VOLUNTARY MEDICAL MALE CIRCUMCISION - Project 300K Campaign Report South Africa - Knowledge ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

VOLUNTARY MEDICAL MALE
CIRCUMCISION
Project 300K Campaign Report
South Africa
November 2020-March 2021
TABLE OF CONTENTS
Acronyms ............................................................................................................................ 5
Executive Summary ........................................................................................................... 6
1. Background ................................................................................................................ 11
2. Aim and objectives .................................................................................................... 13
3. Management approcah .............................................................................................. 13
3.1. Partner co-ordination ....................................................................................................................... 13
3.2. Data quality assurance .................................................................................................................... 14
3.3. Demand generation .......................................................................................................................... 14
4. Implementing partners .............................................................................................. 14
5. Provincial collaboration ............................................................................................ 16
6. Demand generation.................................................................................................... 17
7. Results ........................................................................................................................ 19
7.1. Implementing partner pledges ........................................................................................................ 19
7.2. National performance ...................................................................................................................... 20
7.2.1. Project 300k setting ....................................................................................................................... 20
7.2.2. Project 300k performance ............................................................................................................. 20
7.2.3. Project 300k performance RT35 vs. PEPFAR .............................................................................. 22
7.3. Provincial performance ................................................................................................................... 22
7.4. District performance ........................................................................................................................ 23
7.4.1. Eastern Cape district performance ............................................................................................... 23
7.4.2. Free State district performance ..................................................................................................... 24
7.4.3. Gauteng District Performance ....................................................................................................... 25
7.4.4. Kwa-Zulu Natal district performance ............................................................................................. 26
7.4.5. Limpopo district performance ........................................................................................................ 26
7.4.6. Mpumalanga district performance ................................................................................................. 27
7.4.7. Northern Cape district performance .............................................................................................. 27
7.4.8. North West district performance ................................................................................................... 28
7.4.9. Western Cape district performance .............................................................................................. 28
7.5. Implementing partner performance................................................................................................ 29
7.5.1. Aurum Institute .............................................................................................................................. 30
7.5.2. Dr. N.S Masinga and Partners ...................................................................................................... 30
7.5.3. Gauteng Province (GPR contracts) .............................................................................................. 31
7.5.4. Insimu Trading Enterprise ............................................................................................................. 31
7.5.5. J GALT Express ............................................................................................................................ 32
7.5.6. Jhpiego .......................................................................................................................................... 33
7.5.7. JPS Africa...................................................................................................................................... 33
7.5.8. Population Services International ................................................................................................. 34
7.5.9. Right to Care (PEPFAR) ............................................................................................................... 34
7.5.10. Right to Care (RT35) ..................................................................................................................... 35
7.5.11. Southern Health Foundation ......................................................................................................... 36
7.5.12. TB HIV Care .................................................................................................................................. 36
7.5.13. Thathenda Health Care ................................................................................................................. 37
7.6. Project 300k comparison to previous campaigns ........................................................................ 38
8. Conclusions ............................................................................................................... 39
8.1. Successes ......................................................................................................................................... 39
8.1.1. Improved programme management .............................................................................................. 39
2
8.1.2. Provincial DoH participation .......................................................................................................... 40
8.1.3. Ongoing analysis and sharing of DHIS data ................................................................................. 41
8.1.4. Innovative demand generation strategies ..................................................................................... 41
8.2. Challenges ........................................................................................................................................ 41
8.2.1. Reaching the campaign target ...................................................................................................... 41
8.2.2. Poor co-ordination with provinces and the traditional sector ........................................................ 42
8.2.3. Delay in signing of SLAs ............................................................................................................... 42
8.2.4. Challenges with the reporting of data ........................................................................................... 43
8.2.4.1. Men’s healthcare screening reporting .................................................................................................. 43
8.2.4.2. Lack of General Practitioner (GPR) contracting reporting .................................................................... 43
9. Recommendations ..................................................................................................... 44
9.1.1. Strengthened pledging process .................................................................................................... 44
9.1.2. Strengthened provincial engagement ........................................................................................... 44
9.1.2.1. Pro-active engagement with the Eastern Cape .................................................................................... 44
9.1.2.2. Continued provincial participation......................................................................................................... 44
9.1.3. Adapt data reporting ...................................................................................................................... 45
9.1.3.1. Adapt GPR contracting reporting requirements .................................................................................... 45
9.1.3.2. Re-assess the men’s healthcare screening reporting........................................................................... 45
9.1.4. Continue to provide the DHIS update to implementing partners .................................................. 45
9.1.5. Lessons learned session with implementing partners and PDoH................................................. 46
10. References .............................................................................................................. 47
List of figures
Figure 1: COVID-19 timeline and impact on VMMC services. .......................................................................... 12
Figure 2: Project 300k overall target, pledge and performance ........................................................................ 20
Figure 3: Project 300k performance per month against targets ........................................................................ 21
Figure 4: Project 300k implementing partner data vs. the DHIS data ............................................................... 21
Figure 5: RT 35, GPR contracting, and PEPFAR performance ........................................................................ 22
Figure 6: Project 300k provincial performance vs. target .................................................................................. 23
Figure 7: Eastern Cape district performance ..................................................................................................... 24
Figure 8: Free State district performance .......................................................................................................... 25
Figure 9: Gauteng district performance ............................................................................................................. 25
Figure 10: Kwa-Zulu Natal district performance ................................................................................................ 26
Figure 11: Limpopo district performance ........................................................................................................... 27
Figure 12: Mpumalanga district performance .................................................................................................... 27
Figure 13: Northern Cape district performance ................................................................................................. 28
Figure 14: North West district performance ....................................................................................................... 28
Figure 15: Western Cape district performance .................................................................................................. 29
Figure 16: Implementing partner performance comparison .............................................................................. 29
Figure 17: AURUM institute performance.......................................................................................................... 30
Figure 18: Dr. N.S Masinga and Partners performance .................................................................................... 31
Figure 19: Gauteng Province (GPR contracts) performance ............................................................................ 31
Figure 20: Insimu Trading Enterprise performance ........................................................................................... 32
Figure 21: J GALT Express performance .......................................................................................................... 33
Figure 22: Jhpiego performance ........................................................................................................................ 33
Figure 23: JPS Africa performance ................................................................................................................... 34
Figure 24: PSI performance .............................................................................................................................. 34
Figure 25: Right to Care, PEPFAR performance .............................................................................................. 35
Figure 26: Right to Care, RT35 performance .................................................................................................... 35
Figure 27: Southern Health Foundation performance ....................................................................................... 36
3
Figure 28: TB HIV care performance ................................................................................................................. 37
Figure 29: Thathenda Health Care performance ............................................................................................... 37
Figure 30: Historical campaign performance ..................................................................................................... 39
List of tables
Table 1: PEPFAR (CDC) implementing partner-supported districts ................................................................. 15
Table 2: RT35 service provider-supported districts ........................................................................................... 16
Table 3: Implementing partner driven demand generation initiatives ................................................................ 17
Table 4: Project 300k implementing partner pledges ........................................................................................ 19
4
ACRONYMS
AE Adverse Event
APP Annual Performance Plan
ART Antiretroviral Therapy
CBO Community Based Organisation
CDC Centers for Disease Control and Prevention
COVID Coronavirus disease 2019
DCS Department of Correctional Services
DHIS District Health Information System
DHMIS District Health Management Information System
DOH Department of Health
FBO Faith Based Organisation
GP Gauteng
GPR General Practitioners
HIV Human Immunodeficiency Virus
IEC Information, Education, and Communication
JHD Johannesburg Health District
KZN Kwa-Zulu Natal
MP Mpumalanga
NDoH National Department of Health
NT National Treasury
PDoH Provincial Department of Health
PEPFAR U.S. President’s Emergency Plan for AIDS Relief
PoE Portfolio of Evidence
PSI Population Services International
Q&A Question and Answer
RT35 National Treasury Transversal Contract for VMMC Services
RTC Right to Care
SHF Southern Health Foundation
SLA Service Level Agreement
THC TB HIV Care
TMI Traditional Male Initiation
UNAIDS Joint United Nations Programme on HIV/AIDS
VMMC Voluntary Medical Male Circumcision
5
EXECUTIVE SUMMARY
Background
South Africa continues to have the world’s largest HIV epidemic. In 2018, an estimated 7, 7million people were
living with HIV (UNAIDS, 2019). As one of the most efficacious biomedical HIV prevention interventions,
voluntary medical male circumcision (VMMC) was adopted by the South African National Department, in 2010
(SANAC, 2016), targeting men between the ages 15-49. To date over 4.4 million men have been medically
circumcised in the country (NDoH, 2021).
Historically, the winter season sees the highest uptake of VMMC in South Africa, as such the National
Department of Health (NDoH) strategically aligns the annual project management campaign, aimed at
optimising uptake of VMMC, to the winter season. However, on the 5th of March, South Africa’s Minister of
Health, Dr. Zweli Mkhize, announced the first confirmed case of coronavirus (COVID-19) in the country. The
rapid spread of COVID-19 in the country resulted in the suspension of non-essential services including the
provision of VMMC. The VMMC programme was suspended in March, and although the official resumption
was in June the uptake was minimal resulting in the loss of two-quarters of the programme.
To counter the impact of COVID-19 on the provision of VMMC services, NDoH aimed to optimise on the last
half of the year (remaining two quarters) to reach at least 50% of the annual target of 600 000 circumcisions
through the implementation of the Project 300k campaign.
Aim and objectives
The Project 300k campaign aimed to ensure that partners fully optimise the last half of the financial year
through the implementation of innovative and locally targeted demand generation strategies designed to
support the uptake of VMMC services.
Management approach
NDoH implemented a management approach that had a specific focus on three aspects partner co-ordination,
data quality assurance and innovative demand generation strategies.
NDoH was responsible for the coordination and guidance of implementing partners and sub-national levels to
ensure alignment of objectives throughout the duration of the campaign. Data quality assurance was a critical
component of the campaign, in order to ensure the timely and accurate submission of data at all reporting
levels. Lastly, the focus on demand generation strategies aimed to strengthen awareness of VMMC; provide
accurate information and education, and empower men aged 15-34 to make informed decisions about VMMC.
6
Implementing partners
South Africa’s VMMC programme is being executed with the support of the U.S. President’s Emergency Plan
for AIDS Relief (PEPFAR) funded partners through the Centers for Disease Control and Prevention (CDC),
and through a set of contractual relationships between local implementing partners and the respective
Provincial Departments of Health (PDoH).
The project consisted of eight RT35, and four PEPFAR implementing partners. Implementing partners were
expected to participate in the bi-weekly Project 300k meetings.
Funder Implementing Partner
PEPFAR (CDC) JHPIEGO
Population Services International (PSI)
Right to Care (RTC)
TB HIV Care (THC)
RT35 AURUM
JGALT
Southern Health Foundation (SHF)
Dr N.S Masinga and Partners
Thathenda Healthcare
Insimu Trading Enterprise
Right to Care (RTC)
JPS Africa
Provincial collaboration
As custodians of the VMMC programme at the sub-national level, it was critical to engage provinces in the
implementation and the management of Project 300k. Their participation ensured that provinces were
accountable for the programme’s performance and developments, but also provided a platform for
implementing partners to access the provincial colleagues. All nine provinces participated in the bi-weekly
meetings. Additionally, Kwa-Zulu Natal (KZN), and Gauteng (GP) were requested to submit VMMC data
reported by the contracted General Practitioners (GPRs) to Project 300k on a weekly basis.
Demand generation
Demand generation played a critical role in the implementation of Project 300k due to the unfortunate timing
of the campaign over the summer period. Culturally, circumcisions are conducted during the cold winter
season as it is perceived that wounds heal better in winter. During this period, there was also an increased
hesitancy to undertake VMMC among men due to the potential risk posed by the COVID-19 pandemic. As a
7
result of these challenges, partners had to be innovative in the implementation of their demand generation
initiatives to drive demand for VMMC services.
Results
Implementing partners were required to pledge monthly targets for each of the districts that they were providing
services in, for the duration of the Project 300k campaign.
Due to the reprioritisation of facilities to focus on COVID-19 and the low demand for VMMC services during
this period, implementing partners pledged modestly toward the Project 300k target. In total, implementing
partners pledged a combined target of 202, 405 that resulted in a deficit of 97, 595 towards reaching the 300k
target.
Project 300k ran from November 2020 to March 2021. However, due to the impact of COVID-19 on the
programme, NDoH announced that the April 2020 to October 2020 data from the District Health Information
System (DHIS) would be considered as the Project 300k baseline. Overall, the campaign yielded 172, 744
circumcisions, including the baseline data, reaching 58% of the 300k target.
During these five months the highest number of circumcisions (57, 917) was recorded in December 2020. Not
only were most circumcisions performed during December, but 97% of the monthly target was reached. RT35
service providers contributing 16%, GPR contracted implementing partners contributed 35% and PEPFAR
implementing partners contributed 65% toward the overall Project 300k performance.
The performance varied across provinces and districts. The provinces which contributed to the highest
VMMCs were, Eastern Cape, Gauteng and Kwa-Zulu Natal as seen in the table below:
Target Performance
Eastern Cape 42 603 43 349
Gauteng 34 961 28 687
Kwa-Zulu Natal 73 628 23 738
Eastern Cape was the only province that met and surpassed its targets during the campaign.
Districts that contributed the highest VMMCs were Johannesburg Health District (JHD), Buffalo City and Gert
Sibande as seen in the table below:
Target Performance
Johannesburg 13 294 22 694
Buffalo City 11 050 15 170
Gert Sibande 13 561 12 524
Johannesburg and Buffalo City met and exceeded the target. However, Gert Sibande did not meet the set
target.
8
Partner performance varied monthly. Overall, four of the 12 implementing partners and one province that
participated in the Project 300k campaign exceeded their targets (Gauteng GPR contracts, Dr. N.S. Masinga
and Partners, JSP Africa, and THC) Partner performance ranged from 8% to 250% target achieved as seen
in the table below:
Implementing Partner Target Performance Percentage
JHPIEGO 35111 14601 42%
PSI 34624 34221 99%
RTC_PEPFAR 47310 32061 68%
THC 500 1248 250%
AURUM 5800 1117 19%
JGALT 3925 1301 33%
SHF 14032 1822 13%
Dr N.S Masinga &Partners 5000 7274 145%
Thathenda 28500 3361 12%
Insimu 6080 510 8%
RTC_RT35 5173 1050 20%
JPS Africa 3750 3831 102%
Gauteng GPR contract 12600 24784 197%
Compared to previous campaigns, the 2020/2021 Project 300k campaign performed the lowest (58% of the
300k target) while both Project 218k and Project 300k (2018) surpassed their targets. The 2019 Project 400k,
the biggest campaign yet, also performed well, reaching 88% of its target and completing 39, 814 more
circumcisions than the 2018 Project 300k.
Conclusions
Project 300k was undertaken during an unprecedented time. Under constrained circumstances, the project
was able to achieve 172, 744 circumcisions reaching 58% of the campaign target. This is a commendable
achievement which was due to the effective collaboration of implementing partners, NDoH, PDoH’s, RT35
and PEPFAR implementing partners. There were notable successes and challenges during the
implementation of the campaign.
The successes include the improved programme management; provincial DoH participation; ongoing analysis
and sharing of DHIS data and the implementation of innovative demand generation strategies.
The challenges include the inability for partner pledges to reach the campaign target, poor coordination with
provinces and the traditional sector, the delays experienced in acquiring signed service level agreements
(SLAs) in some districts, and the difficulties with reporting of data required for the duration of the campaign.
9
Recommendations
While the context in which the Project 300k campaign was undertaken was unique and challenging, every
effort was made to make the campaign a success. However, there were various challenges and lessons to be
learned that can be applied to the implementation of future campaigns. These lessons include: strengthening
the pledging process and provincial engagement; adapting the data reporting requirements, continuing to
provide the DHIS data to partners and including lessons learned debriefing sessions with all participating
stakeholders in order to strengthen future campaigns.
101. BACKGROUND
South Africa has the world’s largest HIV epidemic. In 2018, an estimated 7, 700, 000 people were
living with HIV and there were more than 240,000 new HIV infections (Joint United Nations
Programme on HIV/AIDS (UNAIDS), 2018). Voluntary medical male circumcision (VMMC) has
been identified as a key HIV prevention intervention for South Africa as it reduces the risk of
female-to-male HIV transmission by approximately 60% (South African National AIDS Council,
2017). VMMC is not only one of the most efficacious biomedical HIV prevention interventions, but
it is also one of the most cost-effective interventions under South Africa’s Investment Case (South
African Department of Health, South African National AIDS Council, 2016). In 2010, the South
African National Department of Health (NDoH) began implementing a plan to medically circumcise
men between the ages 15-49 (South African National Department of Health, 2016). To date, the
national VMMC programme has achieved extraordinary scale having circumcised close to 4.4
million men - initially, NDoH had set a target of 4.3 million circumcisions by the end of 2016. In
addition to this target, the programme continues to scale-up services and has set ambitious
targets of circumcising an additional 2.5 million men by 2022 to reach 80% of HIV-negative men
aged 15-49 years (South African National AIDS Council, 2017).
In South Africa, the winter season has the highest rate of VMMC uptake, contributing to
approximately 50-60% of the annual VMMC targets. Thus, the previous VMMC campaigns have
been strategically and successfully aligned with the winter period. However, in 2020 the
programme’s implementation was significantly affected by the outbreak of the coronavirus
(COVID-19) pandemic.
On 5 March 2020, the South African Minister of Health, Dr Zweli Mkhize, announced the country's
first confirmed coronavirus (COVID-19) case (South African Ministry of Health, 2020). On March
15, President Cyril Ramaphosa declared a Nationwide state of disaster and on the 23rd of March
a National lockdown was announced to commence as of 26 March 2020. In line with the lockdown
regulations, all elective surgeries were temporarily suspended, subsequently, the National VMMC
programme was suspended in March 2020. The programme was suspended for three months
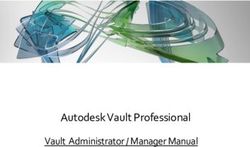
and reinstated in June 2020, as seen in Error! Reference source not found. below. NDoH
recommended a phased return of VMMC services once there was evidence that the programme
could mitigate the COVID-19 risks and comply with the government regulations as it pertains to
reducing the spread of COVID-19 in the country.
11March 5 March 15 March 23
Health Minister President announces President announces
confirms first COVID-19 National State of Disaster planned National
case Lockdown
June 23 June 15 March 26
VMMC services Health Minister National Lockdown
suspension lifted announces all 52 districts implemented
are hotspots
VMMC
VMMC
services
services
remain
suspended
suspended
Figure 1: COVID-19 timeline and impact on VMMC services.
South Africa’s VMMC programme is being executed with the support of the U.S. President’s
Emergency Plan for AIDS Relief (PEPFAR) funded partners through the Centers for Disease
Control and Prevention (CDC); and through a set of contractual relationships between local
implementing partners and the respective Provincial Departments of Health (PDoH). These
contractual relationships are managed through the National Treasury Transversal Contract
(RT35). During the period when VMMC services were suspended, NDoH, together with the
National Treasury (NT) were working toward finalising the RT35 contracting process. This was to
ensure that RT35 partners were awarded contracts to conduct VMMC in time for the resumption
of services. While the suspension of VMMC services was lifted in late June, the RT35 process
was only concluded in September 2020, resulting in delayed resumption of services.
The impact of COVID-19 meant VMMC was suspended for the first quarter of the financial year
(FY20/21) and, even with the lifting of the suspension, partners applied a gradual resumption of
services approach, which meant very few circumcisions were conducted in the second quarter of
the financial year (FY20/21). As a result, the programme was left with two quarters to optimise the
uptake of services. The annual target of 600, 000 circumcisions was set at the beginning of the
year and, despite the suspension of the services, the target remained unchanged due to the
commitments made in the Annual Performance Plan (APP). In order to optimise on the last half
of the year (remaining two quarters) in an attempt to reach at least 50% of the annual target,
NDoH implemented the Project 300k campaign.
122. AIM AND OBJECTIVES
The Project 300k campaign aimed to ensure that partners fully optimise the last half of the financial
year through the implementation of innovative and locally targeted demand generation strategies
designed to support the uptake of VMMC services.
The specific objectives of the campaign were to:
• Meet 50% of the annual target;
• Optimise demand for VMMC for the priority target population of HIV-negative males
aged 15-34 years;
• Align the project to NDoH’s demand generation campaign to ensure effective scale-
up of VMMC services in all districts;
• Monitor the reporting and capturing of data on the DHIS;
• Ensure the effective monitoring of adverse events (AEs) and men’s healthcare
indicators in all districts; and,
• Disseminate best practices and lessons learned.
3. MANAGEMENT APPROCAH
NDoH implemented a management approach which had a specific focus on partner co-ordination,
data quality assurance and innovative demand generation strategies.
3.1. PARTNER CO-ORDINATION
NDoH was responsible for the co-ordination and guidance of implementing partners, as well as
communicating with sub-national levels to ensure alignment and the establishment of the
collective management of data throughout the campaign duration. Partner co-ordination involved
the following:
1. Weekly performance analysis to ensure timely identification of challenges, agreeing
on corrective action, and monitoring of remedial activities.
2. Bi-weekly dissemination of performance data and best practice.
In light of COVID-19, the bi-weekly meetings led by NDoH were hosted virtually. Partners were
responsible for reporting their progress toward targets and their demand generation activities. On
a monthly basis, NDoH prepared a presentation which consolidated project performance
13(consolidating all the partners’ reports) for the month and provided analysis of these against DHIS
performance. PDoH were also part of the bi-weekly meetings as the custodians of the programme,
their participation allowed NDoH to hold the provinces accountable for the success of the project.
3.2. DATA QUALITY ASSURANCE
Data quality assurance was an important pillar for Project 300k as it ensured data was submitted
and captured accurately at all reporting levels. All partners were required to conduct a data
verification process in collaboration with relevant district officials before submitting data for the
project. This was put in place to help eliminate variances between data reported by partners and
data submitted for capturing into the DHIS.
As per the District Health Management Information System (DHMIS) policy, the verification
process had to include the VMMC Portfolio of Evidence (PoE) to certify the validity of all the data
submitted to the district. The PoE consists of a client intake form, a copy of a signed consent form,
a carbonated VMMC register, and the parents’ ID copy for clients younger than 16.
3.3. DEMAND GENERATION
The demand generation approach was aimed to strengthen the public awareness of VMMC
among South African men within the 15 – 34 age category range; to provide basic educational
resources for men regarding the benefits of VMMC; to empower men in enabling them to make
more informed choices regarding their sexual health; and to change people’s negative perceptions
around VMMC.
Partners were requested to provide bi-weekly update reports on demand generation initiatives
which formed part of the public awareness campaign/programme.
4. IMPLEMENTING PARTNERS
Implementing partners are responsible for the service delivery of the VMMC programme and
expected to participate in the bi-weekly Project 300k meetings. The project consisted of eight
RT35 service providers and four PEPFAR(CDC) implementing partners. Table 1 and Table 2
below depict the prime implementing partners and their supported districts
14Table 1: PEPFAR (CDC) implementing partner-supported districts
Province District Partner
Eastern Cape Alfred Nzo Right to Care
Amathole Right to Care
Buffalo City Population Services International
Chris Hani Population Services International
OR Tambo Right to Care
Free State Lejweleputswa Right to Care
Thabo M Right to Care
Gauteng Johannesburg Health District Population Services International
City of Tshwane Right to Care
Ekurhuleni Right to Care
Sedibeng Population Services International
KwaZulu Natal Amajuba TB HIV Care (THC)
eThekwini Population Services International
Harry Gwala Population Services International
uMgungundlovu Population Services International/THC
eThekwini Jhpiego/Population Services International/THC
King Cetshwayo Jhpiego/THC
uGu Jhpiego/THC
uMzinyathi THC
uThukela Jhpiego/THC
Zululand Jhpiego/THC
Limpopo Capricorn Right to Care/THC
Mopani Right to Care
Waterberg THC
Vhembe THC
Mpumalanga Ehlanzeni Right to Care/THC
Gert Sibande Right to Care/THC
Nkangala Right to Care/THC
North West Bojanala Platinum Right to Care/THC
Dr Kenneth Kaunda Right to Care/THC
Ngaka Modiri Molema Right to Care
Western Cape Cape Town Jhpiego/THC
Overberg THC
West Coast THC
15Table 2: RT35 service provider-supported districts
Province District Partner
Eastern Cape Joe Qabi Right to Care
Nelson Mandela Right to Care
Sarah Baartman Right to Care
Free State Fezile Dabi J Galt Express
Mangaung Aurum Institute
Xhariep J Galt Express
Gauteng West Rand Southern Health Foundation
West Rand Insimu Trading Enterprise
KwaZulu Natal Amajuba Thathenda Health Care
iLembe Thathenda Health Care
uMzinyathi Insimu Trading Enterprise
uMkhanyakude Thathenda Health Care
Mpumalanga Gert Sibande Southern Health Foundation
Gert Sibande Dr. N.S. Masinga and Partners
Gert Sibande JPS Africa
North West Dr R S Mopati Aurum Institute
Northern Cape Frances Baard J Galt Express
JT Gaetsewe J Galt Express
Namakwa J Galt Express
Pixley ka Seme J Galt Express
ZF Mgcawu J Galt Express
Western Cape Cape Winelands J Galt Express
Central Karoo J Galt Express
Eden Southern Health Foundation
Overberg Southern Health Foundation
West Coast Southern Health Foundation
5. PROVINCIAL COLLABORATION
Provinces are understood to be the custodians of the VMMC programme at the sub-national level
and, as a result, it was critical to engage provinces in the implementation and the management of
Project 300k. NDoH engaged all provinces and extended an invitation for provincial VMMC
programme colleagues to participate in the Project 300k campaign. The participation aimed to
ensure that provinces were accountable for the programme’s performance and developments, but
also provided a direct platform and avenue for implementing partners to access the provincial
colleagues to engage with them as needed. All provinces participated in the bi-weekly meetings.
Moreover, two provinces Kwa-Zulu Natal (KZN), and Gauteng (GP), which were identified to have
contracts with local general practitioners who provide VMMC, were requested to submit VMMC
data reported by the contracted General Practitioners (GPR) to Project 300k on a weekly basis.
166. DEMAND GENERATION
Demand generation remains a critical component of the VMMC programme as demand initiatives
drive the uptake of services for men aged 15 years and above. Demand generation played an
even more critical role in the implementation of Project 300k due to the unfortunate timing of the
campaign (over the summer period). During this period, there was an increased hesitancy to
undertake VMMC among men due to the potential risk posed by the COVID-19 pandemic. As a
result of these challenges, partners had to be innovative in the implementation of their demand
generation initiatives to drive demand for VMMC services.
Implementing partners implemented various demand generation initiatives including mass media,
social media and new web-based innovations, depending on the resources available. These
initiatives have shown innovation even under the challenging context of COVID-19. Table 3 below
outlines the demand generation initiatives implemented by implementing partners during the
campaign.
Table 3: Implementing partner driven demand generation initiatives
Demand generation initiatives Description
Edutainment • Edutainment was used to reach young men by providing them
with information at social events e.g., soccer tournaments in
most districts.
• Use of celebrities as part of edutainment e.g., Kagiso
Modupe’s celebrity soccer team.
• Client reimbursement campaigns (e.g., airtime vouchers,
Incentives
food vouchers etc.).
Interpersonal communication • Use of social mobilisers in male dominant areas, workplaces
and also in healthcare facilities.
• Activations in taxi ranks, tertiary institutions and shopping
malls.
• Healthcare facility talks.
• House-to-house mobilisation.
• Load-hailer broadcasts in communities.
Leveraging important community • Undertaking Isibaya Samadoda (with the support of Prince
and traditional structures Nhlanganiso Zulu in KZN, GP and Mpumalanga (MP)).
• Working with traditional, religious and community leaders
through Faith Based Organisations and Community Based
Organisations (FBOs /CBOs).
• Use of female VMMC ambassadors.
17Demand generation initiatives Description
Mass media • Radio campaigns
o Campaigns that broadcast on local radio stations.
This is an effective medium as in rural areas there’s a
large radio-listening population.
o Use of roundtable discussions on VMMC and men’s
healthcare.
• Information, education, and communication (IEC) materials
e.g., Posters in healthcare facilities/taxi ranks etc. with VMMC
information.
• Newspaper coverage of VMMC information.
• Online Platforms: Illustrations, videos
New technology • Moya reverse data campaign (RTC) paid for data while client
access VMMC information and call to action.
• Comm care demand creation data app (Jhpiego).
Social Media • Extending VMMC campaign to Facebook and WhatsApp -
captive messages disseminated on all platforms.
• Question and Answer (Q&A) sessions on various platforms.
187. RESULTS
7.1. IMPLEMENTING PARTNER PLEDGES
Implementing partners were required to pledge monthly targets for each of the districts that they
were implementing in for the entire period of the Project 300k campaign (November 2020- –March
2021). These monthly targets were used as a basis to monitor implementing partner performance
throughout the campaign. However, the targets that implementing partners pledged did not reach
the campaign’s target of 300k due to two main reasons. The first was the COVID-19 pandemic.
When the country went into lockdown, VMMC was suspended. When the lockdown regulations
were lifted and the gradual resumption of services commenced, VMMC services were negatively
impacted as most of the facilities previously used for VMMC were being used for COVID-19-
related services.
Additionally, there was low demand for VMMC services during this period (possibly due to fear of
contracting COVID-19 during an elective procedure). The second reason was that the Project
300k campaign was implemented during the summer season, a season where the demand for
VMMC has historically been low. For these reasons, implementing partners pledged modestly
toward the Project 300k target. In total, implementing partners pledged a combined target of
202, 405 that resulted in a deficit of 97, 595 towards reaching the 300k target. Table 4 below
depicts the implementing partner pledges for the Project 300k campaign.
Table 4: Project 300k implementing partner pledges
197.2. NATIONAL PERFORMANCE
7.2.1. Project 300k setting
Project 300k ran for five months from 1 November 2020 to 31 March 2021. At inception, NDoH
announced that the April 2020 to October 2020 data from the DHIS would be considered as the
Project 300k baseline due to the impact of COVID-19. As such, these data (45, 563 circumcisions)
were included in the overall project performance data, which is 127 181 circumcisions performed
by implementing partners during the campaign. Overall, the campaign yielded 172, 744
circumcisions, including the baseline data, reaching 58% of the 300k target by the time the
campaign concluded, as seen in Error! Reference source not found. below.
Figure 2: Project 300k overall target, pledge and performance
7.2.2. Project 300k performance
Implementing partners contributed 127, 181 circumcisions during the five-month period, with the
most circumcisions (57, 917) recorded in December 2020. Not only were most circumcisions
performed during December, but 97% of the monthly target was reached. Error! Reference
source not found. below indicates the campaign’s performance against targets by months.
20Figure 3: Project 300k performance per month against targets
Despite this achievement, December was also the month contributing the highest data variance
(28, 450), indicating that only 29, 467 circumcisions were reflecting on the DHIS, as opposed to
the 57, 917 VMMCs reported by implementing partners. November 2020, February 2021, and
March 2021 show a far better picture. That is, more circumcisions are reflecting on DHIS
compared to what the implementing partners reported for the campaign.
This indicates that implementing partners have reported all, or most, of their performance on the
DHIS. It is worth noting, however, that this is not an exact science since this could also mean that
other implementing partners, not part of Project 300k, may have conducted and reported more
circumcisions on the DHIS, resulting in the picture depicted below. However, for Project 300k, a
negative variance was used as a proxy, indicating that all the data that needs to be on the DHIS
has been submitted by the implementing partners. Error! Reference source not found. below
indicates the number of circumcisions reported by implementing partners compared to data
reflecting on the DHIS per month.
Figure 4: Project 300k implementing partner data vs. the DHIS data
217.2.3. Project 300k performance RT35 vs. PEPFAR
The performance of the RT35 service providers was lower during the campaign, contributing 16%
toward the Project 300k performance. However, the combined contribution of RT35 service
providers and GPR contracted implementing partners (35%) shows a commitment to the
programme by local implementing partners that are funded through the domestic funding
mechanisms. PEPFAR implementing partners contributed 65% toward the Project 300k
performance, this is lower compared to the 78% previously contributed during Project 400k. This
may be indicative of PEPFAR’s transition to stop providing VMMC services to the lower age
groups (10-14 years), an age group that had been supported by PEPFAR implementing partners
in previous campaigns. On the other hand, this could also depict the lingering effects of COVID-
19 on the programme. The total numbers contributed by all the implementing partners are
depicted below in Error! Reference source not found..
Figure 5: RT 35, GPR contracting, and PEPFAR performance
7.3. PROVINCIAL PERFORMANCE
Overall, the Eastern Cape province contributed the highest number of VMMCs conducted during
the campaign, completing a total of 43, 349 circumcisions and surpassing its target by 746
VMMCs, the only province that met and surpassed its targets. GP contributed the second-highest
circumcisions during the campaign, completing a total of 28, 687 circumcisions, however, it fell
short of its target by 6, 274. While KZN contributed the third-highest VMMCs during the campaign
(23, 738), it fell short of its target by 49, 890 circumcisions, this is more than any province.
However, it is worth noting that it was the only province where implementing partners pledged the
most ambitious combined targets of 73, 628. The lowest-performing provinces were Limpopo and
the Northern Cape, completing 850 and 734 circumcisions, respectively. Error! Reference
22source not found. below presents implementing partner performance against targets per
province.
Figure 6: Project 300k provincial performance vs. target
7.4. DISTRICT PERFORMANCE
7.4.1. Eastern Cape district performance
Overall, three districts - Buffalo City, Chris Hani, and Amathole, in the Eastern Cape - surpassed
their targets, contributing a combined 35, 923 VMMCs to the campaign. This is an 84%
achievement towards the province’s pledged target. On the other hand, three districts - Nelson
Mandela Bay, Sarah Baartman, and Joe Gqabi - performed the lowest VMMCs for the duration of
the campaign in the province, as seen in Error! Reference source not found. below.
23Figure 7: Eastern Cape district performance
7.4.2. Free State district performance
The Mangaung and Thabo Mofutsanyane districts completed the highest number of VMMCs in
the province (692 and 644, respectively). However, all five of the districts in the Free State did not
meet their targets. Moreover, no circumcisions were performed in two of the five districts, Fezile
Dabi and Xhariep, for the duration of the campaign as seen as Error! Reference source not
found. below.
24Figure 8: Free State district performance
7.4.3. Gauteng District Performance
In GP, Johannesburg performed 22, 694 VMMCs for the duration of the campaign as seen in
Error! Reference source not found.. This is a 171% achievement of the district’s pledged target.
All the other districts were unable to achieve their targets, resulting in the province not being able
to achieve its overall target.
Figure 9: Gauteng district performance
257.4.4. Kwa-Zulu Natal district performance
In KZN, eThekwini performed the highest total number of VMMCs (5, 709). However, the district did
achieve its target. The uGu and Harry Gwala districts surpassed their targets and achieved 104% and
148%, respectively, of the district’s pledged targets. All the other districts did not meet their targets,
with uMzinyathi only completing 202 circumcisions (as seen in Error! Reference source not found.
below), the lowest performance recorded for the province throughout the campaign.
Figure 10: Kwa-Zulu Natal district performance
7.4.5. Limpopo district performance
In Limpopo province, Mopani recorded the highest number of circumcisions (409) however, the
district was unable to meet the target. Only one of the districts, Waterberg, surpassed its target
by 10 circumcisions. This district only pledged four VMMCs for the duration of the campaign as
seen in
below. All the other districts in the province did not meet their targets and as such, Limpopo is
the second-lowest performing province.
26Figure 11: Limpopo district performance
7.4.6. Mpumalanga district performance
In MP, none of the districts met the pledged targets as seen in Error! Reference source not
found. below. However, Gert Sibande and Ehlanzeni districts came close, reaching 92% and
85%, respectively, in achieving their targets.
Figure 12: Mpumalanga district performance
7.4.7. Northern Cape district performance
In the Northern Cape, only Pixley Ka Seme surpassed their targets by an extra 69 circumcisions.
In two of the districts, Namakwa and ZF Mgcawu, no circumcisions were performed for the
duration of the campaign, as seen in Error! Reference source not found. below. As such,
Northern Cape did not meet its target and was the lowest-performing province overall.
27Figure 13: Northern Cape district performance
7.4.8. North West district performance
In the North West province, only one district, Dr. Kenneth Kaunda, surpassed its target by two
extra circumcisions. Ngaka Modiri Molema, the highest performing district (completed 6, 564
VMMCs) as seen in Error! Reference source not found. below, but fell short of achieving its
targets by 59 VMMCs. The other districts were unable to meet their targets.
Figure 14: North West district performance
7.4.9. Western Cape district performance
In the Western Cape province, none of the districts met their targets. The City of Cape Town
district recorded the highest number of VMMCs in the Province (2, 019). Notably, the Central
Karoo and West Coast were the lowest-performing districts in the province, recording 39 and 38
VMMCs respectively, as seen in Error! Reference source not found. below.
28Figure 15: Western Cape district performance
7.5. IMPLEMENTING PARTNER PERFORMANCE
Overall, four of the 12 implementing partners and one province that participated in the Project
300k campaign exceeded their targets (Gauteng GPR contracts, Dr. N.S. Masinga and Partners,
JSP Africa, and THC). One implementing partner, Population Services International (PSI), came
close (99%) to reaching their targets, falling short by only 1%. Of the 13 implementing partners,
eight showed good effort and contributed to the campaign’s performance, however, they were
unable to meet their targets as seen in Error! Reference source not found. below.
Figure 16: Implementing partner performance comparison
297.5.1. Aurum Institute
Overall, Aurum completed a total of 1, 117 circumcisions in their two supported districts. This is a 19%
achievement towards their total target of 5, 800 circumcisions for the duration of the campaign. For
both districts, i.e., Dr. Ruth Segomotsi Mompati (RSM) and Mangaung, the implementing partners
were unable to meet their targets of 4, 600 and 1, 200, respectively, as seen in Error! Reference
source not found.. Part of the reason for not meeting the targets was the delay in the signing of
service level agreements (SLAs) in the RSM district. Aurum was only able to start implementing in
this district in the last week of February 2021, therefore only had five weeks of implementation and
this impacted their ability to reach their targets.
Figure 17: AURUM institute performance
7.5.2. Dr. N.S Masinga and Partners
Dr. N.S. Masinga and Partners were responsible for providing services in one district, Gert
Sibande, in the Mpumalanga province. Overall, Dr. N.S Masinga and Partners completed 7, 274
circumcisions, which is a 145% achievement of their target of 5, 000 circumcisions for the duration
of the campaign as shown in Error! Reference source not found.. Some of the strategies that
led to the implementing partner’s success included: giving healthcare talks in the facilities they
were providing services in; increasing the demand creation staff; and allowing walk-ins at their
facilities.
30Figure 18: Dr. N.S Masinga and Partners performance
7.5.3. Gauteng Province (GPR contracts)
The Gauteng Province GPR contracting service providers pledged a total of 12, 600 circumcisions
for the Project 300k campaign. Overall, they contributed 24, 784 circumcisions to the Project 300k
campaign, surpassing their targets by 12, 184 and achieving 197% of their pledge. The GPR
contracts submitted data for three districts in Gauteng, of which only one district, Johannesburg,
was able to achieve almost three times its target. The two other districts, the City of Ekurhuleni
and the West Rand, were unable to achieve their target as seen in Error! Reference source not
found. below.
Figure 19: Gauteng Province (GPR contracts) performance
7.5.4. Insimu Trading Enterprise
Overall, Insimu Trading Enterprise completed 510 VMMCs, which is an 8% achievement of their
6, 080 targets for the duration of the campaign, as shown in Error! Reference source not found.
below. Insimu Trading Enterprise provides VMMC services in two districts, one is uMzinyathi in
31KZN and the other is the West Rand in GP. For both the districts, the implementing partner was
unable to reach its targets, and this is related to the difficulties in reaching adult men for VMMCs
despite their demand creation activities and efforts. Furthermore, Insimu Trading Enterprise
reported that they were unable to provide services in some of the facilities in the West Rand as
these were now being used for COVID-19-related activities.
Figure 20: Insimu Trading Enterprise performance
7.5.5. J GALT Express
J Galt Express pledged 3, 925 VMMCs for the duration of the Project 300k campaign. The
implementing partner performed VMMCs in five of the nine districts they had planned to provide
services in. Overall, J Galt Express performed 1, 301 circumcisions, as seen in Error! Reference
source not found. below. This is a 33% achievement of their target. The implementing partner
was only able to meet and surpass their target for one district, Pixley Ka Seme, in Northern Cape
province. The implementing partner was unable to achieve their targets because they had to
suspend their services due to administrative challenges. Additionally, for the duration of the
campaign, the implementing partner had not yet started providing services in the Free State
province.
32Figure 21: J GALT Express performance
7.5.6. Jhpiego
Jhpiego pledged to conduct 35, 11 VMMCs in six districts across the Western Cape and KZN for
the duration of the campaign. Jhpiego surpassed their targets for one of their districts, Ugu, in
KZN, however, they were unable to meet their targets for other districts. In total, Jhpiego
performed 14, 601 circumcisions, achieving 42% of their set target, as shown in Error! Reference
source not found.. Like all the other implementing partners, the COVID-19 pandemic affected
their implementation. Their demand creation activities were suspended in King Cetshwayo district.
Also, the rainy season made it difficult for the implementing partner to reach men with their
demand creation activities.
Figure 22: Jhpiego performance
7.5.7. JPS Africa
JPS Africa provided VMMC services in one district, Gert Sibande, in MP. Overall, JPS Africa
performed 3, 831 circumcisions, as shown in Error! Reference source not found. below, which
is a 102% achievement of their set target of 3, 750 VMMCs. The implementing partner attributed
their success to their demand creation activities which included social mobilisations that yielded
a higher number of men aged 15 years and older.
33You can also read