Assuring Care Experience A Person Centred Care Approach Full Report
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

1
SCOTTISH GOVERNMENT
Chief Nursing Officer, Patients, Public and
Health Professions Directorate
Assuring Care Experience
A Person Centred Care
Approach
Full Report
Author: Heather C. Strachan,
National Clinical Lead, Care Governance
October 2012
Assuring Care Experience Full Report2
Contents
FOREWARD P3
1.0 KEY MESSAGES P4
2.0 INTRODUCTION P5
3.0 HIGH QUALITY CARE AND CARE EXPERIENCE P8
4.0 COMMITMENT TO A VALUES BASED CULTURE P9
5.0 STAFF CAPABILITY TO DELIVER HIGH QUALITY CARE P11
6.0 CONDITIONS REQUIRED FOR HIGH QUALITY CARE P14
7.0 ENACTING CARING VALUES, BEHAVIOURS AND IMPROVEMENT P 17
8.0 MEASURING THE CONSEQUENCE OF CARING P20
9.0 CONCLUSIONS P24
APPENDIX 1 CARE ASSURANCE FRAMEWORK PRINCIPLES P 25
APPENDIX 2 DEFINITIONS OF PERSON CENTRED CARE APPROACHES P 28
APPENDIX 3 CARING THEORIES P 29
APPENDIX 4 CARING AND ENABLING BEHAVIOUR DESCRIPTORS P 30
APPENDIX 5 PERSON CENTRED PROCESSES AND PRACTICE P 36
APPENDIX 6 MEASUREMENT TOOLS P 40
REFERENCES P 43
Assuring Care Experience Full Report3
Foreword
As Chief Nursing Officer for Scotland I care passionately about the quality of care which we
deliver across NHS Scotland. We know that our NHS is capable of delivering World Leading
Quality and we already have some acknowledged and significant achievements in improving
safe and effective care. We have made tremendous strides forward in our quest to embed
that excellence at every level of our organisations as well as achieving greater consistency
across the piece in Scotland. I believe that Scotland can achieve the same level of
recognition for the improvements we are making in person centred care and I am therefore
delighted to be leading the Person Centred Quality Ambition for Scottish Government.
We have looked at the case for improving care experience through the evidence, experience
of our staff and experts, and aligned this with many examples of the excellent work already
happening across Scotland to support improvements in person centred care. This report
presents this as a framework that I believe is ground breaking work of immense importance
to our staff and to the people and families who use our services. I am fully committed to
supporting and enabling our dedicated staff to work in positive practice environments which
are aligned with their values, and which encourage and empower them to drive quality and
innovation at the point of care. This will require an understanding and acknowledgement of
the interdependence of the quality dimensions and the importance of human factors and
relationships in their delivery. With many years of experience as a professional leader and
educator, I understand the importance of role models and clinical leaders in the practice field
and, critically, in having a sound evidence base to inform and underpin our thinking about
the human dynamic of care. This aspect of clinical practice and patients’ experience of care
can become submerged under the weight of evidence about the technical and interventional
aspects of clinical care. Yet patients are clear and consistent in their prioritisation of caring
behaviours alongside the delivery of safe and effective care. This framework, which was
inspired by the Caring Science work of Professor Kristen Swanson, serves to strengthen our
approach to improvement and is underpinned by our shared values and our commitment to
placing the people using, and delivering, our services at the heart of everything we do.
Professor Swanson, Dean and Alumni Distinguished Professor, University of North Carolina
at Chapel Hill, USA has made the following comment on this work:
“Your framework is well conceived and the use of the 5 C's of Caring very creative. You
have taken a very comprehensive approach to assuring that the person centred care
experience should be of the highest quality, focused on the care recipient, and grounded in
an ethic of caring. The challenge will be to enact strategies that get implemented system
wide, that are closely tracked for effectiveness, and that are sustained. Your framework
holds promise for meeting those challenges. I am honoured to see my work being applied in
such a promising manner.”
I commend this framework to you as a resource and look forward to working with you to
progress The Person Centred Health and Care Programme to meet the challenges we face
together as we strive for world leading quality in person centred care.
Ros Moore
Chief Nursing Officer
Directorate for Chief Nursing Officer, Patients, Public and Health Professions
Assuring Care Experience Full Report4
1.0 KEY MESSAGES
A review of the evidence suggests that a wide range of factors interrelate to create and
sustain high quality care and care experience. In particular they include caring and enabling
behaviours but also important aspects at system, organisational and team level. These
factors together underpin not just person centred care but also safe and effective care and
staff experience. All ultimately improve organisational performance. Therefore the case for
assuring care experience can be justified morally, clinically and financially.
For the organisation:
A person centred system is one in which the organisation clearly articulates person centred
care as a value and priority which is enacted through the attitudes and behaviours at all
levels of the organisation from CEO through leaders, managers, teams and individual staff.
Leaders must recognise that organisational effectiveness as well as safe, effective and
person centred care are driven by their values and behaviours. They are also dependent on
staff who work effectively as teams, who feel valued, supported and empowered to drive
quality locally. This is shared governance in action.
A person centred system improves organisational performance and patient experience of
care through: improved wellbeing; better health outcomes; and quality of life for service
users. This leads to reduced lengths of stays, adverse incidents, healthcare associated
infection, staff absence and turnover.
For people who use services
Person centred care enhances the therapeutic relationship between people who use
services and clinical staff which can reduce anxiety associated with health concerns and
healthcare delivery, ultimately improving care experience. This supports healing and may
reduce the need for medication, such as pain relief and hypertensive drugs. It also improves
trust in the team, within the organisation and increases the likelihood of treatment
completion.
Health outcomes are enhanced through more effective engagement in decisions and actions
associated with health promotion activities, treatment, monitoring, and self-management, all
of which impact on people’s ability to stay healthy or return to health
Quality of life is enhanced by improvements in both wellbeing and self-management which is
especially important when cure is no longer an aim of healthcare for older people or people
with long term conditions.
For staff
Staff experience and service user experience are inextricably linked. Those factors that
influence staff health and wellbeing also impact on care experience as well as safe and
effective care. In a person centred system, staff feel valued, empowered and supported;
team working is enhanced and service users care experience is increased further. Success
breeds success.
Jacqui Lunday
Chief Health Professions Officer
Directorate for Chief Nursing Officer, Patients, Public and Health Professions
Assuring Care Experience Full Report5
2.0 INTRODUCTION
Quality from a service user perspective includes: their care experience; the effectiveness of
their care interventions; and the safe delivery of healthcare. NHS Scotland’s Quality
Strategy’s ambitions aim to address these three areas, with efficiency as an overarching
theme. While much good practice takes place across Scotland, care experience can be
variable and the factors required to address the delivery of a consistently high quality care
experience are complex. Evidence is increasingly emerging which indicates person centred
care approaches, demonstrated by the caring and enabling behaviours of staff, are
fundamental to quality healthcare. These behaviours can positively influence service users’
outcomes as well as their overall care experience.
Added to the complexity is the emphasis in recent years on the need for efficiency, meeting
targets, improving safety and ensuring the effectiveness of technical interventions. This has
tended to promote standardised approaches to care delivery, creating challenges to
achieving a balance across the three quality ambitions of safe, effective and person centred
care. As the need to deliver even more efficient and effective services increases, the
challenge of delivering person centred care against apparently competing priorities, could
also be the solution. For example, a positive patient experience, as indicated by caring and
enabling behaviours, has been found in hospitals with better work environments. Good work
environments are influenced by positive leadership, effective team working, education and
development. These factors also influence staff health and well-being which impacts not
only on service users’ care experience but all three dimensions of quality. So success
breeds success. A positive care experience and the factors influencing this ultimately impact
on both effective and efficient healthcare services.
Complex problems have no simple solutions and require multifaceted, whole system
approaches which address relevant issues at every level of the organisation. They require
the collaboration and engagement of staff and service users to create opportunities to care
in flexible and innovative person centred ways. This requires continuous learning to be
integrated with staff and service user feedback and data driven improvements. To achieve
this, staff need to be empowered and supported by their leaders and valued by their team
members. The solutions are as much about human relationships as resources.
To help make sense of the complexity and promote a system wide approach to assure the
quality of care and care experience, a framework has been developed which brings together
key principles based on evidence and experience. The framework has been inspired by the
caring science work of Swanson (1999) that identified fives C’s of caring knowledge. These
are: commitment to values based culture; staff capability to deliver high quality care;
conditions required to deliver this care: enacting caring values, behaviours and
improvement; and measuring the consequence of caring.
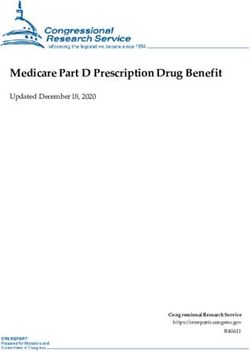
The framework (Figure One) is a continuous cycle in recognition of the need to constantly
reflect, learn and improve how we deliver healthcare as individuals, teams, and leaders
working together with service users. It recognises that there is no particular place to start.
What is important is to start somewhere and address all the issues. However, if we start
anywhere, it is with caring conversations about what matters most to service users and staff.
NHS Boards are already addressing many of the principles outlined in the framework but not
necessarily in an organisation wide manner.
The framework can inform NHS Boards’ existing governance approaches. It should help
leaders, managers and quality improvement staff understand the alignment of current
national and local initiatives, identify and address gaps systems wide, thus helping to ensure
the success of the whole system will be greater than its component parts. However, the
Assuring Care Experience Full Report6
challenges of implementation and sustainability of person centred care are not to be
underestimated.
The remainder of this report references evidence and a wealth of information about what is
taking place across Scotland to support implementation of the principles identified in the
framework and how to track their effectiveness through measurement. More detailed
definitions and examples of caring and enabling behaviours are also provided in the
Appendices together with actual stories from staff, patients and relatives to demonstrate the
impact of these behaviours. Examples of measuring tools that have been psychometrically
tested are also given in the Appendices. A summary report is available which provides an
overview of each of the 5 Cs of Caring through the evidence which underpins it, and an
overview of National Initiatives and what NHS Boards are currently doing to support
implementation of the principle.
This work was commissioned by the Scottish Government’s Directorate for the Chief Nursing
Officer, Patients, Public and Health Professions (CNOPPP), Persons Centred Delivery
Group. It was delivered under the auspices of the NMAHP Coordinating Council and NHS
Board NMAHP Directors. It is relevant across the multidisciplinary team and to both clinical
and non clinical staff. The framework is underpinned by information from a wide range of
sources including research evidence and views from the NMAHP Quality Councils; the Care
Governance Measurement work stream; NMAHP Directors; healthcare professionals,
academics and experts. It draws on the experience of other national programmes such as
Leading Better Care, Releasing Time to Care and the CARE Measure and Approach and
has informed and been informed by the National Staff Experience and Professionalism
Projects. Patients’ and Carers’ perspectives were identified from the Better Together
Programme and Leadership in Compassionate Care Programme.
Assuring Care Experience Full Report7
Figure One: Care Assurance Framework – (adapted from 5 Cs of Caring Knowledge
by Swanson 1999)
Assuring Care Experience Full Report8
3.0 HIGH QUALITY CARE AND CARE EXPERIENCE
The delivery of high quality care and a positive care experience requires a person centred
care approach to healthcare delivery. Person centred care aims to ensure service users are
at the centre of care delivery and is recognised as a multidimensional concept. While a
range of definitions exist the majority highlight the importance of flexible responsiveness;
being treated as an individual; and shared decision making (Duncan 2011). Person centred
care has been defined as “the delivery of a healthcare experience which recognises and
responds flexibly to each person as a unique individual, builds trust and empathy and
engages them in decisions which affect their healthcare and wellbeing (Scottish Government
2011).
The similarity between person centred care and caring theories has been confirmed by
McCance et al (2009) by testing the use of the Edinburgh Caring Dimension Inventory as a
way of measuring both caring and person centred care. As well as caring theories,
relationship based care and enablement concepts also represent person centred care
approaches which contribute to high quality care and care experience. In addition, other
models of person centred care, such as co-production and asset based approaches, are
being promoted. Example definitions are provided in Appendices Two and Three.
It is recognised that these different terminologies can be confusing and even within these
concepts there are few agreed definitions. When examined in more detail, many of the
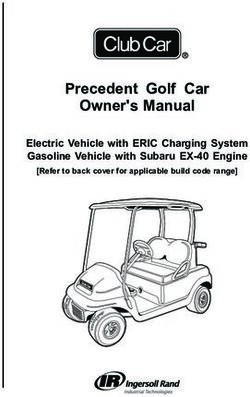
behaviours associated with these concepts overlap. To make sense of this complexity, a
thematic analysis was undertaken which focused on the similarities rather than differences,
to provide a comprehensive view of what high quality care and care experience looks and
feels like. The resulting Caring and Enabling Behaviour Descriptors are outlined in Appendix
Four. These descriptors represent a set of caring and enabling activities and the manner in
which they are to be carried out. They include expressive activities (e.g. compassion) and
instrumental activities (e.g. physical and cognitive). They reflect how we “care about”, “care
for” and “care with” our service users, their families and the multidisciplinary team to deliver
high quality care and care experience (Figure Two).
Figure Two: High Quality Care and Care Experience
Assuring Care Experience Full Report9
4.0 COMMITMENT TO A VALUES BASED CULTURE
An increasing emphasis on person centred care and the caring dimensions in health policy
have been evidenced over the last decade. Most recently, the Quality Strategy for NHS
Scotland (2010) set out its ambitions for a health service which is person centred, safe and
effective. The strategy recognised that the quality of care is at the core of patient experience
and that standards can only be effectively improved by gathering feedback on what service
users want and what they actually experience.
The commitment to high quality care focuses on the values and beliefs which underpin the
culture of the organisation. “Culture” like the concept of “care” is a word used frequently but
hard to define and a challenge to change. ‘Culture’ is an umbrella word which encompasses
a whole set of implicit, widely shared beliefs, traditions, values and expectations that
characterise a particular group of people. To an organisation, culture is what personality and
character are to the individual. Just as an individual's values and beliefs influence behaviour,
so does an organisation's culture influence the behaviour of its members (Leavitt & Bahraini,
1988).
Steins (1985) theory helpfully describes culture as having three levels. Level one:
behaviours exhibited by member of the group. Level two: the values and beliefs espoused
and which may influence behaviours. Level three: assumptions which are the unconscious
beliefs and values which also influence behaviours and are often so engrained they are not
questioned.
Managing cultural change is often suggested as a way of improving quality of care but little is
known about how best to enact this strategically. It is particularly difficult to change values
and assumptions as subcultures exist which may have conflicting interests and power levels
(Paterson et al 2011). Multifaceted approaches are indicated which start with making person
centred care an explicit organisational value or philosophy, with the involvement of staff in
developing the organisation’s vision and how to achieve it based on these values (Alimo-
Metcalfe et al 2007). In addition, enriched learning environments which understand values,
beliefs and experiences of service users, incorporating these into continuous improvement
approaches, have been shown to be enriched care environments and score high on service
user experience (Tresolini et al 1994, Boorman 2009, Brown et al 2010).
Expressing values and vision for person centred care, alongside safe and effective care, can
be undertaken at government, organisational and team level, and provide the foundation for
a values based culture. To ensure these values and beliefs are not simply espoused from
the organisations view point but actually “lived” by staff, requires identification of what is
important to service users, feedback on their care experience, staff’s views, and it is
important to both celebrate success and address potential concerns. The perception of staff
behaviours, which demonstrate those values in action, can be observed by the service user,
family members and team colleagues, and the data collected using interviews, surveys or
observation techniques. Many of these methods can be incorporated into everyday work
processes.
Assuring Care Experience Full Report10
4.1 Current enablers related to Values Based Culture
The Patient Rights (Scotland) Act 2011 was passed by the Scottish Parliament on 24
February 2011, and gained Royal Assent on 31 March 2011. The Act aims to improve
patients' experiences of using health services and to support people to become more
involved in their health and health care. It will help the Scottish Government's aspiration for
an NHS which respects the rights of both patients and staff.1
Person Centred Values are being made explicit in NHS Boards. The Golden Jubilee’s
nursing philosophy promotes both service users’ and staffs experience with “Every piece of
care matters”. The aim is to deliver the highest quality of care by recognising the importance
of both what and how care is delivered so that patients are partners and at the centre of
care. The philosophy highlights: individualised care; the environment; a culture of mutual
respect for each other; and involvement of families. The philosophy also relates to how staff
are treated: valuing each person’s contribution; encouraging innovation; mutual respect and
teamwork.
Better Together is Scotland’s Patient Experience Programme2. It aims to promote the
delivery of consistently high quality person centred care. The programme works in
partnership with NHS Boards, GP practices and other national improvement programmes to
enable the use of shared patient experience data to deliver continuous quality improvement.
An annual survey asks about service users’ perceptions of care to identify overall progress.
In addition, more detailed questions can be asked on a more regular basis to highlight
concerns and provide assurance to NHS Boards.
Caring Behaviours Assurance System 3is an approach to support improvements in care
experience. This approach was commissioned by CNOPPP, developed by Choice Dynamic
International, and tested with a number of NHS Boards. It uses a shared governance
approach to promote a quality culture. It uses multisource feedback on the presence of
caring and enabling behaviours and service user experience of Scotland’s 7 C’s to celebrate
success and identify action plans to improve caring and enabling behaviours.
Leadership in Compassionate Care programme, an NHS Lothian and Napier University
Project, promotes a number of approaches to feedback4. Staff can check regularly “What
have we got right for you? What could we have done differently?” informally to find out what
service users’ experience of care is during their stay so there is an opportunity to address
concerns, improve their experience and understand what works well for people. A more in-
depth approach to asking the patient about their experience of care is Emotional Touch
Points and Stories. Key messages are extracted from patient, family and staff stories and
discussed, enabling staff to learn from the key messages and move to action.
Observation of caring behaviours has been undertaken by Health Improvement Scotland
to support the inspection of older people’s services. NHS Tayside are adapting this tool to
observe caring behaviour, and at the same time observing direct care time observations
undertaken for “Releasing Time to Care”. Of particular importance is a caring approach to
feeding back to staff the presence, or absence, of caring behaviours. This tool could be
further developed to support individual staff multisource feedback on their caring behaviours
as part of reflective practice and performance management approaches.
1
http://www.scotland.gov.uk/Topics/Health/PatientRightsBill
2
http://www.healthcareimprovementscotland.org/programmes/patient_experience/better_together.aspx
3
http://www.knowledge.scot.nhs.uk/media/CLT/ResourceUploads/4011296/CBAS_overview.pdf
4
http://www.napier.ac.uk/fhlss/nmsc/compassionatecare/Pages/Home.aspx
Assuring Care Experience Full Report11
5.0 STAFF CAPABILITY TO DELIVER HIGH QUALITY CARE
The capability debate often centres on whether staff values and capability for caring are
innate, taught or due to having been cared for themselves. In reality, staff capabilities to
care are likely to be influenced by all these factors, both personal (personality, family history)
and professional (education or experience). Research in this area has identified five
capabilities of a caring person including compassion, empathy, knowledge, positive and
reflective (Swanson 1999). Individuals’ attributes found to impact on caring practice (in
nursing) include: interpersonal understanding, empathy, commitment and compassion
(Zhang et al 2001).
In terms of relationship based care, to work effectively staff must develop knowledge and
skills in: self-awareness and continuing self-growth; patient experience of health and illness;
developing and maintaining relationships; communicating clearly and effectively (Resoling et
al 1994). The emphasis is on one’s ability to care for oneself.
These capabilities have considerable alignment with the concept of professionalism which
research suggests incorporates a range of attributes including empathy, compassion,
understanding, patience, manners, verbal and non-verbal communication, an anti-
discriminatory and non-judgemental attitude, as well as technical competence, appearance,
image, confidence level, and appropriate physical contact (Morrow et al. 2011).
Other authors confirm these influences. Benner (1984) highlights professional maturity and
demonstrated that the ability to practice expert caring is enhanced with experience. Finfgeld-
Connette (2008) also suggests capability of staff to deliver person centred care is influenced
by professional maturity in addition to moral foundations. The former includes knowledge
base and competencies while moral foundations are concerned with ethics such as caring
enacted in a conscientious and responsible manner.
The manifestation of caring also depends on professional culture, which evidence suggests
can produce a lack of congruence between healthcare service users’ expectations and
experiences and those of staff (Cortis 2000). One study found healthcare service users
valued behaviours which recognised their individual perspective and behaviours and which
helped them anticipate and prepare for change. However, nurses placed greater emphasis
on behaviours geared more toward the comforting aspects of care by encouraging patients
to express feelings (Hegedus 1999). Another study found that nurses ranked physically
based caring behaviours higher than affective behaviours (Greenhalgh et al 1998). This
may suggest that the current model of professionalism and culture, particularly in nursing,
may need to be more explicitly aligned to models of healthcare that support enablement
This would be more aligned to asset based approaches to person centred care and co-
production. However, physically based caring activities will still be an essential requirement
for more dependent service users.
While most people who work in healthcare are likely to have caring values, clearly
articulating values of the organisation and service users in recruitment processes may
ensure staff understand what is expected of them. Organisations, including Kaiser
Permanente5, highlighted by Planetree and Picker (2008), who have successfully improved
quality of care and care experience, have included professional qualities and caring
knowledge and skills sets relevant to the position in job descriptions, online recruitment
procedures, and interview questions.
5
Transforming Services and Delivering Results through Person Centred Care
http://www.knowledge.scot.nhs.uk/qualitycouncils.aspx
Assuring Care Experience Full Report12
Dingman (2010) suggests that caring behaviours must be continually reinforced. Staff must
value and recognise their own and others’ contributions to quality of care, with each person
being responsible for contributing to the caring culture (Boykin et al 2003, Finfgeld- Connette
2008, Alimo-Metcalf et al 2007). This can be supported by aligning staff objectives with those
of the organisation and team and incorporating their review into performance management
systems (Yeakel et al 2003, Sanghavi 2006).
Yeakel et al (2003) confirmed (nurse) caring and patient satisfaction can be influenced
favourably as part of a multifaceted approach which includes learning and development.
Enriched care environments are found alongside enriched learning environments (Brown
2010, McCormack & McCance 2010). One study which examined the impact of a 15 week
degree level module on “nursing as human caring” found students experienced enhanced
relationships with others and clarification of values. Professionally, their knowledge was
increased and caring practice was enhanced (Hoover 2002). Mercer (2002) also suggests
that empathy can be improved by experiential teaching methods.
Ensuring capability of staff to deliver high quality care and care experience can be supported
by conveying expectations of professionalism and appropriate caring and enabling
behaviours as part of selection, recruiting and induction processes. Staff can be enabled to
deliver high quality care by incorporating knowledge and skills of caring and enabling
behaviours into learning and development initiatives. This includes multisource feedback of
an individual’s caring and enabling behaviours as part of reflective practice. Performance
management systems can support alignment of objectives and ensure staff are aware of
their responsibilities whilst recognising them for their contribution to care.
Assuring Care Experience Full Report13
5.1 Current Enablers for Staff Capability
Professionalism work stream of the NMAHP Co-ordinating Council is currently exploring
the concept of professionalism with a view to articulating and promoting the modern day
principles of professionalism as they relate to today’s healthcare models and the behaviours
expected of staff. Appropriate behaviours will be promoted through recruitment and
education.
Staff Governance standards have recently been revised and published. They require all
NHS Boards to demonstrate that staff are well informed, appropriately trained and
developed. The standard also requires all staff to: keep themselves up to date with
developments within the organisation, commit to continuous personal and professional
development and treat all staff and patients with dignity and respect while valuing diversity.
Dignity at Work Project exists to promote a positive working culture and behaviours across
NHS Scotland and to develop tools and behaviours which will reduce the perceived or actual
levels of bullying and harassment felt across the organisation and support all staff to feel
valued for their contribution.
CARE (Consultation and Relational Empathy) Measure and Approach are two tools
which have been developed to help practitioners reflect on practice, maintain and improve
their communication skills and use these skills to empower and enable the service users.
The CARE measure is completed by services users to provide staff with feedback on their
communication skills. The CARE approach is a web-based learning tool which supports
development of communication skills.
NHS Education for Scotland has a number of initiatives underway which will support staff
education and development in person centred care
Extra Ordinary Everyday Project is working to embed person centred care in
recruitment and retention work.
The NES website Little Things make a Big Difference provides learning resources
and links to support person centred care.
A framework has been developed to help staff enhance their practice in equality and
diversity in line with current legislation. It describes essential knowledge and skills
and acts as a tool to guide staff through the wide array of education and training
available to support Patient Focus and Public Involvement.
An educational resource is being developed to support NHS Boards and staff
prepare for the Patient and Staff Charter.
A website entitled ‘Communicating, Caring and Connecting’ has been developed to
signpost staff to the many resources available.
A rights based approach has been developed to support the care of people with
dementia. Linked to this is a revised version of Essential Shared Capabilities for
generic use in health and social care.
Spiritual Care Matters is a learning resource to support staff in spiritual care. There is
also work entitled Community Chaplaincy Listening which is supporting the
development of the role of the Chaplains in primary care.
Assuring Care Experience Full Report14
6.0 CONDITIONS REQUIRED FOR HIGH QUALITY CARE
The conditions required to deliver high quality care and care experience relate to a range of
service user, staff and organisational factors. These include service users’ health problems,
culture, age, gender, the healthcare setting and their past experiences (Finfgeld-Connette
2008). The need for staff to recognise and respond flexibly to services users’ individual
circumstances is therefore essential.
Organisational climate reflects the values and surface level culture of an organisation. A
number of studies have looked at a range of interrelated factors which promote positive
organisational climate and are described in various ways including; Forces of Magnetism6;
Positive Practice Environments7 and Climate of Care (Paterson et al 2011). The most
common factors are related to resources and relationships and include: clear vision and
shared philosophy of care; leadership; teamwork and work relationships; employee
engagement and wellbeing; and a supportive organisational context e.g. information,
education, resources and recognition.
There is some evidence that positive leadership styles lead to increases in person centred
care and patient satisfaction as well as influencing other quality ambitions such as improved
patient safety (Doran et al. 2004, McNeese-Smith 1999, Wong and Cummings 2007).
Positive leadership styles have been termed ‘transformational’ and these leaders encourage
and enable the development of an organisational culture which is characterised by integrity,
openness, transparency and genuinely valuing others. There is also evidence that
transformational leadership predicts organisational effectiveness including team
effectiveness and productivity, reduced stress, and improved job satisfaction. Important
leadership activities include balancing tensions between efficiency and safety; actively
manage change; and good knowledge management (Page 2004, Borrill et al 2005a&b,
Alimo-Metcalfe et al 2007, Cummings et al 2010).
To deliver high quality care requires a large number of health professionals with diverse
expertise to work together as a team and there is evidence that good teamwork improves not
only service users’ experience but also safe and effective care. Effective teamwork relates
to the quality of task-related and social interactions between team members and can be
judged by the impact of these interactions on both healthcare outcomes and other issues
such as staff experience, team engagement in quality improvement and performance.
(Valentine et al 2011, West et al 2006, Safran et al 2006, West et al 2005).
Improvements in healthcare quality are believed to occur because good team working
results in better decisions; coping better with complex tasks; better integrated care plans;
and better co-ordinated actions. The reasons teamwork falters in healthcare include
professional hierarchy which causes failure to engage in open conversations; frequent
transitions between care givers associated with more coordinating challenges; and general
challenges of human relationships and different personalities (Valentine et al 2011).
Employee engagement has been defined as “a workplace approach designed to ensure
employees are committed to their organisation’s goals and values, motivated to contribute to
organisational success, and are able at the same time to enhance their own sense of well-
6
American Nurses Credentialing Centre. Forces of
Magnetism.http://www.nursecredentialing.org/Magnet/ProgramOverview/ForcesofMagnetism.aspx
7
Global Health Workforce Alliance. Positive Practice Environment
Campaignhttp://www.who.int/workforcealliance/media/news/2010/ppeweblaunch/en/index.html
Assuring Care Experience Full Report15
being”. The components of employee engagement stem from four main enablers, which
relate to many of the influencing factors similar to those already identified: a strategic
narrative; engaging managers, employees having a voice: and organisational integrity
(MacLeod 2009). Evidence suggests benefits resulting from enhanced employee
engagement include: increased productivity; improved performance; reduced staff turnover;
reduced staff sickness absence; and enhanced service delivery (Price Waterhouse Coopers
2008).
Dawson (2009) includes work related injury and stress as components of staff wellbeing.
Promoting wellbeing requires both reduction in causes of injury and stress and improved
ability to deal with stressful situations, which are inevitable in the healthcare situation.
Burnout, which can result from work related stress, has been associated with sub optimal
care (Shanafet et al 2002). Finfgeld-Connette (2008) suggests the ability to manage
personal vulnerability and self-awareness were identified as significant influences on care
experience.
Sufficient resources to manage the workload and efficient work processes will inevitably
have an impact on care experience. Adequate resources and time, which include staff levels
and skill mix, have been found to impact on a range of health outcomes and service user
experience (Page 2004, Needleman et al 2003; Aiken et al 2003, Rafferty 2007, Griffith et al
2000, Kutney-Lee et al 2009). A recent study concluded that improvement in the work
environment might be a relatively low cost strategy to improve patient safety, quality of care
and patient satisfaction after it found that work environment was associated with high care
quality and patient satisfaction (Aiken et al 2012). Ultimately a positive care experience is as
much about relationships as resources. Supported by leaders and managers, staff need to
“care about,” “care for” and “care with” team members and themselves as well as service
users, their families and carers.
Assuring Care Experience Full Report16
6.1 Current Enablers for Conditions Required for High Quality Care
Leading better care8supports Senior Charge Nurses/Midwives and Team Leaders by
providing facilitation, development and educational opportunities to help them achieve high
quality, person centred, safe and efficient care for every patient, first time and every time.
This is achieved by ensuring there are better processes; effective ways of working; efficient;
and person centred care which result in more effective use of all resources.
NHS Scotland’s Strategy: Delivering Quality through Leadership 9 sets out guiding
principles for leadership in NHS Scotland. The strategy relates to both management and
leadership development, reflecting that during times of complexity and change both are
needed. Personal qualities are at the heart of the leadership qualities, and the strategy
describes a code of Personal Governance. The 360° feedback tool from the previous
leadership strategy is currently being reviewed to ensure it reflects the revised leadership
qualities and behaviours.
Effective Practitioner 10 is an initiative that supports NMAHP practitioners achieve the best
in their work. This online resource provides a foundation for work-based support including
developing effective teamwork. It provides access to a learning resource which supports a
team approach to development, which can cultivate a shared vision of quality care.
Shared Governance is an organisational model consisting of a decentralised system of
leadership in which everyone plays a role in decision making. Based on a partnership
approach, it mandates collaboration among team members and gives individuals a high
degree of autonomy at all levels of staff. It is currently being used as an approach to
engaging staff across Scotland in the NMAHP Quality Councils and some NHS Boards.
NHS Employers Staff Engagement Toolkit 11outlines five employee engagement drivers
including: delivering great management and leadership; enabling involvement in decision
making; promoting a healthy and safe work environment; ensuring every role counts; and
supporting personal development and training.
Scotland’s National Staff Experience Project is working closely with the Person Centred
Delivery Group to promote measurable improvement and interventions which can help
strengthen ‘staff experience’ to promote staff health and wellbeing and ultimately a good
person centred healthcare experience for service users and their families. This will include
measurement and interventions related to staff engagement and staff resilience.
Nursing and Midwifery Workforce Development project, which commenced in July 2003,
was commissioned by The Facing the Future group to examine the then current situation in
nursing workload and workforce planning in Scotland. The recommendations from the
project lay the foundation for the development of a more systematic and standardised
approach to nursing and midwifery workload and workforce planning across Scotland.
HeartMath® programme, ‘Transforming Stress and Revitalising Care’ is an approach to
supporting staff resilience. The programme teaches staff simple skills, supported by unique
tools and proprietary technology all designed to boost performance, increase resilience,
vitality and productivity while reducing stress. This and its impact and sustainability are
currently being tested in 5 NHS Boards in NHSScotland.
8
http://www.evidenceintopractice.scot.nhs.uk/leading-better-care.aspx
9
http://www.scotland.gov.uk/Publications/2009/10/29131424/0
10
http://www.effectivepractitioner.nes.scot.nhs.uk/Default.aspx
11
http://www.nhsemployers.org/EmploymentPolicyAndPractice/staff-engagement/staff-engagement-
toolkit/Pages/Staff-engagement-toolkit.aspx
Assuring Care Experience Full Report17
7.0 ENACTING CARING VALUES, BEHAVIOURS AND IMPROVEMENT
Caring, like care, can be viewed in multiple ways. It can be an attitude or ability, an attribute
or characteristic or a complex set of behaviours. In healthcare it is all of these and it has
been suggested that the presence of caring is the ultimate determinant of patient experience
(Watson 2006). Patient experience is influenced by many factors including: what staff are
like; what they do; and how these factors impact on what services users are enabled to be or
do (Entwistle et al 2011). Many of these factors are aligned with caring and enabling
behaviours. To make sense of the wide range of theories and concepts which make up
person centred care and impact on care experience, a thematic analysis was undertaken to
identify common caring and enabling attributes and behaviours which were then mapped to
Scotland’s 7 Cs, defined by the people of Scotland as high quality healthcare (Figure three).
This work was validated by the NMAHP Person Centred Quality Council and the resulting
caring and enabling behaviour descriptors can be used to support staff enact caring values
and behaviours and continuously seek to improve the care experience (Appendix Four).
Figure three: Attributes of caring and enabling behaviours
Many of these behaviours interrelate to achieve a high quality care experience.
Communication behaviours, in particular attitude, play a big part in enabling staff to connect
with patients and determine how approachable and trustworthy staff are (Cole & Bird 2000).
This trust encourages patients to share personal information (Arnold and Boggs 2003). This
requires listening behaviours to ensure staff understand what service users value in their life,
how they make sense of what is happening and what they want to achieve in relation to their
health (McCormack 2010, Davis 2006). In addition, empathy which includes understanding a
person’s situation, perspective and feelings, is essential for enablement to take place
(Mercer et al 2002). Finally, a positive attitude by healthcare staff encourages patients to see
a clear way ahead of them (Little et al 2001).
Overall these attributes and behaviours provide the foundation for an effective therapeutic
relationship between the clinician and service user. An effective therapeutic relationship has
been found to improve engagement, self-management and health outcomes in addition to
care experience (Mercer 2002, Robertson 2008, Wolf 2008, Calnan & Row 2009, Goodrich
2009, Parsons 2010). These behaviours can also be enacted even at the briefest contact
with a service user by both clinical and non clinical staff.
Assuring Care Experience Full Report18
Which caring and enabling behaviours are relevant to enact may differ depending on the role
of staff performing them and patient characteristics. For example, we know that older people
want to remain independent as long as possible. For many, exercising this choice remains a
reality but, for others, frailty and illness pose a threat to maintaining independence and
wellbeing (RCN 2004). In these circumstances “caring for” may be more relevant than
“caring with” but both require staff to “care about” Whilst nurses may enact comforting,
assisting and enabling behaviours, Allied Health Professionals will focus mainly on enabling
behaviours and Doctors may, for example, focus mainly on communication and co-
ordination.
Increasingly, evidence suggests that focusing on improving caring behaviours can be key to
ultimately improving care experience. One organisation which introduced a care model
based on Swanson’s (1991) caring theory and relationship based care found that patient
experience scores, which had remained around the same level despite multiple efforts to
improve, began the first steady and sustained climb in 6 years and quickly exceeded the
target goal (Tonges & Ray 2011). Similar results were found at Kaiser Permanente when
they introduced a caring science model, which included education in caring science,
HeartMath® to support staff resilience, and articulated caring behaviours in recruitment and
selection processes12. Both organisations tracked nurse sensitive outcomes which related to
safe and effective care and found these also improved.
Person centred processes and practice examples, which support staff to enact caring values
and behaviours and improve service users care experience, have been identified from the
literature and good practice in place across NHS Scotland (Appendix four). Many of these
practices have been linked to the various caring and enabling attributes they impact on
within the 7 C’s. These practices has been evaluated and found to improve the quality of
care experience as well as safety and effectiveness in some cases. They can be introduced
using the PDSA cycle, promoted by Healthcare Improvement Scotland13
12
Transforming Services and Delivering Results through Person Centred Care
http://www.knowledge.scot.nhs.uk/qualitycouncils.aspx
13
http://www.healthcareimprovementscotland.org/programmes/patient_safety/tissue_viability_resources/plan_do_
study_act_pdsa.aspx
Assuring Care Experience Full Report19
7.1 Current Enablers for Enacting Caring Values, Behaviours and Improvement
The Caring Behaviours Assurance System 14 promotes the development of action plans
which are agreed by the team following multisource feedback on the presence of caring and
enabling behaviours across the 7 C’s. This supports celebration of successes and changes
to practice which improve the quality of care and care experience.
Leadership in Compassionate Care programme (LCCP) was a 3 year action research
study underpinned by relationship centred care and appreciative inquiry undertaken by NHS
Lothian and Edinburgh Napier University. It aimed to develop and embed compassionate
care in both clinical practice and education. The LCCP focused on identifying and testing out
key processes which enable compassionate care to happen more of the time with staff,
patients and families across a range of care settings. A framework developed from the
analysis and identifying compassionate caring practice is:
Caring conversations: discussing, sharing, debating and learning how care is
provided, amongst staff, patients and relatives and the way in which we talk about
caring practice.
Flexible, person centred risk taking: making and justifying decisions about care in
respect of context and working creatively with patient choice, staff experience and
best practice.
Feedback: Staff, patients and families giving and receiving specific feedback about
their experience of care.
Knowing you, knowing me: developing mutual relationships and knowing the
person’s priorities, to enable negotiation on the way things are done.
Involving, valuing and transparency: creating an environment throughout the
organisation where staff, patients and families actively influence and participate in the
way things are done.
Creating spaces that work: the environment: considering the wider environment and
where necessary be flexible and adapt the environment to provide compassionate
care.
Releasing Time to Care focuses on redesigning work processes and environments to
improve efficiency and help NMAHPs spend more time on direct patient care. This approach,
which focuses on releasing time, is complementary to approaches which improve caring and
enabling behaviours such as the Caring Behaviours Assurance System.
Person Centred Processes and Practice which support staff enact caring and enabling
behaviours and improve service users care experience, have been identified from the
literature and good practice in place across NHS Scotland. These practices have been
linked to the various caring and enabling attributes upon which they impact within the 7 C’s.
The effectiveness of some of these practices has been evaluated and shown to improve
care experience as well as safety and effectiveness. They can be introduced using the
PDSA cycle, promoted by Healthcare Improvement Scotland (Appendix five).
Scottish Person Centred Intervention Collaborative (ScoPIC) is a research project being
conducted by the NMAHP research unit. It will examine interventions which improve person
centred healthcare experience including RTC, CBAS and HeartMath®, to define the
interventions, how they impact on patient experience and outcomes, and how context might
affect their impact. It will also test aspects of care governance measurement framework, in
particular the real time data collection and reporting of patient reported experience
measures.
14
http://www.knowledge.scot.nhs.uk/media/CLT/ResourceUploads/4011296/CBAS_overview.pdf
Assuring Care Experience Full Report20
8.0 MEASURING THE CONSEQUENCE OF CARING
Measuring caring and enabling behaviours and their consequence in terms of care
experience is challenging. The person centred nature of these behaviours means the
relevance of enactment is likely to be different for different people. This, together with the
complexity and interrelationship of the factors that influence their enactment, adds to the
research and improvement challenge. A scoping of the literature revealed, however, that
there are studies that point us in the direction we need to go. In addition, it appears that if
we make improvements in certain areas which impact on service users’ experience, these
can also impact on other areas which further improve that experience. For example, a
positive patient experience, as measured by caring and enabling behaviours has been found
in hospitals with better work environments (Aiken et al 2012, Kutney Lee et al 2009). Good
work environments are influenced by positive leadership, effective team working and
education and development (Alimo Metcalf 2007, Page 2004). These factors also influence
staff health and wellbeing (West et al 2005, Borrill et al 2005b). Staff health and well-being
impacts, not only on patient satisfaction (Dawson 2009), but on all three dimensions of
quality (Boorman 2009). Success breeds success.
There are also a number of studies which examined specific caring and enabling behaviours
and found links to a range of health outcomes and quality of life issues including: a reduction
in anxiety levels; and improvements in service users’ involvement in their treatment; health
promoting activities; and self-management. This suggests that caring and enabling
behaviours are required across the spectrum of healthcare needs as an adjunct to technical
interventions and are especially important when cure is no longer an aim of healthcare for
people with long term conditions or older people.
Consequently there are indications that a good care experience for service users, influenced
by staff’s caring and enabling behaviours, together with those factors that influence the
ability of staff to enact them, can improve service users well-being and support their effective
engagement in decisions and actions that impact on their ability to stay healthy or return to
health and, ultimately, improve organisational performance.
Improving service users’ experience has been shown to result in:
reduced levels of anxiety which can lead to improved healing rates, reduction in
hypertension and the need for medication for pain relief;
improved emotional and spiritual wellbeing;
improved trust in the health services and closer family relationships
(Swanson 1999, Erci et al 2003, Chang et al 2005, Goodrich & Cornwell 2009, Calnan &
Rowe 2009).
Effective engagement of service users is supported, leading to:
increased service users’ recall and confidence to manage appropriate treatment;
better involvement with health promotion activities, treatment, monitoring, self-
management.
(Mercer et al 2001, Coulter & Ellis 2006, Robertson et al 2008, Goodrich & Cornwell 2009).
Organisational performance is improved through:
improved patient safety demonstrated by a reduction in mortality, morbidity and
adverse events;
reducing hospitalisation and length of stay;
improved staff experience, health and wellbeing leading to reduced intention to leave
and absence rates
(Swanson 1999, Saultz et al 2005, West et al 2005, Safran et al 2006, Goodrich & Cornwell
2008, Dawson 2009, Valentine et al 2011).
Assuring Care Experience Full Report21
In order to provide assurance of the presence of caring and enabling behaviours, their
impact and how to improve them requires measurement and data driven improvements. This
involves; identification of relevant metric; seeking regular feedback from service users and
staff; access to real time or near real time information to highlight concerns and provide
assurance; effective and efficient knowledge management systems; and feeding back
information to staff to drive improvement plans. (Davies 2005, Griffith et al 2008, Pencheon
2010).
Informatics principles and a measurement framework are proposed to support measurement
and data driven improvements for assuring care experience whilst recognising the data
burden. While these principles may seem fairly obvious, there are still significant challenges
in their implementation which relate to information technology and education to support
metric identification, collection, reporting and use. The principles are:
What should be measured.
• Direct care quality, what influences this and its impact.
• Evidence based priorities.
• What is important to service users and professional values.
• National shared data where evidence is unquestionable or when learning is
supported by benchmarking.
• Local data as necessary.
How data should be collected.
• Quantitative and qualitative methods.
• Valid and reliable tools with clear unambiguous data and metadata.
• Current data should be better used, and where possible data should be collected
once and used for multipurpose.
• The frequency of collection should allow for introduction of improvement intervention
and be reduced when sustained improvement is achieved.
Reporting and use
• Information should be made accessible to staff in near real time, at team level, be
easy to understand and shared openly.
• Regular review of usefulness of data collected.
The measurement framework proposed is shown in Figure Four. The measurement
framework helps to make sense of the complexity of healthcare by outlining the variables
which describe quality healthcare; expected outcomes; what influences its delivery; and their
interrelationships. It is aligned with data at level three to the National Quality Measurement
Framework and Boards can use it to guide the identification of quality metrics for inclusion
within their quality dashboards. Only one or two measures need be collected in each theme
as required with the exception of outcome themes which need to be collected more regularly
depending on the service being measured. All measures should build on current national
and local measurement, for example LBC15, the SPSP16 and the CARE Measure17 and
address gaps, particularly around person centred care. Following a review of measures in
use and available to support the measurement framework it was noted that there are
particular gaps in measures of caring and enabling behaviours. However, no one tool exists
which has been validated for the multidisciplinary team, for all settings, and service users
groups and development work is required. Example measures available are highlighted in
Appendix Six.
15
Leading Better Care/Releasing Time to Care. http://www.evidenceintopractice.scot.nhs.uk/leading-
better-carereleasing-time-to-care.aspx
16
Scottish Patient Safety Programme. http://www.patientsafetyalliance.scot.nhs.uk/programme
17
CARE Measure
http://www.gla.ac.uk/departments/generalpracticeprimarycare/research/caremeasure/
Assuring Care Experience Full ReportYou can also read