Operational Guidance for Continuity of Essential Services Impacted by COVID-19 - A practical guide for program implementation and adaptation - Jhpiego
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Operational Guidance for Continuity of Essential Services Impacted by COVID-19 A practical guide for program implementation and adaptation
June 2020 Cover photo: National Health Ministry, Government of Assam, India Jhpiego is a nonprofit global leader in the creation and delivery of transformative health care solutions that save lives. In partnership with national governments, health experts and local communities, we build health providers’ skills, and we develop systems that save lives now and guarantee healthier futures for women and their families. Our aim is revolutionizing health care for the planet’s most disadvantaged people. Jhpiego is a Johns Hopkins University affiliate. Published by: Jhpiego Corporation Brown’s Wharf 1615 Thames Street Baltimore, Maryland 21231-3492, USA www.jhpiego.org © Jhpiego Corporation, 2020. All rights reserved.
Table of Contents Acknowledgments ...................................................................................................................... iv Abbreviations .............................................................................................................................. v Impact of COVID-19 on Global Health Indices................................................................................ 1 The Time to Act Is Now! ............................................................................................................... 1 Critical Considerations ................................................................................................................. 3 How Is This Guidance Organized? ................................................................................................. 5 Context and Assumptions............................................................................................................. 6 Prioritize Essential Health Services and Adapt to Changing Contexts and Needs............................. 7 Optimize Service Delivery Settings and Platforms ....................................................................... 10 Establish Effective Patient Flow (Screening, Triage, and Targeted Referral) at All Levels............... 17 Model of Effective Facility Patient Flow (Screening, Triage, and Targeted Referral) at Facility or Community Outreach................................................................................................................. 20 Rapidly Optimize Health Workforce Capacity.............................................................................. 21 Critical Health Workforce Considerations.................................................................................... 25 Maintain the Availability of Essential Medications, Equipment, and Supplies............................... 26 Global Guidance and Resources.................................................................................................. 29 Operational Guidance for Continuity of Essential Services Impacted by COVID-19 iii
Acknowledgments This guidance is the result of the combined efforts of many people, all of whom deserve special thanks for their contributions and commitment. Jhpiego wishes to acknowledge and thank the following for their role in the technical development and drafting of operational guidance content: Radha Karnad, Myra Betron, Meghan Greeley, Ricky Lu, Megan Christofield, Susheela Engelbrecht, Christopher Morgan, Chandrakant Ruparelia, Stacie Stender, Silvia Kelbert, Katherine Wolf, Gladys Tetteh, Julia Bluestone, Leah Hart, Jennifer Breads, Peter Jackson, Erica Troncoso, Rajat Chabba, and Somesh Kumar. Thank you to Abbey Becker, Courtney Weber, and Young Kim for their help producing this document. iv Operational Guidance for Continuity of Essential Services Impacted by COVID-19
Abbreviations ANC antenatal care ART antiretroviral therapy ARV antiretroviral CHW community health worker ENC essential newborn care FP family planning GBV gender-based violence HTS HIV testing services IPC infection prevention and control IPTp intermittent preventive treatment of malaria in pregnancy IRS indoor residual spraying ITN insecticide-treated net KMC kangaroo mother care KP key population LARC long-acting reversible contraception MNH maternal and newborn health PLHIV people living with HIV PNC postnatal care PPE personal protective equipment PrEP pre-exposure prophylaxis SRH sexual and reproductive health STI sexually transmitted infection VMMC voluntary medical male circumcision WHO World Health Organization Operational Guidance for Continuity of Essential Services Impacted by COVID-19 v
vi Operational Guidance for Continuity of Essential Services Impacted by COVID-19
Impact of COVID-19 on Global Health Indices
Beyond its direct effect on
mortality, the COVID-19 pandemic “A well organized and prepared health system has the
is disrupting the provision of capacity to maintain equitable access to high-quality
health care services globally, essential health services throughout an emergency,
resulting in an increase in the limiting direct mortality and avoiding indirect
number of deaths from non- mortality.”
COVID-19 causes. –Maintaining essential health services: operational
guidance for the COVID-19 context, interim guidance
Hard-earned global health gains from the World Health Organization (June 1, 2020)
are being reversed, with health
inequalities widening, as
resources meant for routine health programming and health service delivery are directed toward
the pandemic.
The Time to Act Is Now!
Countries and global health
programs are making difficult “High-priority categories include:
decisions to balance the demands • essential prevention and treatment services for
of responding directly to communicable diseases, including immunizations;
COVID-19 while simultaneously • services related to reproductive health, including
engaging in strategic planning and during pregnancy and childbirth;
coordinated action to maintain • core services for vulnerable populations, such as
essential health service delivery, infants and older adults;
mitigating the risk of system • provision of medications, supplies and support from
collapse. health care workers for the ongoing management of
chronic diseases, including mental health conditions;
The World Health Organization • critical facility-based therapies;
(WHO) released operational • management of emergency health conditions and
guidance that included a set of common acute presentations that require time-
targeted immediate actions that sensitive intervention; and
countries should consider at • auxiliary services, such as basic diagnostic imaging,
national, regional, and local levels laboratory and blood bank services.”
to reorganize and maintain access
–Maintaining essential health services: operational
to essential, high-quality health
guidance for the COVID-19 context, interim guidance
services for all (June 1, 2020). Ten
from the World Health Organization (June 1, 2020)
key priorities in the WHO
guidance are:
Adjust governance and coordination mechanisms to support timely action.
Prioritize essential health services and adapt to changing contexts and needs.
Optimize service delivery settings and platforms.
Establish safe and effective patient flow at all levels.
Rapidly optimize health workforce capacity.
Maintain the availability of essential medications, equipment, and supplies.
Fund public health and remove financial barriers to access.
Strengthen communication strategies to support the appropriate use of essential services.
Strengthen the monitoring of essential health services.
Use digital platforms to support essential health service delivery.
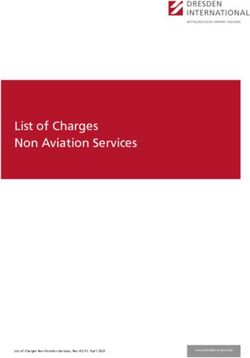
Operational Guidance for Continuity of Essential Services Impacted by COVID-19 1The global health community’s response to this pandemic presents an unprecedented opportunity to reinvigorate health systems strengthening measures that prioritize
decentralized, community-based, and client-focused mechanisms for accessing health products, services, and information, as traditional modalities for accessing these may
be compromised and disrupted due to COVID-19.
Client/Patient
Products Services Information
Door-to- Visit Health Provider Visits Need Additional
Visit Facility Self-Care
Door Access Facility/Provider You Information
Key Decisions
Key Decisions
Type of facility: public/private?
Type of products required:
Level of facility: primary/secondary?
OTC vs. prescription, essential vs. nonessential
How to triage? When to visit?
Existing knowledge about usage and adoption
Map: space, staff, supplies, and systems?
When to buy, how to get it to you? How to buy?
Type of provider
Authenticity of products?
Key services available?
Establish authenticity and credibility of service
How to Increase Surge Capacity? provider/information/tools?
Online Marketplaces Leverage Online Symptom Mapping of Private- Virtual Approaches Leverage Telehealth Solutions
Checkers Sector Resources (Telemedicine)
Innovative Service Delivery Models Connect to Relevant Portals/Helplines
Leverage Telehealth Strategic Purchasing Access to Personal
Mapping of Private-Sector Solutions of Services Protective Equipment Maximize Community and Civil Society
Organization Engagement
Resources
Pooled Procurement/ Connectivity, Digital Literacy,
Innovative, Technology-Enabled Capacity-Building of Health Providers
Volume Guarantee Devices
2 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Critical Considerations
Children
Children are particularly vulnerable when health resources or social structures are stressed.
Lack of access to preventive or curative health care, food, and other factors that contribute to
healthy development can have lasting consequences on growth and well-being.
Every child health encounter should be maximized for preventive care, such as by combining
growth assessments, checks for illness, and/or screening for abuse with vaccination visits.
Adolescents and Youth
Changes to service delivery may particularly impact adolescent girls and youth. These changes
may result in increased sexual exploitation and abuse, gender-based violence (GBV), poor
educational outcomes, adolescent pregnancies, and unequal access to information.
While the technical components of service delivery may remain the same, alterations to the
mode of delivery may be needed to ensure all needs are met.
Programs should advocate for waiving restrictions, such as age or marital status, parental or
spousal consent, and costs, to facilitate adolescents’ and youth’s access to sexual and
reproductive health (SRH) and HIV services.
For more information on adolescent and youth health service considerations, see p. 26–28 of
WHO’s Maintaining essential health services: operational guidance for the COVID-19 context
(June 1, 2020). The United Nations Population Fund’s COVID-19 preparedness and response
interim technical brief on adolescents and young people (March 24, 2020) and WHO’s
Q&A: Adolescents, youth and COVID-19 (May 4, 2020) may also be helpful.
Gender
SRH and rights is a significant public health issue that requires extra attention during pandemics.
Safe pregnancies and childbirth depend on functioning health systems and strict adherence to
infection prevention. Provision of family planning (FP) and other SRH commodities, including
menstrual health items, are central to women’s health, empowerment, and sustainable
development, and may be impacted as supply chains undergo strains from pandemic response.
Obstacles and barriers must be addressed to ensure that women and girls can access services,
including psychosocial support services, especially those who are subject to or may be at risk of
violence in quarantine. Pandemics make existing inequalities for women and girls worse,
including increasing the risk of intimate partner and domestic violence.
Women represent 70% of the health and social sector workforce globally. Their work on the
frontlines means they face a higher risk of exposure to COVID-19. Special attention should be
paid to how their work environment may expose them to discrimination and should address
their SRH and psychosocial needs as frontline health workers.
As the majority of the health and social sector workforce, women should be adequately
represented in the leadership, policymaking, and action-planning for national COVID-19
responses. See the United Nations Population Fund’s COVID-19: A Gender Lens: Protecting
Sexual and Reproductive Health and Rights, and Promoting Gender Equality (March 2020).
Operational Guidance for Continuity of Essential Services Impacted by COVID-19 3Infection Prevention and Control
This guidance does not address infection prevention and control (IPC) and the use of personal
protective equipment (PPE) in detail. Reference to additional IPC/ PPE guidance in highlighted
throughout the document.
To guarantee the safe delivery of services, the minimum requirements for IPC must be
established.
Adherence to standard precautions for all patients at all times should be strengthened,
particularly regarding distancing, hand hygiene, the appropriate use of PPE, and surface and
environmental cleaning and disinfection.
Additional IPC measures will depend on the local COVID-19 transmission scenario and the type
of contact required by the activity.
It is key that health care providers and community health workers (CHWs) be trained on
COVID-19 prevention and use PPE based on situation.
4 Operational Guidance for Continuity of Essential Services Impacted by COVID-19How Is This Guidance Organized?
Each section/chapter addresses one of the service delivery key priorities from the WHO Maintaining essential health services: operational guidance for the COVID-19
context (June 1, 2020).
Cross-cutting guidance for each service delivery key priority that applies across all technical areas is presented first.
Within each chapter/ section, each column highlights the specific guidance for a technical area (SRH/FP, MNH, Immunization, GBV, TB and HIV, Malaria)
Focus of this operational guidance: service delivery interventions
Prioritize Strengthen
Adjust essential communicati
Maintain the Fund public Strengthen Use digital
governance health Optimize Rapidly on strategies
Establish safe availability of health and the platforms to
and services and service optimize to support
and effective essential remove monitoring of support
Key Priority coordination adapt to delivery health the
patient flow medications, financial essential essential
mechanisms changing settings and workforce appropriate
at all levels equipment barriers to health health service
to support contexts and platforms capacity use of
and supplies access services delivery
timely action needs essential
services
Guidance must be contextualized and finalized with in-country
decision-makers, in line with national guidance and priorities.
5 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Context and Assumptions
The focus of this Jhpiego operational guidance is how to adapt and implement the five service
delivery priorities listed in WHO’s Maintaining essential health services: operational guidance for the
COVID-19 context (June 1, 2020):
Prioritize essential health services and adapt to changing contexts and needs (the what of
service continuity).
Optimize service delivery settings and platforms.
Establish safe and effective patient flow at all levels (the where of service continuity).
Rapidly optimize health workforce capacity (the who of service continuity).
Maintain the availability of essential medications, equipment, and supplies (the with what of
service continuity).
These priorities rely on strong system governance, coordination, and financing mechanisms.
Communications strategies need to be strengthened to support the appropriate use of essential
services. This guidance does not include specific content for communications with clients and
communities about the changes to service delivery addressed—which is beyond the scope of this
guidance at this time—but it is critical to inform and engage clients and communities.
Further relevant resources are included as hyperlinks, both to technical guidance and approaches to
operationalize them (e.g., telehealth/digital health and self-care).
The content of this guidance will need to be contextualized and finalized with in-country
decision-makers, in line with national guidance and priorities.
This guidance does not specifically address how to strengthen essential health services monitoring.
There is a critical need to monitor and work with countries to draft, develop, and use context-
relevant data to understand the impact of COVID-19 on health service uptake, delivery, and quality;
evidence-based operationalization, prioritization, and adaptation for continuity of services; and
measuring performance and outcomes.
6 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Prioritize Essential Health Services and Adapt to Changing Contexts and Needs
SRH/FP Maternal and Newborn Health Immunization GBV TB and HIV Malaria
(MNH)
Contraceptive education and Individualized counseling, • Newborn and child Identify and inquire about • Targeted HIV testing • Core preventive and
counseling preparation of birth immunizations given GBV with standard services (HTS), case management
• Group education preparedness/complication as per schedule; protocol. including targeted interventions
(facility/community) readiness plans (adapted to newborn provider-initiated HIV
change in services), and advice First-line support for GBV:
• Intermittent preventive
• Counseling for new vaccinations after testing and counseling treatment of malaria in
on self-care, in addition to delivery; zero-dose • Listen closely without
clients • Same-day pregnancy (IPTp; see
COVID-19-specific messages vaccination (oral judgment.
• Counseling for antiretroviral therapy Delivery of Community
See Providing Antenatal Care polio vaccine,
continuation, follow-up, Counseling in the Context of
• Inquire about needs (ART) initiation for all Intermittent Preventive
hepatitis B, and and concerns. newly diagnosed with Treatment in
side effect management, COVID-19. Bacille Calmette- HIV Pregnancy in the
and routine check • Validate experiences.
Guérin) per national Context of COVID-19)
Essential and emergency • Enhance safety (safety • Optimized ART
immunization
Contraceptive service maternal care interventions schedule) planning). regimens and • Distribution of
delivery • appropriate dosing for insecticide-treated nets
Screening/management of • Primary series • Connect clients with
• Minimum service all people living with (ITNs) through
anemia, pre-eclampsia/ vaccinations, additional services.
package that would allow HIV (PLHIV) antenatal care (ANC)
eclampsia, sexually
for access to safe
especially for • Provide care for • Treatment support for and growth
transmitted infections measles-rubella- or
contraception and FP injuries and urgent all PLHIV groups monitoring/vaccination
(STIs)/HIV, TB, GBV, poliomyelitis- medical treatment. • Intermittent preventive
based on informed infection, • 12-monthly viral load
containing vaccines
decision-making. antenatal/postpartum treatment in infants
and other Minimum package of post- • Children and
• For interval FP care: hemorrhage, and labor and combination vaccines rape care: adolescents in • Seasonal malaria
- For new long-acting childbirth complications chemoprevention for
• Vaccination for • Counseling orphans and
reversible • Preventive measures per diseases with risk of vulnerable children young children
contraception (LARC) country guidelines • Rapid HIV testing with
programs • Vector control
outbreaks: measles,
clients, discuss and referral to care and
• Auxiliary services: polio, diphtheria, and • HIV self-testing activities, including
offer interim treatment, as
ultrasound, laboratory yellow fever including for sexual ITNs and indoor
contraceptive appropriate
residual spraying (IRS)
options.
7 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP Maternal and Newborn Health Immunization GBV TB and HIV Malaria
(MNH)
- Defer permanent services, and blood bank • Pneumococcal, • Post-exposure partner/contacts of campaigns across
methods and discuss services meningococcal, and prophylaxis if the index cases communities and
interim • Registration of maternal seasonal influenza individual is reached • Continued access to households
contraceptive deaths vaccines for within the first 72 pre-exposure
options until elective Essential and emergency vulnerable population hours prophylaxis (PrEP) for
procedures restarts. newborn care interventions groups • STI screening/testing those at elevated risk
- Consider delay of • Initiation of skin-to-skin and treatment of HIV
long-acting methods contact and early and • Key population (KP)
• Emergency
(implant/intrauterine exclusive breastfeeding services
contraception if the
device) removal with
• Screening/management of individual is reached in • Voluntary medical
use of another
asphyxia, congenital the first 120 hours male circumcision
method of
anomalies, birth injuries, (VMMC)
contraception to
infection, feeding problems, postoperative follow-
avoid pregnancy at
breathing difficulties, up (delay new VMMCs
this time.
hypo-/hyperthermia, and if guidance about
• Maximize immediate preterm or low-birthweight mass gatherings
postpregnancy newborns cannot be followed)
(postpartum and
• Prophylactic treatment as • Process for
postabortion) methods
indicated: antibiotics, prioritization of clients
to be initiated prior to
antiretroviral (ARV) dugs, TB in need of intensified
discharge from a facility.
drugs virtual or in-person
LARC continues to be an
• Essential care: oral polio, support (poor
option for use.
Bacille Calmette-Guérin, and adherence, pregnant
hepatitis B vaccinations; and breastfeeding
thermal protection; eye and women living HIV,
cord care; and vitamin K etc.)
• Individualized counseling • TB symptom
messages for screening of PLHIV
parents/caregivers and others at
increased risk
8 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP Maternal and Newborn Health Immunization GBV TB and HIV Malaria
(MNH)
• Registration of all births, • TB diagnosis
regardless of place of birth (molecular where
• Registration of perinatal available), TB contact
deaths tracing, TB treatment
initiation, and
• Consider COVID-19 sentinel
continuous adherence
surveillance by testing
support
women at a few facilities.
9 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Optimize Service Delivery Settings and Platforms
Consider optimal service delivery setting and platform for each service to minimize clients’ and health care workers’ exposure. This may vary depending on availability of
service locations to safely provide services, disruptions to movement and transport, need to limit nonessential facility-based encounters, and local policy and guidance.
Facility-based services should be delivered remotely where appropriate and feasible. Where feasible, services that would routinely be delivered across multiple visits should
be integrated.
Where necessary, community events should be organized in a manner that minimizes the gathering of people (i.e., social distancing and limiting numbers), and participants
should use available PPE.
Be prepared to shift rapidly to providing care through alternative ways by creating effective response plans (e.g., by ensuring frontline health care workers have phones and
can charge them). Protocol to ensure continued safe document storage in case of sudden lockdown.
Adapt monitoring and tracking tools for capturing changes and progress in project implementation; guide programmatic course correction as needed.
SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
Remote Remote Remote Remote Remote Remote Remote Remote
See Ensuring Quality • Assess risk: • Triage and • Triage and • Provide family • Outreach
• Information, • Virtual HTS
Family Planning co-morbidities; advice for provide advice reminders of services/
adherence • Differentiated
Services during under- or women who on concerns or the importance mobile clinics,
support, and models of care
COVID-19 Pandemic. overweight; think they are in preoccupations of routine particularly to
referral for
• Explore and use < age 19; labor and danger immunization, • Mobile health expand access
services
phones and tobacco, signs. by SMS and strategies to ANC/IPTp
other digital alcohol, or other where feasible
• Provide
technologies for other substance communication to provide
counseling on
screening, use; mental means. clinical care and
FP, pregnancy
triaging, ad health proactively
spacing, and
referral for conditions communicate
complication
with PLHIV
10 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
care; education (e.g., anxiety, readiness plan using positive
and counseling depression); (adapt for messaging
when feasible; GBV; and other changes to about the need
responding to vulnerable services). to stay healthy
questions about groups • Advise on self- and adhere to
method use, • Triage and care. ART
side effects, and provide advice • Phone calls to
management,
• Advise on visit
on common schedule, reach contacts
and supporting discomforts, of index cases.
newborn
client continue concerns or
using the
vaccinations, • Telephonic
preoccupations, etc. VMMC
method; and and danger consultation as
information and signs. an initial
accessing
resupply of
• Provide screening,
counseling on before an in-
short-acting
FP, pregnancy person visit
methods, such
spacing, and • Empowering
as condoms,
pills, and birth clients
preparedness/ themselves to
subcutaneous
complication provide peer
depot
readiness plan support
medroxyproges
(adapt for
terone acetate.
changes to
• Establish services).
telehealth
mechanisms for
• Advise on
individual self-care.
counseling of • Advise on visit
adolescents schedule based
that adhere to on risk
11 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
the principles of assessment.
confidentiality Prioritize third-
and trimester visits.
noncoercive
decision-
making.
Community-based Community-based Community-based Community-based Community/ Community-based Community-based Community/
• Increase visits with a trained providers visits with a trained household-based • CHWs to • Maximized use household
availability of CHW using point-of- • Triage and CHW: • Avoid/postpone provide first- of HIV self- • Provide malaria
methods care devices: advice for • Visits at 48–72 mass vaccination line response to testing for case
requiring less • Discontinuation women who hours and 7–14 campaigns GBV, with targeted management,
contact with of group ANC think they are in days temporarily special community including
health care • Visits at 20, 26, labor • Integrated where there is attention on testing testing and
workers 34, and 38 • Maternity management of no active ensuring privacy • Community- treatment. Do
through weeks waiting homes newborn illness outbreak of a and based testing, not to suspend
pharmacies, (where they vaccine- confidentiality, including for the planning for
• Advice on • Follow-up of
CHWs, and exist): Follow preventable and measures KPs and rapid or
common problems/
other outlets. appropriate IPC disease. to keep ART initiation implementation
discomforts infections/illnes
• Increase guidance. • In the event of themselves safe of vector
• Voluntary ses being • Differentiated
control
availability and • Safe transport managed by a an outbreak, service delivery
access to counseling and consider rapid activities,
testing for HIV, to care for skilled provider models for
contraceptives vaccination including ITN
syphilis, women and • Support for community
that can be campaigns after and IRS
hepatitis B newborns continued distribution and
used by the a careful risk campaigns.
kangaroo adherence
client without • Hemoglobin, analysis that support to
urinalysis with mother care
service provider considers both orphans and
urine dipsticks, (KMC) in the
support, the potential vulnerable
rapid test for home
including impact of the children;
malaria outbreak and the services
12 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
various self-care • Follow-up of • Distribution of possibility of provided
methods. problems/ 2–3 months of adapting through home
• Ensure infections/ micronutrient campaign visits only if a
availability of illnesses being supplements procedures to critically ill
in-person managed by a and ARV drugs ensure staff and beneficiary
contraceptive skilled provider families’ safety. urgently needs
• Distribution of
transport; a
services • Distribution of mebendazole • Refer to the
(including both WHO framework child or adult
2–3 months of and ITNs
information and for decision- exposed to
micronutrient • Short-acting
methods) making on physical harm,
supplements, methods: offer
through places implementation abuse, or
ARV drugs, IPTp 2–3 months’
other than of mass neglect;
• Distribution of supply at each children living
health care vaccination
mebendazole visit with HIV (or
facilities, such campaigns in the
and ITNs • Triage and adult due to
as pharmacies, context of
drug shops, • Treatment of referral for COVID-19. disability/other
online malaria, urinary problems/ School-based limitation) who
platforms and tract infection/ danger signs vaccination may cannot access
other outlets, asymptomatic continue only if ART and is in
home bacteriuria infection control danger of
treatment
deliveries, and • Triage and can be
CHWs, whether guaranteed. If interruption
referral for
outreach, identified mass campaigns • KP services:
community- problems/ are suspended, Continue to
based, or danger signs school-based access
home-based. campaigns treatment,
should also be PrEP, viral load
avoided. testing, and
• Integrated other care
outreach should through
13 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
be used to community
identify platforms.
potential
COVID-19 cases
and provide
immunization
and ANC so that
those clients do
not access
facilities for
care.
Facility-based Facility-based visits Facility-based with a Facility-based visits Facility-based visits Facility-based Facility-based Facility-based
• Optimize with a skilled skilled provider with a skilled with a skilled • First-line • Introducing/stre • Triage,
opportunities provider and private or public provider provider response to ngthening including,
for integration laboratory capacity sector • Inpatient care • Routine GBV, with clinical, lab, and where possible,
with other • Discontinuation • Provision of for sick women immunization special pharmacy have pregnant
essential of group ANC essential and and newborns, can be provided attention on appointments women coming
services, emergency including at facilities ensuring privacy systems for ANC or
• First visit at any
including maternal and neonatal adhering to IPC and delivery enter
gestational age • Targeted
immediate newborn care intensive care recommendatio confidentiality, through a
(12 weeks), to provider-
postpartum and during labor, unit ns. and measures different door
include initiated testing
postabortion ultrasound childbirth, and • KMC for • Reduce missed to keep and counseling, than sick
care. estimation of the immediate preterm and opportunities by themselves safe including HTS patients, and
gestational age postpartum low-birthweight integrating other • Informing for clients with screening
period newborns services (well- survivors of TB and STIs, and febrile patients
• Visits at 30, 36,
• Prioritization of baby, illness ways they can in ANC settings, for malaria in
and 40 weeks • PNC and ENC
malarial areas
support for check, maternal protect nutrition clinics
• Catch-up of before
initiation of health, and FP) themselves and • Malaria case
missed ANC discharge/withi • Early infant
skin-to-skin with primary providing small, management,
n the first 24 diagnosis
14 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
contacts, contact and hours in the vaccination credit card- including
including early and case of a home visits. Consider sized cards testing and
delivery of exclusive birth vaccine delivery listing relevant treatment; in
tetanus toxoid breastfeeding, • Counseling on along with other phone numbers situations with
vaccination, and with complication routine health for support significant
HIV and syphilis appropriate readiness plan service delivery. service
testing precautions before • Delay continuity
• Catch-up of • Performance of discharge introduction of disruption,
incomplete cesarean (adapt for any new consideration of
home-based section changes to vaccine(s) in the temporary
records operations services) national return to
based solely on immunization presumptive
• Distribution of • Visit at 6 weeks,
obstetric schedule. malaria
2–3 months of to include
indications treatment (i.e.,
recommended newborn without the
micronutrient independent of vaccination
COVID-19 benefit of
supplements • Catch-up of
transmission diagnostic
and ITNs missed
scenario and confirmation,
• Evaluation and
the COVID-19
PNC/ENC such as through
management of status of the contacts or a rapid
danger signs essential diagnostic test)
woman
• In- or elements, or the use of
outpatient including mass drug
management of vitamin K and administration
complications birth dose if there are
immunizations, significant
and of stock-outs of
incomplete rapid diagnostic
home-based tests
records
15 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC Labor and Postnatal Care Immunization GBV TB and HIV Malaria
Childbirth (PNC)/Essential
Newborn Care
(ENC)
• Evaluation and
management of
danger signs
• Outpatient
management of
complications
• Provision of
short-acting
methods: offer
2–3 months’
supply at each
visit
• Initiation of
LARC and
sterilization
16 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Establish Effective Patient Flow (Screening, Triage, and Targeted Referral) at All Levels
Reorganize facilities to include a screening area at health facility entrances and standard operating procedures to isolate clients with suspected or confirmed COVID-19,
ensure adequate social distancing in in- and outpatient client areas, strengthen use of PPE for health workers depending of type of exposure, and develop patient flow that
minimizes contact between clients. Consider booking system for appointments (clinical consultation, medication pickup, and laboratory work) to minimize crowding and
wait times.
Offsite Triage: Consider triage via phone.
Onsite Triage and Screen: For client and companion, for COVID-19, consider temperature check at entrance of health care facility (using infrared thermometer whenever
possible) and assess clinical symptoms and/or contact with clients with suspected or confirmed COVID-19 using a simple checklist. Prioritize clients with respiratory
symptoms and/or respiratory distress for clinical evaluation, and follow up with/refer and manage as needed. Consider if administrative staff or other nonclinical staff can
be involved in triage. Provide training on COVID-19 triage, screening, standard precautious, and PPE, with direct communication and support to clinical backstop.
Other facility-based patient flow considerations include:
Ensure there are handwashing stations at facility entrance(s). Instruct all clients to wash their hands before entrance, wear a cloth mask, and keep physical distance in
waiting areas.
Limit number of companions with clients coming to health care facilities.
Consider use of online tool so clients can assess themselves and self-identify with symptoms. Conduct follow-up clinical assessment.
Isolate clients with suspected/confirmed COVID-19 in a dedicated treatment area separate from other patients, where possible, and provide them with a facemask
See COVID-19 Personal Protective Equipment for Healthcare Workers and Community Health Workers.
Refer clients experiencing moderate/severe disease and requiring higher-level acute care and intervention to designated facilities (private or public sector).
Follow guidance for wearing masks and require quarantine/self-isolation for exposed clients.
Where possible, have clients wait in a comfortable area outside or in a well-ventilated area with handwashing facilities. Seating should ensure social distancing and limit
number of clients in indoor waiting areas.
Disinfect all surfaces between visits/clients.
Reorganize client flow and movements to bypass emergency or fever clinics to minimize exposure risk.
In areas of malaria transmission, ensure all those with fevers are screened for malaria. Implement procedures to ensure that malaria cases are not exposed to
suspected COVID-19 cases where and as possible.
17 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC/PNC Labor and Childbirth/ENC Immunization GBV TB/HIV Malaria
• In the waiting For all situations: • Separate • Identify/update • Institute clinical • Ensure women are
area: • Ensure adequate distance preventive information on and pharmacy not sharing cups
- Prioritize between examination clinics from local services for appointment for IPTp by directly
visits for spaces/limit access to only treatment survivors, including systems if they do observed therapy.
women/ one woman in areas. hotlines, shelters, not already exist.
newborns triage/examination room. • Consider rape crisis centers, • Consider staggering
with danger • Facilitate frequent smaller, more and counseling. clinical
signs. handwashing. frequent clinics • Share opening appointments, ARV
- Conduct • Keep women and their to reduce hours, contact PrEP pickup, TB
group babies together, crowding. details, and treatment, and TB
education regardless of their • When facility whether these preventive
sessions. COVID-19 status, with outreach is services can be treatment to avoid
• Where possible, appropriate precautions. possible, offered remotely, crowding and to
conduct history maximize and establish streamline clinic
and provide Obstetric triage/initial advance referral linkages. flow so PLHIV do
individualized examination of woman in communications • Make information not interact with
counseling in a labor to encourage available to health multiple health
private area. See Initial Assessment of attendance but care providers and care workers
Clients Presenting for with CHWs, and ensure (e.g., avoiding
• Call only one
multiple points of
woman (and her Intrapartum Care: Summary of appropriate it is easily
Key Considerations in the timing and accessible to clients contact between
baby) from the PLHIV and health
waiting area for Context of COVID-19. space to reduce coming to a facility.
crowding. care workers).
consultation/ • Prioritize care for danger
investigation/ signs or imminent birth.
results and plan • Provide care and monitor
of care/ labor, assist with
collection of childbirth, and provide
prescriptions. immediate care to woman
• Ensure and newborn. Facilitate
adequate early and exclusive
distance breastfeeding, and
18 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC/PNC Labor and Childbirth/ENC Immunization GBV TB/HIV Malaria
between practice skin-to-skin
examination contact, regardless of
tables/limit COVID-19 status, with
access to only appropriate precautions.
one woman • Provide care for the
(and her baby) postpartum woman and
in the newborn.
examination
- Consider early
room/
discharge after an
laboratory/
uncomplicated vaginal
pharmacy.
birth (after 6 hours)
and cesarean section
(after 2 days) for
healthy women and
newborns, and for
stable preterm or
low-birthweight
newborns receiving
KMC (with follow-up).
- Limit the number of
caregivers providing
KMC support to one
or two using
appropriate PPE.
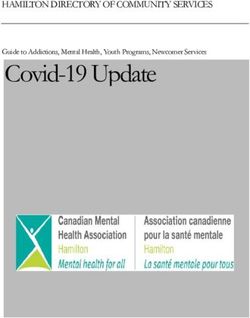
19 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Model of Effective Facility Patient Flow (Screening, Triage, and Targeted Referral) at Facility
or Community Outreach
WAITING AREA Documentation/health
Registration/screening for Facility- or community-
• Large waiting area, preferably outdoors with social education messages, including
service eligibility based service offering
distancing (may require makeshift shade); limit on prevention of COVID-19
number of clients in waiting area indoors
Maintain social distancing. Staffed by health care Maintain social distancing.
• Mobile handwashing station Require use of PPE for workers wearing Consider use of face mask as
• Group education on hand hygiene, respiratory providers and facility staff appropriate PPE and per WHO/national
etiquette, and physical distance relating to COVID-19 based on risk of exposure. following other IPC recommendations.
practices.
• Display and distribution of risk communication
materials for COVID-19
• Separate well clients seeking preventive care from
sick clients and treatment areas if possible
Screening for COVID-19 Infection
Clients with confirmed or suspected COVID-19
1. Does patient have acute respiratory illness or acute respiratory infection
(characterized by fever > 38o C and cough or shortness of breath), AND
Screening for COVID-19 using surveillance a. A history of travel to or residence in area reporting community transmission of
case definition COVID-19 during past 14 days OR
ENTRANCE Social distancing between staff and b. Having been in contact with a confirmed or probable COVID-19 case in the past
beneficiaries, hand hygiene station 14 days prior to symptoms OR
Use of PPE for providers and facility staff 2. Does patient have severe acute respiratory infection AND require hospitalization
based on risk of exposure AND there is no alternative diagnosis that fully explains clinical presentation EXIT
Ensuring malaria screening of febrile
clients in relevant settings Probable case of COVID-19
1. A suspect case for which testing for the COVID-19 is inconclusive OR
2. A suspect case for which testing could not be performed for any reason
Remove from the routine patient flow and isolate patients who meet any of the
Triage for further evaluation, including criteria (1 or 2) above, provide a medical mask and arrange for further evaluation,
taking temperature and referral for including testing.
testing
Social distancing: maintaining a spatial distance of 6 feet between beneficiaries
20 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Rapidly Optimize Health Workforce Capacity
Redistribute/reassign staff:
Regional/district level: Assess health workforce needs and consider redirecting staff to priority areas based on burden and HR available. Identify changes in volume of
essential services related to COVID-19 and staffing levels in districts. Deploy staff from over- to understaffed districts.
Facility level:
Identify changes in volume of essential services related to COVID-19 and staffing levels in units. Reassign staff from over- to understaffed units.
Reassign/hire staff to screen, triage, and test clients on arrival.
Where possible, designate ANC and labor and delivery staff who do not circulate through curative services to minimize COVID-19 exposure risk.
Strengthen capacity to assume new roles/tasks:
All staff at all levels: Develop job aids and use remote training/teletraining/eLearning to train on use of PPE, IPC, and screening and triaging of clients.
Reassigned staff: Orient staff on new duties and assign a preceptor to mentor them as they assume new duties. Provide one-on-one training using low-dose,
high-frequency training as needed.
Deployed staff: Orient staff on the facility infrastructure, workflow, policies and procedures, documentation, and monitoring.
Remote/telehealth providers: Develop job aids/algorithms and use remote training/teletraining/eLearning to train on triage and provision of counseling over the
phone.
Reorganize facilities to include a screening area, ensure adequate social distancing in in- and outpatient client areas, and develop patient flow that minimizes contact
between clients. If needed, develop job aids and use remote training/teletraining/eLearning to train on reorganization of services in the context of COVID-19.
Update quality assurance indicators, data collection tools, and supervision tools to reflect task shifting and shifts in care provision. Formalize and strengthen roles of
community-based volunteers and lay health workers. Utilize them to assist supportive functions, but ensure clear roles, safe interactions, and adequate training.
Develop tools and systems to support remote supervision and teleconsultation.
21 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC/PNC Labor and Childbirth/ENC Immunization GBV TB and HIV Malaria
• Leverage trained • Where possible, designate ANC and labor and • Involve and train • Inform and alert • Ensure all staff Community-based
CHWs to continue delivery staff who do not circulate through curative health care all service working in TB • ITN distributors
providing services to minimize COVID-19 exposure risk. providers not providers about program are • IRS personnel/
counseling at the engaged in the heightened oriented to spray teams
community level • Strengthen capacity of • Community-based/ COVID-19 risk of GBV disease
all maternal and nonfacility providers
• Integrated
about response, related to manifestation
newborn health (depends on country community case
contraceptive including from prevention and management
management
options, where providers to promote strategies for task NGOs and civil measures, such as of COVID-19.
relevant and self-care. shifting and health society isolation, stigma, • Optimize
• Community IPTp,
appropriate - Develop aids for worker learning needs) organizations, to mental health where already
community
provide providers and to conduct: start enumerating effects and being
health worker
commodities, clients. - Triage for women the cohorts of socioeconomic implemented
impact by
make referrals - Use remote in labor, children who have stresses related integrating
when needed and training/ postpartum missed their to the pandemic. COVID-19 and TB
support continuing teletraining/ women, and vaccine doses and • Train CHWs on contact tracing
users. eLearning on newborns develop an action first-line response efforts.
self-care. - Counseling during plan for tailor- to GBV, with
pregnancy and the made catch-up special attention
• Identify resources
immunization.
used by postpartum to ensuring
pregnant/postpartum - Counseling for privacy and
women and parents/ women in labor confidentiality,
caregivers of prior to transport and measures to
newborns to a facility with a keep themselves
(e.g., pharmacies, skilled provider safe.
traditional healers, - Counseling on • Build provider
religious leaders) and what to expect in capacity on:
distribute client aids labor, childbirth, - Providing GBV
for self-care for use if and the immediate first-line
they are asked for postnatal period support and
advice. - Counseling on care crisis
of the newborn
22 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC/PNC Labor and Childbirth/ENC Immunization GBV TB and HIV Malaria
• Community-based/ - Contents of management
nonfacility providers PNC/ENC visits by phone
(depends on country - PNC/ENC visit - Conducting
strategies for task schedule by point case
shifting and health of care management
worker learning - FP counseling by phone
needs) to conduct: - Initiation of short- - Conducting
- Contents of ANC acting postpartum safety
visit by GA FP methods planning with
- ANC visit survivors over
- Breastfeeding
schedule by point the phone
support
of care - Ensuring
- Continuation of
- Point-of-care confidentiality
KMC at home
diagnostics in
- Management documentatio
- Voluntary (e.g., malaria, mild n
counseling and anemia, urinary
testing tract infection) and
- Management of follow-up (e.g.,
common HIV, nonsevere
discomforts in pre-eclampsia,
pregnancy chronic
- Counseling on hypertension) of
and provision of select problems
micronutrient - Management of
supplements, select
anthelmintics, breastfeeding and
IPTp, ARV drugs newborn problems
- Triage
- Management
(e.g., malaria,
mild anemia,
23 Operational Guidance for Continuity of Essential Services Impacted by COVID-19SRH/FP ANC/PNC Labor and Childbirth/ENC Immunization GBV TB and HIV Malaria
urinary tract
infection/
asymptomatic
bacteriuria) and
follow-up (e.g.,
HIV, nonsevere
pre-eclampsia,
chronic
hypertension) of
select problems
24 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Critical Health Workforce Considerations
Service delivery modality (i.e., can the service be offered successfully and at a high Repurposing/mobilizing health workforce:
quality): • Consider sources for temporary health workforce surge capacity/service continuity:
By the client/family (self-care) part-time staff, staff in quarantine (can support remote tasks, such as
By a health provider: telemedicine/hotlines), staff from nonaffected areas, and health workers available for
• Remotely/virtually temporary reassignment.
• Within a home/community • Consider working shifts to limit exposure to COVID-19 (every 7–10 days).
• Within a facility • Recruit additional health workers, including licensed retirees and medical trainees for
Health status of health worker: appropriate supervised roles; nongovernmental, military, and private-sector health
workforce; workers from nonhealth sectors to support tasks and functions in health
• Asymptomatic: Have not had and are not currently exhibiting symptoms of COVID-19, care facilities (administration, maintenance, other support services for staff and
including recovered post-positive COVID-19 testing (criteria based on WHO and/or patients, etc.); and volunteers.
local authorities)
• Provide additional capacity-building, which may have to be delivered virtually
• Symptomatic/confirmed cases/exposed: health workers currently exhibiting COVID-19 (eLearning, telementoring, hub-and-spoke communities of practice, WhatsApp-based
symptoms under investigation and/or have COVID-19 confirmed as well as health training).
worker caring for someone who is exhibiting symptoms of COVID-19 without applying
• Link training to HR information management systems so it can be closely monitored
standard precautions and applicable PPE and health workers health workers who have
and adjusted based on the what and where.
had contact with household/family member
• Co-morbidities that place health worker at high risk (including hypertension, diabetes,
cardiac disease, respiratory disease, and malignancy)
Protecting physical health of frontline health workers: Scopes of work:
• Appropriate work hours and enforced rest • Critical for delivery of the essential health service
• Consider working shifts (every 7–10 days) • Noncritical for delivery of the essential health service
• Appropriate training and availability of PPE for rational PPE/IPC and standard • Opportunity for task shifting/sharing
precautions
• Health worker partner for doffing and donning of PPE
• Occupational health: reporting symptoms, self-isolation/quarantine, safe return to
work
• Mental health and psychosocial support
25 Operational Guidance for Continuity of Essential Services Impacted by COVID-19Maintain the Availability of Essential Medications, Equipment, and Supplies
Based on strategies for task shifting and shifts in provision of care (e.g., self-care, provision of care at community vs. facility, multimonth provision of medications):
Update norms/standards for equipping all levels of care.
Update data collection tools for stock inventory and the supply chain to reflect updated standards.
Consider a cloud-based inventory management system to track inventory. Use mobile apps to trigger reordering.
Where feasible, deploy multimonth dispensing to assist clients in reducing facility visits. Clients should preferentially receive their drug supplies outside health
facilities.
Develop/distribute job aids for:
Estimating and forecasting needs for equipment, supplies, and medications, given the shifts in care provision and increased needs with COVID-19 (consider longer
lead times, given freight disruptions)
Establishing minimum levels that trigger orders; implement order staggering to prevent delivery delays
Improving accuracy of data to follow inventory
Calculating and maintaining safety stock
Develop and implement strategies to engage all providers to take responsibility for:
Alerting relevant staff when stocks reach the minimum level or equipment need repair/replacement to ensure continuous availability of essential medications,
equipment, and supplies
Ensuring rational use of PPE, medications, and diagnostic tests
Facilitate monthly facility (with associated communities)-, district-, regional, and national-level reviews of data on stock:
Identify trends and issues. Troubleshoot to identify bottlenecks and strategies to improve stock levels and reduce stock-outs and waste/loss from theft or expiration
or poor storage conditions.
Conduct prioritization exercises to ensure that the most urgent need is met. Ongoing supply plan and inventory data (PPM/R) review to identify and respond to
urgent need.
Strengthen relationships between vendors and public-sector procurers.
Strengthen linkages and communication between:
People responsible for the supply chain at all levels to ensure timely provision of needed equipment, medications, and supplies
26 Operational Guidance for Continuity of Essential Services Impacted by COVID-19 Facilities and communities to facilitate availability of essential equipment, medications, and supplies at the community level
Facilities/communities to facilitate moving or trading equipment, medications, and supplies as needed
Partner with providers of PPE to improve availability and timely delivery of PPE. Engage the private sector to bridge gaps in the public sector.
SRH/FP MNH Immunization GBV TB and HIV Malaria
• Facilities, pharmacies, • Multimonth (2–3 • Consider other partners • Community distribution • Uninterrupted supply of
and CHWs to carry months) dispensing of (such as resource of condoms and essential malaria
extra supplies of short- micronutrients, ARV extraction companies) lubricants commodities, such as
term methods (pills, drugs, contraceptives, making regular • Multimonth (3–6 long-lasting ITNs, rapid
condoms, injectables) condoms, and IPTp essential transport as months) of ART, ideally diagnostic tests,
• Advance distribution of specifically partners to maintain through community- artemisinin-based
emergency • Increased availability freight chains for based distribution combination therapy,
contraception to clients and access to vaccines and injection points; also of PrEP and drugs for severe
postpartum LARC equipment. TB preventive malaria, and
• Increased availability
sulfadoxine-
and access to those methods and • Maximize sharing of the treatment
sterilization that can be vaccine cold chain for pyrimethamine for IPTp
contraceptives that can • Community-based
be used by the client initiated prior to temperature-sensitive treatment prioritized
without service discharge from the supplies from other for TB clients
provider support, facility after childbirth programs, such as
• Substitute for
including various self- • Increased availability COVID-19 diagnostics,
equivalent products/
care methods and access to oxytocin, insulin, and
formulations where
(condoms, fertility postpartum birth HIV diagnostic kits,
limiting this to products necessary
awareness-based control methods that
methods, lactational can be used by the that do not pose any
amenorrhea, pill or client without service risk to vaccine
mini-pill, emergency provider support programs.
contraception pills, and
subcutaneous depot
medroxyprogesterone
acetate/Sayana Press,
depending on country
27 Operational Guidance for Continuity of Essential Services Impacted by COVID-19You can also read