CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CalAIM and Health Data Sharing:
A Road Map for Effective Implementation
of Enhanced Care Management and
In Lieu of Services
MAY 2021
AUTHORS
Jonah Frohlich, Kevin McAvey, and Jonathan DiBello
Manatt Health StrategiesContents
About the Authors 3 Executive Summary
This paper was authored by the following team
10 CalAIM ECM and ILOS Background
of individuals at Manatt Health Strategies:
Jonah Frohlich, MPH, managing direc- 12 Methodology
tor; Kevin McAvey, MA, MPP, director; and
Jonathan DiBello, MPH, consultant. Manatt 12 ECM and ILOS Program Data Functions
Health Strategies is a consulting subsidiary 1. ECM Member Identification, Review, and Authorization
of Manatt, Phelps & Phillips, and combines 2. ECM Assignment and Member Engagement
legal excellence, firsthand experience in
3. ECM Care Plan Development, Sharing, and Use
shaping public policy, strategy insight, and
deep analytic capabilities to provide pro- 4. ECM Care Coordination and Referral Management
fessional services to the full range of health
5. ECM and ILOS Billing and Encounter Reporting Practices
industry players.
6. ECM and ILOS Quality Measure and Performance
Reporting
About the Foundation
7. ILOS Needs Assessment and Referral Management
The California Health Care Foundation is
dedicated to advancing meaningful, measur- 20 Implementation Road Map
able improvements in the way the health care
1. Legal and Regulatory Alignment for Data Exchange
delivery system provides care to the people of
California, particularly those with low incomes 2. Statewide Infrastructure for Data Exchange
and those whose needs are not well served 3. Care Management, Shared Care Plans, and Assessments
by the status quo. We work to ensure that
4. Community Resource Closed-Loop Referrals for Social
people have access to the care they need,
and Human Services
when they need it, at a price they can afford.
5. Performance Reporting and ECM and ILOS Billing
CHCF informs policymakers and industry
38 Funding Considerations
leaders, invests in ideas and innovations,
and connects with changemakers to create 40 Appendices
a more responsive, patient-centered health A. Interviewees, by Organization
care system.
B. Advisory Committee Members, by Organization
C. Glossary of Abbreviations
44 Endnotes
California Health Care Foundation www.chcf.org 2Executive Summary
I
n 2022, the California Department of Health Care The ECM and ILOS programs will engage a broad
Services (DHCS) will launch an ambitious and inno- set of MCPs, providers, county agencies, and com-
vative program designed to address the complex munity-based organizations (CBOs). Many of these
physical, behavioral, and social needs of Medi-Cal’s organizations, especially CBOs, do not currently inter-
most vulnerable members. The California Advancing act extensively with the health care system and have
and Innovating Medi-Cal (CalAIM) program will build limited information technology capacity. Nevertheless,
upon the plan-based Health Homes Program (HHP) their participation in the program and ability to share
and county-based Whole Person Care (WPC) pilots and use administrative, health, and social service
that use whole-person care approaches to address information will be vital in carrying out ECM and ILOS
underlying social determinants of health (SDOH). program functions including:
CalAIM envisions enhanced coordination, integra-
tion, and information exchange among managed care $ ECM member identification, review, and autho-
plans (MCPs); physical, behavioral, community-based, rization, where MCPs will identify target ECM
and social service providers; and county agencies by populations by compiling and analyzing data and
establishing new benefits and services including: information received from counties, providers,
members, and others.
$ Enhanced Care Management (ECM) benefit,
$ ECM assignment and member engagement,
which will provide intensive whole-person care
where MCPs will assign members to an ECM
management and coordination to address the
provider based on their previous provider relation-
clinical and nonclinical needs of Medi-Cal mem-
ships, health needs, and known preferences, and
bers with complex needs. MCPs will administer
ECM providers will use available information to
and oversee ECM benefits, identifying members in
reach and engage members into the ECM benefit.
each of the ECM target populations and assigning
them to “ECM providers” who will be responsible $ ECM care plan development, sharing, and use,
for conducting outreach and for coordinating and where ECM providers will develop care plans using
managing care across a broad spectrum of physi- data acquired from the MCP, the member, and
cal, behavioral, and social service providers. ECM other sources, and make the care plan available for
services will be community-based, with high-touch, use by a member’s care team.
on-the-ground, face-to-face, and frequent interac-
$ ECM care coordination and referral management,
tions between members and ECM providers.
where ECM providers will support coordinated and
transitional care, and engage MCPs’ referral net-
$ In Lieu of Services (ILOS), which are cost-effective,
work for community and social services, including
health-supporting services that may be substituted
ILOS.
for existing State Plan–covered services to reduce
hospitalization and institutionalization, reduce cost, $ ECM and ILOS billing and encounter reporting
and address underlying drivers of poor health. practices, where ECM and ILOS providers will
DHCS will allow 14 ILOS categories, including record and report services rendered to MCPs, and
housing transition and navigation services, respite MCPs will report complete and accurate encoun-
care, day habilitation programs, and nursing facil- ters of all services provided by contracted ECM and
ity transition support to assisted living facilities or ILOS providers to DHCS.
a home. MCPs may choose which ILOS to cover, in
which counties, and to which members.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 3$ ECM and ILOS quality measure and performance road map recommendations address three categories
reporting, where MCPs will report DHCS-specified of data sharing barriers and the steps necessary to
quality and performance metrics to demonstrate mitigate them, including:
ECM and ILOS program impact on member health,
$ Regulations and policies to facilitate safe and
well-being, and costs.
secure information sharing
$ ILOS needs assessment and referral manage-
$ Technical infrastructure and standards to support
ment, where MCPs and ECM and ILOS providers
the efficient collection, exchange, and use of mem-
will identify members requiring ILOS benefits, and
ber information
MCPs, primary care physicians, or ECM providers
will connect members to ILOS through a closed- $ Financing, contracting, and operations, where
loop referral process. aligning incentives, contracting, and tactics is cru-
cial to institutionalizing the programs and ensuring
This implementation road map identifies data, data their long-term success
exchange, and information system barriers to imple-
menting ECM and ILOS program functions, and offers Each recommendation offers a proposed set of actions,
a set of recommendations and actions for policy- including their sequence and timing for implementa-
makers, government agencies, MCPs, and providers tion. Road map development was informed by over
(see Table 1 on page 5). As the road map describes, two dozen interviews and an advisory group com-
whole-person approaches to care require all parties posed of DHCS, MCPs, county agencies, providers,
in a community to step outside of their traditional and community-based organizations.
boundaries to provide a level of collaboration and
coordination that addresses drivers of health. These
California Health Care Foundation www.chcf.org 4Table 1. Road Map Recommendations Overview: CalAIM and Health Data Sharing, continued
RECOMMENDATIONS LEGEND ROAD MAP ACTIONS
$ Regulations/Policies
$ Technical Infrastructure/Standards
$ Financing/Contracting/Operations 2021 2022–24 2025+
1. L
egal and regulatory alignment for data exchange: Sharing physical, behavioral, and social service information implicates a
broad cross-section of federal and state privacy rules and regulations, with differing levels of associated consent policies, and
financial and criminal penalties.
$ Extend WPC authorizing State lawmakers should work with DHCS to develop legis-
legislation to apply to all lation and subsequent guidance that permits information
entities participating in ECM, exchange activities in support of CalAIM and Medi-Cal
ILOS, and other Medi-Cal program objectives.
care management programs.
$ Develop “universal consent” DHCS should establish a The DHCS workgroup should develop recommendations that
guidance. workgroup to support the address federal law and refine state law to create a statewide
development of standard universal consent form. Depending on the findings of the
consent form elements and workgroup, the California Health & Human Services Agency
case examples. (CHHS) should work with stakeholders and the legislature to
craft legislation or an executive order to facilitate creation of
$ Remove statutory barriers to CHHS should establish a a universal consent form.
a universal consent form. multi-department workgroup
to assess statutory barriers
to implementing a universal
consent form, and required
actions to resolve them.1
$ Develop legal guidance for California Office of Health Information Integrity (CalOHII)
health information exchange should work closely with DHCS to draft and refine State
(HIE) for ECM and ILOS Health Information Guidance (SHIG) to clarify laws and
stakeholders. regulations that affect disclosure of physical, behavioral,
and social service information, and should offer technical
assistance to advise when various data may be shared to
support program functions.
$ Develop member condition MCPs should work with MCPs and ECM/ILOS data sharing providers should imple-
or status identifiers to reduce ECM/ILOS providers to ment proxy measures where DHCS/CalOHII exchange tactics
unnecessary sensitive data determine where standard indicate that full release of patient data may not be feasible.
sharing. proxy indicators may be
shared in lieu of full
patient data.
$ Implement electronic consent MCPs should develop and MCPs should implement consent management systems,
management systems. test data sharing consent refining access and utilities as needed.
management systems with
ECM, ILOS, county, and
other providers.
$ Integrate ECM participation DHCS should assess options DHCS should implement collection of ECM participation and
and data sharing consent in to acquire ECM and other data sharing consent during enrollment and redetermination
the Medi-Cal enrollment program and data sharing and share consent information with MCPs.
application. member consents during
enrollment.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 5Table 1. Road Map Recommendations Overview: CalAIM and Health Data Sharing, continued
RECOMMENDATIONS LEGEND ROAD MAP ACTIONS
$ Regulations/Policies
$ Technical Infrastructure/Standards
$ Financing/Contracting/Operations 2021 2022–24 2025+
2. S
tatewide infrastructure for data exchange: Many ECM and ILOS participants including providers, county agencies,
CBOs, and payers do not have information technology capabilities necessary to support robust cross-sector data exchange.
Standards, data sharing specifications, and infrastructure are needed, especially for housing, justice, and other social data.
ECM and ILOS program participants will build on the WPC pilot infrastructure to advance ECM and ILOS objectives.
$ Develop a legislative mandate The governor’s office, DHCS, $ State agencies should be required to implement and
requiring participation in CalPERS (California Public enforce legislative requirements that specify goals,
HIE activities and care Employees’ Retirement funding and incentives program opportunities,
transition notifications. System), Covered California, reporting requirements, and penalties in subsequent
and other stakeholders regulatory guidance.
should work with the legisla- $ State agencies should report progress against goals
ture to craft legislation that and identify remaining barriers and additional actions
defines a vision for state- that can be taken.
wide information exchange,
including use cases, financ- $ State agencies should provide additional implementation
ing mechanisms, and types guidance and support development of necessary
of data and providers that amendments.
should be required to share
information.
$ Develop requirements for CHHS, the Board of State CHHS, BSCC, and CDCR
correctional facilities to send Community Corrections should implement HIE
health information to the (BSCC), the California funding programs for
next provider of record upon Department of Corrections correctional facilities
member release. and Rehabilitation (CDCR), and enforce data sharing
county jails and sheriff’s requirements.
departments, and other
stakeholders should work
together to identify funding
sources and define HIE
requirements for correctional
facilities to share health
information with community
providers.
$ Develop standards and DHCS, CalOHII, and other $ DHCS and CalOHII should
guidance for the exchange stakeholders should establish develop SDOH coding
of SDOH information. standards for the collection guidance.
and sharing of SDOH $ MCPs should provide
information. training on how to use
new standards and ILOS
billing codes.
$ Establish working groups to CHHS, CalOHII, DHCS, and $ CHHS, CalOHII, and
develop state standards and other stakeholders should DHCS should develop
recommend guidance for establish a workgroup to California-specific
nonmedical event notifications define requirements for implementation guides,
(e.g., housing, incarceration, sharing nonmedical event guidance, and case
employment status changes). notifications and develop studies.
plans to test nonmedical $ The state and workgroup
event notification. participants should
test event notification
protocols.
California Health Care Foundation www.chcf.org 6Table 1. Road Map Recommendations Overview: CalAIM and Health Data Sharing, continued
RECOMMENDATIONS LEGEND ROAD MAP ACTIONS
$ Regulations/Policies
$ Technical Infrastructure/Standards
$ Financing/Contracting/Operations 2021 2022–24 2025+
$ Develop Homeless CHHS should convene state $ State and county health agencies including HMIS Lead
Management Information and county agencies and Agencies and correctional facilities should incorporate
System (HMIS) and correc- stakeholders to develop data exchange requirements into vendor contracts.
tional facility data exchange template contract language $ Agencies should identify and use funding to defray
contracting requirements requirements for data HMIS and state and county correctional facility HIE
and financing programs. sharing. implementation costs.
$ Develop financing and $ DHCS should establish DHCS, MCPs, and other
incentive payment programs an incentive payment stakeholders should enable
to invest in delivery system program and provide identified incentive and
infrastructure, build care MCPs with guidance for funding programs.
management and In Lieu plans to include incentive
of Services capacity, and payments in their
improve quality performance program structure.
and measurement reporting
$ DHCS should work with
that can inform future policy
legislators, MCPs, and
decisions.
other stakeholders to
identify additional funding
for needed HIE, ECM and
ILOS providers, HMIS Lead
Agencies, correctional
facilities, and others to
support capacity building
and infrastructure
investments.
$ Develop contractual DHCS, CalPERS, and $ DHCS, CalPERS, and Covered California should
requirements to participate Covered California incorporate requirement into MCP contract language,
in data exchange. should define contractual providing a glide path for implementation, and assess
obligations for MCPs that whether further expansion of requirements is warranted.
require contracted providers $ Public and private payers should develop patient visit
to participate in data summary, ADT (admission, discharge, transfer), and other
sharing activities. nonmedical alert notification requirements into MCP
contracts.
$ MCPs should develop processes for sharing patient visit
summary and ADT data with ECM providers and support
training on use of ADT data.
3. C
are management, shared care plans, and assessment capabilities: Many ECM providers will not have robust system
capabilities to unify and share care plans and to receive, aggregate, and integrate care management and care coordination
information.
$ Develop minimum necessary DHCS should work with MCPs to develop care management documentation system
care management documenta- expectations and requirements, and further define MCP responsibilities for ensuring
tion system capabilities and ECM providers have access to such systems.
guidance.
$ Develop shared care plan DHCS should work with stakeholders to define a minimum set of sharable care plan data
policy guidance. elements, formats, and exchange methods required to be exchanged by MCPs and their
contracted ECMs.
$ Implement common care MCPs should implement DHCS guidance on minimum care
plan standards. plan data elements and transmission standards.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 7Table 1. Road Map Recommendations Overview: CalAIM and Health Data Sharing, continued
RECOMMENDATIONS LEGEND ROAD MAP ACTIONS
$ Regulations/Policies
$ Technical Infrastructure/Standards
$ Financing/Contracting/Operations 2021 2022–24 2025+
$ Develop accessible care MCPs should test care $ MCPs should deploy care management and care plan
management documentation management documenta- sharing platforms.
systems for ECM providers tion systems and options for $ MCPs should provide ongoing technical assistance (TA)
lacking internal capabilities sharing care plans with ECM to ECM and other providers to help implement care plan
capacity. providers. systems and sharing technologies and services.
$ Assess development of a DHCS, MCPs, and ECM Depending on assessment, establish regional or statewide
statewide care plan repository. providers should assess shared care planning infrastructure.
options to create regional or
state care plan repositories.
$ Develop care management MCPs should develop training program to support ECM provider adoption and use of shared
documentation systems care plans and care management documentation systems.
and care plans training and
TA programs.
$ Develop financing programs DHCS and MCPs should DHCS and MCPs should implement financing programs.
to build technical capabilities develop plans to access
for ECM and ILOS providers. funding that supports
ECM and ILOS information
technology (IT) capacity.
4. C
ommunity resource closed-loop referrals for social and human services: Many ILOS providers lack access to a technical
platform, infrastructure, and capabilities to receive referrals and to access demographic, eligibility, and authorization infor-
mation from MCPs and referring providers. Also, referring providers often do not have access to electronic directories and
associated workflows to close the loop on ILOS referrals.
$ Develop guidance for refer- DHCS should develop
ral and information sharing guidance to help MCPs and
among MCPs and ECM and providers establish closed-
ILOS providers. loop referral platforms and
processes.
$ Develop and deploy refer- MCPs should collaborate MCPs should test and roll out closed-loop referral platforms.
ral service standards and and deploy a standard set
platforms accessible to of closed-loop referral data
contracted ECM and ILOS elements and processes.
providers.
$ Provide training and TA to MCPs should develop MCPs should update train-
ECM and ILOS providers to training for ECM and ILOS ings to reflect evolving
support workflow changes providers on ILOS referral system designs and program
and access to systems used processes and systems. requirements.
to authorize, track, and
close referrals.
California Health Care Foundation www.chcf.org 8Table 1. Road Map Recommendations Overview: CalAIM and Health Data Sharing, continued
RECOMMENDATIONS LEGEND ROAD MAP ACTIONS
$ Regulations/Policies
$ Technical Infrastructure/Standards
$ Financing/Contracting/Operations 2021 2022–24 2025+
5. P
erformance reporting and ECM and ILOS billing: Many ECM and ILOS providers will not have the technical capabilities or
capacity to submit claims to MCPs in compliance with state and national standards, and their systems will not be configured to
capture and store clinical data in a structured, standardized format to support performance reporting.
$ Develop guidance to support DHCS should convene MCPs MCPs should implement
standardized ECM and ILOS and ECM and ILOS providers minimum billing data
invoicing and billing. to develop a minimum set element requirements.
of data elements for invoic-
ing and billing, including
minimum requirements for
ECM/ILOS providers unable
to submit compliant claims.
$ Establish clear ECM and DHCS should review program $ DHCS should finalize measure selection and provide MCP
ILOS quality and perfor- goals and objectives with reporting guidance.
mance improvement goals, ECM and ILOS stakeholders $ DHCS should evaluate ECM/ILOS programs by selected
objectives, and performance and define measures to measures and refine measure selection, as needed.
metrics. assess program efficacy.
$ Develop standard ECM and MCPs should collaborate MCPs should implement and refine billing templates, as
ILOS billing templates. with other plans and provid- needed.
ers to develop and test a
standardized set of minimum
billing data elements and
requirements and to develop
invoicing templates and
processes for ECM and
ILOS providers.
$ Define performance metric DHCS should develop and DHCS should update measure specifications, as needed.
technical specifications. refine existing performance
measure specifications,
as needed.
$ Develop ECM and ILOS MCPs should develop ECM MCPs should update training programs as needed to reflect
provider training and TA to and ILOS training programs updates and changes to billing guidelines and practices.
support billing and reporting. on coding and billing
practices.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 9and information exchange across managed care plans
CalAIM ECM and (MCPs); physical, behavioral, community-based, and
social service providers; and county agencies to pro-
ILOS Background vide members with a comprehensive array of health
Medi-Cal is the nation’s largest Medicaid program and social services to address the underlying drivers of
as measured by enrollment and spending, providing poor health outcomes, including inequity. Two primary
health care coverage for over 13 million Californians.2 elements of the new CalAIM program include:
The California Department of Health Care Services
(DHCS), which administers Medi-Cal, has used its Enhanced Care Management (ECM). The ECM
1115(a) waiver authority to test novel initiatives benefit will provide whole-person care management
aimed at improving outcomes and managing costs to help address the clinical and nonclinical needs of
for its members. In 2015, the Centers for Medicare Medi-Cal MCPs’ highest-risk members. MCPs will
& Medicaid Services (CMS) approved DHCS’s “Medi- administer and oversee ECM benefits, identifying
Cal 2020” waiver, including its county-based Whole members in ECM target populations who would ben-
Person Care (WPC) pilots, to transform and improve efit from long-term coordination of physical health,
the quality of care, access, and efficiency of health behavioral health, and social services across delivery
care services. WPC is focused on improving the coor- systems. ECM services will be community-based and
dination of physical health, behavioral health, and locally provided, with high-touch, on-the-ground,
social services for vulnerable members with poor face-to-face, and frequent interactions between mem-
health outcomes who were identified as high users bers and “ECM providers,” which will be responsible
of multiple systems.3 Concurrently, DHCS, through for the coordination and management of patient care.7
State Plan Amendment 16-007, established a plan- MCPs and the ECM providers with whom they con-
based Health Homes Program (HHP) to serve eligible tract will need to collaborate with a broad contingent
Medi-Cal members with complex medical needs and of physical, behavioral, and social service providers,
chronic conditions.4 The HHP was designed to sup- county and state agencies, and others to securely
port members who could benefit from stronger care share member data to support care coordination and
management and coordination services for a full range management. DHCS expects that MCPs will build on
of physical health, behavioral health, and community- the expertise and health information technology (HIT)
based long-term services and supports (LTSS).5 infrastructure developed through the WPC pilots and
HHP to support ECM implementation.
In Lieu of Covered Services (ILOS). MCPs will have
Social determinants of health (SDOH) —
the conditions in the environments where the option to offer ILOS, which are cost-effective,
people are born, live, learn, work, play, worship, health-supporting — though generally nonmedical —
and age — are estimated to be up to 80% activities that may substitute for State Plan–covered
responsible for a health outcome. services to reduce hospitalization and institutionaliza-
tion or that otherwise address underlying drivers of
poor health. If states choose to opt to provide ILOS
In 2022, DHCS is sunsetting the HHP and WPC pilots, and receive federal funds to support them, federal law
drawing lessons from that experience, and transitioning requires that they are optional for MCPs to provide
critical program elements into its California Advancing and for enrollees to accept.8
and Innovating Medi-Cal (CalAIM) program. CalAIM
builds upon these initiatives to manage member care MCPs may choose to offer ILOS in counties they
and need through whole-person care approaches, serve and if they do, they must offer them to all mem-
while addressing social determinants of health.6 bers in the county who qualify. If MCPs elect to offer
CalAIM envisions enhanced coordination, integration, ILOS, they must also establish and maintain networks
California Health Care Foundation www.chcf.org 10of community-based organizations to provide ser- $ Business drivers, incentives, and financing to sus-
vices, and integrate those services with their ECM tain the program. Building technical infrastructure
approaches.9 Offered ILOS will be accounted for in and providing support for CBOs not integrated
MCP rate setting. with the health care system will require alignment
of contracting incentives and funding sources to
DHCS expects MCP implementation of ILOS will sup- underwrite and sustain necessary investments.
port the transition of its WPC pilot and HHP, covering
previously provided services that may not otherwise Each actor — from policymakers, to state and
be included under the State Plan benefits. county agencies, to CBO — will have an important
role to play in successfully launching and sustaining
CalAIM’s ECM and ILOS programs will engage a the ECM and ILOS programs in California. Whole-
broad set of providers, county agencies, and com- person approaches to care require whole-community
munity-based organizations, many of whom have not approaches to care, necessitating that all parties step
extensively interacted with the health care system, outside of their traditional service boundaries to col-
creating unique challenges to implementation. laborate and coordinate care to effectively address
root drivers of health.
This road map defines the program information sys-
tem, data sharing, and data use activities that will be
necessary for ECM and ILOS stakeholders to carry out
core program functions, as well as potential barriers to DHCS has proposed covering 14 ILOS,
implementation across three dimensions:
including:
1. Housing transition and navigation services
$ Technical infrastructure to support information 2. Housing deposits
sharing and use. Most ILOS and some ECM provid-
3. Housing tenancy and sustaining services
ers will not be integrated with their partner health
care systems and may lack necessary information 4. Short-term post-habilitation housing
technology capacity to effectively participate in the 5. Recuperative care (medical respite)
program. Further, most communities in California 6. Respite care
lack the robust data exchange infrastructure neces-
7. Day habilitation programs
sary to support access to and sharing of physical,
behavioral, and social service data needed to coor- 8. Nursing facility transition support to assisted
dinate complex care. living facilities
9. Community transition services / nursing facility
$ Legal and policy environment to facilitate infor- transition to a home
mation sharing. Sharing information to coordinate 10. Personal care and homemaker services
care and improve access to behavioral health and
11. Environmental accessibility adaptations
social services implicates an extensive and complex (home modifications)
set of federal and state rules that extend beyond
12. Meals / medically tailored meals
traditional governing statutes (e.g., HIPAA [Health
Insurance Portability and Accountability Act]). 13. Sobering centers
Understanding these rules and developing respon- 14. Asthma remediation
sive policies to obtain and manage consent has
proven difficult for WPC pilot and HHP program
participants and will likely prove similarly difficult
for ECM and ILOS stakeholders.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 11Methodology ECM and ILOS Program
In 2020, Manatt worked with DHCS and WPC pilot Data Functions
and HHP stakeholders including counties, MCPs, pro-
Manatt, DHCS, and the advisory group identified
viders, and CBOs to assess the data, data exchange,
seven critical data-dependent use cases required to
and information systems that DHCS and future ECM
support the ECM and ILOS programs. Each function
and ILOS providers, MCPs, counties, and other partici-
describes the activities that need to be carried out
pating organizations will need to support critical ECM
by program participants to ensure program success,
and ILOS program functions. Manatt further assessed
as explicitly required in DHCS or MCP contracts or
the current capabilities of prospective ECM and ILOS
implied but not mandated through policy guidance or
stakeholders to identify potential challenges and gaps
contracting. These functions include:
in technology, data exchange infrastructure, standards,
policy, and business drivers. Manatt’s assessment was 1. ECM member identification, review, and authori-
informed by the following activities: zation. MCPs will identify target ECM populations
by compiling and analyzing data and information
$ Research and analysis of the WPC pilots and HHP.
received from counties, providers, and members,
Manatt reviewed published reports on lessons
among other sources.
learned from these foundational pilot programs.
2. ECM assignment and member engagement.
$ Stakeholder interviews. Manatt interviewed over
MCPs will assign members to an ECM provider
50 people across a diverse set of two dozen orga-
based on their previous provider relationships,
nizations from August through October 2020 to
health needs, and known preferences. Member
understand and document lessons from California’s
outreach and engagement into the ECM benefit
WPC pilots and HHP and to discuss potential bar-
will be conducted by ECM providers to the extent
riers to ECM and ILOS program implementation.
possible.
(See Appendix A for a list of interviewees.)
3. ECM care plan development, sharing, and use.
$ DHCS ECM/ILOS data strategy workgroup. Manatt
ECM providers will develop care plans using data
facilitated meetings with DHCS program and oper-
acquired from the MCP, the member, and other
ational staff from August 2020 through January
sources, and make the care plan available for use
2021 to discuss ECM and ILOS stakeholder data
by a member’s care team.
use expectations for specific program functions,
and potential mitigation strategies for identified 4. ECM care coordination and referral manage-
issues. ment. ECM providers will support coordinated and
transitional care and engage MCPs’ referral net-
$ ECM/ILOS data strategy advisory committee.
works for community and social services, including
Manatt convened a stakeholder advisory commit-
ILOS.
tee of 14 WPC and HHP organizations to advise
on potential ECM and ILOS stakeholder data use 5. ECM and ILOS billing and encounter reporting
expectations, potential barriers to program imple- practices. ECM and ILOS providers will record and
mentation, and resolution strategies. The advisory report services rendered to MCPs in standard for-
committee met three times between October 2020 mats, as specified by DHCS (e.g., claims, invoices).
and January 2021. (See Appendix B for a list of MCPs will be expected to report complete and
committee members.) accurate encounters of all services provided by
contracted ECM and ILOS providers to DHCS using
Manatt supplemented stakeholder feedback with identified codes.
original legal, policy, and program research.
California Health Care Foundation www.chcf.org 126. ECM and ILOS quality measure and performance $ People at risk for institutionalization with serious
reporting. MCPs will report DHCS-specified qual- mental illnesses, children with serious emotional
ity and performance metrics to demonstrate ECM disturbances, or substance use disorders (SUDs)
and ILOS program impact on member outcomes with co-occurring chronic health conditions
and MCP operational performance.
$ People transitioning from incarceration who have
7. ILOS needs assessment and referral manage- significant complex physical or behavioral health
ment. MCPs, ECM providers, and ILOS providers needs requiring immediate transition to the
will identify members requiring ILOS benefits, and community
MCPs, PCPs, or ECM providers will connect mem-
$ Additional target populations identified by an MCP
bers to ILOS through a closed-loop referral process.
and approved by DHCS.10
Stakeholders should review the latest DHCS guidance
MCPs will be expected to identify members for ECM
to understand their organization’s exact data use and
through a combination of data sources, including
reporting expectations.
enrollment, Medi-Cal fee-for-service, and encoun-
ter data they receive from DHCS and generate and
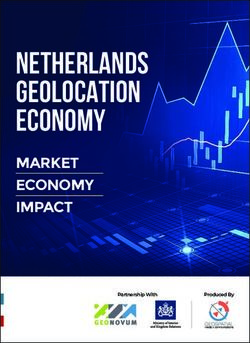
1. ECM Member Identification,
Review, and Authorization Potential Data Exchanges
MCPs will be responsible for identifying high-cost,
high-needs members eligible for the ECM ben- Enrollment, Claims, Encounter, Pharmacy,
Lab, Behavioral Health, Clinical Data
efit who could gain the most from the program’s
comprehensive, high-touch, interdisciplinary, and
WPC Pilot +
community-based care management services, par- HHP Rosters
ticularly as they move through significant health and 1 2
5 3 Needs
social transitions. The identification of members within Assessment
each of the DHCS-defined “target populations” will Data
be supported by providers, county agencies, and xxxxxxxxxxxxxxx
HIO
community-based organizations who have physical,
MCP CM/Data Systems
behavioral health, and social service information and
insights. Target populations shall include: Clinical, Clinical,
4 SDOH Data ADT Data
$ Children or youth with complex physical, behav-
ioral, developmental, and oral health needs
$ People experiencing chronic homelessness or who ECM Member Health Care County CBOs
or Family Provider
are at risk of becoming homeless
$ High utilizers with frequent hospital admissions, 1 Member enrollment and encounter files
short-term skilled nursing facility stays, or emer-
2 Methodology for identifying ECM members
gency room visits
3 Risk stratification and analytics using available data
$ Nursing facility residents seeking to transition to (e.g., claims/encounters, clinical data)
the community 4 Identification or requests from providers, counties,
other CBOs, and members/families
$ Those at risk for institutionalization who are eligible 5 “Supplemental” reporting (to be determined)
for long-term care services
Note: See Appendix C for a glossary of abbreviations.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 13manage themselves; other administrative, clinical, Files will include a list of members authorized for the
social service, and care needs; and assessment infor- ECM benefit, and available encounter and/or claims
mation they can securely access through partnerships data; physical, behavioral, administrative, and SDOH
with county agencies, providers, community and (e.g., housing) data; and reports of performance on
social service providers, and health information orga- quality measures. ECM providers will be expected to
nizations (HIOs). MCPs will also be required to assess reach out to assigned members and use data from the
requests for the ECM benefit from providers, mem- MCP and other sources to support member engage-
bers, and member caretakers. ment.12 Specifically, ECM providers will:
$ Notify the member of ECM benefit and authoriza-
Implementation of ECM and ILOS will be phased in
tion, and allow the member to choose a different
beginning in counties with a HHP or a WPC pilot.
ECM provider, if desired
MCPs will authorize the ECM benefit for all members
enrolled or in the process of enrolling in the HHP and $ Obtain member consent to participate in the ECM
will develop an approach for transitioning members program
enrolled or in the process of enrolling in WPC pilots
that includes consideration of which members would
benefit from ECM. MCPs will determine whether other Potential Data Exchanges
members meet ECM authorization criteria and will
include them in member assignment files distributed
to ECM providers.11 MCPs will report to DHCS, based
on provided specifications, the members that have
been authorized and are receiving the ECM benefit.
5
2. ECM Assignment and Member
1
Engagement
xxxxxxxxxxxxxxx
Once members are identified and authorized for the
MCP CM/Data Systems
ECM benefit, MCPs will identify the providers each
member has engaged with and determine the most
2 4 Member Preferences
appropriate provider for ECM assignment based on
that member’s physical, behavioral health, and social
needs. ECM providers may include primary care pro-
3
viders (PCPs), behavioral health specialists, county ECM Provider ECM Member or Family
behavioral health providers, and community clinics,
among others. If a member’s preferences for a specific
1 MCP analysis of available member data to determine
ECM provider are known to the MCP, it will assign the ECM provider assignment
member to that ECM provider to the extent practica- 2 MCP assignment files
ble. If the member’s assigned PCP is an ECM provider,
3 ECM provider outreach to members; request for
the MCP will assign the member to the PCP, unless consent confirmation
the member has expressed a different preference or 4 ECM provider reports member engagement activity
a more appropriate ECM provider is identified, given and consent (+ change requests) to MCPs
the member’s individual needs and conditions (e.g., a 5 MCP sends supplemental reports to DHCS
behavioral health entity).
Note: See Appendix C for a glossary of abbreviations.
After assignment is confirmed, MCPs will be required
to share member assignment files with ECM providers.
California Health Care Foundation www.chcf.org 14The ECM benefit will be initiated once verbal or writ- ECM providers will be expected to engage members
ten consent is obtained from authorized members. directly and, where feasible in person, proactively
ECM providers will communicate member consent to monitor member progress against care plan goals,
the MCP, which will manage consent records across its and, along with the rest of a member’s care team,
ECM population.13 ECM providers will inform MCPs update progress toward goals and any changes in the
of members they could not reach, who may be incor- member’s needs and goals. Members will have access
rectly assigned, or who declined to participate in the to their care plans, among other information “created,
benefit. MCPs will send supplemental reports that gathered, managed, and consulted by authorized
DHCS will define and that describe member engage- health care clinicians and staff” per proposed federal
ment activity to DHCS. Individual Right of Access requirements.14
3. ECM Care Plan Development, Potential Data Exchanges
Sharing, and Use
Once a member is assigned to and engaged by an Organizations Involved in Member Care
ECM provider, the provider will work directly with the Physical, Behavioral, Dental, LTSS, Developmental,
Social Service, Administrative, and Other Data
member to perform a comprehensive assessment and
develop an individualized, person-centered care plan
xxxxxxxxxxxxxxx
that documents the member’s health risks, needs, MCP County HIO Other Providers
goals, and preferences for care. To develop care
plans, ECM providers will use member data acquired 1
from MCPs, directly from members and caretakers,
ECM Provider
and from other sources including state and county
agencies (e.g., behavioral health, substance use disor-
der, justice data), other health care providers directly 3 2
or through HIOs (e.g., clinical data, care plans), and Care Team Care Plan CM/Data
Systems
community-based and social service providers.
ECM providers will be expected to use a care man- ECM Member or Family
agement documentation system or process that aligns
with MCPs’ Model of Care and is capable of integrat- 1 ECM provider acquires member information from MCP,
county, other providers and/or HIO
ing physical, behavioral, dental, LTSS, developmental,
social service, and administrative information from 2 Care plan developed using information available to
the ECM provider care team
other entities in order to create, manage, and maintain
3 Care plan shared with and updated by care team and
a care plan that can be shared with other providers
shared with member; care plan may also be shared
and organizations involved in a member’s care. with other organizations involved in member’s care
Note: See Appendix C for a glossary of abbreviations.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 154. ECM Care Coordination and MCPs will establish parameters for ECM providers to
maintain care management documentation systems or
Referral Management
processes that can track and elevate changes in mem-
MCPs will be required to ensure that members
ber health status, support care team notification of
authorized for ECM benefits receive enhanced care
relevant health status changes, and manage referrals
coordination services, including:
to physical and behavioral health, and social service
$ Coordinated, continuous, and integrated patient providers. Information gathered through member
care, as outlined in the care plan and facilitated engagement and referral processes will be used to
through care team information exchange update the member’s care plan.
$ Support for member treatment adherence
$ Tracking member admissions and discharges Potential Data Exchanges
$ Developing care transition plans and performing
Organizations Involved in Member Care
engagement activities that seek to reduce avoid-
able member admissions and readmissions
xxxxxxxxxxxxxxx
$ Communicating and sharing of member care needs MCP Medical & BH Providers HIO County
preferences and other necessary information with
1 5
the member’s care team
ECM Provider
Most of these activities will likely be assigned to
ECM providers. ECM providers will be expected to 2
proactively monitor assigned members’ health and
CM/Data
well-being and provide responsive care management Care Team Care Plan Systems
interventions, using alerts from a variety of sources that
3
signal changes in assigned members’ situations and Directory
4
health status. Upon receiving notification of a member ECM Member
clinical or nonclinical event — including admission to a
hospital, changes to incarceration status, and changes
that would otherwise necessitate outreach and action 1 ECM provider will monitor changes to member health
using a variety of data and referral sources
— and as the care team identifies other member
changes or needs that necessitate follow-up, the ECM 2 ECM provider updates care plan
provider will seek to engage and connect the member 3 ECM provider engages care team and member, and
refers member to appropriate provider
to the appropriate providers, services, and resources,
consulting the MCP’s provider directory as needed to 4 Member referred to appropriate medical or ILOS
provider; referral noted in CM system
make referrals, coordinating care, and supporting care
5 Completed referral noted in CM system by ILOS
transitions. Referrals that require prior authorization provider or through ECM provider follow-up
from MCPs will follow established MCP authorization
Note: See Appendix C for a glossary of abbreviations.
processes and policies. ECM providers will be notified
or will follow up to confirm that their assigned mem-
bers received the referred services (i.e., will “close the
loop”).
California Health Care Foundation www.chcf.org 165. ECM and ILOS Billing and Potential Data Exchanges
Encounter Reporting Practices
ECM and ILOS providers will generate and submit
claims/invoices to MCPs, either directly or through
clearinghouses or managed services organizations
using DHCS-defined billing codes, standard speci-
3 4
fications (ANSI ASI x12 837P), and electronic data
interchange transmission methods.15 Some ECM and 5
ILOS providers will not have the technical capabilities xxxxxxxxxxxxxxx
and systems to submit a compliant 837 claim, and will 6 MCP
Clearinghouses
be permitted to submit invoices to MCPs for generat- and MSOs
ing payments and encounter data to submit to DHCS.
1 2
Minimum data elements will include:
$ Member demographic and identifier information
ECM and ILOS
(e.g., Medi-Cal managed care plan member ID) Providers
$ Services provided with relevant HCPCS (Healthcare
Common Procedure Coding System) and modifier 1 ECM/ILOS provider invoices, claims, and encounters
codes16 2 MCP transmits error reports for ECM/ILOS provider
resolution
$ Units or number of services provided
3 MCP submits ECM/ILOS provider encounters,
$ Date service rendered and end date, if applicable supplemental reports
4 DHCS transmits error reports for MCP resolution
MCPs will review ECM and ILOS provider claims and 5 ECM/ILOS providers may submit claims to
invoices for accuracy and completeness, will gener- clearinghouses/MSOs for MCP submission may do
similarly for DHCS file submission
ate “error reports” back to submitters (e.g., incorrect
coding, syntax, or submission), and will request reme- 6 Magellan Rx pharmacy encounter data transmitted
to MCPs
diation as needed. Error reports may be transmitted
Note: See Appendix C for a glossary of abbreviations.
as standard x12 999 error reports for providers able
to receive and process them, and in an alternative,
simplified format for providers that cannot. MCPs
will be prohibited from imposing additional reporting
requirements on ECM and ILOS providers.17
MCPs will be responsible for submitting ECM and ILOS
encounters to DHCS and ensuring those encounters
are complete and accurately coded per DHCS speci-
fications. MCPs will also be responsible for submitting
supplemental reports to DHCS that may include ECM
and ILOS engagement and service use data, which
DHCS may use to verify encounter data completeness.
DHCS will process MCP encounters and supplemen-
tal reports, and generate and send error and other
response reports to MCPs.
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 176. ECM and ILOS Quality Measure Potential Data Exchanges
and Performance Reporting
DHCS will establish ECM and ILOS quality improve-
ment and performance requirements for MCPs based
on existing Medi-Cal managed care measure sets.
MCPs will calculate measures using available claims/
4
encounter, clinical, and social data as required by
DHCS. Should metrics include hybrid measures, MCPs
will be expected to acquire the necessary administra-
3
xxxxxxxxxxxxxxx
tive, clinical, and social service data from ECM and
MCP CM/Data Systems
ILOS providers to support measure calculation, aggre-
gation, and reporting. DHCS may choose to separately
1 2
compile and analyze submitted claims/encounter,
clinical, and social service data to calculate quality 5
ECM and
measures and report results back to MCPs. DHCS may Other Providers ILOS Providers
integrate measures into its managed care quality strat-
egy and performance improvement programs.18
1 ECM and other providers transmit administrative and
clinical data
MCPs will conduct oversight of participation in the
2 ILOS provider transmits claims and invoices
ECM benefit and ILOS with respect to all subcontrac-
3 MCP calculates quality and performance measures
tors to ensure benefit quality and ongoing compliance
with program requirements. DHCS expects MCPs will 4 MCP reports ECM and ILOS quality and performance
measures (through External Quality Review
share reports with ECM and ILOS providers of per- Organization process)
formance on quality measures, as requested. To the
5 MCP transmits quality measure reports for assigned
extent metrics attributed to ECM and ILOS provid- members back to ECM and ILOS providers
ers are shared by MCPs, MCPs may set expectations
Note: See Appendix C for a glossary of abbreviations.
that they use this information to enhance and improve
their processes, workflows, and outcomes.
California Health Care Foundation www.chcf.org 18ILOS providers will accept referrals, conduct out-
7. ILOS Needs Assessment and reach to referred members (as needed), and confirm
Referral Management whether members receive the referred service. ILOS
An MCP will be responsible for coordinating ILOS providers will provide updates to members’ MCP and
for members, to the extent the MCP offers ILOS. ECM providers upon outreach and service delivery
Coordination of and referral to community and social and may request that additional ILOS be authorized
support services will include determining appropriate depending on member need. MCPs will be required
services to meet member needs, including services to ensure that referral loops are “closed,” confirming
that address social determinants of health, housing, whether services were rendered.
and other ILOS offered by the MCP.
Many of these obligations will be assigned by the MCP Potential Data Exchanges
to ECM providers, which may use available claims/
encounter, clinical, housing, social service, admission, ECM
1
MCP
discharge and transfer (ADT), and other data to iden-
xxxxxxxxxxxxxxx
tify members in need of offered ILOS. ECM providers
Provider (if applicable) Plan CM/Data Systems
will also assess ILOS referral requests from members,
the member’s family, or providers, and will evaluate 3
alerts they may receive that signal a change in health
status, admission or discharge from a facility, or a tran- Care Team Referral System Directory
sition between care settings (e.g., discharge from a
short-term residential facility stay) to determine if that 5
member would benefit from available ILOS.19
ILOS User
2
ILOS authorization requests will be submitted to MCPs ILOS Provider 4
(may be affiliated
to assess appropriateness and member eligibility. with ECM providers)
MCPs may authorize ILOS where they are determined
to be a medically appropriate and cost-effective
substitute for covered services or settings. When 1 MCP analyzes data to identify member who may
authorization decisions are reached, MCPs will notify benefit from ILOS services; ECM and ILOS providers
may identify members who may benefit from ILOS
members and their ECM and ILOS provider or other
2 Members may self-identify
requesting provider of the decision. The member will
be referred to an ILOS provider within the established 3 MCP refers member to ILOS provider via closed-loop
referral process
MCP-ILOS network, and the MCP will securely share
4 MCP notifies member’s ECM provider/PCP of referral
the member’s:
5 ILOS provider communicates with members’ ECM
$ Demographic and administrative information con- providers / care teams
firming the member’s eligibility and authorization Note: See Appendix C for a glossary of abbreviations.
status
$ Administrative, clinical, and social service informa-
tion, as appropriate and necessary to help the ILOS
provider understand the member’s needs
$ Billing information to support invoicing
CalAIM and Health Data Sharing: A Road Map for Effective Implementation of Enhanced Care Management and In Lieu of Services 195. Performance reporting and ECM and ILOS bill-
Implementation ing. Many ECM and ILOS providers will not have
the technical capabilities or capacity to submit
Road Map claims to MCPs in compliance with state and
The implementation road map identifies potential national standards, or systems to capture, store,
ECM and ILOS program implementation challenges and share health and social data needed to support
based on research, interviews with previous WPC pilot performance reporting.
and HHP participants, and advisory group feedback.
For each issue, the road map proposes strategies for
Each issue includes a description of the challenges
overcoming these barriers, along with specific actions
that ECM or ILOS providers, MCPs, DHCS, or other
that the state, MCPs, counties, health care providers,
stakeholders are likely to face before outlining the
and other community-based organizations can take
actions that can be taken to overcome them. Five
to resolve them. The strategies are segmented into
barrier categories have been identified as being of
three categories: regulatory and policy; technical; and
paramount importance requiring resolution including:
financing, contracting, and operations. The road map
1. Legal and regulatory alignment for data concludes with a discussion of the potential fund-
exchange. Sharing physical, behavioral, and social ing sources available to support the recommended
service information implicates a broad cross-section approaches.
of federal and state privacy rules and regulations,
with differing levels of associated consent policies,
and financial and criminal penalties. 1. Legal and Regulatory Alignment
for Data Exchange
2. Statewide infrastructure for data exchange.
Many ECM and ILOS participants, including pro- CHALLENGES
viders, county agencies, CBOs, and MCPs, will Coordinated efforts to address health disparities and
not have the HIT capabilities necessary to support to promote health equity for vulnerable populations
robust cross-sector data exchange. Data sharing require the secure exchange of sensitive information
infrastructure, standards, and specifications are subject to a large and complex set of federal and
needed — especially for data domains including state privacy laws, most of which were not written with
housing and justice facilities — to enable safe and broad multisectoral and electronic data exchange
secure information exchange. in mind. Also, California’s health privacy laws do not
always align with federal rules. State law can be more
3. Care management, shared care plans, and assess-
restrictive than federal rules in certain instances, such
ments. Many ECM providers will not have robust
as allowing patient information to be disclosed for
system capabilities to unify, manage, and share care
treatment purposes only if the recipient is a health care
plans or to receive, aggregate, and integrate care
provider, while HIPAA (Health Insurance Portability
management and care coordination information.
and Accountability Act) does not have this limitation.20
4. Community resource closed-loop referrals for HIPAA, for example, envisions disclosures of protected
social and human services. Many ILOS providers health information being made between “covered
lack access to a technical platform, infrastructure, entities,” while federal rules regulating Medicaid and
and capabilities to receive referrals and to access the Supplemental Nutrition Assistance Program allow
demographic, eligibility, and authorization informa- personal information being disclosed for program
tion from MCPs and referring providers. Referring operations purposes, and criminal history privacy laws
providers also often do not have access to elec- typically assume that such information will be used
tronic provider directories or workflows to support exclusively for criminal justice purposes and for back-
closed-loop referrals. ground checks.20 The lack of an established framework
that enables health, social service, and other providers
California Health Care Foundation www.chcf.org 20You can also read