Influenza Update 2020 2021: Avoiding the Twindemic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

9/22/2020
Influenza Update 2020‐2021:
Avoiding the Twindemic
Litjen (L.J) Tan, MS, PhD
Chief Strategy Officer,
Immunization Action Coalition
Co‐Chair, National Adult and
Influenza Immunization Summit
September 23 and 24, 2020
Today’s Webinar
• Adobe Features:
– Chat Box - Lower Right
Hand Corner of Your Screen
• Today’s session is being recorded
• Slide Handouts and Notes/References available on
webinar webpage
2
1
9/22/2020
Evaluation & CE Credits
Nursing Contact Hours, CME and CHES credits
are available.
To receive these credits, please visit
www.vaccinateny.org and click the Influenza Tab
to reach the page with today’s program and
complete the evaluation and post-test.
3
Conflict of Interest &
Disclosure Statements
• LJ Tan, MS, PhD has no relevant financial relationships which could result in
a conflict of interest.
• Sarah Hershey, RN, BSN spouse owns stock in Bristol Meyers Squibb
• None of the other planners and presenters have any relevant financial
relationships to disclose.
• All relevant financial relationships have been mitigated.
• LJ Tan, MS, PhD will NOT discuss an unapproved or investigative use of a
commercial product/device in my presentation.
• No commercial funding has been accepted for this activity.
• The opinions expressed in this presentation are solely those of the
presenter and do not necessarily represent the official positions of the
Immunization Action Coalition, or the National Adult and Influenza
Immunization Summit.
2
9/22/2020
Learning Outcome
As a result of this activity, the learner will expand their
knowledge and competence on the influenza
recommendations during the COVID pandemic.
Learning Objectives
• Discuss the epidemiology and burden of disease of influenza of
the previous influenza season.
• Discuss any updates to influenza vaccination recommendations.
• Discuss the impact of co‐circulating influenza and COVID‐19
disease during the upcoming influenza vaccination season.
• Summarize innovative approaches to improving influenza
immunization access during COVID‐19.
The 2019‐2020 Influenza Season
(all data presented through August 15, 2020)
3
9/22/2020
FluB 1st; H1N1 2nd
COVID‐19
COVID‐19
7
80% were
unimmunized!
8
4
9/22/2020
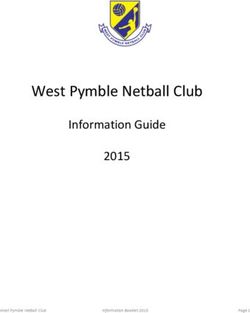
Influenza-Associated Pediatric Deaths by
Age Group (percent of total deaths)
100%
90% 16.7 19.7
25.7 23.5 23.5
30.5
80% 56.9%
70%
36 12‐17 years
60% 32.9 37.2
31.1 35.5
36.2 5‐11 years
50%
40% 2‐4 years
15.5 25.4 20.7
30% 22.4 18
13.3 58.6% had
20% 18.2 NO high-risk
16.5 13.3 16.4 16.7 16
10% condition
9.5 4.7 6.7 6.6 5.3 6.4
0%
2014‐15 2015‐16 2016‐17 2017‐18 2018‐19 2019‐20
2019 – 2020 Hospitalization Rates…
65 + years
Cumulative Rate: 173.7/100,000
5‐17 years
Cumulative Rate: 24.0/100,000
18‐49 years
Cumulative Rate: 34.4/100,000
0‐4 years
Cumulative Rate: 93.8/100,000
50‐64 years
Cumulative Rate: 90.2/100,000
5
9/22/2020
Prevalence of Chronic Conditions & their Association
with Influenza Hospitalizations in Adults 50 Years of
Age and Older
• Americans 50 years of age and older
Prevalence of Chronic Conditions are a priority group for influenza
US Adults 50‐64 Years of Age1 immunization.2
• In a study covering the 2005-2006,
30% 20% 2006-2007, and 2007-2008 influenza
1 chronic seasons, >80% of adults hospitalized
No chronic
condition
condition with lab-confirmed influenza had 1 or
more underlying medical condition; half
Diagnosed had 2 or more conditions3
with 2 or more
• In the 2016-2017 influenza season,
50% chronic
94.2% of hospitalized adult patients
conditions
with influenza had at least 1 underlying
medical condition4
11
Influenza & Cardiovascular Disease
• Incidence of admissions for acute myocardial infarction was six
times as high during the 7 days after laboratory confirmation
of influenza infection1
• A study in VA patients showed that 24% of 600 VA patients
who tested positive for influenza had acute cardiac injury and
80% occurred within 3 days of the influenza diagnosis2
• A systematic review showed consistent associations between
influenza and acute myocardial infarction, with weaker
evidence of an association with cardiovascular death3
• Acute infections, such as influenza, have been associated
with cardiovascular events, and it is hypothesized to be
due to triggering of inflammation that elicit cardiovascular
events4
6
9/22/2020
Influenza & Diabetes
• People with diabetes experienced more hyperglycemic events,
and substantial increases in pneumonia, sepsis, and coronary
heart disease up to 4 weeks after an influenza claim, as
compared to a non‐influenza period in the same year1
• People with diabetes are 3‐6 times more likely to be
hospitalized during influenza epidemics2
• People with diabetes have a much higher rate of death
associated with an influenza infection3
• Influenza vaccination recommended by the World Health
Organization for high risk patients with diabetes
Influenza Testing at Public Health Laboratories
CDC Virologic Surveillance ‐ 2019‐2020 Season
14
7
9/22/2020
Summary of Influenza Activity 2020
• Two overlapping waves of influenza activity
– B first
– Then A/H1
• Significant pediatric deaths, high hospitalization
rates
– Potential reflection of early B season?
• COVID‐19 Impact 15
The 2019‐2020 Influenza Season
– Vaccination Coverage
8
9/22/2020
Healthy People 2030 Objective
for Influenza: Increase the
proportion of persons who are
vaccinated annually against
seasonal influenza
Target: 70.0 percent
2018‐2019 Pediatric Influenza Vaccination Coverage
• 62.6% of all children 6 months ‐ 17 years of age vaccinated
• 73.4% of children 6 months to 4 years vaccinated
• 63.6% of children 5 to 12 years vaccinated
• 52.2% of children 13 to 17 years vaccinated
18
9
9/22/2020
2018‐2019 Adult Influenza Vaccination Coverage
• Only 45.3 of all adults over 18 years of age vaccinated
• Only 68.1% of those over 65 years of age vaccinated
• Only 47.3% of adults 50‐64 years of age vaccinated
• Only 39.0% of adults 18‐64 years of age vaccinated
– Only 47.9% of adults 18‐64 years of age with at least one
high‐risk medical condition vaccinated
19
19
2018‐2019 Influenza Vaccination Coverage –
Healthcare Personnel
100 95.2
90
79.8 77.9
80
67.9
Percent vaccinated
70
60
50
40
30
20
10
0
Hospital Ambulatory care Long‐term care Other se ngs‡
se ng†
20
109/22/2020
2018‐2019 Influenza Vaccination Coverage –
Healthcare Personnel
100 96.7
91.0 91.8 91.5
90 85.8
80 75.5 72.3
Percent vaccinated
70
60
50
40
30
20
10
0
Physician Nurse Nurse Pharmacist Other clinical Non‐clinical Assistant/aide
practitioner/ personnel$ personnel@
Physician
assistant
21
Impact of Employer Policy on Healthcare
Personnel Vaccination, 2018 ‐ 19
100 98
90 Coverage Rate
83
80 76 76 More
70 than 800
Percent Vaccinated
organiza
60
tions!
50
42
40
30
20
10
0
Requirement On‐site vax offered On‐site vax offered Other vax offering No requirement or
more than once once promotion
Work setting
22
119/22/2020
2018‐2019 Influenza Vaccination Coverage in
Healthcare Personnel ‐ Summary
• 81.1% vaccinated by internet panel surveys, similar
results to the previous season data.
• Long‐term care facilities had lower coverage (67.9%)
than other facility types (hospitals at 95.2%).
• Higher vaccination coverage among HCP was
associated with employer vaccination requirements or
access to vaccination at the workplace.
23
2018‐2019 Influenza Vaccination Coverage –
Pregnant Women
Pregnant Women
• 53.7% vaccinated
• Of the pregnant women who reported visiting a
doctor or other medical professional at least once
before or during pregnancy
– 73.3% reported receiving a recommendation, and
offer or referral, for flu vaccination from a doctor
or other medical professional
– 8.2% received only a recommendation for and no
offer of flu vaccination
– 18.5% did not receive a recommendation for or an
offer of flu vaccination
24
129/22/2020
Influenza Vaccination Among Pregnant Women by
Provider Recommendation or Offer of
Vaccination, 2018‐19 Season*
Influenza vaccination coverage before and during pregnancy among
women pregnant any time after August 1, 2018, by provider
recommendation or offer
100%
Percent Vaccinated
80% 65.7%
60%
35.9%
40%
20% 18.5%
0%
Recommended,
offered or Recommended,
referred not offered, not No
referred recommendation
Provider recommendation or offer
Impact of Influenza on Pregnant Women
• Up to 4X increased risk of hospitalization, especially
in third trimester, and for those with co‐morbid
conditions*
• Up to 8X increased risk for influenza‐associated
complications, including death, particularly for those
with co‐morbid conditions**
• Increased risk for influenza‐associated complications
among postpartum women
– Risk highest during the first postpartum week
26
139/22/2020
Some Coverage Thoughts
Influenza vaccination coverage appears to still be well below
HP2030 target
• Despite improvement in adults, still too low
• Steady improvement in the pediatric population
• Coverage in the 65 years and older population remains
poor...
• Coverage in the 18-64 years of age high risk adults
unacceptably low…
• Coverage in pregnant women remains flat; a strong
provider recommendation makes a difference
• HCW coverage remains strong, except in LTCF!
27
Impact of COVID‐19 on Adult
Immunization Rates
• Declines in adult immunization coverage rates widespread
and across all vaccines and risk/age groups
– E.g., 67% decline in HZ vaccination coverage
– E.g., 88% reduction in use of PCV‐13 at VA facilities
• Regional variability in COVID‐19 infections will impact
vaccination‐seeking behavior disparately
– Increase in COVID‐19 leads to decline in coverage rates.
– Localized planning will be key to address different situations
and differences in timing
• Routine immunization rates
– Returning to pre‐COVID levels…in pediatrics
– Adult rates lag
149/22/2020
Impact of COVID‐19 on Adult
Immunization Rates
• Pediatric and adult catch‐up vaccination remains
absent; large numbers remain under‐immunized
• Significant decline also seen in wellness visits for
adults of all ages
– No recovery to pre‐COVID‐19 levels yet
– Elder and high‐risk patients being targeted for visits
first
• Visits to ambulatory care also plummeted and are still
33% below pre‐COVD‐19 levels
• Telehealth increasingly being implemented
Vaccine Effectiveness
159/22/2020
Preliminary VE Against Medically Attended
Influenza, US Flu VE Network, 2019‐20
• Interim results for 2019–2020 season through June 9,
2020) indicate protection against influenza1
− 39% (CI: 36, 53) vaccine effectiveness against any
influenza virus
− 31% (CI: 190, 52) against H1N1pdm09
− 44% against B/Victoria
• Insufficient H3N2 to estimate VE at this time
− Canadian data2 suggested adjusted VE of 62%
31
Preliminary Adjusted VE Against Medically
Attended Influenza, US Flu VE Network
2019‐20, Influenza A and B
32
169/22/2020
Preliminary Adjusted VE Against Medically
Attended Influenza, US Flu VE Network
2019‐20, Influenza A(H1N1)pdm09
33
Preliminary Adjusted VE Against Medically
Attended Influenza, US Flu VE Network
2019‐20, Influenza B/Victoria
34
179/22/2020
Preliminary VE Against Influenza
Hospitalizations in Adults, HAIVEN, 2018‐19
Any Influenza A and B Adjusted VE* (95% CI)*
All patients aged ≥ 18 years 25% (1 to 41)
18–49 1% (-58 to 38)
50-64 47% (22 to 63)
≥65 15% (-24 to 41)
35
Preliminary VE Against Pediatric Influenza
Hospitalizations, NVSN, 2018‐19
Any Influenza A and B Adjusted VE* (95% CI)*
All patients aged 6 mos. to 17 years 31% (5 to 51)
6 mos. to 8 years 26% (-6 to 49)
9 to 17 years 53% (5 to 77)
By virus subtype
H3N2 13% (-31 to 43)
H1N1pdm09 48% (14 to 68)
36
189/22/2020
Summary of Interim VE for the
2019‐20 Influenza Season
• Vaccination reduced medically attended illness due to
any influenza virus type by 39% (95%CI: 32, 45) based on
enrollment through June 9, 2020
– 33% (CI: 17 to 45) VE against any influenza in children
6m–8 years
• Vaccination provided 44% (CI: 35 to 51) protection
against predominant influenza B/Victoria virus (clade
V1A.3)
Summary of Interim VE for the
2019‐20 Influenza Season
• Overall effectiveness against H1N1pdm09 = 31% (CI: 22 to 40)
– Protection against A/H1N1pmd09 virus lower than
previous seasons; Investigation of contributing factors
ongoing
• Vaccine offers significant protection against influenza
hospitalizations
– Vaccine reduced influenza hospitalizations by 22% among
all adults and by 24% among adults ≥65 years of age
(influenza A and B viruses) in 2017‐18 season
199/22/2020
Another Way to Look at Influenza Vaccine
Effectiveness – Negative Outcomes Averted
39
Even When VE Is < 50%, Current Vaccines
Can Have A Major Impact
CID; Modeling Effect of VE on Preventing
Hospitalizations in 65+
40% VE would prevent 60,000
hospitalizations
PNAS; Optimizing the Impact of Low‐
efficacy Influenza Vaccines
20% VE projected to avert 130,000
hospitalizations and 62,000 deaths
40
209/22/2020
Vaccine Effectiveness – Influenza & CVD
• Acute respiratory illness or influenza‐like illness increases acute MI
risk 2x; 5x is those with history of MI
• Influenza vaccination effectiveness: Meta‐analyses1–2
– 29% (95%CI 9,44) against acute MI in persons with existing CVD
– 36% (95%CI 14,53) against major cardiac events with existing
CVD
• Vaccine effectiveness 29% in acute MI prevention
– “On par or better than accepted preventive measures [as]
statins (36%), anti‐hypertensives (15–18%), and smoking
cessation (26%)”
– Influenza vaccination recommended as secondary prevention
by American College of Cardiology and American Heart
Association
Vaccine Effectiveness –
Influenza & Diabetes
• Six cohort and five case‐control studies were included in a
recently‐published systematic review and meta‐analysis1.
• In working age persons with diabetes mellitus,
– There was pooled VE of 58% against all cause
hospitalization
– No significant effects on all‐cause mortality and
influenza‐like illness
• In elderly patients with diabetes mellitus, adjusted VEs of
38% against all‐cause mortality and 23% against all‐cause
hospitalization were seen.
219/22/2020
Vaccine Effectiveness –
Influenza & Diabetes
• A retrospective study demonstrated that influenza
vaccination was associated with a significant decrease in
risk for hospital admission due to stroke, heart failure, and
influenza or pneumonia.1
• However, another recent systematic review that factored in
confounders such as indirect health outcomes, selection
and health seeking bias, and the frequent absence of
adjustment for pneumococcal vaccination status, suggested
that the overall evidence for influenza vaccine effectiveness
could be low.2
• Yet another report states that the present evidence
suggests that influenza vaccination among adults and
elderly with diabetes mellitus is efficacious and safe.3
Resilience to Influenza with Aging
Frailty
Index Inflammaging &
Multimorbidity
0 0.05
0.1
0.15
0.2
0.25
0.3
0.4
0.5 0.6 0.7
Graphic courtesy of Janet McIlhaney, MD
44
229/22/2020
Keeping your glass half
full!
0
0.1 Exercise, diet, smoking
cessation
0.2
and vaccination
0.3
Are you willing to risk
0.4
your independence this 0.5
winter? 0.6
0.7
45
Graphic courtesy of Janet McIlhaney, MD
Influenza Vaccines
46
239/22/2020
2020‐2021 Influenza Vaccine Strains
• Egg‐based influenza vaccines will contain hemagglutinin
derived from:
– an A/Guangdong‐Maonan/SWL1536/2019 (H1N1)pdm09‐
like virus
– an A/Hong Kong/2671/2019 (H3N2)‐like virus
– B/Washington/02/2019 (Victoria lineage)‐like virus
– (for quadrivalent vaccines) a B/Phuket/3073/2013
(Yamagata lineage)‐like virus
• Non egg‐based influenza vaccines will contain hemagglutinin
derived from:
– an A/Hawaii/70/2019 (H1N1)pdm09‐like virus
– an A/Hong Kong/45/2019 (H3N2)‐like virus
– a B/Washington/02/2019 (Victoria lineage)‐like virus
– a B/Phuket/3073/2013 (Yamagata lineage)‐like virus
47
Influenza Vaccines 2020‐2021
(www.immunize.org/catg.d/p4072.pdf)
48
249/22/2020
Influenza Vaccine Availability Tracking System
(IVATS)
https://www.izsummitpartners.org/ivats/
49
ACIP Influenza Recommendations (2020‐21)
• All persons 6 months of age or older should
receive influenza immunization (unchanged)
• Influenza vaccination should not be delayed to
procure a specific vaccine preparation if an
appropriate one is already available
50
259/22/2020
ACIP Influenza Recommendations (2020‐21)
• Vaccination should be offered as long as
influenza viruses are circulating, and unexpired
vaccine is available
• Vaccine administered in December or later, even
if influenza activity has already begun, is likely to
be beneficial in the majority of influenza seasons
• Final 2020 – 21 recommendations (released
8/20/2020):
https://www.cdc.gov/mmwr/volumes/69/rr/rr6908a1.htm
51
ACIP Pediatric Algorithm (2020‐21)
For children aged
8 years who
require 2 doses of
vaccine, both
doses should be
administered
even if the child
turns age 9 years
between receipt
of dose 1 and
dose 2.
52
269/22/2020
What To Expect This Unique Flu Season??
• Not clear what impact the current COVID 19
pandemic will have on the upcoming influenza
season in the U.S.
– There may be less influenza than usual because of social
distancing and other measures to reduce COVID 19.
– However, influenza viruses and SARS‐CoV‐2 likely will co
circulate.
• People may be co infected with influenza and SARS‐
CoV‐2.
• Co‐circulation of SARS‐CoV‐2 and influenza at the
same time could place tremendous burden on the
health care system and result in many illnesses,
hospitalizations, and deaths
53
#Avoidthetwindemic
#Takefluoffthetable
• Overlapping high risk conditions between influenza and
COVID‐19 makes it critical that we protect against VPDs,
such as influenza
• A twindemic of flu and COVID‐19 will create surge
capacitry issues for our healthcare systems
• A strong, unified, national message to seek flu vaccination
even while under “shelter‐in‐place” instructions can result
in increased vaccinations. E.g. Australia
• Vaccination efforts must be accompanied by reassuring
messaging that COVID‐19 safety is being handled
• Access points must be varied, innovative
• Vaccination season must be extended
54
279/22/2020
Immunization Action Coalition/
Coalitions Resource Repository
IAC Mass Immunization
Clinic Resource Repository
289/22/2020
During COVID‐19 & Beyond…
• All in this ship together!
– Unified, coordinated messages & multiple
stakeholders
– Provider remains the trusted voice
• Innovative approaches to increase access
– Innovation and alternative delivery options
– Address inequalities
• EXPAND the flu vaccination season
#takefluoffthetable #avoidthetwindemic
– Extend season into December and January
57
Discussing Vaccine Effectiveness
• Address vaccine effectiveness directly, early, and as
needed, during season
• Communicate the variability and unpredictability of flu
• Acknowledge that flu vaccination is not a perfect tool,
but it is the best way to protect against flu infection
• Communicate the benefits of flu vaccination beyond
prevention of disease:
– Quality of Life (vaccine preventable disability)
– Flu vaccination can reduce doctors’ visits, missed
work and school due to flu, as well as prevent flu‐
related hospitalizations and deaths.
58
299/22/2020
Dispelling Myths & Handling
Objections About Flu Shots
OBJECTION: The flu shot will give me the flu.
It’s impossible to get the flu from the flu vaccine. It is made with viruses that are not
RESPONSE:
infectious or with no viruses at all. You can get the flu from someone else.
OBJECTION: I’m healthy. I don’t need a shot.
Every year, healthy people get sick from the flu, and some even die. Many people have
RESPONSE: underlying conditions that they are not aware of. Even with a mild case, you can still
pass the virus along to the people you love and care about.
OBJECTION: I’ve never had the flu.
Every year, up to 20% of Americans get the flu—that’s up to 60 million people—many
RESPONSE:
of whom have not had the flu before.
OBJECTION: The flu shot doesn’t work.
Effectiveness varies from season to season and between flu strains. Vaccine
effectiveness is not just measured by the percentage of disease prevented but more
RESPONSE:
importantly, by the myriad of negative outcomes that vaccination prevents even if you
catch the flu, such as hospitalization and quality of life (disability).
59
NAIIS Virtual Meetings (Archived)
• Developing COVID‐19 Vaccines in Record Time, Part 2: Status
of Clinical Trials (September 9, 2020)
• Impact of COVID‐19 on Adult Immunization Coverage Rates
and Update from CDC on Influenza Communications for
2020–21 (July 30, 2020)
• Influenza Prevention in the Era of COVID‐19 (May 21, 2020)
• Developing COVID‐19 Vaccines in Record Time (May 12, 2020)
• In planning
– Influenza Vaccination on College Campuses (October 2020)
– Implementation of COVID‐19 vaccines (November 2020)
309/22/2020
Influenza & Older Americans
• National Foundation for Infectious Disease (NFID) Call to Action ‐
https://www.nfid.org/wp‐content/uploads/2019/08/flu‐older‐
adults.pdf
• CDC Flu& People 65 and Older
https://www.cdc.gov/flu/highrisk/65over.htm?CDC_AA_refVal=
https%3A%2F%2Fwww.cdc.gov%2Fflu%2Fabout%2Fdisease%2F6
5over.htm
• CDC Flyer:
https://www.cdc.gov/flu/pdf/freeresources/seniors/seniors‐
vaccination‐factsheet‐final.pdf
• 65+ Flu Defense – Resources for Clinicians (partnership
between Immunization Action Coalition and SEQIRUS)
Why do we
immunize
against Breanne, died at age 15 mos from
Amanda, died at age 4½ yrs from
influenza influenza? influenza complications
Alana, died at age 5½ yrs from Barry, a veteran fire‐fighter, died at
Lucio, died at age 8 yrs from influenza age 44 yrs from influenza
influenza complications
Slide Courtesy of Families Fighting Flu
62
319/22/2020
Access IAC Resources!
• IAC’s Influenza Educational Materials
– https://immunize.org/influenza
• Read our publications!
– http://www.immunize.org/publications/
• Visit our websites!
– www.immunize.org
– www.vaccineinformation.org
– www.immunizationcoalitions.org
– www.izsummitpartners.org
• Stay ahead of the game! Subscribe to our updates!
63 – http://www.immunize.org/subscribe/
Thank You
for your
attention!
64
329/22/2020
To obtain CE credits for
Influenza Update 2020-2021:
Avoiding the Twindemic
please go to www.vaccinateNY.org
Click on the Influenza Tab
to complete your evaluation and post test
33You can also read