I benefici dell'associazione Ezetimibe e statina nei pazienti con Cardiopatia Ischemica Cronica - Furio Colivicchi Ospedale S.Filippo Neri Roma
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

I benefici dell’associazione Ezetimibe e
statina nei pazienti con Cardiopatia
Ischemica Cronica
Furio Colivicchi
Ospedale S.Filippo Neri
Roma
Approccio Clinico all’Ipercolesterolemia. 1 • La presenza di elevati valori di Colesterolo LDL si accompagna ad un’elevata probabilità di eventi cardiovascolari avversi. • Le linee guida internazionali e nazionali sono concordi nel raccomandare la riduzione dei livelli di Colesterolo LDL come intervento terapeutico fondamentale per contrastare il rischio cardiovascolare. • Le evidenze scientifiche disponibili indicano che la riduzione del rischio è proporzionale alla diminuzione dei livelli di Colesterolo LDL.

Approccio Clinico all’Ipercolesterolemia. 2 • Al fine di rendere efficace e sicuro l’intervento terapeutico ipolipemizzante, il medico deve commisurare il trattamento al reale livello di rischio del singolo paziente. • Pertanto, la terapia non deve essere avviata solo sulla base dei valori assoluti della colesterolemia, ma può essere prescritta solo dopo una adeguata valutazione clinico-diagnostica del profilo di rischio cardiovascolare del paziente.

Outcomes in primary prevention, stable and unstable
coronary disease
16
12
Death/nonfatal MI (%)
Unstable angina/non-Q-wave MI (FRISC II)
8 Stable angina (SAPAT)
Primary prevention (WOSCOPS)
4
0
0 2 4 6 8 10 12
Months of follow-up
Wallentin L, et al. Lancet 2000;356:9-16.
Juul-Moller S, et al. Lancet 1992;340:1421-1425.
Shepherd J, et al. N Engl J Med 1995;333:1301-1307.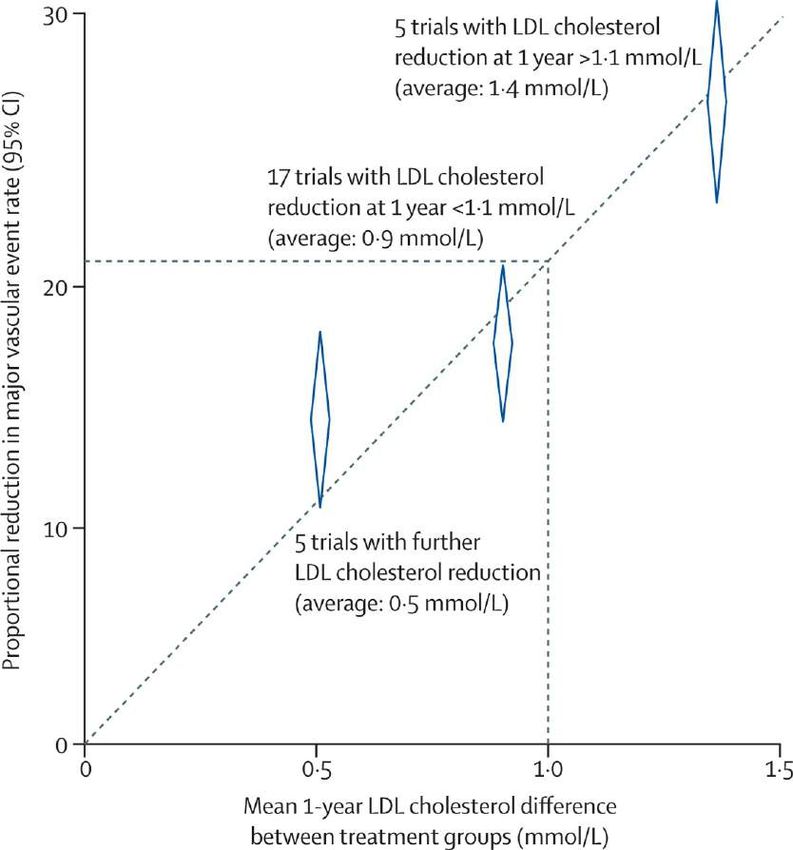
REACH: 1-year event curves for CV death, MI, stroke &
combined endpoints in Stable Atherosclerotic CV Disease
5.0
n=64,977
4.5
Event distribution function (%)
4.0 Non-fatal stroke Non-fatal MI
3.5 CV death CV death/MI/stroke
3.0
2.5 44% of these stable
patients had an event
2.0
within 10 years
1.5
1.0
0.5
0.0
0 1 2 3 4 5 6 7 8 9 10 11 12
Time in months
Steg PG et al, on behalf of the REACH Registry Investigators. JAMA 2007;297(11):1197-1206.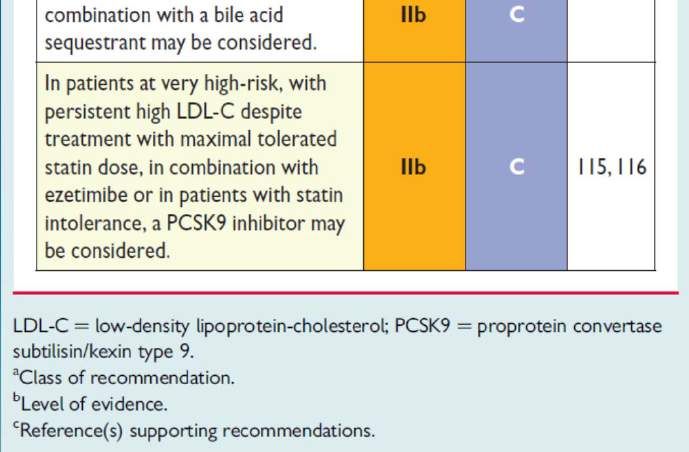

Relative risk reduction for major coronary events
La riduzione del Rischio
Relativo risulta
indipendente dai livelli
iniziali di LDL-C e dalle
caratteristiche cliniche
del paziente
Ogni riduzione di LDL-C di
38 mg/dl si associa ad una
riduzione del Rischio
Relativo del 24%
LDL Cholestrol reduction (mmol/l)
Baigent C, et al, Cholesterol Treatment Trialists’ (CTT) Collaborators.
Lancet 2005;366:1267–1278.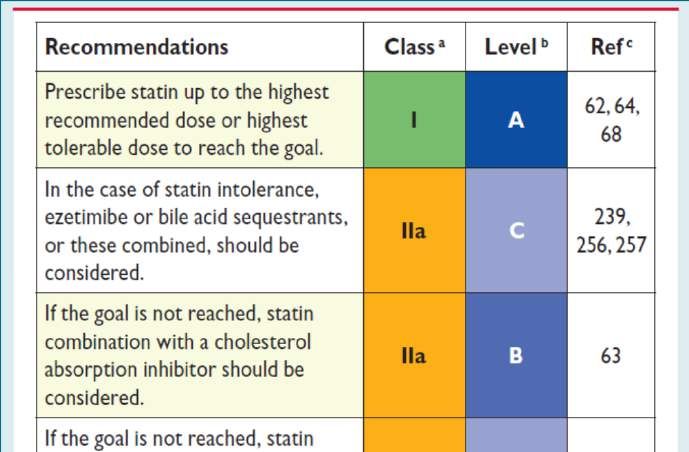
Proportional major vascular event reductions versus absolute LDL cholesterol reductions in RCTs of routine statin therapy versus no routine statin use and of more intensive versus less intensive regimens Collins R et al. Interpretation of the evidence for the efficacy and safety of statin therapy Lancet 2016; Published Online September 8, 2016

Statin therapy is the cornerstone of lipid-lowering
treatment
• There is indisputable evidence that statins reduce the risk of
cardiovascular disease, both in patients without or with a
previous major cardiovascular event (MI or stroke).
• There is also evidence that lower LDL cholesterol levels
achieved with more intensive statin therapy may result in
greater reduction in cardiovascular events.
1. Baigent C, Keecah A, Kearney PM et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from
90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267-78.
2. Baigent C, Blackwell L, Emberson J et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data
from 170,000 participants in 26 randomised trials. Lancet 2010;376:1670-81.
Lipid control for CV Prevention • Elevated levels of plasma LDL-C are causal to atherosclerosis. • Reduction of LDL-C decreases CV events. • Low HDL-C is associated with increased CV risk, but manoeuvres to increase HDL- C have not been associated with a decreased CV risk. • Lifestyle and dietary changes are recommended for all. • Total CV risk should guide the intensity of the intervention. • Total cholesterol and HDL-C are adequately measured on nonfasting samples, thus allowing non-HDL-C to be derived.
Recommendations for Lipid Control
• Most cholesterol is normally carried in LDL-C.
• There is a strong association between LDL-C and risk
of CVD.
• The evidence that reducing plasma LDL-C reduces
CVD risk is unequivocal.
• Every 1.0 mmol/L reduction in LDL-C (38 mg/dl) is
associated with a corresponding 20–25%reduction in
CVD mortality and non-fatal MIA systematic reviewand meta-analysis of the therapeutic equivalence of statins
Lipid control for CV Prevention • Patients with dyslipidaemia, particularly those with established CVD, DM or asymptomatic high-risk individuals, may not always reach treatment goals, even with the highest tolerated statin dose. • Therefore, combination treatment may be needed. It must be stressed, however, that the only combination that has evidence of clinical benefit is that of a statin combined with ezetimibe.
IMPROVE IT: Modificazioni del Colesterolo LDL
1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
∆ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5
Median Time avg
69.5 vs. 53.7 mg/dLIMPROVE IT: Endpoint primario
Simva — 34.7%
HR 0.936 CI (0.887, 0.988) 2742 events
p=0.016
NNT= 50
EZ/Simva — 32.7%
2572 eventsIMPROVE IT: Eventi durante follow up
HR Simva* EZ/Simva*p-value
All-cause death 0.99 15.3 15.4 0.782
CVD 1.00 6.8 6.9 0.997
CHD 0.96 5.8 5.7 0.499
MI 0.87 14.8 13.1 0.002
Stroke 0.86 4.8 4.2 0.052
Ischemic stroke 0.79 4.1 3.4 0.008
Cor revasc ≥ 30d 0.95 23.4 21.8 0.107
UA 1.06 1.9 2.1 0.618
CVD/MI/stroke 0.90 22.2 20.4 0.003
0.6 1.0 1.4 *7-year
event rates
Ezetimibe/Simva Simva (%)
Better BetterIMPROVE IT: Analisi dei sottogruppi
Simva† EZ/Simva†
Male 34.9 33.3
Female 34.0 31.0
Age < 65 years 30.8 29.9
Age ≥ 65 years 39.9 36.4
No diabetes 30.8 30.2
Diabetes * 45.5 40.0
Prior LLT 43.4 40.7
No prior LLT 30.0 28.6
LDL-C > 95 mg/dl 31.2 29.6
LDL-C ≤ 95 mg/dl 38.4 36.0
†7-year
0.7 1.0 1.3
event rates
Ezetimibe/Simva Simva
Better *p-interaction = 0.023, otherwise > 0.05
BetterIMPROVE IT: Primi eventi ed eventi successivi durante il follow up
Murphy SA, et al. J Am Coll Cardiol. 2016;67(4):353‐361IMPROVE IT: Primi eventi ed eventi successivi durante il follow
up in rapporto al trattamento
Total Events RR 0.91
P=0.007
Additional Events
RR 0.88 (0.79-0.98)
1st Event HR 0.936
P=0.016IMPROVE IT: riduzione del numero di eventi
Riduzione di eventi per 100 pazienti
trattati con associazione ezetimibe-
simvastatina per 10 anni rispetto al
trattamento con sola statina
Murphy SA, et al. J Am Coll Cardiol. 2016;67(4):353‐361I Valori di C-LDL in corso di terapia ipolipemizzante predicono
eventuali successivi eventi post-SCA
Quanto più basso è il livello di C-
LDL in corso di terapia tanto
minore sarà il rischio di recidive
ischemiche
J Am Coll Cardiol. 2016;67(4):362-364. doi:10.1016/j.jacc.2015.11.016General Recommendations for the Pharmacological Management of Hypercholesterolemia 2016 European Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal (2016) 37, 2315–2381 2016 ESC/EAS guidelines for the management of dyslipidaemias. European Heart Journal (2016) doi:10.1093/eurheartj/ehw272.
You can also read

















































