HIGH GRADE GEP NEN MEDICAL TREATMENTS - Nicola Fazio, M.D., Ph. D. Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors - ESMO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

HIGH GRADE GEP NEN MEDICAL
TREATMENTS
Nicola Fazio, M.D., Ph. D.
Division of Gastrointestinal Medical Oncology and Neuroendocrine Tumors
European Institute of Oncology, IRCCS,
Milan, Italy
DISCLOSURE OF INTEREST
Personal financial interests: Novartis, Ipsen, Pfizer, Merck Serono, Advanced Accelerator
Applications, MSD (Advisory board,public speaking)
Institutional financial interests: Novartis, Ipsen, Merck Serono, MSD, Pharmacyclics, Incyte,
Halozyme, Roche, Astellas, Pfizer (Clinical trial or research projects: principal investigator, steering
committee member)
Non-financial interests:
o ESMO: Coordinator of the Neuroendocrine, Endocrine neoplasms and CUP Faculty
o ENETS: advisory board chairman
o AIOM: coordinator for ITALIAN NEN guidelines
o ITANET: Scientific committee member
Neuroendocrine tumors (NETs)
GEP
Lung
Other 5%
Neuroendocrine carcinomas (NEC)
LUNG
H&N, GU
GEP
MCC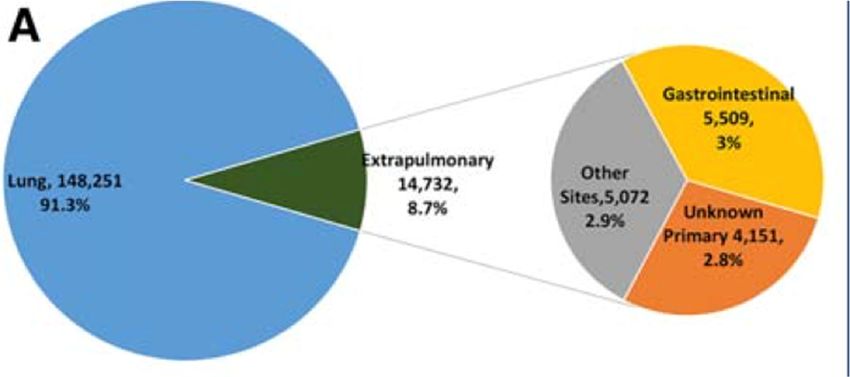
High grade GEP NENs Dasari et al., Cancer 2017

GEP NENs Midgut GI extra-midgut Pancreas

GEP NECs:
Survival is related to the primary site
Dasari et al., Cancer 2017
Table 1. Clinico-pathological features of 136 patients with NEC
ALL Type A Type B Type C
Total 136 24 30 82
Gender
Men 81 15 15 51
Women 55 9 15 31
Tumor site
Esophagus 5 0 1 4
Stomach 28 5 6 17
Duodenum 5 0 3 2
Ileum cecum appendix 17 4 3 10
Colon rectum 46 4 8 34
Pancreas 33 11 9 13
Gallbladder 2 0 0 2
Mitotic count /10HPF
Pancreas was the most frequent primary site among NET G3
Milione et al., Neuroendocrinology Mar 2016
High grade GEP NENs: ENETS 2016 guidelines Garcia-Carbonero R et al., Neuroendocrinology 2016

Chemotherapy in SCLC CISPLATIN CARBOPLATIN ETOPOSIDE IRINOTECAN
Cisplatin vs Carboplatin: toxicity profile
CDDP CBDCA
• Neurotoxicity • Bone marrow
• Nephrotoxicity toxicity
• GI toxicity
• OtotoxicityHigh grade NECs: CDDP + VP-16
Author Drugs N. pts WD PD PR/CR % RD m TTP m OS m tumors
- 18 67 8 11 19
CDDP + VP-
Moertel 1991 45 mix
16
25 - 7 - - -
- 41 42 9.2 8.9 15
CDDP + VP-
Mitry 1999 53 mix
16
12 - 9 8.5 2.3 17.6
- 9 40 - - Pancreas
CDDP + VP-
Fjallskog 2001 36 19 foregut
16
27 - 33 - - midgut
Hainsworth Taxol + CDDP Small-cell,
78 0 58 42 nr 7.5 14.5
JCO 2006 + VP-16 Merkel, G3“… the clinical behavior of G3 poorly differentiated
neuroendocrine carcinomas of the GEP tract does not
necessarily correspond to that of small cell cancer of
the lung or any other sites”
Rindi et al., Virchows Arch 2006. TNM staging…..High grade GEP NENs: ENETS 2016 guidelines Minimal consensus statement on treatment For patients with localized disease, combination of platinum -based chemotherapy wit h local treatment consisting of surgery, radiotherapy or both probably offers the greatest likelihood of long-term survival. Debulking or surgical resect ion of metastasis are not recommended. Systemic chemotherapy is indicated in advanced inoperable disease, provided the patient has adequate organ function and perf ormance status and patients should be rapidly referred for consideration of palliative chem otherapy. The combination of cisplatin and etoposide, or alternative regimens substituting carboplatin for cisplatin, or irinotecan for etoposide, are recommended as first-line therapy. Since response rates of these regimens are low er in patients with Ki-67 in the lower range of G3 (20-55%), other treat ment options may be explored in these patients (especially perhaps for NEC of GI origin). While 2nd-line re gimens have not been evaluated rigorously, options include temozolomide-, irinotecan- or oxaliplatin- based schedules as main alternatives. There ar e no data to support the use of somatostatin analogs or PRRT in patients with GEP NECs expressing so matostatin receptors. Prophylactic cranial irrad iation is not indicated in patients with limited-stage disease in complete remission. Garcia-Carbonero R et al., Neuroendocrinology 2016
Ki-67-related tumor response in G3 GEP NENs
Tumor differentiation ?
Sorbye H et al., Ann Oncol 2013High grade GEP NENs: ENETS 2016 guidelines Garcia-Carbonero R et al., Neuroendocrinology 2016
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
Elvebakken, ENETS 2019 Poster oral presentation
GEP NEC heterogeneity: possible clinical implications
WD = well differentiated; PD = poorly differentiatedGEP NEC heterogeneity: possible clinical implications
PD = poorly differentiatedPlatinum/Etoposide in high grade extra-lung NENs:
An ESMO survey
• Most respondents agreed on using CDDP or
CBDCA + EP as first-line regardless of Ki-67 and
differentiation.
• The used schedules were various.
• EP predominantly I.V.
Lamarca et al., Clin Transl Oncol 2018Carboplatin (CBDCA) + Etoposide (EP)
in advanced NECs
• 113 pts from two Institutions (Christie and IEO)
• All with advanced NEC (54% GEP)
• All receiving CBDCA/EP (86% 1°-line)
• DCR 75%
• No significant difference between oral and I.V. EP
• mPFS 6 months
• mOS 11.5 months
Frizziero et al., Neuroendocrinology 2019GEP NEC heterogeneity: possible clinical implications
WD = well differentiated;CAP-TEM in NET G3 and NEC
32 pts
PFS OS
15 mo 22 mo NET G3
3 mo 4 mo NEC
Rogowski et al., Endokrynol Pol 2019CAP-TEM in NET G3 and NEC
32 pts
PFS OS
15 mo 22 mo NET G3
3 mo 4 mo NEC
Rogowski et al., Endokrynol Pol 2019PRRT in high grade NENs Carlsen et al., End Rel Cancer 2019
Everolimus in panNET G3
15 pts with panNET (all well/moderately differentiated) and 20-55% Ki-67
All pre-treated, mostly with chemotherapy
mPFS = 6 mo
mOS = 28 mo
Panzuto et al., Pancreas 2017Sunitinib in NET/NEC G3
• 31 pts
• Responders:
• 4 PR, 14 SD
• 4/6 NET G3
• 11/20 NEC
Higher pAKT espression = lower tumor response to sunitinib
Pellat et al., Neuroendocrinology 2018Pancreatic “NET G3”
IEO patient with liver mets from
moderately differentiated pancreatic NET, Ki67 40%
Resistant to platinum-based chemotherapy
1 month of Sunitinib 37.5 mg/dCONCLUDING REMARKS Advanced GEP NEC should be treated with a platinum-based chemo as first-line therapy CDDP or CBDCA can be equally combined with etoposide Advanced GEP NET G3 should be managed as G2, considering a CAP-TEM or FOLFOX/XELOX as first-line therapy
European Institute of Oncology, IEO, Milan, Italy
ENETS Center of Excellence for GEP NETs
IEO NET multidisciplinary team
Email: nicola.fazio@ieo.it
Twitter: hermestoroYou can also read

















































