Operational Plan 2019/20 - NHS Coventry & Rugby Clinical Commissioning Group NHS Warwickshire North Clinical Commissioning Group - Coventry and ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Operational Plan 2019/20
NHS Coventry & Rugby Clinical Commissioning Group
NHS Warwickshire North Clinical Commissioning Group
Page 1 of 82
Operational Plan 2019/20 Final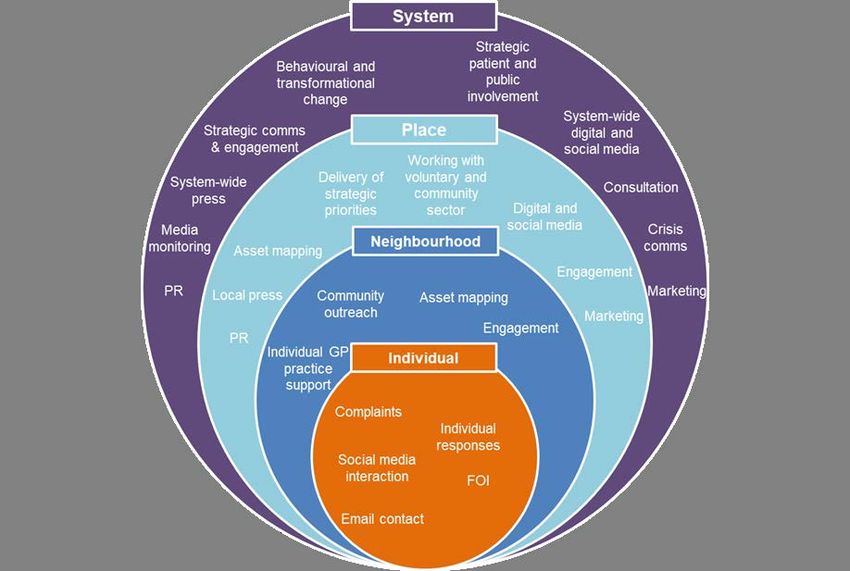
Page 2 of 82 Operational Plan 2019/20 Final
Contents
Section Page
1 About this document 4
2 Our system 7
3 Our place 9
4 Our plan 18
• Assurance & performance 18
• Quality 120
• Finance 21
• Engagement 23
• Risks 24
5 Our response to the NHS Planning guidance for 2019/20 27
• Cancer 27
• Maternity Care 43
• Mental health 47
• Out of Hospital care (OOH) 59
• Personalisation 70
• Planned Care 77
• Urgent & Emergency Care 79
6 Appendix 82
1. Coventry JSNA profile 82
2. Warwickshire JSNA profile 82
Page 3 of 82
Operational Plan 2019/20 FinalSECTION 1: About this document
This document sets out the Warwickshire North and Coventry and Rugby CCGs Operational Plan for 2019/20.
Developed in response to the publication of the NHS Long Term Plan (NHS LTP) and associated NHS Operational
Planning and Contracting Guidance (the NHS OP&CG), this plan recognises that 2019/20 will be a pivotal year for the
two CCGs and the wider Coventry and Warwickshire health and care system. Just as the NHS LTP describes
2019/20 as a ‘transitional year’ for the NHS, this Operational Plan gives a clear signal that 2019/20 will be a year of
transition in Coventry and Warwickshire – one in which the architecture of our system will change and both CCGs and
Providers will redefine their ‘business as usual’ ways of working. All of this with the aim of creating conditions in
which, over the coming five years, real progress is able to be made in transforming the way that health and care
services are commissioned and delivered, resulting in improving outcomes for individuals and populations, so that
over time the people of Coventry and Warwickshire are healthier and more able to live fulfilled lives.
As this Plan will demonstrate, we have strong foundations to build from moving into 2019/20. The NHS LTP describes
a new world of system working, in which, by April 2021, Integrated Care Systems (ICS) cover the whole country.
Section 2 outlines what has already been achieved in 2018/19 in relation to the development of an ICS for Coventry
and Warwickshire and how we will build on this during 2019/20. The formation of the Coventry and Warwickshire
Better Health, Better Care, Better Value (BHBCBV) Partnership in 2016 is recognised as a critical milestone in the
local ICS journey. As a consequence of the experience gained over the last two years through the development and
delivery of the BHBCBV programme, Commissioner and Provider organisations from across the Coventry and
Warwickshire system are firmly of the belief that if we are going to deliver the best possible outcomes for our
population within the resources available to us:
• We cannot keep doing things the way that we have always done them; and
• Greater collaboration between organisations (be that between Commissioners, between Providers or between
Commissioners and Providers) is needed to transform services and manage resources.
The work (both completed and planned) described in Section 2 demonstrates every BHBCBV partner organisation’s
full commitment to accelerating the development of the ICS in 2019/20, driving the transition of our system from its
current form to a new one which both enables and prioritises collaboration.
Section 2 provides an overview of the work streams established within the BHBCBV programme. These are five
transformational work streams (Planned Care, Urgent and Emergency Care, Mental Health and Emotional Wellbeing,
Maternity and Paediatrics and Proactive and Preventative Care) and three enabling work streams (Productivity and
Efficiency, Digital Transformation and Estates). Each work stream has established its priorities for 2019/20 and the
work stream plans will drive the achievement of deliverables identified in the NHS OP&CG. Section 2 also highlights
the work undertaken by the BHBCBV Clinical Design Authority (made up of senior clinicians from across Coventry and
Warwickshire) during 2018/19 to develop a system-wide clinical strategy. The clinical strategy identifies three priority
areas for the local system which are frailty, mental health and musculoskeletal (MSK) services. These are areas
where there is a clear opportunity to deliver improved outcomes for patients and a recognised need to test whether the
combined financial investment being made by the system represents value in relation to the outcomes being
delivered. We are rolling out Place Based profiles as part of our JSNA process. These allow us to dig deeper into the
needs, health inequalities, assets and priorities for our local communities than our city and borough wide profiles
allow. As Place Based profiles are developed these will inform our place based approaches to improving health and
wellbeing and reducing inequalities. We want to ensure that the first chapter of all our work streams is prevention and
reduction in inequalities and this will be overseen by our Proactive and Preventative Care work stream.
As we have already signalled in our commissioning intentions for 2019/20, the future Coventry and Warwickshire ICS
will be a place-based system, made up of four places including South Warwickshire. Section 3 sets out what we
expect to be happening at Place level in 2019/20. Our own experience through the on-going local Out of Hospital
transformation programme and that of other areas nationally, tells us that place will be the level where most service
change will take place in the future ICS, where decisions about how money is spent will be made and where
opportunities to get better value will be identified. As such, place development will continue to be an area of focus in
2019/20. We will again be able to build on the foundation of work completed in 2018/19. Design principles agreed in
January 2019 will provide a framework for the three CCGs to work with providers in each place in a way that will
Page 4 of 82
Operational Plan 2019/20 Finalensure that there is consistency of purpose across the places whilst allowing local variation on the delivery of the
purpose, recognising the need to reflect different populations and provider landscapes in each place.
In line with the NHS LTP and as part of place development, supporting the development of GP networks will also
continue to be a priority in 2019/20. Networks will be the building blocks of the future ICS and much progress has
already been made. We have seven networks in Coventry and three in development in WNCCG and one PCN in
Rugby – however some of these networks are larger than the 50,000 and may be subdivided to reflect the new PCN
contract requirements. Section 3 recaps what has been achieved locally in relation to Network development to date
and what we will be focusing on in 2019/20. We acknowledge that considerable effort and resource will need to be
directed into expanding engagement with our GP and broader general practice workforce during 2019/20 to ensure
that they understand and are confident in the purpose of their participation in both Networks and place. We expect
that the publication of the new national network contract during 2019 will provide additional impetus for this
engagement.
As set out in Sections 2 and 3, both CCGs and Providers will need to devote significant time, resource and energy to
reshaping the architecture of the local system in 2019/20. For CCGs the focus will be on the roadmap to developing a
single commissioning function for Coventry and Warwickshire. This “Strategic Commissioner” will move away from
commissioning volume and activity to commissioning improved outcomes for defined groups of people or populations,
as well as focusing on health inequalities within the population. This commissioning approach will be fundamentally
driven by engagement with patients and the public to understand what outcomes matter most and are meaningful to
them. Whilst the development of the single commissioning function will accelerate the CCG’s ability to act as a
Strategic Commissioner, it is not contingent on it; indeed our commissioning intentions clearly articulate our intent to
act as a Strategic Commissioner as our standard approach in 2019/20. Already we have done this within the local Out
of Hospital and CAMHS (Child and Adolescent Mental Health Services) transformation programmes, which have
delivered two new outcome based contracts.
Section 3 sets out how, acting as a Strategic Commissioner and as the system architecture gradually evolves to that
of a fully functioning ICS, we will focus on a number of ‘developmental’ contracts during 2019/20. Not only will this
enable the CCG and Providers to further develop and embed the competencies and capabilities that will be required
within the future ICS, it will also allow us to drive improvements in quality, outcomes and financial sustainability in the
short to medium term. A number of national and local priorities (including frailty, mental health and MSK services) will
ultimately sit in one the developmental contracts. The developmental contracts should not, however, in themselves be
seen as a solution; what they will enable us to do is put in place the financial and contractual incentives for
transformation to happen at place level.
In Sections 4 and 5 we confirm that we will not be distracted from the need to remain focused on the delivery of our
statutory functions as a CCG (as these relate to performance, quality, finance and engagement) and the continued
delivery of priorities set out in our 2016-2020 strategy ‘Translating our 2020 Vision into Reality’ in the coming year of
transition. Although 2019/20 is the final year of the strategy, the key drivers for it remain relevant and the priorities
that it identifies are aligned to national priorities set out in the NHS LTP and reflected in the NHS OP&CG. The
strategy’s focus on the transformation of out of hospital care is particularly noteworthy. Through the local Out of
Hospital transformation programme, which was a major area of focus within the CCG’s previous two year Operational
Plan, the out of hospital system in Warwickshire North, Coventry and Rugby is already being fundamentally reshaped
in line with the new model described in the NHS LTP. The Transformation Programme also gives us local proof of the
effectiveness of contracts delivered through an outcome based approach in driving integrated, person-centred care.
Our strategy and associated plans will continue to be a focal point for our work in 2019/20 and we remain committed
to finishing what we have started, even as we work on the development of the ICS and begin to pave the way for a
seamless transition to a new system wide strategy.
In order to ensure that our population and stakeholders have maximum clarity regarding our response to the NHS LTP
and NHS OP&CG, in Section 5 we confirm our priorities and deliverables for 2019/20 against the key areas identified
in the NHS OP&CG. We have ensured that there is a clear read across between the priorities identified in Section 5
and the deliverables outlined in sections 4.1 to 4.9 of the NHS OP&CG.
This Operational Plan should be read in conjunction with other published documents including our commissioning
intentions 2019/20, Primary Care strategy and GP workforce strategy. These can be downloaded from:
Page 5 of 82
Operational Plan 2019/20 FinalWarwickshire North CCG: https://www.warwickshirenorthccg.nhs.uk/
Coventry and Rugby CCG: https://www.coventryrugbyccg.nhs.uk/Home
Page 6 of 82
Operational Plan 2019/20 FinalSECTION 2: Our System
The NHS Long Term Plan (LTP) describes 2019/20 as a transition year for the NHS as we move from our traditional,
competitive ways of working towards a more collaborative and integrated approach. During this period, the Coventry
and Warwickshire health and care system, will focus on three key priorities; continue to deliver great care for our
patients; to develop, test and embed the building blocks which allow us to transform the way we commission and
provide services in the future; and to refresh our system Health and Well Being Strategy and develop an associated
five year Transformational Plan that ensures we deliver the best quality and outcomes for our population, within the
resources available.
Priority 1
Throughout 2019/20, the BHBCBV programme will maintain over-arching responsibility for driving system-wide
achievement of all national deliverables including the NHS Constitutional Standards and the targets/milestones
identified in the LTP. Each programme work-stream has already identified the national deliverables for 2019/20
underpinned by a project plan. Where appropriate, these plans are mirrored at organisation and place level to ensure
system alignment. Monthly progress will be monitored and reported through existing governance arrangements up to
the BHBCBV Board.
Alongside the national priorities, senior clinical leaders across the system have worked together as the BHBCBV
Clinical Design Authority (CDA) to produce a Clinical Strategy. This identifies three local priorities that will be our focus
for 2019/20; frailty, musculoskeletal (MSK) and mental health services. These were prioritised following a full review of
all services and were thought to offer the biggest opportunity to demonstrate improved value-based outcomes.
Throughout 2019/20, the CDA will oversee work to develop best practice pathways for these areas and at place, work
will be undertaken to redesign pathways to maximise quality and outcome for minimal cost. To support this we have
invested in a Value Improvement Programme for our clinical leaders, which will be rolled out in 2019/20.
Priority 2
As highlighted in the LTC, significant transformational change is expected over the next five years. As such, in
2019/20 we will have all the necessary foundations in place to commence this transformational change at three levels;
system, place and network. At system level, the BHBCBV programme will be redesigned to better support system-
wide transformational projects and performance such as our ‘single shared-care’ record project, system-wide estates
and digital strategies and a system-wide performance framework.
The Coventry and Warwickshire place forum have identified that our system will be made up of four places; North
Warwickshire, Rugby, Coventry and South Warwickshire. Through our Out of Hospital (OOH) programme we have
already successfully tested our assumption that significant amounts of the service transformation can be delivered in
place and that these defined communities are the most appropriate for our system. To accelerate place development,
we have also produced a set of design principles that support the Strategic Commissioner and the Provider Alliance to
interact with each other across the four places in a consistent manner whilst allowing for local variation of need and
delivery.
In 2019/20 we intend to build on these strong foundations at place and further engage our local populations with
regards to defining the services they want. We will align this with Place JSNA/population health management data to
identify true population need and then utilise this information to define the outcomes required for that defined Place
population.
As part of place development, we will focus significant energy on supporting 100% system-wide coverage of well-
developed GP Networks. These are critical building blocks within our ICS and they will be key partners in identifying
possible place- based opportunities for more out-of-hospital models of care, for the co-location of integrated
community and mental health teams, for supporting the redesign of care pathways and for implementing horizontal
efficiencies such as shared clinical workforce and back office functions.
As well as embedding a process to allow transformational change to accelerate at system, place and network level,
we recognise the need to redesign the way we commission and provide services. For our three CCGs, the focus for
2019/20 will be working together and with the Local Authority to develop of a single Strategic Commissioner function
Page 7 of 82
Operational Plan 2019/20 Finalas identified within their 2019/20 commissioning intentions. Their commissioning approach will move away from the
traditional commissioning of volume and activity style contracts to commissioning improved outcomes for defined
groups, underpinned by robust engagement with patients and the public and population health management data.
This approach has already been successfully demonstrated through the commissioning of the current OOH and
CAMHs contracts. Throughout 2019/20, our Strategic Commissioners will develop and award more outcome-based
contracts initially Maternity and Paediatrics and Planned Care as well as explore the transition to our preferred end-
state of a single ICP contract per Place.
Throughout 2019/20, we will also focus on how we redesign our services to respond to the identified commissioning
outcomes. Both horizontal and vertical Provider Alliance discussions have commenced with 2019/20 priorities already
agreed at system (maternity and paediatrics and cancer) and at Place (frailty, MSK and mental health). System
providers have developed a Provider Alliance/Network (within our STP footprint and across into Hereford and
Worcestershire) with 2019/20 agreements being made as to how they more effectively utilise resource, capacity and
expertise across the systems in selected specialties. Providers are also well embedded in discussions at Place with
regards to ensuring best practice pathways are delivered and clinicians are engaged in redesigning care pathways.
Priority 3
In response to the NHS LTP we will take the opportunity throughout the spring and summer of 2019/20 to work with
our Health and Well Being Boards, our Local Authority colleagues, other partners, our staff and the patients and
populations of Coventry and Warwickshire to refresh our system-wide Health and Well Being Strategy. This will be
underpinned by a revised system Transformation Delivery Plan that outlines the programmes of work we will
undertake over the next five years to deliver the best quality and outcomes for our patients and population within the
resources available.
Page 8 of 82
Operational Plan 2019/20 FinalSECTION 3: Our Place
Setting the CCG Operating Plan within the ICS System Plan:
The NHS Long term plan sets out an intention to continue to develop Integrated Care Systems, building on the
progress the NHS has already made. By April 2021 ICSs will cover the whole country. NHS England described an
integrated care system as an arrangement in which NHS organisations, in partnership with local councils and others
take collective responsibility for planning and commissioning care, managing resources, delivering NHS standards,
and improving the health of the population they serve. (NHS England 2017b in March 2017,).
Coventry and Warwickshire ICS will operate at 3 interdependent levels: Primary Care Networks (PCN) Places
(Coventry, Rugby, Warwickshire North and South Warwickshire) and System (Coventry and Warwickshire).
As a CCG we have developed our operating plan within the context of this emerging ICS architecture, setting out our
CCG ambitions for each of our places within the local ICS system; alongside our CCG strategic work programme
priorities which we anticipate will be delivered across place’s or across the wider STP foot print by undertaking
commissioning activities at the most appropriate foot print, be this at place (or across places) or as a single
commissioner across our Coventry and Warwickshire system.
Consequently our plan represents a transition plan which recognises the statutory accountability of the CCGs and the
population they serve, with clear reference to our commitment to drive forward delivery to achieve the requirements of
the NHS operating plan / performance requirements; and contributing as a system partner in delivering the Coventry
and Warwickshire system plan to deliver improving health outcomes for our populations.
Place:
Coventry and Rugby CCG has two distinct places. Coventry which serves a population of 490,000 with 69 GP
practices and a unitary authority, and Rugby which has a population of 190,000 with 12 GP practices which sits within
the County of Warwickshire.
Warwickshire North CCG is classed as one distinct place which serves a population of 125,000 with 26 GP practices
which sits within the County of Warwickshire. The geography and population profile of each place is reflected in
JSNA’s produced by Public Health (see appendix).
As health commissioners the 3 CCGs have worked together to develop a suit of consistent design principals for Place:
Place design principles
Robust systems and processes in place to in order to understand the needs of the local population
and develop an agreed population health improvement plan that fits with the Health & Wellbeing
Board Strategy;
1 E.g. Integrated IT systems that support a population health management system and then the process and
governance structures which allow clinicians to analyse the data and make decisions about people’s mental and
physical health needs.
Mechanisms to effectively deploy the resources of all public sector organisation in a coordinated
way to meet needs and promote Place based integration;
E.g. We are able to mobilise the education sector to respond to young people’s mental health needs either through
2
partnership working, or more formally risk and gain share agreements across all public sector organisations at
Place, that allow the system to effectively use public money to address need, regardless of which organisation
financially or operationally benefits.
Have in place arrangements that enable ability to respond to system wide outcomes in a way that
is sensitive to place;
3
E.g. Across the system we are all working to reduce obesity, but we can all tackle it in a different way to that of the
other three places as long as we achieve a reduction.
Mechanisms to facilitate joint ownership of demand and cost;
E.g. instead of the CCG commissioning GPs considering how to reduce demand for hip replacements on their own,
4
they do it collectively with the orthopaedic surgeons and both groups take ownership for reducing system cost for
hip replacements.
Page 9 of 82
Operational Plan 2019/20 FinalSets the environment for effective community engagement in improving outcomes and planning;
5 E.g. Engagement with the community is frequent to ensure that services are meeting their needs and that they are
encouraged to take action to improve their own health.
Encourages a collaborative provider market that is supported to innovate, in which there will be a
collective GP and primary care voice;
6
E.g. General practice has the mechanisms in place to be able to speak to the rest of the system in a way that that
transforms service at practice, network and Place level. Other people in Place know who to talk to in primary care.
Clear and visible leadership;
E.g. Identified planning lead to take lead on Place planning and assurance of population health
7 improvement as agreed in the Place plan (in 1 above),
E.g. Identified lead organisation/s that will be accountable for identifying and managing risk for the Place and its
capitated budget set by the strategic commissioner, to deliver population health improvements.
Clear and effective governance arrangements that allow effective decision making at network,
8
place and system levels.
For our CCG ‘place’ is about a move away from operating as individual organisations, towards collective action, with
blended commissioner and provider functions, to achieve efficient, cost effect care, that delivers improved patient
outcomes for our defined place population. The specific activities that will be undertaken at place are currently being
scoped, (and as a membership organisation, we are currently engaging with our member practices), in recognition that
some of the CCG commissioning activities are likely to transition to place within a future ICS arrangement.
Over the 2019/2020 operating plan period, each of our places will establish governance arrangements and embed
clear reporting arrangements that connect our PCNs, Place Partnership Board, wider Integrated Care Partnership
forum, and Provider Alliance, and Strategic Commissioner to achieve a fully functioning and mature ICS. At a place
our focus will be on driving the local delivery system, engage meaningfully with local partners, coordinating and
segmenting care delivery (uninhibited by organisational boundaries) through multi-disciplinary / integrated workforce,
to deliver our operating plan and system plan priorities, contribute towards long term health plan reforms, and in so
doing achieve improved population health outcomes.
Primary Care Networks and Out of Hospital Care:
General Practice is considered to be the foundation of the health service now and in the future; with care continuing to
be based around general practice holding primary responsibility for a registered patient list. However, it is widely
accepted that, demographic growth, aging population, more people living with chronic conditions, comorbidities and
complex care needs are resulting in increased demand on general practice. This is further exacerbated by increased
patient expectations characterised by demand for flexible convenient access to care, the impact of wider social
determinants of health particularly for our most deprived population groups, provide a compelling case that our
existing fragmented care system is unsustainable. It is in this context that we are seeking to build the resilience and
sustainability of general practice, whilst transforming out of hospital care within each of our Places.
Our ambition is to provide each of our citizens within each place, with a primary care and out of hospital offer, that
includes support and tolls to facilitate and promote proactive preventative and self-care, access to anticipatory and
same day urgent care, rapid response and new standardised models of care for key cohort groups to address
variation and inequality.
A fundamental building block for delivering and co-ordinating this care ambition within each of our places will be the
development of our Primary Care Networks around which out of hospital care will be organised. NHSE describes the
function of a PCN as ‘Enabling the provision of proactive, accessible, coordinated and more integrated primary and
community care improving outcomes for patients; formed around natural communities based on GP registered lists,
often serving populations of around 30,000 to 50,000.
Within each of our places we have already made significant headway with regard to developing PCNs. Our operating
plan appendix now sets out our intention to mobilise a support offer that will enable each of our PCNs to develop and
mature, so that they provide the personal care valued by both patients and GPs, achieve increased resilience through
deeper collaboration between practices and others in the local health (community and primary care) and social care
system, and provide the foundation for delivering sustainable care within each of our Places now and in the future.
Page 10 of 82
Operational Plan 2019/20 FinalWe will continue to build on the progress we have made in Out Of Hospital care; we already have an outcome based
contract for OOH service in place across our CCG, with Place Based Teams already mobilised in each of our Places.
Over the coming year we will utilise PCN’s as a vehicle to provide re-designed community-based and home-based
services, in partnership with social care, the voluntary and community sector.
Over the coming year we will further strengthen risk stratification and MDT case management, with Place Based
Teams and general practice working alongside other local partners to provide proactive care to people at risk of
becoming acutely unwell, as well as urgent rapid response capacity for individuals with escalating needs, to avoid
hospital admission where is safe to do so. Our PCNs will provide a local focal point for partnership collaboration and
will be the delivery vehicle for holistic integrated care delivered by a range of providers including voluntary sector and
primary care.
As a CCG we are committed to continued investment in primary care as set out in the spending review and
underpinning the commitments in the General Practice Forward View. This investment will focus on resilience and
sustainability at a practice level and transform the care and services provided through PCNs for their local population.
We have already made considerable progress in achieving 100% coverage of GP practices in PCN’s well ahead of
the national 30 June 2019 target. We will now work with our PCN’s to support their journey through the NHSE maturity
matrix and to work with PCN’s to identify and deliver on population health priorities, including focused action to
manage demand, reduce variation, and extend the range of services available in out of hospital settings.
The CCG is already in the process of refreshing its primary care strategy, which will be set within an overarching
system strategy by autumn 2019. We will build on existing engagement with general practice, through our
relationships with the LMC, GP federations and PCN to co-produce our refreshed strategy and to develop credible
plans to mobilise and implement our plans.
We already have a PCN development plan for each of our places, which will now be further developed in response to
the NHS Long Term Plan. By June 2019 we will confirm our PCN local support and investment offer, and work with
PCN leads to agree transformation priorities, local workforce plans and support requirements to enable our PCNs to
mature.
As a CCG with delegated primary medical care commissioning responsibilities we have set out plans for internal
audits to provide assurance that our statutory functions are being discharged effectively. The scope of the planed
audit will be:
• primary care commissioning and procurement activities;
• primary care contract and performance management;
• primary care financial management; and
• governance of all primary medical care delivery.
We will work with Public Health and CCG intelligence teams to further enhance existing data packs and
neighbourhood JSNA profiles that are currently available to PCNs, so that they have the data analytics for population
segmentation and risk stratification, according to a national data set, complemented with local data indicator
requirements, so that PCNs understand in depth their populations’ needs for symptomatic and prevention
programmes including screening and immunisation services.
General Practice Workforce:
In order to achieve sustainable general practice and an extended Out of Hospital offer for our patients, we have
developed a credible work force strategy, premised on the principal that: “A growing and ageing population, with
complex, multiple conditions, means that personal and population-orientated primary care is central to our local health
system, and the belief that, “if general practice fails, the whole NHS fails”.
As a CCG we are clear that some work force challenges will require system wide action whilst others will be specific to
place. It is in this context that we have led on the development of The Coventry and Warwickshire Primary Care
Workforce Framework – Our Journey to Sustainable Primary Care Workforce. This document sets out the workforce
implications, challenges, and opportunities we face as a local system, if we are to achieve sustainable transformed
general practice, which is at the centre of new models of out of hospital care.
As a system (STP) we currently anticipate a GP workforce gap of 180 WTE. Our Primary Care Workforce Framework
outlines the strategic objectives to address this gap and details the actions that we will take collectively across our
Page 11 of 82
Operational Plan 2019/20 Finalhealth system to deliver and support a resilient primary care workforce, working as part of a multi-disciplinary team
working together to deliver out of hospital care, organised around general practice lists.
In summary our latest work force trajectory plans to deliver:
• 5.4% increase in GPs
• 7.1% increase in nurses
• 8.3% increase in direct patient care roles
• 324.1% increase in Clinical Pharmacists
As a CCG we are committed to working at a system level through the LWAB, STP work stream and our Primary Care
GPFV workforce sub group; to ensure we have credible plans to meet the projected work force and skill mix gaps. As
a CCG we will focus on:
I. Stabilising current primary care workforce – with recruitment and retention activities
II. Putting in place the foundations for a more robust approach to workforce planning, so we have
workforce succession plans in place, encourage carer development and on-going professional development
and training.
III. Investing in the development of the wider primary care workforce – encouraging new roles to expand the
general practice team skill Mix, development of portfolio roles and extended GP roles, ensuring staff are
empowered to work to their clinical competence.
IV. Supporting the continuing development of primary care networks – to encourage sharing of resources,
skill mix, peer support, mentoring, vital for a resilient workforce.
The key workforce initiatives that we will take forward during this operating plan period reflect the planning guidance
requirements for providers in respect to action focused on, work force supply and retention challenges, move towards
establishing bank first temporary staffing model, workforce transformation encouraging new roles, attracting and
retaining trainees. The specific initiatives we will implement during this operating planning period include:
Local GP Retention scheme and promotion of HEE scheme
Recruitment campaign across all areas of PC
Encouraging practices to become training practices and offer training placements and ‘Taster’ clinical
sessions in local practices.
GP Mentor Development programme
Workforce survey and succession planning
General Practice staff bank/network development
Development of Portfolio GPs with community and acute providers
Clinical Pharmacists deployed in general practice
Leadership development programme for primary care
HCA Training
Nurse prescribing training
Nurse Associate training
Nurse Mentorship
We will continue to work closely with NHSE and our local capacity planners to ensure that all our member practices
are aware of the workforce implications associated with EU Exit and through our localities teams, Practice Managers
Forums, members meetings and PCN’s work to minimise any potential resilience risk in general practice.
General Practice Digital Transformation:
As a CCG we have identified 6 strategic priorities that will drive our GPIT work programme during this operational plan
period:
IT infrastructure and digital solutions that reduce general practice work load and optimise efficiency
Increase timely and convenient access to general practice
IT enabled care co-ordination and care planning to support multidisciplinary working across locations and
settings.
Page 12 of 82
Operational Plan 2019/20 Final Respond to GP estate utilisation pressures releasing space for clinical capacity, and optimising extended
access
Promoting and supporting self-care
Enhance quality and safety – shared access to full patient records, remote access to records
We have an established GPIT work programme with a refreshed governance and reporting structure that connects our
local GPIT working group with the STP Digital Transformation Board at a system level, so that at each place our
local GPIT working group (which includes GP clinical representation and practice manager representation), as the
end user shape our IT programme and drive achievement of our strategic digital transformation priorities; with a
detailed delivery plan setting out the specific range of initiatives that will be implemented during this operational
planning period through four focused delivery work streams summarised below:
1. Net-work infrastructure improvements - such as increased band width HSCN procurement to support
2. Hardware refresh – Updating GPTI infrastructure such as PC’s and sever cabinets and WIFI speed
3. Software refresh – Updating windows 10, Cyber security, improvements to Doc Man.
4. GPIT enabled productive general practice – such as digital dictation, single sign on, two way text
messaging, on line consultations, self-check-in and digitisation and summarisation of patient records, on line
services such as prescription re ordering, on line consultations, telephone triage, on line booking, access to
shared records, and access to self-care apps.
Our Digital work program reflects the GPIT Operating Model ‘Securing Excellence in GPIT Service and the 2019/18
addendum. We will assess the impact of our GPIT work programme using the national Primary Care Digital Maturity
Assessment.
Our Plan – Commissioning Intention Priorities – summary Warwickshire North and Coventry and Rugby CCGs:
Primary Care
• Enhance the resilience and sustainability of general practice by working with member practices to maximise
opportunities available through the General Practice Forward View to, embed high impact actions, adopt new
ways of working eg IT solutions, and actively encouraging general practice to be part of a local primary care
network (Clusters).
• Encourage GPs to proactively engage with the development of the Out of Hospital model ( MDT’s and Risk
Stratification )
• Work towards having a full coverage of GP extended hours
• To continue working with GP practices in developing flexible, timely access to general practice, as the
foundation for our local integrated care system.
Out of Hospital
• Improve the quality of life for people with long term conditions
• Identify people at risk of ill health or hospital admission who are ‘frail’
• Better coordinate the care of people with complex problems via joined up hospital and community services
Maternity and Paediatrics
• To reduce the numbers of stillbirths and neonatal deaths by 20% in 2021 and 50% in 2025
• Achieve 35% of women receiving continuity of carer during pregnancy (by March 2020)
• Increase access to specialist perinatal mental health services
• Continue working in a multi-disciplinary way across the Local Maternity System (LMS)
Urgent Care
• To provide better, clearer and easier-to-access alternatives to A&E,
• Provide holistic support service for frequent A&E attenders to help address their non-clinical needs
• To develop and implement plans to ensure urgent treatment centres meet the national specification standards
for integrated urgent care
Planned Care
• Deliver reduction in avoidable demand for elective care by tackling variations in referrals and providing referral
advice to GPs
• Creation of redesigned and efficient hospital pathways, avoiding duplication and unnecessary hospital visits
• To support patients to live well with cancer through the implementation of the Macmillan recovery package
Page 13 of 82
Operational Plan 2019/20 Final• To increase knowledge of the benefits of cancer screening across all population groups
• Patients with diabetes receive the right support in accessing the right education and self-care resources to
self-manage their condition and live well
• Review phlebotomy provision in Rugby
Mental Health
• Increase dementia diagnosis rate
• Increase number of people accessing talking therapies
• Improves services for people experiencing first episode of psychosis.
• Reduction in out of area mental health and learning disability placements
• Improve the system’s response for children and young people in crisis.
• Continue to reduce hospitalisation of people with a learning disability and/or autism.
Self-Care
An overarching theme for the 2019/20 localised commissioning intentions will be Self-care. Patients need to be
provided with the necessary skills and education to help them better manage their own condition. Improved
partnerships and collaborative working will contribute to:
• Strengthening self-care and education provision for our patients
• Continue to strengthen our partnership working with Public Health to promote healthy lifestyles
• Improve our population access to information to support them to self-care, and access life style services, local
community assets through effective sign posting and navigation support.
• Develop in partnership with the Local Authority a sustainable social prescribing offer that addresses the social
determinant of health and diverts non clinical demand appropriately.
• Multi-disciplinary working with community pharmacists, secondary, primary care diabetes services
• Improved investment into local diabetes services
Page 14 of 82
Operational Plan 2019/20 FinalKey Focus Areas for 2019/20 Commissioning Intentions (in reference to JSNA priority areas and key
deliverables from the NHS operating Plan)
JSNA Priority WN Cov Rugby Operating Plan Priority
Mental Health Improvement in diagnosis for people with Dementia diagnosis rate to be delivered at / maintained at
dementia. 67% of prevalence
Improvement in quality of life for people Maintain delivery of access target for IAPT ( 19% of
with a mental illness prevalence in 2019/20)
Maintain 2 week standard for being seen in early
intervention for Psychosis
Reduction in Out of Area placements
Reducing Self Harm in young people in Further develop crises response for Children and young
particular including building resilience people and fully implement a ‘CAMHs 3.5 service’ model
Cancer Reduction in under 75’s mortality rates Ensure all eight waiting time standards are met, including
from Cancer by supporting the following: the 62 day referral –to-treatment cancer standard.
• Halt rise of obesity in children
and reduction in adults who are
obese
• Reduction in smoking in adults
• Increase in physical activity
• Increase screening uptake
• Reduce inequality of screening
uptake
Cardiovascular Reduction in under 75’s mortality rates
Disease from Cardiovascular Disease (CVD)
Increase in Health Check uptake
Children & Reducing Teenage Pregnancy rates Deliver improvements in safety towards the 2020 ambition
Young People to reduce stillbirths, neonatal deaths, maternal death and
and Maternity Vulnerable Children (including LAC) brain injuries by 20 and by 50% in 2025
Improving levels of educational attainment Increase the number of women receiving continuity of the
and employment person caring for them during pregnancy
Reducing higher rates of child mortality Continue to increase access to specialist perinatal mental
health services
Reducing higher rates of 0-4 years A&E
attendances
Reducing higher rates of self-harm related
hospital admissions for 10-24 yr olds
Reducing higher rates of admissions due
to substance misuse amongst those aged
15-24 years
Reducing higher rates of under 18
conceptions
Lower rates of breastfeeding at 6-8 weeks
Physical Reducing obesity, improving diet and
wellbeing physical activity
Reducing higher rates of smoking in those
aged 35 years +
Reducing levels of substance misuse –
alcohol and smoking
Reducing levels of infectious diseases
including HIV, TB and increasing
immunisation rates
Planned Care Reducing higher rates of hip fractures in Meet and maintain planned care referral to treatment
those aged 60 years + waiting time standards
Deliver reduction in avoidable demand for elective care by
tackling variations in in referrals and providing advice first
options for primary care
Creation of redesigned and efficient hospital pathways,
avoiding duplication and unnecessary hospital visits
Page 15 of 82
Operational Plan 2019/20 FinalJSNA Priority WN Cov Rugby Operating Plan Priority
Expanding cancer screening uptake – focus on bowel,
breast and cervical cancer
Primary Care Providing extended access to GP services, including at
evenings and weekends, for 100% of the population
Delivering their contribution to the workforce commitment
to have an extra 5,000 Doctors and 5,000 other staff
working in primary care
Ensuring every practice implements at least two of the
high impact ‘time to care’ actions
Actively encourage every practice to be part of a local
primary care network
Urgent and Higher excess winter mortality Deliver national performance targets for A&E and other
Emergency urgent care targets
Care
Deliver integrated urgent care services with simple access
for patients
Standardise Urgent Treatment Centres in line with
national standards
Transforming Continue to reduce inappropriate hospitalisation of people
Care for with a learning disability, autism or both
people with
Learning
Disabilities
Prevention and Health Inequalities
Coventry and Warwickshire face complex health and wellbeing challenges and inequalities across our geography.
Healthy life expectancy and many of our health outcomes mirror patterns of deprivation across the region, generally
with worse outcomes affecting the north east of Coventry and the Nuneaton and Bedworth areas of North
Warwickshire. These patterns mean that certain areas may need greater resource to improve health outcomes than
others. Coventry has an ethnically diverse population and our approaches and interventions need to be tailored to
reflect this.
The two Health and Wellbeing Boards (HWB) for Coventry and Warwickshire are meeting on a regular basis as the
Place Forum to work on collective system challenges. As a key organisational member of the HWBs and Place Forum
we have signed up to the Coventry and Warwickshire Health & Wellbeing Concordat and system design. These
outline our principles and ways of working to prioritise prevention, strengthen our communities, coordinate our
services and share responsibility across organisations and partnerships. We have agreed system level priorities for a
Coventry and Warwickshire wide Year of Wellbeing 2019; celebrating and sharing good practice, improving physical
activity, tackling social isolation and promoting workplace wellbeing. Both Coventry and Warwickshire local authorities
are leading on Place Based Joint Strategic Needs Assessments, helping us to better understand the needs and
assets of our local communities engage with local communities and provide evidence to inform our commissioning
intentions.
The coming years offer great opportunities for improving health and wellbeing through physical activity, sports and the
arts. Coventry is European City of Sport 2019, City of Culture 2021 and Birmingham and the wider region will host the
Commonwealth Games in 2022.
The Marmot programme approach emphasises the need for a broader view of health inequalities, recognising our
need to influence wider determinants of health such as housing and employment, take a life course approach
promoting the best start in life through our maternity and paediatrics work programme and the need for a proportionate
universalism approach to our resources with greater emphasis on those with greater needs. We work to ensure these
principles are at the heart of our commissioning and partnership approach.
We know that alcohol, smoking, obesity, inactivity and many more issues impact on the health and wellbeing of our
population, increasing the risk of long term conditions and early preventable death. Our local Public Health teams
Page 16 of 82
Operational Plan 2019/20 Finalcommission a range of services and programmes that can support people to live well, including healthy lifestyles,
sexual health, drug and alcohol services and affordable warmth programmes. We will work to ensure that our
pathways and services link in to these, giving brief advice, signposting and referring as appropriate. Health checks are
a great opportunity to identify and respond to lifestyles risks, cardiovascular disease risk and pre-diabetes. The
National Diabetes Prevention Programme (NDPP) started in Coventry and Warwickshire in April 2018 and we will
continue to roll this out across the region as the programme expands. Where our primary care networks and wider
NHS partner organisations deliver or contribute to these services we will support improvements in uptake and delivery
through our partnerships and contractual processes.
Long term conditions often represent the onset of regular contact with health services for people and impact on quality
of life and healthy life expectancy. In addition to the NDPP we are actively working to improve our offer for people with
diabetes, strengthening our self-care and education offer and improving delivery of care and outcomes across
primary, community and secondary care pathways. We recognise the importance of supporting prevention and better
outcomes for people with cancer through improving uptake of screening programmes, improving early diagnosis rates
and streamlining site specific pathways. We are actively working to improve in these areas and have created a
network of cancer champions and strengthened our approach to the promotion of bowel and cervical screening. We
are working to improve our identification and treatment of atrial fibrillation and wider cardiovascular disease risks. Our
out of hospital transformation programme for 2019 onwards includes work to strengthen our community pathways for
heart failure and respiratory disease. We know that people with severe and enduring mental illness and learning
disabilities are disproportionately affected by lifestyles risks and poor health outcomes and are actively working to
ensure that they have good access to physical health checks and appropriate risk reduction and management.
We are working with our communities and partners to promote strong resilient communities and networks influencing
how and when people access our services. We are strengthening our links to community pharmacies recognising the
role they can play in self-care and prevention. We are working through our primary care networks, out of hospital
transformation programme and voluntary and community sector partners to strengthen our approach to healthy ageing
and frailty including approaches such as social prescribing, navigation and buddying to recognise the wider
contributors to health and wellbeing and help people engage with support beyond formal services.
Page 17 of 82
Operational Plan 2019/20 FinalSECTION 4: Our Plan
Assurance & Performance
The NHS Long Term Plan 2019 highlights the key priorities that are fundamental to Coventry & Rugby CCG and
Warwickshire North CCG to achieving further progress in the provision of high quality care for its residents, and there
are several important performance measures that are used to demonstrate progress through the year, covering each
individual area of care.
Emergency Care
The two CCGs will work to ensure that both Coventry and Warwickshire University Hospitals NHS Trust (UHCW) and
the George Eliot NHS Trust (GEH), will move to a comprehensive model of Same Day Emergency Care (SDEC)
operating at least 12 hours a day, seven days a week by September 2019. This will ensure that the proportion of acute
admissions discharged on the day of attendance increases from around a fifth to a third of all patients.
In addition both hospitals will ensure that by December 2019 their current frailty services are in operation for at least
70 hours per week, so that such patients can be assessed, treated and supported by skilled multidisciplinary teams
delivering comprehensive geriatric assessments in A&E or care of the elderly receiving wards.
Both CCGs are working with providers on the redesign of urgent care services outside main A&Es, to designate
community based services as Urgent Treatment Centres by December 2019, this simplifies the offer for patients and
adds additional services into previous minor injury centres, WICs so that less severe conditions can be dealt with
more quickly away from the main A&E, with access to a range of diagnostics and operated by a multi-disciplinary team
and being open at least 12 hours a day. One key performance measure will be the ability to book appointments to this
service directly from the patient contacting NHS 111, doing so helps remove uncertainty by the patient as they know
they are expected and have a time for their appointment.
Across Coventry and Warwickshire we have seen the numbers of delayed transfers of care in acute hospitals reduce
by over 40% during 2018-19, which has had the effect of freeing up the equivalent of 67 acute medical beds, the
CCGs have agreed through the Health and Well Being Boards (HWBs) how to sustain these reductions in (DToC)
rates through 2019-20.
Care Uk who provide NHS 111 services for the West Midlands and therefore for our residents, have in year increased
the proportion of calls with a clinical assessment to over 50%, this improvement will be sustained in 2019-20, and we
will work to enable patients to be directly book patients triaged by the service into a face-to-face appointment where
needed.
During 2019-20 there will be a national clinical standards review that will develop new ways to focus on patients with
the most serious illness and injury, and indicate new clinical standards to be measured, likely to be in place by
October 2019. Until the review is completed the existing NHS Constitution standards remain in force, namely that 95%
of patients attending A&E need to be seen, treated and discharged within 4 hours. This is a measure where, as
Coventry and Warwickshire we have seen real improvements in 2018-19 over the previous year, and expect to see
further improvements in the first half of 2019-20.
Elective Care
Referral to treatment times RTT have shown significant improvement during 2018-19, and both CCGs are committed
to sustaining this improvement into 2019-20, and we will continue to provide patients with a wide choice of options for
quick access to elective care, including promoting the choice of patients via e-Referral service to include referral to
providers with the shortest waiting times. This will include agreeing options for patients who have been waiting six
months or longer being contacted by the provider on whose waiting list they appear, to be given the option of faster
treatment at an alternative provider.
Page 18 of 82
Operational Plan 2019/20 FinalWe have worked hard during 2018-19 to reduce very long waits for treatment to ensure that no-one waits more than
52 weeks for treatment going into 2019-20 and this position will be sustained, through the whole of 2019-20.
The CCGs and providers (UHCW & GEH) have been working jointly through 2018-19 on transformation programmes
that help to reduce cancellations and non-attendances, as well as looking for opportunities to deliver care differently
through the use of new technologies, such as increasing virtual appointments by phone and/or Skype like services, or
removing the need for follow up appointments altogether, or through the development of direct access services such
as MSK First Contact Practitioners; these will all be developed further in 2019-20.
Part of improving the patients experience and reducing unnecessary waits is the delivery of shorter waiting times for
access to diagnostic tests, the standard is that no more than 1% of patients should wait more than six weeks for a
diagnostic test, this was met in 2018-19, for example that last monthly information showed that for Coventry & Rugby
CCG only 0.1% (7 patients) were waiting more than 6 weeks, and that Warwickshire North CCG had no one waiting
over 6 weeks, this was against a national position of 2.4% waiting over 6 weeks.
Cancer treatment
Both CCGs see that the delivery of all eight clinically set cancer waiting times standards remain an absolute priority,
with most of these targets being met regularly on a monthly basis through 2018-19 these targets are:
• 93% of patients have first outpatient attendance within 2 weeks of being referred with suspected cancer.
• 93% of patients with breast symptoms have their first hospital assessment within a maximum of two weeks.
• 96% of patients wait no more than one month (31 days) for their first definitive treatment, from the date a
decision to treat is made, for all cancers.
• 94% of patients wait no more than one month (31 days) for subsequent treatment, where the treatment is
surgery.
• 98% of patients wait no more than one month (31 days) for subsequent treatment, where the treatment is drug
treatment.
• 94% of patients wait no more than one month (31 days) for subsequent treatment, where the treatment is
radiotherapy.
• 85% of patients receiving an urgent referral for suspected cancer should wait no more than two month (62
days) for their first definitive treatment, for all cancers.
• 90% of patients receiving an urgent referral from NHS cancer screening programmes should wait no more
than two months (62 days) for their first definitive treatment.
Mental Health
The CCGs already spend more than their indicative spending target for Mental Health, but intend to use the extra
resources outlined in the NHS Plan to deliver improved services such as community mental health teams, enhanced
crisis services for adults, children and young people, and perinatal mental health services.
Key deliverables are:
• By March 2020 Improving Access to Psychological Services (IAPTs) should be provided for at least 22% of
people with anxiety disorders and depression.
• At least 50% of people who complete IAPT treatment should recover.
• At least 75% of people referred to IAPT programme should begin treatment within 6 weeks of referral.
• At least 95% of people referred to IAPT programme should begin treatment within 18 weeks of referral.
• At least two thirds of people with dementia, aged over 65 should receive a formal diagnosis.
• At least 56% of people aged 14-65 experiencing their first episode of psychosis should start treatment within
two weeks.
• At least 34% of children and young people with a diagnosable mental health condition receive treatment from
an NHS-funded community mental health service.
• At least 60% of people with a severe mental illness should receive a full annual physical check-up.
Page 19 of 82
Operational Plan 2019/20 FinalYou can also read