EUROPEAN SYMPOSIUM ON LATE COMPLICATIONS AFTER CHILDHOOD CANCER - 19-20 APRIL 2007 LUND SWEDEN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

EUROPEAN SYMPOSIUM ON LATE
COMPLICATIONS AFTER CHILDHOOD CANCER
19–20 APRIL 2007 LUND SWEDEN
PROGRAMME AND ABSTRACT BOOK
www.eslccc2007.com
Table of Contents Welcome 3 Programme 4 Speakers 7 Useful information & social events 8 Venue overview 9 List of participants 10 Abstracts A - Invited Speakers 14 Abstracts C - Cognition, Psychology and Quality of Life 20 Abstracts E - Endocrinology, Growth and Metabolism 27 Abstracts F - Follow-up 34 Abstracts G - Gonads and Fertility 38 Abstracts M - Miscellaneous 45 Index of Authors 53 Map of Lundagård 55 Sponsors

Welcome to Lund and Sweden
W
Organizing committee elcome to Lund – “the City of Ideas”, located in the centre of the Öresund
region. Lund offers a rich selection of cultural experiences, with the Cathedral,
Christian Moëll, chairman Scandinavia’s most distinguished church in the Romanesque style, at centre stage.
christian.moell@skane.se
The events are many and varied, with Lund’s strong tradition of comedy and farce making
Veronica Bojsen its mark on many of them. In Lund a creative, dynamic and innovative cultural spirit is alive
verabojsen@hotmail.com and well. Lund has charm and wit and will make you feel welcome.
Thomas Wiebe
thomas.wiebe@skane.se ESLCCC April 19-20 2007
The continuing success of the treatment for childhood cancer is an important medical ac-
Lars Hjorth hievement. It has however become increasingly evident that some survivors may pay a
lars.hjorth@skane.se considerable price for their cure.
Late effects after childhood cancer often have a gradual and subtle presentation that may
Scientific committee involve any organ system of the body. The follow-up will often require cooperation between
several different medical specialities.
Hamish Wallace, chairman
hamish.wallace@luht.scot.nhs.uk The European Symposium on Late Complications after Childhood Cancer in Lund, ESLCCC
2007, is the first major European meeting to focus on several different aspects of this im-
Christian Moëll portant and developing clinical area.
christian.moell@skane.se
The meeting is organized from the Department of Paediatrics at the University Hospital,
Thomas Wiebe which has a long tradition in the follow-up of late effects after childhood cancer.
thomas.wiebe@skane.se
Professor Stanislaw Garwicz has pioneered research in this field and this Symposium is
held in his honour on his retirement from the Division of Paediatric Oncology at the Uni-
versity Hospital in Lund.
Christian Moëll
On behalf of the Organizing Committee

European Symposium
on Late Complications after Childhood Cancer
Lund April 19–20 2007
Thursday April 19, 2007
TIME SUBJECT SPEAKER ABSTRACT
09:00 Welcome Christian Moëll
09:10 Introduction of Morning session Kjeld Schmiegelow
09:20 Late effects - where do we go from here? Daniel Green A:01
10:00 Modifications of treatment to minimize Guenther Schellong A:02
complications, the Hodgkin experience
10:30 Coffee
11:00 Antracycline cardiotoxicity in children – Leontien Kremer A:03
What is the risk and how can we avoid it?
11:30 Discussion Chairman: K. Schmiegelow
12.00 Poster viewing
12.30 Lunch
13:30 Children’s Cancer Foundation 25 years Olle Björk
13:40 Introduction of Afternoon session Olle Björk
13:50 Is childhood cancer a chronic disease? Guilio D’Angio A:04
14:30 Presentation of selected posters 1 Christian Moëll
Poster C:03, page 21 Ilse Schuitema
Poster E:06, page 29 Dalit Modan-Moses
Poster M:02, page 45 Marieke De Bruin
Poster M:06, page 47 Marianne Jarfelt
15:00 Coffee
15:30 Neurocognitive sequele after brain tumours Jacques Grill A:05
16:00 Neuropsychological consequences of Christine Eiser A:06
childhood cancer
16:30 Discussion Chairman: O.Björk
18:30 Welcome reception

Friday April 20, 2007
TIME SUBJECT SPEAKER ABSTRACT
09:00 Introduction of Morning Session Christian Moëll
09:10 Second neoplasms and late mortality Stanislaw Garwicz A:07
09:50 How is the Follow-up done now? Lars Hjorth
10:00 Presentation of selected posters 2 Lars Hjorth
Poster F:01, page 34 J. Hazelhoff
Poster F:05, page 36 Kate Absolom
Poster F:07, page 37 Francesca Fioredda
Poster F:08, page 37 Thorsten Langer
10:30 Coffee
11:00 The role of the nurse in the Follow-up clinic Faith Gibson A:08
11:30 Models of Follow-up after childhood cancer Andrew Toogood A:09
12:00 Discussion Chairman: L. Hjorth
12:20 Lunch
13:20 Introduction of Afternoon session Hamish Wallace
13:30 GH deficiency after Childhood cancer – Stephen Shalet A:10
whom to treat?
14:10 Presentation of selected posters 3 Hamish Wallace
Poster G:04, page 39 Yvonne L. Giwercman
Poster G:09, page 42 Jeanette Falck Winther
Poster G:06, page 40 M.H. van den Berg
Poster G:12, page 43 Kirsi Jahnukainen
14:40 Coffee
15:10 Who is at risk of gonadal dysfunction? Charles Sklar A:11
15:50 Fertility preservation in young people Victoria Keros A:12
treated for cancer
16:20 Discussion Chairman: H. Wallace
16:40 Presentation of Poster prize
16:50 Closing remarks Christian Moëll
19:00 Symposium dinner
Welcome to the European Symposium on Late Complications after Childhood Cancer.
Please see us at our exhibition stand.
Daniel Richards
F1 Championship
Nürburgring 2022
Treatment is much more than medicine –
Novo Nordisk® is dedicated to support at all levels to achieve greater heights
Growing support Growing commitment
Novo Nordisk® is a major supporter of Our aspiration is to lead the way in
endocrine research as well as meetings and improving the lives of children and adults
congresses on endocrinology, and we offer with growth hormone disturbances through
a whole range of healthcare professional our user-friendly pen systems, training
training initiatives including: training courses programmes and continued support and
(Henning Andersen Courses), fellowship education to patients and parents
support (ESPE Research Fellowship Awards),
conferences, symposia and literature
Growing ambitions. Growing potential. Growing support.
Novo Nordisk Scandinavia AB
Vattenverksvägen 47
Box 50587
nordiscience
202 15 Malmö ®
Sweden
Tel: +46 40 38 89 00
Speakers
Olle Björk Jacques Grill Kjeld Schmiegelow
Children´s Cancer Foundation Gustave Roussy Institute Pediatric Clinic
Barncancerfonden Villejuif, France University Hospital Rigshospitalet
Stockholm, Sweden Copenhagen, Denmark
Lars Hjorth
Giulio D´Angio Dept of Paediatrics Stephen M. Shalet
Department of Radiation Oncology Lund University Hospital Department of Endocrinology
Hospital of the University Lund, Sweden Christie Hospital
of Pennsylvania Manchester, United Kingdom
Philadelphia, USA Victoria Keros
Obstetrics and gynecology Charles A. Sklar
Christine Eiser Karolinska University Hospital Department of Pediatrics
The University of Sheffield Stockholm, Sweden Memorial Sloan-Kettering
Sheffield, United Kingdom Cancer Center
Leontien C.M. Kremer New York, USA
Stanislaw Garwicz Pediatric Oncology
Dept of Paediatrics Emma Children´s Hospital Andrew Toogood
Lund University Hospital Amsterdam, Netherlands University Hospital Birmingham
Lund, Sweden United Kingdom
Christian Moëll
Faith Gibson Dept of Paediatrics Hamish Wallace
UCL Institute of Child Health Lund University Hospital Royal Hospital for Sick Children
Great Ormond Street Hospital Lund, Sweden Edinburgh, United Kingdom
for Children
London, United Kingdom Guenther Schellong
University of Münster
Daniel Green Münster, Germany
Roswell Park Cancer Institute
Buffalo, New York, USA
www.barncancerfonden.se

Useful information
BANKS
Banks are open between 10.00 and 15.00 on weekdays.
CLIMATE
The weather in Lund in April is usually nice but showers can occur.
For weather forecast please visit www.smhi.com
CERTIFICATE OF ATTENDANCE
Will be available at the registration desk on individual request.
CURRENCY
The official currency is Swedish Krona (SEK).
USD 1 = SEK 7.00 (April 2007)
EUR 1 = SEK 9.35 (April 2007)
DISCLAIMER
The Organizing Committee and Congrex Sweden AB accept no liability for injuries/losses of whatever nature incurred by
participants and/or accompanying persons, nor loss of, or damage to, their luggage and/or personal belongings.
INTERNET
Wireless LAN will be available to all participants at the Symposium Venue.
You will receive your user identity and password upon registration
MEALS
Coffee and lunches are included in the registration fee and will be served daily.
Your name badge is your ticket. The lunch will be served at Akademiska Föreningen (Students’ Union).
LANGUAGE
The official language of the Congress is English
(no translation facilities will be provided).
TAXI
We recommend the following taxi companies:
Taxi Skåne, Phone: +46 (0)406 330 330
Taxi Kurir, Phone: +46 (0)406 700 700
Taxi Lund, Phone: +46 (0)46 12 12 12
Social events
WELCOME RECEPTION
Thursday 19 April 18.30 at The University Building
Drinks will be served
Included in the registration fee
SYMPOSIUM DINNER
Friday 20 April 19.00 at Grand Hotel
Price/person: SEK 400

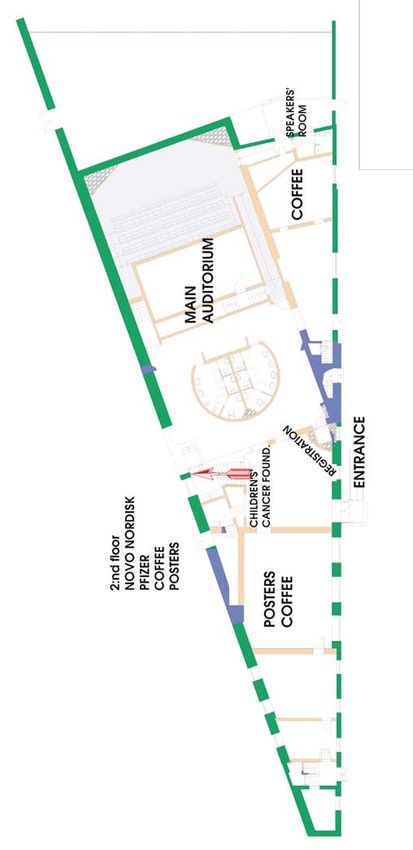
Venue Overwiev

List of participants
Blaauwbroek, Ria
University Medical Center Groningen
D
D´Angio, Giulio
Paediatric Oncology
(2007-04-12) Hanzeplein 1
Hospital of the University of Pennsylvania
Department of Radiation Oncology
9700 VB Groningen, Netherlands
HUP, Donner 2
A Bojsen, Veronica Philadelphia, PA 19104, United States
Absolom, Kate Children’s Hospital
Dahlberg, Karin
University of Sheffield Dept of Paediatrics
Barn och Ungdomssjukhuset
Department of Psychology 221 85 Lund, Sweden
Onkologi
Western Bank Bokenkamp, Arend 221 85 Lund, Sweden
Sheffield, S10 2TP, United Kingdom VU Medical Center
Davies, Helena
af Sandeberg, Margareta Pediatric Nephrology
Sheffield Childrens Hospital
Astrid Lindgrens Hospital De Boelelaan 1117
Western Bank
Pediatric Oncology 1081 HV Amsterdam, Netherlands
Sheffield S10 2TH, United Kingdom
Karolinska University Hospital Bolton, Jeff
171 76 Stockholm, Sweden De Bruin, Marieke
Pfizer Limited
Netherlands Cancer Institute
Aksnes, Liv Hege Walton Oaks
Epidemiology
Rikshospitalet-Radiumhospitalet Medical Centre Dorking Road, Tadworth
Plesmanlaan 121
Cancer Clinic Surrey, KT20 7NS, United Kingdom
1066CX Amsterdam, Netherlands
Montebello Borgström, Birgit
0310 Oslo, Norway Inst for Clinical Science, Karolinska Institutet
Albanese, Assunta Pediatrics E
Karolinska University Hospital, Huddinge Edberg-Posse, Ebba
The Royal Marsden NHS Foundation Trust
141 86 Stockholm, Sweden Kuratorskliniken
Paediatric Oncology
Karolinska Universitetsjukhuset, B44, Huddinge
Downs Road Braam, Katja 141 86 Stockholm, Sweden
Sutton SM2 5PT, United Kingdom VU University Medical Center
Pediatric oncology/ hematology Ehrstedt, Christoffer
Alston, Aileen
De Boelelaan 1117 Uppsala University Hospital
Royal Marsden Hospital
1081 HV Amsterdam, Netherlands Child Neurology
Paediatric Endocrinology
Murklevägen 15
Downs Road Bresters, Dorine 756 46 Uppsala, Sweden
Sutton SM2 5PT, United Kingdom Lumc
Wa-Kjc/Ihoba Eiser, Christine
Amoroso, Loredana
P.O. Box 9600 The University of Sheffield
Institut Gustave Roussy
2300 RC Leiden, Netherlands Sheffield S10 2TP, United Kingdom
39 Rue Camille Desmoulins
94805, France Brouwer, C.A.J. Ek, Torben
University Medical Center Groningen Barnkliniken
Andersson, Christina
Paediatric Oncology Länssjukhuset
Gävle-Dala Barncancerförening
Hanzeplein 1 30185 Halmstad, Sweden
Sweden
9700 RB Groningen, Netherlands Eldeeb, Bettina
Andersson, Ylva
Burack, Richard Royal Shrewsbury Hospital
Barncancerfonden
Great Ormond Street Hospital Paediatric Oncology
Box 5408
Oncology/Late Effects Mytton Oak Road
114 84 Stockholm, Sweden
26 Tempest Mead Shresbury SY3 8XQ, United Kingdom
Arvidson, Johan
North Weald, United Kingdom Elfving, Maria
Department of Womens and Childrens Health
Bökkerink, Jos Paediatrics
Akademiska Sjukhuset
University Hospital St Radboud Nijmegen University Hospital
752 85 Uppsala, Sweden
Pediatric Hematology and Oncology 221 85 Lund, Sweden
PO Box 9101 Elson, Ruth
B 6500 HB Nijmegen, Netherlands Bristol Royal Hospital for Children
Bashore, Lisa Oncology Day Beds
Cook Children’s Medical Center Upper Maudlin Street
Hematology/Oncology, Survivorship C Bristol BS2 8BJ, United Kingdom
901 7th Avenue, Suite 220 Caflisch, Ueli
Fort Worth, Texas, United States Paediatric Oncology Enriquez, Raquel
Kinderspital Children Hospital Aarau
Behrendtz, Mikael Pediatric Oncology
CH-6000 Luzern 16, Switzerland
University Hospital Tellstrasse
Department of Pediatrics Carlsson, Annelie
5000 Aarau, Switzerland
581 85 Linköping, Sweden Dept. of Paediatrics
Lund University Hospital Eshelman, Debra
Berg, Rickard
221 85 Lund, Sweden Children’s Medical Center Dallas
Novo Nordisk Scandinavia
Carlsson, Göran 1935 Motor Street
GHT Team, Box 50587
Astrid Lindgrens Barnsjukhus Dallas , TX 75235, United States
202 15 Malmö, Sweden
Barnonkologen Ewers, Sven-Börje
Bergsträsser, Eva
Karolinska Universitetsjukhuset Solna Dep of Oncology
University Children’s Hospital
171 76 Stockholm, Sweden University Hospital
Oncology
Clausen, Niels 221 85 Lund, Sweden
Steinwiesstr. 75
8032 Zürich, Switzerland University Hospital of Aarhus at Skejby Pediatrics
Björk, Olle
Brendstrupgaardsvej
DK-8200 Aarhus N, Denmark
F
Barncancerfonden Fahlén, Eva
Box 5408 Cohn, Richard Barncancerföreningen i Västra Sverige, Sweden
114 84 Stockholm, Sweden Sydney Children’s Hopsital
Fioredda, Francesca
Centre for Children’s Cancer and Blood Disorders
Giannina Gaslini Children Hospital
Björk-Eriksson, Thomas High Street, Randwick
Haematology-Oncology
Sahlgrenska Universitetssjukhuset 2029 Sydney, Australia
Largo Gerolamo Gaslini 5
Dep of Oncology Costa, Vitor 16134 Genova, Italy
Blå Stråket 2 Baxter, Avenida da Liberdade, 103
413 45 Göteborg, Sweden Follin, Cecilia
1269-049, Portugal
Endokrin, Kraftgatan 7b
10 231 34 Lomma, SwedenForinder, Ulla
Stockholm University
H Jakobsson, Jörgen
Novo Nordisk Scandinavia
Hakvoort-Cammel, Friederike G.A.J.
Social work GHT Team, Box 50587
Erasmus MC-Sophia Children’s Hospital
106 91 Stockholm, Sweden 202 15 Malmö, Sweden
Hematology/Oncology
Fors, Hans Dr. Molewaterplein 60 Jarfelt, Marianne
Barnklin NÄL 3015 GJ Rotterdam, Netherlands The Queen Silvia Children´s Hospital
461 85 Trollhättan, Sweden Pediatric Hematology and Oncology
Hamre, Hanne M.
Inst. of Clinical Sciences
Forslund, Karin Rikshospitalet-Radiumhospitalet HF
416 85 Göteborg, Sweden
Barncancerfonden Kreftklinikken, seksjon for langtidsstudier
Box 5408 Montebello Jernberg, Birgitta
114 84 Stockholm, Sweden 0310 Oslo, Norway Akademiska Barnsjukhuset 95B
751 85 Uppsala, Sweden
Frenos, Stefano Harila, Marika
Anna Meyer Children Hospital-Univ. of Florence Oulu University Hospital Johannsdottir, Inga Maria Rinvoll
Onco-Hematology Dept of Rehabilitation Rikshospitalet
Via Luca Giordano 13 Po Box 23 Pediatric hemato-/oncology
50132, Italy 90029 Oys, Finland Bekkeliveien 14B
Frey, Eva Harila-Saari, Arja 0375 Oslo, Norway
St. Anna Children´s Hospital Oulu University Hospital Johansson, Magnus
Oncology Pediatrics, PL23 Pfizer Limited, Sweden
Kinderspitalgasse 6 90029 OYS, Oulu, Finland
Jonmundsson, Gudmundur
1090 Vienna, Austria
Haugan, Nils Henry Landspitali Children’s Hospital
Frisk, Per Ullevål Universitetssykehus Oslo Hringbraut
Uppsala University Children’s Hospital Barneavdeling og Poliklinikk IS-101 Reykjavik, Iceland
Women’s and Children’s health Kirkev.166
751 85 Uppsala, Sweden 0407 Oslo , Norway
K
Frost, Britt-Marie Haupt, Riccardo Kazanowska, Bernarda
Uppsala University Gaslini Children Hospital, Scientific Directorate Wroclaw Medical University
Womens and childrens health Largo G. Gaslini, 5 Dept. of Pediatric Oncology
Akademiska Sjukhuset 16147 Genova, Italy Bujwida 44
751 85 Uppsala, Sweden 50-345 Wroclaw, Poland
Hazelhoff, Janneke
Emma Children’s Hospital/Academic Medical Center Kepak, Tomas
G Po Box 22660 University Hospital Brno
Garwicz, Stanislaw 1100 DD Amsterdam, Netherlands Pediatric Oncology
Lund University Hospital Hellman, Ann-Mari Cernopolni 9
221 85 Lund, Sweden Barncancerfonden 625 00 Brno, Czech Republic
Gavras, Christoforos Box 5408 Keros, Victoria
Ahepa University Hospital 114 84 Stockholm, Sweden Karolinska University Hospital
Hematology-Oncology Unit Hengartner, Heinz Obster-gyn department
Votsi 12 Ostschweizer Kinderspital K 57
60100 Katerini, Greece Hematology/Oncology 141 86 Stockholm, Sweden
Gibson, Faith Claudiusstrasse 6 Kiserud, Cecilie
UCL Institute of Child Health 9600 St. Gallen, Switzerland Rikshospitalet-Radiumhospitalet HF
Great Ormond Street Hospital for Children Hess, Siri Lothe Enhet for langtidsstudier
7th Floor Old Building Great Ormond Street Rikshospitalet - Radiumhospitalet Medical Centre Fagområde klinisk kreftf
WC1N3JH London, United Kingdom Montebello 0310 Montebello, Oslo, Norway
Gisselbaek, Mogens 0310 Oslo, Norway Krawczuk-Rybak, Maryna
Novo Nordisk Hjorth, Lars Medical University, Pediatric Oncology
Baeverdalen 26 Children’s Hospital, Dept of Paediatrics Kilinskiego 1
3400 Hillerod, Denmark 221 85 Lund, Sweden 15-089 Bialystok, Poland
Giwercman, Yvonne Holmer, Helene Kremer, Leontien C.M.
Lund University Medicinkliniken A.M.C.
Clinical Sciences Centralsjukhuset Postbox 22660
CRC, Building 91, Plan 10 291 94 Kristianstad, Sweden 1100 DD, Amsterdam, Netherlands
205 02 Malmö, Sweden
Horne, Beverly
Goldkuhl, Christina St. James’s University Hospital L
Sahlgrenska University Hospital Paediatric Oncology & Haematology Lafay-Cousin, Lucie
Dep.of Oncology Beckett Street Alberta Children’s Hospital, Pediatric Oncology
Blå Stråket 2 LS9 7TF Leeds, United Kingdom 2888 Shaganappi Trail NW
413 45 Göteborg, Sweden T2T 1X4, Canada
Hou, Mi
Green, Daniel Karolinska Institute Langer, Thorsten
Roswell Park Cancer Institute Dept. of Woman and Child Health University Hospital for Children and Adolescents
Elm & Carlton Streets Pediatric Endocrinology Unit, Q2:08 Late Effects Surveillance System
Buffalo, New York 14263, United States 171 76 Stockholm, Sweden Loschgestr. 15
Greenfield, Diana 91054 Erlangen, Germany
Cancer Research Centre
University of Sheffield
I Leiper, Alison
Ishida, Yasushi Haematology
Weston Park Hospital, Whitham Road Great Ormond Street Hospital
Ehime University Graduate School of Medicine
Sheffield, S10 2SJ, United Kingdom London WC1N 3JH, United Kingdom
Pediatrics
Grill, Jacques Shitukawa, Touon-city Levitt, Gill
Gustave Roussy Institute Ehime, 791-0295, Japan Oncology/Haemartology
39 Rue C. Desmoulins Great Ormond St
94805 Villejuif, France London WC1 N 3JH, United Kingdom
J
Gullersbo, Malin Jahnukainen, Kirsi Lidén, Karin
Barnkliniken Astrid Lindgren Children´s Hospital Barn- och Ungdomskliniken
Universitetssjukhuset Department of Woman and Child Health Centralsjukhuset
581 85 Linköping, Sweden Pediatric Endocrinology Unit, Q2:08 651 85 Karlstad, Sweden
171 76 Stockholm, Sweden 11Lindgren, Maria Moelgaard Hansen, Lene Pettersson, Liselott
Akademiska Barnsjukhuset Aarhus University Hospital, Skejby Sygehus Akademiska Barnsjukhuset
Avd för blod och tumörsjukdomar Paediatrics Avd för Blod-och tumörsjukdomar
Ing 95 Brendstrupgaardsvej 100 Ing 95
751 85 Uppsala, Sweden 8200 Aarhus N, Denmark 751 85 Uppsala, Sweden
Link, Katarina Moëll, Christian Peyrl, Andreas
The Universityhospital in Malmö Children’s Hospital Novo Nordisk Pharma GmbH
The department of Endocrinology Dept of Paediatrics Opernring 3
205 02 Malmö, Sweden 221 85 Lund, Sweden 1010 Vienna, Austria
Longhi, Alessandra Moser, Andrea Postma, Aleida
Istituto Ortopedico Rizzoli University Children Hospital Graz University Medical Center Groningen
Chemotherapy Div Pediatric Hematology/Oncology Pediatric Oncology
Via Pupilli 1 Auenbruggerplatz 30 Post Box 30001
40136 Bologna, Italy 8036 Graz, Austria 9700 RB Groningen, Netherlands
Lundsten, Ann Muszynska-Roslan, Katarzyna
Barncancerföreningen i Västra Sverige Medical University R
Sweden Pediatric Oncology Radvanska, Jitka
Waszyngtona 17 Teaching Hospital Motol
Lyons, Shoshanah
15-274 Poland Children Clinic Hematology and Oncology
Royal Holloway, Univeristy of London
Department of Clinical Psychology Möller, Torgil R. V Uvalu 84
Egham, Surrey TW20 OBX, United Kingdom Lund University Hospital 150 06, Czech Republic
Regional Tumour Registry Radvansky, Jiri
Lähteenmäki, Päivi
Klinikgatan 22 Charles University 2nd Medical Faculty
Turku University Hospital
221 85 Lund, Sweden Sports Medicine
Dept of pediatrics
Po Box 52 V Uvalu 84
150 00 Prague, Czech Republic
FIN-20521 Turku, Finland N
Löf, Catharina M Niedzielska, Ewa Rebholz, Cornelia Eva
Karolinska Institutet, Department of Pediatrics Akademia Medyczna Swiss Childhood Cancer Registry
146 86 Stockholm, Sweden Klinika Hematologii i Onkologii Dzieciêcej Department of Social and Preventive Medicine
Wroc³aw Finkenhubelweg 11
Bujwida 44 30-345, Poland 3012 Berne, Switzerland
M Nilsson, Ann-Sofie Rechnitzer, Catherine
Magnusson, Susanne
Endokrin Rigshospitalet
Dept of Oncology
Läsvägen 9 Pediatrics
Clinical Sciences
224 67 Lund, Sweden Dept of pediatric oncology 5054, Rigshospitalet
221 85 Lund, Sweden
2100 Copenhagen, Denmark
Nussey, Stephen
Malmberg, Lena
St. Georges Hospital nhs trust Rollof, Lena
Dpt. of Oncology
Endocrinology University Hospital
Onkologikliniken Centralsjukhuset
Blackshaw Road Pediatric Department
651 85 Karlstad, Sweden
London SW17 OQT, United Kingdom 221 85 Lund, Sweden
Martinsson, Ulla
Nyenget, Tove Ross, Emma
Onkologikliniken
Ullevål Universitetssykehus Oslo Leicester Royal Infirmary
Akademiska sjukhuset
Barneavdeling og Poliklinikk Paediatric Oncology
751 85 Uppsala, Sweden
Kirkev.166 Infirmary Square
Mattsson, Elisabet 0407 Oslo, Norway Leicester LE1 5WW, United Kingdom
Public Health and Caring Sciences
Nysom, Karsten Ruud, Ellen
Psychosocial Oncology
Rigshospitalet Rikshospitalet
Uppsala Science Park
Paediatric Haematology/Oncology Dep. of Pediatrics
751 85 Uppsala, Sweden
Section 4064, Blegdamsvej 9 Sognsvannsveien 22
Mehta, Susan DK-2100 Copenhagen, Denmark 0027 Oslo, Norway
Haematology/Oncology
Ryalls, Michael
Great Ormond Street
London WC1N 3JH, United Kingdom O Royal Surrey County Hospital
Opperud, Vigdis Paediatrics
Michel, Gisela Rikshospitalet - Radiumhospitalet Medical Center Egerton Road
University of Bern Montebello Guildford GU2 7XX, United Kingdom
Dept of Social and Preventive Medicine 0310 Oslo, Norway
Finkenhubelweg 22
3012 Bern, Switzerland S
Mitchell, Anne
P Schellong, Guenther
Pal, Annacarin University of Münster
Wellington Hospital Germany
Astrid Lindgrens Barnsjukhus
Paediatrics
Karolinska Universitets sjukhuset Schmiegelow, Kjeld
48B Madras Street, Kandhallah
171 76 Stockholm, Sweden University Hospital Rigshospitalet
Wellington, 6004, New Zealand
Paulides, Marios Pediatric Clinic
Mittal, Rakesh University Hospital for Children and Adolescents Blegdamsvej 9
Kuwait Cancer Control Centre Late Effects Surveillance System 2100 Copenhagen, Denmark
Medical Oncology Loschgestr. 15 Schomerus, Eckhard
Post Box - 1846 91054 Erlangen, Germany Klinikum Augsburg
Hawally – 32019, Kuwait
Pekkanen, Kirsti 1. Kinderklinik
Modan-Moses, Dalit Drottning Silvias Barn och Ungdomssjukhus Stenglinstraße 2
The Edmond and Lily Safra Children’s hospital SU/Östra 86156 Augsburg, Germany
Pediatric Endocrinology Barncancercentrum Avd 322 Schröder, Hildegard
Tel-Hashomer, Ramat-Gan 416 85 Göteborg, Sweden University Hospital
52621, Israel Petersen, Cecilia Dept.: Pediatric Oncology and Hematology
Karolinska Institutet Ratzeburger Allee 160
Pediatric Endocrinology Unit 23538 Germany
Astrid Lindgren Children´s Hospital, Q2:08
171 76 Stockholm, Sweden
12Schuitema, Ilse Thorvildsen, Anne Benedicte van Leeuwen, Flora
Leiden University/VU University Medical Center Rikshospitalet-Radiumhospitalet HF Netherlands Cancer Institute
Maria van Hongarijelaan 4 Center for Shared Decision Making and Nursing Rese Epidemiology
2353 EM Leiderdorp, Netherlands Forskningsveien 2b Plesmanlaan 121
NO-0027 Oslo, Norway 1066CX Amsterdam, Netherlands
Sega-Pondel, Dorota
Wroclaw Medical University Toogood, Andrew Vandecruys, Els
Department of Pediatric Hematology/Oncology/BMT University Hospital Birmingham Ghent University Hospital
ul. Bujwida 44 NHS Foundation Trust Edgbaston Pediatric Hemato-Oncology
50-345 Wroclaw, Poland Birmingham, B15 2TH, United Kingdom De Pintelaan 185
9000 Ghent, Belgium
Sehested, Astrid Turup, Eva
Rigshospitalet Akademiska Sjukhuset Wells, Robert
4064 Barnonkologen U. T. M. D. Anderson Cancer Center
Blegdamsvej 9 751 85 Uppsala, Sweden Pediatrics
2100 Copenhagen Ø, Denmark 1515 Holcombe Blvd, Unit 87
Houston, TX 77030, United States
Shalet, Stephen Michael U
Christie Hospital Uhlig, Helena Wennström, Lovisa
Department of Endocrinology Akademiska Sjukhuset Sahlgrenska Universitetssjukhuset
Wilmslow Road Psykosociala Enheten Sektionen för hematologi
M20 4BX Manchester, United Kingdom Akademiska Barnsjukhuset, ing 95 NBV 2413 45 Göteborg, Sweden
Sklar, Charles A. 751 85 Uppsala, Sweden Widing, Eva
Memorial Sloan-Kettering Cancer Center Urquhart, Tanya Ullevål University Hospital
Department of Pediatrics Sheffield Childrens NHS Foundation Trust Dept og Paediatrics
23 East 20th Street, #6 Nursing Kierkeveien 166
10003 New York, United States C Floor, Stephenson Wing, Western Bank 0407 Oslo, Norway
Slaby, Krystof Sheffield, South Yorkshire, S10 2TH Wiebe, Thomas
Charles University in Prague 2nd Medical Faculty United Kingdom Children´s Hospital Dept of Paediatrics
Department of Sports Medicine 221 85 Lund, Sweden
V Uvalu 84
15006 Prague, Czech Republic
VW Wiklund, Jan-Åke
Wahlgren, Aida Novo Nordisk Scandinavia
Smedler, Ann-Charlotte Pediatric Endocrinology Unit GHT Team
Stockholm University Dep of Woman and Child Health Box 505 87
Dept of Psychology Q2:08 Astrid Lindgrens Children’s Hospital 202 15 Malmö, Sweden
106 91 Stockholm, Sweden 171 76 Stockholm, Sweden
Winter, Anita
Stille, Jenny Wallace, Hamish University Children Hospital Graz
Queen Silvia Children’s Hospital Royal hospital for Sick Children Pediatric Hematology/ Oncology
Centre of Pediatric Oncology Consultant Paediatric Oncologist Auenbruggerplatz 30
416 85 Göteborg, Sweden 17 Millerfield Place 8036 Graz, Austria
Edinburgh EH9 1LF, United Kingdom
Strömberg, Bo Winther, Jeanette Falck
Uppsala University Children’s Hospital Wallenborg, Carina Danish Cancer Society
Deparment of Women’s and Children’s Health Gävle-Dala Barncancerförening Institute of Cancer Epidemiology
Uppsala Sweden Sweden Strandboulevarden 49
751 85 Uppsala, Sweden DK-2100 Copenhagen, Denmark
van Baalen, Manita
Sugden, Elaine Erasmus University Medical Centre Sophia Winther, Marianne
Oxford Radcliffe Hospitals van Ostadeplein 19 Novo Nordisk Scandinavia
Clinical Oncology 5151 SW Rotterdam, Netherlands ABRegion DanmarkArne Jacobsens Allé 15
Churchill Hospital DK-2300 Köbenhavn SDenmark
van den Berg, Marleen
Oxford OX20NA, United Kingdom
VU University Medical Center Wooding, Katherine
Sundberg, Kay Dept. of Paediatrics Morriston Hospital
Uppsala Universitet, Inst.för folkhälso-och vårdve- Po Box 7057 Morriston Swansea
tenskap 1007 MB Amsterdam, Netherlands SA6 6NL United Kingdom
Uppsala science Park
van den Bos, Cor Wynn, Belynda
751 83 Uppsala, Sweden
Emma Children’s Hospital Christchurch Hospital
Sunnvius, Ann Pediatric Oncology and Late Effects Study Group Paediatric Department
Uppsala Barncancerförening Room F8-243, Po Box 22660 Private Bag 4710
Uppsala, Sweden 1100 DD Amsterdam, Netherlands Christchurch, New Zealand
Sällfors Holmqvist, Anna van den Heuvel-Eibrink, Marry M.
Barn- och Ungdomssjukhuset Erasmus MC-Sophia Childrens Hospital Z
221 85 Lund, Sweden Pediatric Oncology Zaletel-Zadravec, Lorna
P.O. Box 2060 Institute of Oncology Ljubljana
3000 CB Rotterdam, Netherlands Zaloska 2
T 1000 Ljubljana, Slovenia
Taj, Mary van der Linden, Gerard H.M.
The Royal Marsden NHS Foundation Trust Erasmus University Medical Centre Sophia
Paediatric Oncology Hematology/Oncology
Downs Road Po Box 2060
Sutton SM2 5PT, United Kingdom 3000 CB Rotterdam, Netherlands
Teixeira, Ana van der Pal, Heleen
Instituto Português de Oncologia Academic Medical Center
Paediatrics Medical Oncology
Rua Castilho, 185, 8º Meibergdreef 9, room F4-224
1070-051 Lisboa, Portugal 1105 AZ Amsterdam, Netherlands
Thomsen, Line van der Sluis, Inge M.
Novo Nordisk Scandinavia Erasmus MC-Sophia Childrens Hospital
ABRegion DanmarkArne Jacobsens Allé 15DK-2300 Pediatric Oncology
Köbenhavn SDenmark P.O. Box 2060
3000 CB Rotterdam, Netherlands
13Invited Speakers
Late Effects Of Treatment Modifications of treatment to minimise late
For Childhood Cancer A:01 complications after childhood cancer:
The Hodgkin Lymphoma experience A:02
Green, Daniel M.
Roswell Park Cancer Institute, Department of Pediatrics, Buffalo, Schellong, Guenther
United States University Children’s Hospital, Haematology/Oncology, Muenster,
Survival after the diagnosis of cancer in children and adolescents has become Germany
the rule. Adult survivors of childhood cancer have concerns regarding tre-
atment effects on their longevity, fertility and offspring. The standardized Hodgkin’s disease (HD) takes a special place amongst cancer diseases of
mortality ratio (SMR) for male five-year survivors who participated in the childhood. Cure rates are very high, but long term survival goes along with
Childhood Cancer Survivor Study (CCSS) was 8.5, and was 18.2 for female a large spectrum of therapy-induced late effects. This is especially proven for
CCSS participants. The most frequent causes of premature mortality are the the therapy concepts applied until 25 to 30 years ago, when radiotherapy
original cancer, cardiac disease and second malignant neoplasms (SMNs). was still extensively practiced and several chemotherapeutic agents were
Data which are population based from the Nordic countries are similar. The given at high cumulative doses now known to produce long-term compli-
SMR for males was 9.2 for males and 14.6 for females. cations. Since the 1970ies many paediatric therapy studies have tried to
Anthracycline antibiotics and direct cardiac irradiation cause cardiac minimise the late consequences by treatment modifications.
morbidity. The risk factors for anthracycline cardiomyopathy include the 1387 patients below 18 y with all disease stages were enrolled in the
cumulative dose of anthracycline received and exposure of the left ventricle first 5 German-Austrian DAL-studies HD-78 to HD-90 between 1978 and
to radiation. Radiation therapy can damage the cardiac valves, coronary arte- 1995 by 104 centres. Following therapy extended long-term surveillance
ries, myocardium and pericardium. Female childhood cancer survivors who has been organised continuously into adulthood (Project HD-Late Effects).
were treated with > 20 Gy have a relative risk (RR) of obesity (body mass in- During the initial years follow-up information was provided by the parti-
dex > 30) of 2.59. The RR of obesity for males was 1.86. Obesity predispo- cipating departments. After the patients had reached adulthood the study
ses individuals for diabetes mellitus, hypertension and dyslipidemia, factors centre established direct contact to them and/or their physicians. At the last
that will interact with known treatment effects on cardiac health. Growth evaluation (January 07) information was available from 78% of the patients
hormone deficiency may underlie several of these abnormalities. from the last 6 years. At last information the median follow-up was 13.4
The fertility of childhood cancer survivors is impaired. The adjusted re- (max. 28.2) y, and median age 26.1 (max. 44.0) y. Overall survival of the
lative fertility of survivors, compared to that of their siblings was 0.85 (95% total group with all treatment modifications was 95% at 10 y and 92% at
CI - 0.78 - 0.92). Fertility may be impaired by the absence of sperm and ova 20 y.
or abnormal uterine structure. The offspring of female CCSS participants Chemotherapy: In the general framework of combined modality tre-
who received pelvic irradiation were at increased risk (RR - 1.84) of weig- atment chemotherapy in the initial DAL-HD-studies consisted of a mo-
hing < 2500 grams at birth. Most chemotherapeutic agents are mutagenic. dification of MOPP. Mechlorethamine was replaced by doxorubicin and
Recent studies have not identified an increased frequency of major conge- cyclophosphamide resulting in OPPA and COPP, respectively. The number
nital malformations, genetic disease or childhood cancer in the offspring of of cycles was reduced according to the risk of disease: 2 OPPA for early
childhood cancer survivors. stages, 2 OPPA + 2 COPP for intermediate and 2 OPPA + 4 COPP for
The standardized incidence ratio (SIR) for a SMN among CCSS parti- advanced stages. Radiotherapy followed chemotherapy. Treatment results
cipants who had a median follow-up of 15.4 years after diagnosis was 6.38. were favourable.
The SIR reported for Nordic pediatric cancer patients who had a mean fol- Late effects: The cumulative incidence of secondary leukaemias/MDS
low-up of 6.1 years after diagnosis was 3.6. Risk factors for SMNs include was 0.5%. Only 1 cardiomyopathy developed in 171 patients without me-
genetic predisposition, gender and treatment factors. Thyroid carcinoma, diastinal irradiation and without additional chemotherapy due to relapse or
breast cancer, brain tumors and skin cancer are among the more frequently second malignancy, (cumulative total doxorubicin dose in all patients 160
diagnosed radiation related SMNs. Tobacco use increases the risk of subse- mg/m2). By contrast, a considerably higher incidences of testicular dysfun-
quent lung cancer in patients who received lung irradiation. CCSS parti- ction were detected primarily by hormonal parameters. Elevated FSH levels
cipants reported smoking rates that were significantly lower than those of were noted in 40% of the examined post-pubertal male patients indicating
the general population. However 19% of males and 17% of females were impairment of spermatogenesis. The prevalence of abnormal findings was
current smokers, increasing their risks for lung disease, heart disease and related to the cumulative doses of procarbazine. In the subsequent studies
SMNs. SMNs may develop after exposure to alkylating agents and topoiso- it was tried to eliminate procarbazine, the main gonadotoxic drug for boys,
merase II inhibitors. from the protocols. In a successful step etoposide was substituted for procar-
Medical care for childhood cancer survivors must be based on accurate bazine in OPPA arriving at OEPA for boys in HD-90 and -95. This combi-
knowledge of the treatment exposures of the survivor and informed assess- nation had no gonadotoxic effect and did not increase the risk of secondary
ment of the survivor by medical professionals. Only 72% of CCSS parti- leukaemias (cumulative incidence at 15 years 0.5%). Next, dacarbazine was
cipants accurately reported their diagnosis. Recall by CCSS participants of substituted for procarbazine in COPP (COPDac). While the efficacy of
treatment with specific chemotherapeutic agents or exact radiation therapy the OEPA /COPDac regimen to control HD has already been proven in
treatment volumes is poor. Exposure specific care will be difficult unless the Pilot HD-2002, testicular function has to be tested in late adolescence or
patient is given a physical and/or electronic record of his/her diagnosis and early adulthood. Radiotherapy: While the radiation doses were 36-40 Gy
treatment. in the first study HD-78 they were stepwise reduced to 20 Gy in the sub-
Future research will be necessary to determine the most effective follow- sequent studies. Extended field was changed to involved field and later to
up program for survivors. Several models, including prolonged follow-up reduced involved field irradiation. Treatment results were not affected by
at a cancer center, transition of care to appropriately trained physicians in a these reductions. In GPOH-HD-95 radiotherapy was omitted in patients
specialty setting, or transition to community physicians supported by com- with complete remission after chemotherapy. This strategy was successful in
puter based practice guidelines, have been suggested. Many current follow- terms of DFS in early, but not in intermediate and advanced stages.
up evaluations are based primarily on expert opinion. Research is necessary Late effects: At the present time it cannot be determined whether the
to document that expert opinion results in care that is cost effective and reduction of radiotherapy has indeed diminished the cumulative incidence
reduces morbidity and/or mortality. Such studies require large sample sizes of secondary solid tumours as intended. A longer follow-up of the patients
and prolonged follow-up. from the low dose studies is needed. Preliminary data from studies with
intermediate doses show some important trends.
14Anthracycline cardiotoxicity in children. Is Childhood Cancer A Chronic Disease?
What is the risk and can we avoid it? A:03 A:04
Kremer, Leontien D’Angio, Giulio
Emma Childrens’ Hospital, Pediatric Oncology, Amsterdam, Department of Radiation Oncology, Philadelphia, United States
Netherlands
Definitions*:
Anthracycline-induced cardiotoxicity is a widely prevalent problem. The 1) Chronic: marked by long duration; relapsing, unremitting
consequences of anthracycline-induced cardiotoxicity are extensive. First, 2) Disease: disquiet (obsolete); disordered normal health status
it can cause a reduction in the amount of anthracyclines that a patient *Oxford Universal Dictionary
was supposed to receive and as a result, the chance of survival of that Background: --- The Erice Conference in November 2006 was conve-
patient can be reduced. Also, it can lead to cardiac death. The risk of ned to address the question, ”Is there such a thing as total cure of childhood
developing heart failure remains a lifelong threat, especially to children cancer?” It is another way of asking whether it is a chronic disease. The con-
who have a long life-expectancy after successful antineoplastic treatment. sensus answer was, ”No”, based on both definitions. There was another issue
Several risk factors for anthracycline-induced cardiotoxicity, like a hig- that was very important to the long-term survivors, their representatives and
her cumulative anthracycline dose, different anthracycline derivates, a hig- the clinicians present in Erice. It was the question, ”When can the patient be
her anthracycline peak dose, radiation therapy involving the heart region, told he/she has been cured?” It elicited several different answers.
female sex, younger age at diagnosis, black race, additional treatment with Discussion: --- The myriad primary and secondary effects entailed in
for example cyclophosphamide or mitoxantrone and presence of trisomy cancer therapy include continuing dis-ease and disease in the patient. Dis-
21 have been identified. quiet is felt not only by members of the family, but by a wider circle that
Serial monitoring of the cardiac function of children receiving an- includes health care workers as well. The effects on these latter--- nurses,
thracycline therapy allows early identification of cardiac damage. During doctors, social workers, clinical laboratory staff, pharmacists, students, et
therapy, the anthracycline dosage can then be adjusted or anthracycline al. --- deserve more attention and study. But is the primary cancer itself not
therapy can be even stopped, which, hopefully, can prevent more cardiac a chronic illness? Does it never recur after a long interval? That is known
damage to occur. Unfortunately, at the moment, there is no evidence on to be true for certain rare entities like the mesenchymal chondrosarcoma.
the most optimal way to monitor cardiac function in children treated with Recent studies indicate that late recurrence of the primary are being seen
anthracyclines. in the more common cancers, too. So when can the patient be told he/she
If cardiotoxicity could be prevented or at least be reduced, higher doses is cured; i.e., the original cancer will never come back? Perspective --- Cu-
of anthracyclines could potentially be used, thereby possibly further in- ring a child of cancer does not render that boy or girl immortal. He/she
creasing cancer survival. Extensive research has been devoted to the iden- is subject to all the ills and misadventures of the general population. This
tification of methods or agents capable of ameliorating anthracycline-in- led Easson about 60 years ago to propose his ”Concept of Cure”. His idea
duced cardiotoxicity. The following methods for primary prevention have was this: the patient can be told that death from the original cancer poses
been identified: 1) Avoiding the use of anthracyclines in the treatment no excess risk when the likelihood of dying of the primary neoplasm is not
of childhood cancer, 2) The use of possible less cardiotoxic anthracycline greater than the risk of death from any cause in age peers in the general
analogues and anthracenediones, 3) Reducing the cumulative dose of an- population. It should be noted that, for those who survive a decade or
thracyclines, 4) Reducing the anthracycline peak dose, 5) Use of cardio- more, second malignant neoplasms (SMNs) appear in increasing propor-
protective agents. tions among the listed causes of death; indeed, in a recent report, recur-
Important insight in the current state of the evidence on anthracycline rence of the primary tumor was in second place. Some SMNs, at least,
cardiotoxicity is provided. could be prevented by strongly discouraging cigarette smoking. Many of
these patients are particularly vulnerable to the other damage caused by
smoking depending on the curative treatments used. Impaired lung fun-
ction if irradiated, is an example. The tobacco companies are targeting
the ’teen and young adult population with candy-flavored cigarettes and
enticing labeling; e.g., a coconut flavored product called, ”Kauai Kolada”.
Surveillance and counseling are needed. Returning to the primary cancer,
the Easson construct avoids unwonted over-optimism or pessimism on
the part of individual physicians. It provides a more solid foundation on
which to express an opinion when a long-term survivor asks, ”Will my
tumor come back to kill me?”
Conclusion: --- The question, ”Is childhood cancer a chronic disease?”
elicits a Talmudic answer, ”Well, it depends ....”
15Neurocognitive sequelae of Neuropsychological consequences
brain tumors in children A:05 of childhood cancer A:06
Grill, Jacques Eiser, Christine
Gustave Roussy Institute, Pediatric and adolescent oncology, University of Sheffield, Psychology, Sheffield, United Kingdom
Villejuif, France Concern about the neuropsychological consequences of cancer and its tre-
As prognosis of brain tumors is improving, concerns are growing for the atment initially focused on treatment of acute lymphoblastic leukaemia
quality of survival. As for other neoplasms, strategies to mitigate sequelae (ALL) in children. Although the earliest reports suggested there were no
have been developped to minimize the use of irradiation. These strategies identifiable effects, burgeoning work in the 1970s and 1980s pointed to
rely on the assumption that irradiation is the principal cause of treatment intellectual deficits for many children. Younger age on diagnosis was iden-
related side effects. However, surgery and chemotherapy may bring ad- tified as a risk factor, as was female gender. There was also much discussion
ditional and substancial morbidity. In the modern age, it is of paramount about whether the deficit was a general one, or specific to certain skills.
importance that all the caregivers are aware of the specific sequelae as- Attention and concentration were viewed as especially vulnerable.
sociated with each treatment modality alone and in combination, before Cranial irradiation was initially seen to be the most likely cause of
definite therapeutic decisions are made. It is now possible for some tumors any deficits, though subsequent work focused on comparisons between
like medulloblastoma to draw algorithms to predict long-term cognitive standard and reduced dose radiation, and later chemotherapy alone. In
outcome based on the principal parameters that can influence IQ : age practice, it is clear that many factors determine neuropsychological outco-
at diagnosis, interval since diagnosis and irradiation volume and dose, mes, including treatment protocols, as well as socioeconomic and family
anatomical and neurologic damage. This later risk factor being the most variables.
important one in our later studies. Many issues remain. Critical is the question of the underlying cause of
Studying the long-term results of patients treated with old-fashioned the condition. Two main hypotheses have been proposed. The first is that
strategies can learn us a lot when choosing a given new strategy. Indeed, treatment disrupts elementary psychological processes such as attention
one can guess the late sequelae of a given modality based on the type of or learning, and this compromises further development and acquisition
refinement of the treatment. In addition, any new modality has to be of subsequent skills. The second involves a physiological process that is
fully evaluated on the long-term (or with appropriate surrogates such as on-going and results in continued neuronal damage.
early MRI changes), before it can be adopted as a standard. Certainly in While the focus of research has been on identifying whether or not
the future, all new protocols will need to incorporate careful evaluation deficits occur, the more pressing question of remediation has received less
of late sequelae attention. Drawing to a large extent on the brain injury rehabilitation
In addition to treatment related risk factors, age at diagnosis is a major literature, several techniques have now been described, including pharma-
predictor for impaired cogniotive outcome. Damage to specific structures cotherapy, cognitive remediation and ecological interventions. The latter
may have a strong impact on further development of brain functions and emphasises the important role of schools and families in acknowledging
this impact may depend on the age at which the structure is damaged. the child’s problems and engaging them in the child’s education.
There will be critical period for each brain region, eg around two years School achievement and acquistion of skills is vital for successful adult
for the cerebellum. We may need to take into account these issues for functioning, and especially so given the excellent survival rates now being
treatment planning in the future. achieved. Waiting until the child is a long-term survivor before conside-
Finally, rehabilitation by dedicated teams is still the best garanty to ring these issues is not acceptable, and regular assessment, and associated
lower the burden of disease and treatment-related late complications. remediation if needed, is vital.
16Second malignant neoplasms and What is the role of the nurse in the
late mortality as complications after late effects practice/clinic? A:08
cancer in childhood and adolescence A:07
Gibson, Faith
Garwicz, Stanislaw UCL Institute of Child Health and Great Ormond Street Hospital for
Division of Pediatric Oncology, Department of Pediatrics, Lund, Children, Centre for Nursing and Allied Health Research, London,
Sweden United Kingdom
Second malignant neoplasms The observations that children treated for Though cure from cancer is not guaranteed, children’s chances of survival
cancer are at increased risk of developing second malignant neoplasms have increased significantly. As a result the paediatric oncology commu-
(SMN) are not new. Starting with single case reports more than four deca- nity is focused on providing appropriate follow-up care to an increasing
des ago, the literature now encompasses more than hundred publications number of cancer survivors. However, while there is theoretical agreement
of various size and quality. Combining elements of pediatric oncology, about how future follow-up care should be designed and delivered the
adult oncology, cancer epidemiology, radiobiology, legislation and sta- current service remains somewhat inconsistent and fragmented. There
tistics, every investigation of SMN must address several methodological remains some uncertainty around ’whom’, ’how’, ’when’ and ’why’ in re-
issues, which are sometimes not readily recognizable. At the same time, lation to follow-up care: with some tensions existing between health care
when interpreting the results, readers should be aware of different ap- professionals and young person’s views. This presentation mainly addres-
proaches in different studies. ses the ’who’ factor in this debate, focusing exclusively on the role of the
In the hospital-based studies, the standardized incidence ratio (SIR) of nurse, but within this context the ’why’ will also receive some attention:
SMN is between 5 and 20 and the cumulative risk at 20 years of follow-up drawing on both professional and service users perspectives.
is between 3% and 12%. In the population-based studies the correspon- Nurses can play a key role in follow-up care by: decreasing the full im-
ding figures are: SIR 3.6 - 6.4 and cumulative risk 2.6% - 3.6%, compared pact of long-lasting effects of treatment; assisting the child/young person
with 0.6% expected. Absolute excess risk (AER) is between 1 and 3.5 cases and family to cope effectively while monitoring and treating late effects;
of SMN per 1,000 person-years. The risk is higher in the patients treated helping them and their family gain perspective on the cancer experience
more recently. so that they can be vigilant toward potential late effects. There is evidence
As SMN, bone and connective tissue tumors, breast cancer, CNS already in existence that supports maximising the role of the nurse in fol-
tumors and thyroid cancer have highest SIR. The interval between first low-up care. For example, nurse-led follow-up clinics have been in place
and second cancer is in average more than 10 years, being shortest for in the USA since 1983, and in the UK there is evidence that nurses have
leukemia and longest for breast cancer and tumors of the digestive tract begun to take a role in long-term follow-up. However, some roles are not
as SMN. Among specific combinations of the first and second cancers, consistent in either approach or intentions and outcomes are rarely de-
especially worrying is the high cumulative risk of breast cancer among scribed, leaving posts fragile when service re-organisations take place. This
women surviving Hodgkin lymphoma. Results of the investigations on presentation draws on data collected from nurses working in late effects
the etiological factors in the development of SMN are partly conflicting. in the UK and elsewhere with the specific aim of capturing a moment in
Genetic factors, radiation therapy, chemotherapy and possibly also relapse time to describe the characteristics of this evolving role. There is a need
of the primary tumor per se, are all incriminated in increasing the risk of to move beyond traditional frameworks of treatment and care that are
SMN, but their quantitative contribution is difficult to establish and it situated in historical professional boundaries in order that we embrace
varies greatly depending on the nature of first and second cancer. enhanced cancer care for survivors.
Late mortality Cumulative mortality among 5-year survivors diagnosed
in sixties through eighties is 8 - 10% at 15 years after diagnosis and 12
- 14% at 25 years. Standardized mortality ratio (SMR) is about tenfold
higher than in the general population. SMR is highest at 5 - 10 years after
diagnosis and decreases with longer follow-up. Absolute excess risk (AER)
is about 7 deaths per 1,000 person-years at risk. Cumulative mortality is
higher in males than females, while SMR is higher in females, depending
on lower background mortality in women. The highest percentage of dea-
ths is observed among patients with Hodgkin lymphoma, CNS tumors
and leukemia. Relapse status in the first 5 years after diagnosis, age at
diagnosis, treatment era and treatment modality appear to be important
prognostic indicators. The pattern of causes of death depends on primary
diagnosis and varies with the lengths of follow-up. While recurrence of the
primary tumor dominates greatly at shorter follow-up, second malignant
neoplasms, cardiac toxicity and pulmonary complications emerge as im-
portant causes of death with longer follow-up. Since mortality continues
to be excessive many years after diagnosis, further long-term follow-up of
survivors of cancer in childhood and adolescence is mandatory.
17Models of Follow Up After Childhood Cancer GH deficiency after childhood cancer –
A:09 whom to treat? A:10
Toogood, Andy Shalet, Stephen, Michael
University Hospital Birmingham NHS Foundation Trust, Birming- Christie Hospital NHS Trust, Endocrinology, Manchester, United
ham, United Kingdom Kingdom
The evolution of multidisciplinary management of malignant disease that In 1981, the first results of the experience with GH treatment were re-
occurs during childhood has led to improved survival into adult life. Ho- ported in 6 children who had survived a brain tumour(CBT). All re-
wever, this success has come at a cost. In excess of 60% of survivors of sponded to GH therapy, and growth rates increased to 6.0-10.1 cm
childhood cancer have one or more on-going medical problem and are at during the first year. Final height outcomes in CBT survivors treated
risk of additional problems such as endocrine dysfunction or second ma- with GH were subsequently reported by various centres, with a signifi-
lignancy. Consequently this cohort of patients require life-long follow-up cant proportion of children reaching final heights above the third centile.
in a service that provides appropriate management of the conditions the A study of the effects of spinal irradiation on final height in 79 CBT pa-
patient already suffers and surveillance for those they may develop in the tients (not treated with GH) estimated the radiation-related spinal height
future. To a certain extent long-term follow-up services have evolved out loss to be at least 9 versus 7 versus 5.5cm when irradiation was given at
of necessity and their nature has been dependent upon local geographical the age of 1 versus 5 versus 10 years, highlighting the vulnerability of very
arrangement of services and personnel who are willing to be involved. young children to suffer the most severe spinal growth retardation.
The ideal service should facilitate seamless care of patients from treat- Another factor, often encountered in CBT survivors, contributes to the
ment in childhood to independent living young adults. Transition bet- relatively poor spinal growth response: early (although less frequent true
ween paediatric and adult services is important. Many patients are lost precocious) puberty, which tends to be of normal duration. The predicted
to follow up during this period so a robust process needs to be in place age of onset of puberty is positively correlated with the age at cranial irradia-
to ensure that the necessary information and the patient are moved bet- tion. Both the radiation osteitis of the spine and abnormal pubertal tempo
ween the two services. Each part of the service must provide education, in the context of early onset contribute to the poor response of sitting height
psychological support and access to specialist facilities appropriate to the to GH treatment. Analysis of auxological data of the last 25 years of GH
patient’s age. treatment in CBT survivors in our unit revealed a gradual improvement in
Further evaluation of current models is required to determine the opti- final height outcome for both cranial irradiation (r=0.5, p=0.03) and crani-
mal follow up strategies of this complex cohort of patients. ospinal irradiation patients (r=0.6, pYou can also read