drug products
40. Van der Weijden GA, Hioe KPK. A systematic 1998. Quintessence. 1998. for over-the-counter human use. Federal
review of the effectiveness of self-performed 58. Bergenholtz A, Olsson A. Efficacy of plaque- Register. September 6, 2016. Accessed June
mechanical plaque removal in adults with removal using interdental brushes and 9, 2020. https://www.federalregister.gov/
gingivitis using a manual toothbrush. J Clin waxed dental floss. Scand J Dent Res. documents/2016/09/06/2016-21337/safety-and-
Periodontol. 2005;32(Suppl 6):214-228. 1984;92(3):198-203. effectiveness-of-consumer-antiseptics-topical-
41. Deery C, Heanue M, Deacon S, et al. The 59. Kiger RD, Nylund K, Feller RP. A comparison antimicrobial-drug-products-for
effectiveness of manual versus powered of proximal plaque removal using floss 74. Pradeep AR, Karvekar S, Nagpal K, et al. Efficacy
toothbrushes for dental health: a systematic and interdental brushes. J Clin Periodontol. of locally delivered 1.2% rosuvastatin gel to
review. J Dent. 2004;32(3):197-211. 1991;18(9):681-684. non-surgical treatment of patients with chronic
42. Van der Weijden GA, Timmerman MF, Nijboer 60. Noorlin I, Watts TLP. A comparison of the efficacy periodontitis: a randomized, placebo-controlled
A, et al. A comparative study of electric and ease of use of dental floss and interdental trial. J Periodontol. 2015;86(6):738-745.
toothbrushes for the effectiveness of plaque brushes in a randomised split mouth trial 75. Ralston D, Carrasco R, Jacobsen PL, Wink C.
removal in relation to toothbrushing duration. J incorporating an assessment of subgingival Comparison of plaque removal capabilities
Clin Periodontol. 1993;20:476-481. plaque. Oral Health Prev Dent. 2007;5(1):13-18. between two dentifrices. J Oral Hyg Health.
43. Bass CC. An effective method of personal 61. Drisko CL. Periodontal self-care: evidence-based 2014;2:157. doi: 10.4172/2332-0702,1000157
oral hygiene; part II. J La State Med Soc. support. Periodontol 2000. 2013;62(1):243-255. 76. Vanni R, Waldner-Tomic NM, Belibasakis GN, et
1954;106(3):100-112. 62. Goyal CR, Lyle DM, Qaquish JG, Schuller R. al. Antibacterial efficacy of a propolis toothpaste
44. Gilson CM, Charbeneau GT, Hill HC. A Comparison of water flosser and interdental and mouthrinse against a supragingival
comparison of physical properties of several soft brush on reduction of gingival bleeding and multispecies biofilm. Oral Health Prev Dent.
toothbrushes. J Mich Dent Assoc. 1969;51:347. plaque: a randomized controlled pilot study. J 2015;13(6):531-535.
45. Macgregor ID, Rugg-Gunn AJ. Toothbrushing Clin Dent. 2016;27(2):61-65. 77. de Camargo Smolarek P, Esmerino LA, Chibinski
duration in 60 uninstructed young 63. Slot DE, Dörfer CE, Van der Weijden GA. The AC, et al. In vitro antimicrobial evaluation of
adults. Community Dent Oral Epidemiol. efficacy of interdental brushes on plaque toothpastes with natural compounds. Eur J Dent.
1985;13(3):121-122. and parameters of periodontal inflammation: 2015;9(4):580-586.
46. Bergström J, Preber H. Tobacco use as a risk a systematic review. Int J Dent Hyg. 78. Namiranian H, Serino G. The effect of toothpaste
factor. J Periodontol. 1994;65(Suppl 5):545-550. 2008;6(4):253-264. containing aloe vera on established gingivitis.
47. Hart TC, Shapira L, Van Dyke TE. Neutrophil 64. Hoenderdos NL, Slot DE, Paraskevas S, Van Swed Dent J. 2012;36(4):179-185.
defects as risk factors for periodontal diseases. J der Weijden GA. The efficacy of woodsticks on 79. Azaripour A, Mahmoodi B, Habibi E, et al.
Periodontol. 1994;65(55):521-529. plaque and gingival inflammation: a systematic Effectiveness of a miswak extract-containing
48. Deacon SA, Glenny A-M, Deery C, et al. Different review. Int J Dent Hyg. 2008;6(4):280-289. toothpaste on gingival inflammation: A
powered toothbrushes for plaque control and 65. Cronin MJ, Dembling WZ, Cugini M, et al. A 30- randomized clinical trial. Int J Dent Hyg.
gingival health. Cochrane Database Syst Rev. day clinical comparison of a novel interdental 2017;15(3):195-202.
2010;(12):CD004971. cleaning device and dental floss in the 80. Brooks JK, Bashirelahi N, Reynolds MA. Charcoal
49. Gjermo P, Flötra L. The plaque removing effect of reduction of plaque and gingivitis. J Clin Dent. and charcoal-based dentifrices: A literature
dental floss and toothpicks a group–comparison 2005;16(2):33-37. review. J Am Dent Assoc. 2017;148(9):661-670.
study. J Periodontal Res. 1969;4(2):170. 66. Task Force on Peri-Implantitis. Peri-implant 81. Haps S, Slot DE, Berchier CE, Van der Weijden GA.
50. Saint Louis C. Feeling guilty about not flossing? mucositis and peri-implantitis: a current The effect of cetylpyridinium chloride-containing
Maybe there’s no need. New York Times. August understanding of their diagnoses and clinical mouth rinses as adjuncts to toothbrushing on
DentalAcademyOfCE.com 9D ENTA L ACA D EM Y OF CON TIN U IN G ED U CATION
plaque and parameters of gingival inflammation: plaque accumulation and gingival inflammation. MARIA L. GEISINGER, DDS,
A systematic review. Int J Dent Hyg. Eur J Dent. 2015;9(2):272-276. MS, is a professor and director
2008;6(4):290-303. 89. Liochev SI. The mechanism of ‘Fenton-like’ of advanced education in
82. Stoeken JE, Paraskevas S, van der Weijden reactions and their importance for biological periodontology in the
GA. The long-term effect of a mouthrinse systems. A biologist’s view. Metal Ions Biol Syst. Department of Periodontology in
containing essential oils on dental plaque and 1999;36:1-39. the University of Alabama at
gingivitis: a systematic review. J Periodontol. 90. Lachapelle J-M, Castel O, Casado AF, Birmingham (UAB) School of
2007;78(7):1218-1228. et al. Antiseptics in the era of bacterial Dentistry. Dr. Geisinger received
83. Sharma N, Charles CH, Lynch MC, et al. resistance: a focus on povidone iodine. Clin her BS in biology from Duke
Adjunctive benefit of an essential oil- Pract. 2013;10(5):579-592. University, her DDS from Columbia University School
containing mouthrinse in reducing plaque 91. Kanagalingam J, Feliciano R, Hah JH, et al. of Dental Medicine, and her MS and Certificate in
and gingivitis in patients who brush and floss Practical use of povidone-iodine antiseptic in the Periodontology and Implantology from the University
regularly: A six-month study. J Am Dent Assoc. maintenance of oral health and in the prevention of Texas Health Science Center at San Antonio. Dr.
2004;135(4):496-504. and treatment of common oropharyngeal Geisinger is a diplomate in the American Board of
84. Eley BM. Antibacterial agents in the control infections. Int J Clin Pract. 2015;69(11):1247-1256. Periodontology. She has served as the president of
of supragingival plaque–a review. Br Dent J. 92. Kensche A, Reich M, Kümmerer K, et the American Academy of Periodontology
1999;186(6):286-296. al. Lipids in preventive dentistry. Clin Oral Foundation and on multiple national and regional
85. Anauate-Netto C, Anido-Anido A, Leegoy HR, et Investig. 2013;17(3):669-685. organized dentistry committees. She currently
al. Randomized, double-blind, placebo-controlled 93. Kuroyama M, Kagawa H, Kitada S, et al. serves as chair of the ADA’s Council on Scientific
clinical trial on the effects of propolis and Exogenous lipoid pneumonia caused by Affairs and as a member of the American Academy
chlorhexidine mouthrinses on gingivitis. Braz repeated sesame oil pulling: a report of two of Periodontology’s Board of Trustees. She has
Dent Sci. 2014;17(1):11-15. cases. BMC Pulm Med. 2015;15:135. authored over 45 peer-reviewed publications and
86. Kilian M, Chapple ILC, Hanig M, et al. The oral 94. Shaikh S, Kumar SM. Beneficial effects of specific her research interests include periodontal and
microbiome–an update for oral healthcare natural substances on oral health. Saudi Med J. systemic disease interaction, implant dentistry in the
professionals. Br Dent J. 2016;221(10):657-666. 2017;38(12):1181-1189. periodontally compromised dentition, and novel
87. Tsourounakis I, Palaiologou-Gallis AA, Stoute D, 95. Jepsen S, Blanco J, Buchalla W, et al. Prevention treatment strategies for oral soft- and hard-tissue
et al. Effects of essential oil and chlorhexidine and control of dental caries and periodontal growth. She lectures nationally and internationally
mouthwashes on gingival fibroblast survival and disease at individual and population level: on topics in periodontology and oral health care.
migration. J Periodontol. 2013;84(8):1211-1220. consensus report of Group 3 of joint EFP/ORCA
88. Ercan N, Erdemir EO, Ozkan SY, Hendek MK. The workshop on the boundaries between caries
comparative effect of propolis in two different and periodontal disease. J Clin Periodontol.
vehicles; mouthwash and chewing gum on 2017;44(Suppl 18):S85-S93.
QUICK ACCES S CO DE 21000
ONLINE COMPLETION
Take this test online for immediate credit. Visit dentalacademyofce.com and sign in. If you have not previously purchased the course, select it from the “Online Courses” listings
and complete your purchase. The exam will then be added to your “Archives” page, where a “Take Exam” link will be provided. Click on this link, complete all questions, and submit your
answers. An immediate grade report will be generated. If you receive a score of 70% or higher, your verification form will be provided immediately for viewing and printing. View and print
forms at any time by visiting the site and returning to your “Archives.”
QUESTIONS
1. The primary etiologic factor for 3. Patient compliance with regular and 5. The 2015-2020 Dietary Guidelines for
both dental caries and periodontal sustained daily use of dental floss America omitted, for the first time
disease is: for interdental cleaning has been since 1979, recommendations for all
A. Dental calculus estimated to be as low as: of the following except:
B. Xerostomia A. 2% C. 15% A. Consumption of fluoridated water
C. Dysbiotic dental plaque biofilm B. 10% D. 25% B. Reduction of sugary food and beverage
D. Tobacco use consumption
4. According to a survey from C. Toothbrushing and flossing as effec-
2. Despite recommendations from the the American Academy of tive methods to reduce the risk of den-
American Dental Association that Periodontology, ___% of individuals tal caries
individuals brush for two minutes state that they would rather perform D. Increasing consumption of vegetables
twice daily, how long does the an unpleasant task, such as filing a and fruits
average individual brush in total tax return or cleaning toilets, than
daily? floss.
A. 15-30 seconds A. 15
B. 45-70 seconds B. 25
C. 60-90 seconds C. 35
D. 120-240 seconds D. 50
10 DentalAcademyOfCE.comQUICK ACCES S CO DE 21000
ONLINE COMPLETION
Take this test online for immediate credit. Visit dentalacademyofce.com and sign in. If you have not previously purchased the course, select it from the “Online Courses” listings
and complete your purchase. The exam will then be added to your “Archives” page, where a “Take Exam” link will be provided. Click on this link, complete all questions, and submit your
answers. An immediate grade report will be generated. If you receive a score of 70% or higher, your verification form will be provided immediately for viewing and printing. View and print
forms at any time by visiting the site and returning to your “Archives.”
QUESTIONS
6. Intraoral bacteria use simple sugars as 11. NHANES III data suggest that 16. It is important to counsel patients
a food source and produce metabolic periodontitis affects an estimated to replace toothbrushes regularly
acids as a part of the process to ___% of US adults. as bristle wear after ___ weeks of
break down those sugars. This A. 27 C. 42 normal use can affect the efficacy of
demineralization is influence by: B. 38 D. 57 plaque removal.
A. Salivary flow A. 4 C. 12
B. Dietary sugar and acid content 12. Patients report that the top B. 9 D. 20
C. Fluoride availability rationale for performing oral
D. All of the above hygiene includes all of the following 17. A meta-analysis suggests that powered
except: toothbrushes were found to reduce
7. Nearly ___ million school hours are A. Preserving systemic health plaque and gingivitis more than
lost each year due to dental-related B. Fresh breath manual toothbrushing in the short
illnesses. C. Attractive smile (0-3 months) and long (> 6 months)
A. 10 C. 51 D. Avoiding disease terms. Powered toothbrushes may
B. 26 D. 80 improve plaque removal in patients
13. Oral hygiene interventions require who struggle to achieve adequate
8. Employed adults lose ___ million reinforcement over time. Patients’ levels of oral hygiene or who have an
work hours each year to dental effectiveness and compliance for increased susceptibility to periodontal
disease. oral hygiene has been shown to diseases or high caries rates.
A. 68 C. 128 decrease after 12 months. A. Both statements are true.
B. 96 D. 164 A. Both statements are true. B. The first statement is true; the second
B. The first statement is true; the second statement is false.
9. Water fluoridation has proven to statement is false. C. The first statement is false; the second
be one of the most cost-effective C. The first statement is false; the second statement is true.
methods for reducing overall caries statement is true. D. Both statements are false.
rates in the population with every D. Both statements are false.
$1 spent on water fluoridation 18. Individuals who floss regularly
returning from___ in decreased 14. ___ of motivational interviewing to demonstrate all of the following
health-care costs within the improve oral home care has/have except:
community. been shown to improve gingival A. Lower levels of caries and gingival
A. $1-$4 bleeding scores and plaque index. inflammation
B. $5-$32 A. One session B. Decreased visible plaque
C. $28-$64 B. Once-weekly sessions over a month C. Decreased caries rates over five years
D. $75-$100 C. Bimonthly sessions D. Altered subgingival flora with decreased
D. Every three-month sessions proportion of T. denticola, P. gingivalis, T.
10. All patients are susceptible to forsythia, P. intermedia, A. actinomycetem-
gingivitis and will develop gingivitis 15. Softer toothbrush bristles are comitans, and S. mutans
within 21 days after cessation of associated with___ plaque removal
oral hygiene measures. 93.9% of subgingivally and interproximally 19. Interdental brushes remove
adults without attachment loss have due to their increased flexibility and ___ plaque interproximally
gingivitis. result in less gingival recession and when compared to floss and
A. Both statements are true. abrasion to oral soft tissues than demonstrated ___ reduction in
B. The first statement is true; the second hard toothbrush bristles. interproximal probing depths and
statement is false. A. Equivalent gingival bleeding.
C. The first statement is false; the second B. Superior A. As much; more C. More; similar
statement is true. C. Inferior B. More; less D. Less; more
D. Both statements are false. D. Excellent
DentalAcademyOfCE.com 11You can also read

















































