Der Amyloidose auf der Spur - Kardiologische Symptome, Screening, Diagnose und Behandlung - Innere Medizin Online
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Der Amyloidose auf der Spur
Kardiologische Symptome, Screening, Diagnose und Behandlung
Prof. Dr. Diana Bonderman
Leiterin der Abteilung für Kardiologie, Klinik Favoriten
Abteilung für Kardiologie, Medizinische Universität Wien
1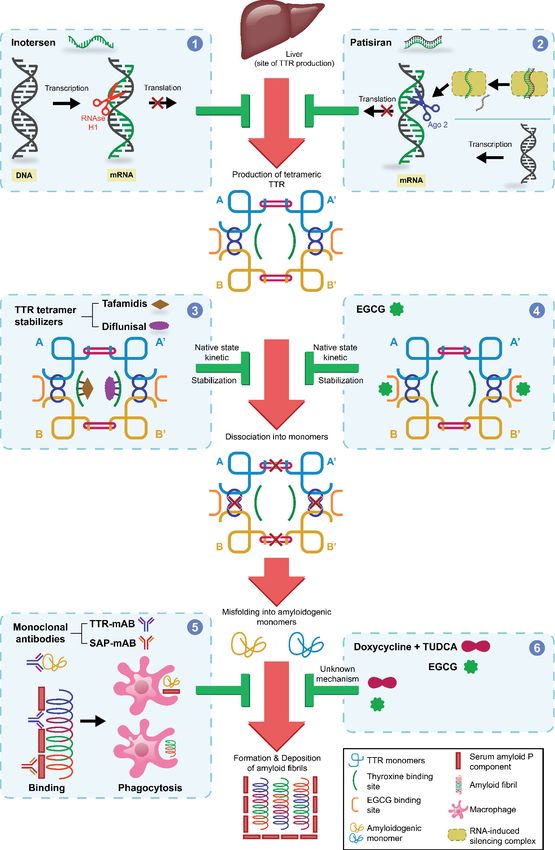
Disclosures
Honoraria and research grants from
Actelion, Johnson & Johnson, AOP, United
Therapeutics, GSK, Pfizer, Böhringer Ingelheim, Daiichi
Sankyo, Alnylam, Akcea, Shire, Novartis, MSD, Bayer,
Zoll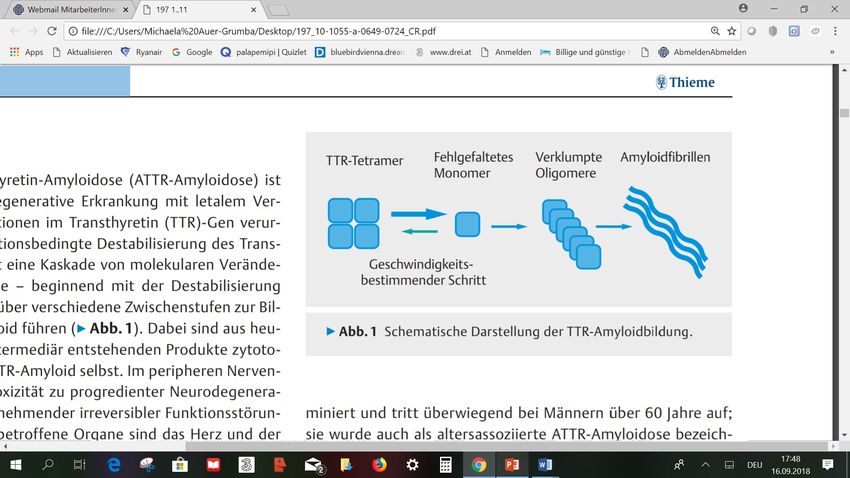
Diagnose und Therapie der kardialen Amyloidose – ein
interdisziplinäres Konsensusstatement
Diana Bonderman1; Gerhard Pölzl2; Klemens Ablasser3; Hermine Agis4;
Stefan Aschauer1; Michaela Auer-Grumbach5; Christina Binder1; Jakob
Dörler2; Franz Duca1; Christian Ebner6; Marcus Hacker7; Renate Kain8;
Andreas Kammerlander1; Matthias Koschutnik1; Alexander Stephan
Kroiss9; Agnes Mayr10; Christian Nitsche1; Peter P. Rainer3; Susanne
Reiter- Malmqvist 11; Matthias Schneider1; Roland Schwarz12; Nicolas
Verheyen3; Thomas Weber13; Marc Michael Zaruba2; Roza Badr Eslam1;
Martin Hülsmann1; Julia Mascherbauer1
Geteilte Erstautorenschaft: Bonderman – Pölzl
Wiener Klinische Wochenschrift 2020
Systemische Erkrankung
4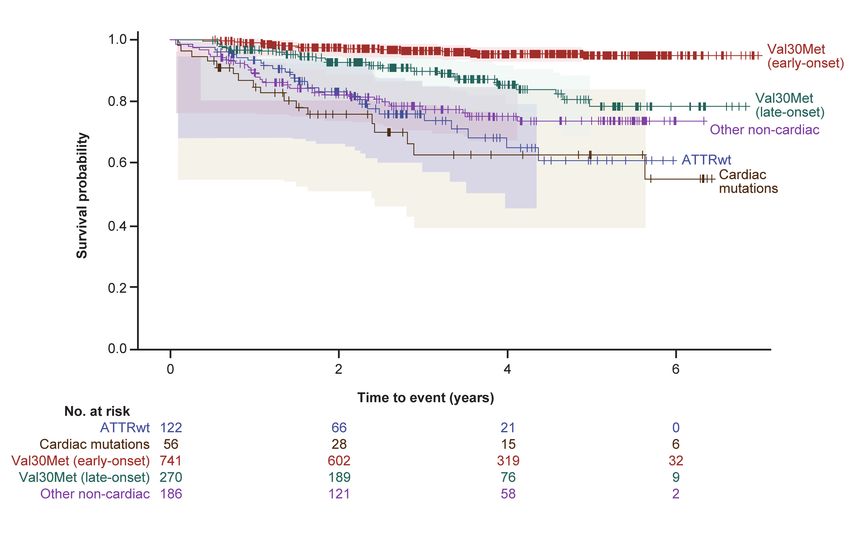
Oncology &
Hematology
Cardiology
Nephrology
Radiology & Pathology &
Nuclear Imaging Molecular Pathology
Gastroenterology
Transfusionmedicine
Rheumatology
Bone Marrow TX
Study - Amyloidosis
HTX, NTX, LTX Surgery
Center Center Vienna
Interdisciplinary Amyloidosis Center
Medical University Vienna
Organisational unit Presentation title / topic OR Presenter's name
5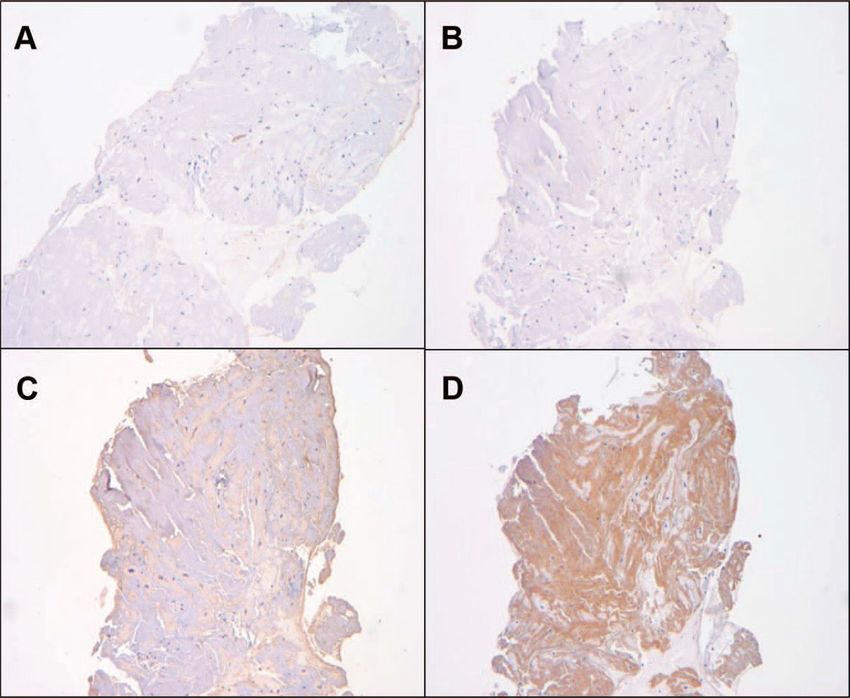
Klassifizierung kardialer Amyloidosen
Ando Y et al., Arch Neurol 2005 Falk R et al., N Engl J Med 1997
Merlini G et al., J Intern Med Sekijima Y et al. Curr Pharm Des 2008
6
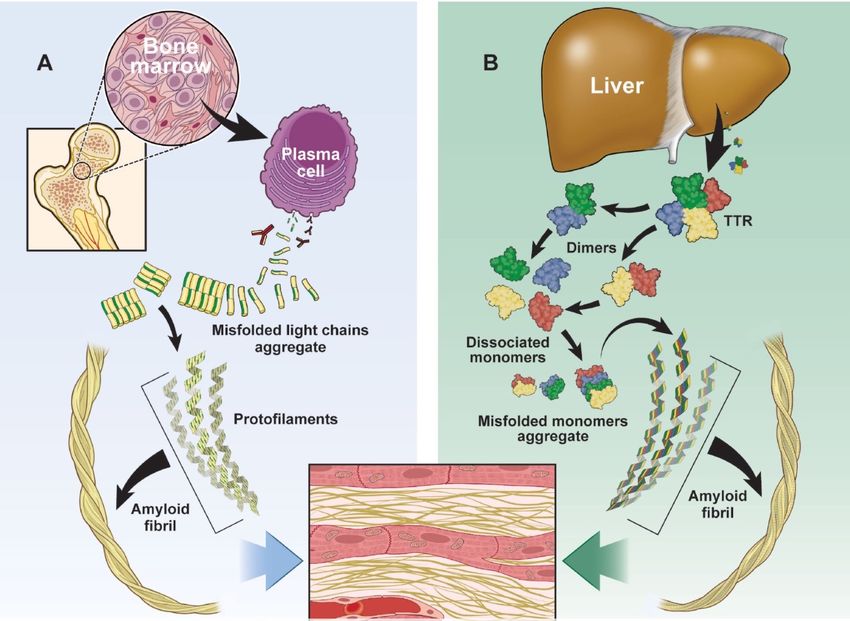
AL ATTR
7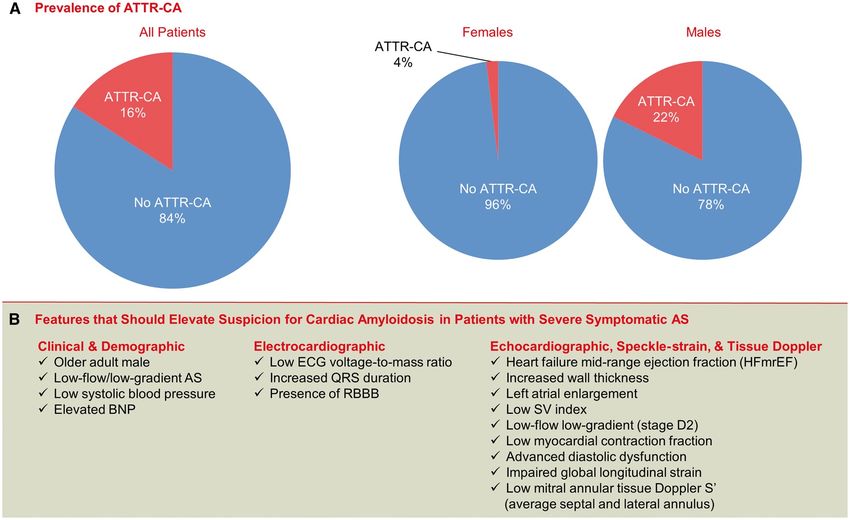
Pathomechanismen
Hund E et al; Aktuelle Neurologie, September 2018 8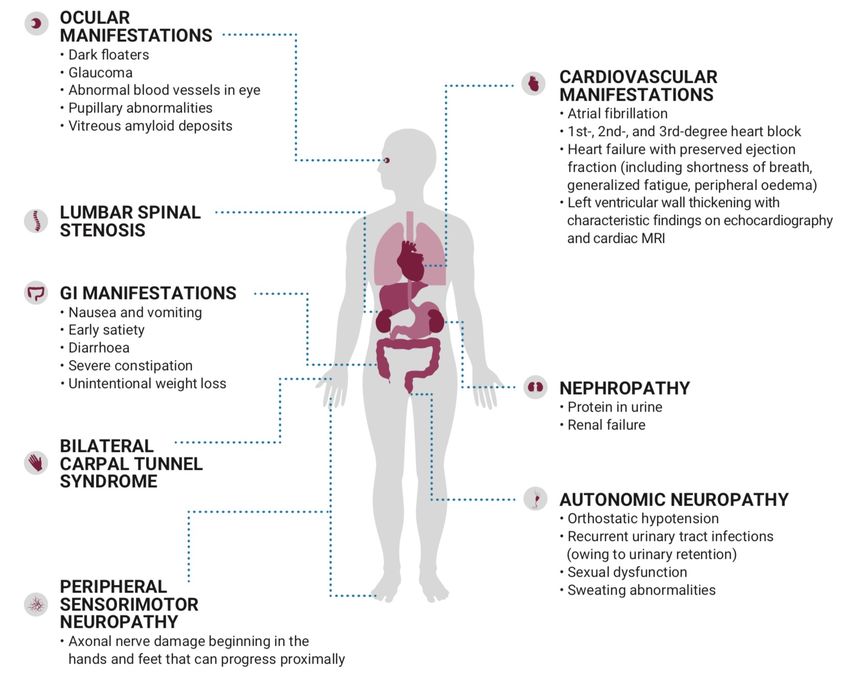
Pathophysiologie: Amyloidablagerungen
9
Echokardiographie: Amyloidose
10Echokardiographie: Amyloidose
99mTc-DPD Szintigraphie
Grading system according to Perugini et al. JACC 2005 12Magnetresonanztomografie bei kardialer Amyloidose
Myokardbiopsie: Histologie
Lichtmikroskop Polarisationsmikroskop
Kongorot-Färbung von myokardiale Gewebe eines Patienten mit kardialer Amyloidose
Ruberg et al. Circulation 2012 14Myokardbiopsie: Histologie
Kappa-Leichtketten Lambda-Leichtketten
Serum Amyloid A TTR Amyloid
TTR-Amyloid Kardiomyopathie nach immunhistochemischer Färbung mit Antikörper
Ruberg et al. Circulation 2012 15Diagnosepfad kardiale Amyloidose
Schritt 2:
Weiterführende Abklärung des klinischen Verdachts auf kardiale Amyloidose
(Erstversorger und / oder lokales Zentrum)
Kard. MRT entweder vor oder
Kard. MRT: nach Knochen-Scan –
• Diffuses LGE je nach lokaler Verfügbarkeit
• Erhöhtes extrazelluläres und Expertise
Volumen und T1 Mapping
Leichtketten-Amyloidose (AL) Transthyretin-
• Serum: Elphor, Immunfixation, Amyloidose (ATTR)
quantitative Bestimmung von
Immunglobulinen und freien
und
Leichtketten • Knochen-Scan
• Harn: Elphor, Immunfixation,
Quantifizierung von
Immunglobulinen und freien Schritt 3:
Leichtketten , Bestimmung der Weitere Abklärung gemäß AL- und ATTR-Status (spezialisiertes Zentrum)
Protein/Kreatinin-Ratio sowie der
Albumin/Kreatinin-Ratio im 24-
Stunden-HarnTTR (Transthyretin) -Gen • Exons: 4 • Aminosäuren: 147 • > 120 Mutationen bekannt • Häufigste Mutation Val30Met (Val50Met): endemisch in Portugal, Schweden, Frankreich, … • Einteilung in Val30Met und Non-Val30Met Patienten
Geographische Verteilung
p.Val40Ile
p.His108Arg p.His108Arg
p.Val50Met p.His108Arg
p.His108Arg p.Val50Met
p.Val113Leu
p.Ile127Phe
p.Val40Ile p.Ile127Phe19 González-López E et al. Eur Heart J. 2017
González-López E et al. Eur Heart J. 2017 20
Kardiale Amyloidose bei HFpEF
21Kardiale Amyloidose bei TAVI Patienten
22
Castanõ et al. Eur Hart J. 2017Therapie der kardialen Amyloidose
Supportive Therapie
Diuretika
Absetzen von Antihypertensiva und bradykardisierenden Medikamenten
Behandlung oder Schutz vor Arrhythmien (Kardioversion, Ablation, PM, ICD/Lifevest)
AL Amyloidose TTR Amyloidose
Chemotherapie TTR Stabilisatoren
AntikörpertherapieTherapeutic strategies in TTR amyloidosis Doxycyclin, IDOX, TUDCA und Diflunisal sind nicht für die Behandlung der ATTR-CM zugelassen. Gene Silencer sind nicht für die Behandlung von ATTR-CM zugelassen Ueda M. et al. Translational Neurodegeneration. 2014, 3:1
Doxycyclin, IDOX, TUDCA und Diflunisal sind nicht für die Behandlung der ATTR-CM zugelassen. Gene Silencer sind nicht für die Behandlung von European Journal of Heart Failure, Volume: 22, Issue: 1, Pages: 39-53, First published: 07 January 2020, DOI: (10.1002/ejhf.1695) ATTR-CM zugelassen
44 M.L. Müller et al.
Table 2 Overview of all studies analysing the effect of various pharmaceuticals on transthyretin-associated amyloid
polyneuropathy (status as of June 2019)
Author Patients Application Primary outcomes
............................... ............................................
n TTR status Dose Time (months)
(ATTRv /−wt)
...........................................................................................................................................
Tafamidis
Coelho et al.27 128 ATTRv (V30M only) 20 mg once daily 18 NIS-LL
Norfolk QoL-DN
Coelho et al.28 85 ATTRv (V30M only) 20 mg once daily 12 (extension) NIS-LL
Norfolk QoL-DN
Merlini et al.32 21 ATTRv (non-V30M) 20 mg once daily 12 TTR stabilization
(week 6)
Barroso et al.82 93 ATTRv (all mutations) 20 mg once daily 42 (extension) NIS-LL
Norfolk QoL-DN
Lozeron et al.31 36 Advanced ATTRv 20 mg once daily 30 NIS-LL/UL
(V30M only)
Cortese et al.83 61 ATTRv (all mutations) 20 mg once daily 36
Not defined, but
outcomes included
NIS and NIS-LL
Planté-Bordeneuve et al.84 43 ATTRv (all mutations) 20 mg once daily 24 NIS
...........................................................................................................................................
Diflunisal
Berk et al.18 130 ATTRv (all mutations) 250 mg twice daily 24 NIS+7
Sekijima et al.85 40 ATTRv (all mutations) 250 mg twice daily 38 (mean) Not defined
Takahashi et al.86 6 ATTRv (V30M only) 250 mg twice daily 53 (mean) Not defined
...........................................................................................................................................
Inotersen
Benson et al.51 (NEURO-TTR) 172 ATTRv (all mutations) 300 mg once a week
mNIS+7 15
Norfolk QoL-DN
...........................................................................................................................................
Patisiran
Adams et al.62 (APOLLO) 225 ATTRv (all mutations) 0.3 mg/kg bodyweight 18 mNIS+7
every 3 weeks
ATTRv, variant transthyretin amyloidosis; ATTRwt, wild-type transthyretin amyloidosis; NIS-LL/UL, Neuropathy Impairment Score in the Lower Limbs/Upper Limbs; QoL-DN,
Quality of Life Diabetic-Neuropathy; TTR, transthyretin; (m)NIS+7, (modified) neuropathy impairment score +7.
>1200 mg) and liver (especially at >2000 mg), as assessed by SAP Findings concerning ATTR-associated
..............................
scintigraphy and liver stiffness, in a dose-dependent fashion.81 An
polyneuropathy
European Journal of Heart Failure, Volume: 22, Issue: 1, Pages: 39-53, First published: 07 January 2020, DOI: (10.1002/ejhf.1695) Diflunisal ist nicht für die Behandlung der ATTR-CM zugelassen.
effect on cardiac amyloid deposits could not be shown, although
transient increases in N-terminal pro-brain natriuretic peptide Tafamidis has been evaluated in a total of seven studies with
(NT-proBNP) were interpreted as the initiation of a mechanism primary endpoints concerning polyneuropathy. Due to a lack of
for potential cardiac amyloid clearance.81 validated outcome measures for ATTR-associated polyneuropa-
thy in particular, all studies used scores with previously demon-
strated validity in diabetic polyneuropathy.90,91 These included the
Clinical efficacy – what do we response to treatment (hATTR amyloidosis is a life-threatening disease that can progress
rapidly1-5
Rapid disease progression2
• A natural history study in the United States found that 41% of patients with hATTR amyloidosis died
of inanition from progressive peripheral & autonomic neuropathy3
• The median survival is 4.7 years following diagnosis4 with a reduced survival of 3.4 years for patients
presenting with cardiomyopathy5
• References: 1. Ando et al. Orphanet J Rare Dis 2013;8:31. 2. Araki et al. Proc Jpn Acad 2010;86: 694-706. 3. Gertz et al. Mayo Clin Proc 1992;67(5):428-40.
4. Swiecicki et al. Amyloid 2015;22(2):123-31. 5. Sattianayagam et al. Eur Heart J. 2012 May;33(9):1120-7Survival: Phenotype
Eur Heart J 2019Survival: Genotype
Eur Heart J 2019Emerging therapies in transthyretin amyloidosis 45
Table 3 Overview of all studies analysing the effect of various pharmaceuticals on transthyretin-associated amyloid
cardiomyopathy (status as of June 2019)
Author Patients Application Primary outcomes
............................................. ........................................
n TTR status Dose Time (months)
...........................................................................................................................................
Tafamidis
Damy et al.87 21 ATTRv (non-V30M) 20 mg once daily 12 TTR stabilization (week 6)
Maurer et al.29 35 ATTRwt (89%) & 20 mg once daily 12 TTR stabilization (week 6)
ATTRv (11%)
Maurer et al.30 (ATTR-ACT) 441 ATTRwt and ATTRv 20 mg or 80 mg once 30 All-cause mortality
daily
Cardiovascular-related
hospitalizations
...........................................................................................................................................
Diflunisal
Castaño et al.88 13 ATTRv and ATTRwt 250 mg twice daily 11 (mean) Not defined (exploratory
cardiac outcomes)
...........................................................................................................................................
Patisiran
Solomon et al.89 (APOLLO) 126 (cardiac ATTRv (all mutations) 0.3 mg/kg bodyweight 18 mNIS+7
subpopulation) every 3 weeks
...........................................................................................................................................
Doxycycline and TUDCA
Karlstedt et al.67 53 ATTRwt (89%) & Doxycycline 100 mg 22 (median) None (retrospective
ATTRv (11%) (2x/d) and analysis of clinical data)
ursodeoxycholic
acid 250 mg (3x/d)
ATTRv; variant transthyretin amyloidosis; ATTRwt, wild-type transthyretin amyloidosis; TTR, transthyretin; TUDCA, tauroursodeoxycholic acid; mNIS+7, modified neuropathy
impairment score +7.
(n = 65) once daily for 18 months. Whilst they could not show
27 single-arm open-label study in non-V30M patients discussed below
Doxycyclin, IDOX, TUDCA und Diflunisal sind nicht für die Behandlung der ATTR zugelassen. Gene Silencer sind nicht für die Behandlung von
........................................
significant differences in the intention-to-treat population, analysis reinforced these results in V30M patients for a treatment duration
ATTR-CM zugelassen of up to 6 years.82
of the efficacy-evaluable population showed significantly more
NIS-LL response (60.0% vs. 38.1%, P = 0.041) and less change in Unfortunately however, non-V30M ATTRv patients (n = 18)
the Norfolk QoL-DN (0.1 vs. 8.9 points, P = 0.045), suggesting progressed in respect to neurologic dysfunction (least-squares
European Journal of HeartinFailure,
mean change NIS-LL Volume: 22, Issue:
of 14.2 points 1, Pages:and
in 48 months) 39-53, First
quality of published: 07 January 2020, DOI: (10.1002/ejhf.1695)
a decelerated deterioration of neurological function that led to
preserved quality of life in patients treated with tafamidis. In life (least-squares mean change in Norfolk QoL-DN of 24.8 points
particular, tafamidis prevented muscle weakness, especially at distal in 48 months), despite being treated with tafamidis.82 Preceding
these findings, Merlini and colleagues published congruent results
joints, reduced the loss of small nerve fibre function and improved
for a variation of non-V30M mutations from a phase 2 open-label
nutritional status, as measured by modified body mass index.27
study (n = 21).32 Based on equal results, they concluded that
These results could be replicated in an open-label exten-
tafamidis elicits similar effects across different non-V30M muta-
sion study, in which all patients received tafamidis 20 mg for
tions. However, in light of the small number of participants, this
12 months (n = 85), indicating sustained efficacy of tafamidis over
conclusion appears speculative. Additionally, they found that neuro-Transthyretin Amyloidosis Cardiomyopathy
Clinical Trial
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
32ATTR-ACT: Ziel
Ziel der Studie war die Erfassung der
• Wirksamkeit
• Sicherheit und
• Verträglichkeit
der oralen Einnahme von 20mg oder 80mg Tafamidis meglumin (1x täglich) im Vergleich
zu Placebo über einen Zeitraum von 30 Monaten bei Wildtyp oder hereditären ATTR-CM
Patienten mit zusätzlicher Behandlung laut lokalem Standard-of-care.
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
33ATTR-ACT Studiendesign
30-monatige Behandlungsphase,
zusätzlich zum lokalen Behandlungsstandard
Männer & Frauen,
Randomisierung
18-90 Jahre Tafamidis 80 mg 1 x täglich
Screening Tafamidis 20 mg 1x täglich Extensionstudie
Placebo 1x täglich
• 441 Patienten mit Wildtyp oder hereditärer Amyloidose wurden in die randomisierte Studie eingeschlossen
• Studienteilnehmer wurden in einer 2:1:2 Ratio zu 80mg, 20mg Tafamidis und Placebo randomisiert.
• Die Stratifizierung erfolgte hinsichtlich Genotyp (Wildtyp und Hereditär) und Schweregrad der Erkrankung (NYHA Klasse)
• Es wurde angenommen, dass mit 400 Patienten in der Studie eine statistische Trennschärfe von mindestens 90% erreicht werden würde, um unter
einer Behandlung mit Tafamidis eine 30%ige Reduktion der Mortalität, eine Reduktion der kardiovaskulär-bedingten Hospitalisierungen von 2,5 auf 1,5
oder beides zu erreichen.
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
34Einschluss- und Ausschlusskriterien
Einschlusskriterien Ausschlusskriterien
• Transthyretin-assoziierte Kardiomyopathie (wtATTR oder
hATTR) bestätigt durch kardiale oder nicht-kardiale Biopsie, • New York Heart Association (NYHA) Klasse IV Herzinsuffizienz
Immunhistochemischer Analyse, Szintigraphie oder • Leichtketten-Amyloidose (AL)
Massenspektrometrie
• Vorhergegangene Leber- oder Herztransplantation oder Implantation
eines ICD (implantierbarer Kardioverter/Defibrillator)
• Kardiale Beteiligung bestätigt durch enddiastolische
• Vorangegangene Behandlung mit Tafamidis
intraventrikuläre Wanddicke von >12mm im Echo
• Krankengeschichte mit Herzinsuffizienz (HF) mit zumindest
einer vorhergehenden HF-bedingten Hospitalisierung oder
klinischen Evidenz für Herzinsuffizienz (ohne Hospitalisierung),
welche eine Behandlung mit Diuretika zu Folge hatte.
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
35Ergebnisse zur Wirksamkeit
• Primärer Endpunkt
• Eine hierarchische Kombination aus Gesamtmortalität, gefolgt von der Häufigkeit
der kardiovaskulär-bedingten Hospitalisierungen verglich die gepoolten Tafamidis
Daten mit jenen von Placebo mittels der Finkelstein-Schoenfeld Methode
• Die wichtigsten sekundären Endpunkte veränderten sich vom Studienstart bis Monat 30
• 6 Minuten Gehtest (6MGT)
• Kansas City Cardiomyopathy Questionnaire - Overall Summary (KCCQ-OS) Score
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
36Demographische Baseline Charakteristika
Charakteristika Tafamidis gepoolt (N=264) Placebo (N=177)
Alter, Durchschnitt (SD) 74.5 (+/- 7.2) 74.1 (+/- 6.7)
Männlich, n (%) 241 (91.3) 157 (88.7)
hATTR, n (%) 63 (23.9) 43 (24.3)
wtATTR, n (%) 201 (76.1) 134 (75.7)
Ethnizität, n (%)
Kaukasisch 211 (79.9) 146 (82.5)
Afro-Amerikanisch 37 (14.0) 26 (14.7)
Asiatisch 13 (4.9) 5 (2.8)
andere 3 (1.1) 0
mBMI, mean (SD) 1058.8 (173.8) 1066.4 (194.4)
mBMI= modified Body Mass Index, hATTR= hereditäre Transthyretin Amyloidose, wtATTR= Wildtyp Transthyretin Amlyoidose, n=Anzahl
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
37Klinische Baseline Charakteristika
Charakteristika Tafamidis gepoolt (N=264) Placebo (N=177)
LV Auswurfsfraktion, Durchschnitt (SD) 48.4 (10.3) 48.6 (9.5)
Interventrikuläre Wanddicke, Durchschnitt (SD) 16.7 (3.8) 16.2 (3.5)
LV Posteriore Wanddicke, Durchschnitt (SD) 17.0 (3.9) 16.7 (4.1)
LA anterior-posterior Durchmesser, Durchschnitt (SD) 43.8 (7.0) 43.7(6.1)
LV Schlagvolumen, Durchschnitt (SD) 45.8 (16.1) 45.1 (16.9)
Globaler Longitudinalstrain, Durchschnitt (SD) -9.3 (3.5) -9.4 (3.6)
NYHA Klasse, n (%)
NYHA Klasse I 24 (9.1) 13 (7.3)
NYHA Klasse II 162 (61.4) 101 (57.1)
NYHA Klasse III 78 (29.5) 63 (35.6)
NT-proBNP, Median (Q1, Q3) 2995.9 (1751.5, 4861.5) 3161.0 (1864.4, 4825.0)
Troponin I, Median (Q1, Q3) 0.14 (0.09, 0.20) 0.14 (0.08, 0.19)
LV, Linksventrikulär; SD, Standard deviation; LA, linkes Atrium; NYHA, New York Heart Associaten; NT-proBNP, N-terminal pro b-type natriuretic peptide; Q, Quartile
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
38Reduktion der Gesamtmortalität unter Tafamidis 1
Cox-proportional-Hazardmodell
NNT (nach 2.5 Jahren)= 7,5 2
• 30% Reduktion der Gesamtmortalität mit Tafamidis verglichen zu Placebo (HR= 0,70; 95% CI, 0.51 - 0.96)
• 33% Reduktion der Gesamtmortalität, wenn Herztransplantationen und Implantationen eines mechanischen Herz-Kreislaufunterstützungssystems nicht als Tod gewertet wurden (HR=0.67;
95% CI, 0.49 - 0.94)
NNT= Number needed to treat
1. Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016; 2. Maurer MS & Mann DL, JACC Basic Transl Sci 2018, 3(6):871-873
40Häufigkeit der kardiovaskulär bedingten
Hospitalisierungen
Im Vergleich zu Placebo kam es in der mit Tafamidis-behandelten Gruppe zu einer 32%igen Reduktion der
Hospitalisierungsrate!
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
41Gesamtmortalität und CV- bedingte Hospitalisierungsrate
im Voraus festgelegte Subgruppen
Insgesamt waren die Gesamtmortalität als auch die CV-bedingte Hospitalisierungsrate niedriger unter Tafamidis als bei
Placebo
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
42Wichtige sekundäre Endpunkte
6-Minuten Gehtest und KCCQ-OS
In Monat 30 zeigte sich unter Tafamidis eine geringere Reduktion der Gehstrecke im 6-MGT (75,68m [Standardfehler, ± 9,24m; pVerträglichkeitsprofil von Tafamidis
• Tafamidis wurde im Allgemeinen sehr gut vertragen und zeigte ein vergleichbares Verträglichkeitsprofil wie Placebo
• Nebenwirkungen waren mild bis moderat
• Ein dauerhaftes Absetzen der Medikation wurde häufiger in der Placebogruppe als in der Tafamidisgruppe
beobachtet
• Die häufigsten Nebenwirkungen bei der Tafamidisgruppe, im Vergleich zur Placebogruppe: Flatulenz (4,5 % vs 1,7 %)
und Anstieg der Leberfunktionsparameter (3,4 % vs 1,1 %). Ein kausaler Zusammenhang wurde nicht festgestellt.
• Durchfälle und Harnwegsinfekte waren seltener unter Tafamidisbehandlung als bei Behandlung mit Placebo (12.1%
vs 22.0% und 9.5% vs 15.3%)
Maurer MS et al, N Engl J Med. 2018, 379(11):1007-1016
44EMA Zulassung für Vyndaqel 61mg bei ATTR-CM
Februar 2020
• Im Februar 2020 wurde von der EMA die positive CHMP Empfehlung vom 12.12.2019 angenommen.
• Vyndaqel 61mg wurde als ‚Orphan medicinal product for human use‘ in der EU als erstes Medikament zur
Behandlung der Wildtyp oder hereditären kardialen Transthyretin Amyloidose zugelassen
• Vyndaqel 61 mg (Tafamidis) entspricht 80 mg Tafamidis-Meglumin. Tafamidis und Tafamidis-Meglumin sind auf
Basis der mg-Angabe nicht gegeneinander austauschbar.
CHMP, Committee for Medicinal Products for Human Use; EMA, European Medicines Agency
49TIMELINE
SPECT/CT SPECT/CT
SUVmax: 19.84 SUVmax: 14.19
SUVpeak: 18.95 SUVpeak: 13.27
SUVmean: 10.65 Baseline Follow Up SUVmean: 8.31
50CLINICAL CASE
PATIENT MEDICAL
HISTORY
NYHA III, progressive
AGE: 57
GENDER: Female
HEIGHT: 172 cm
WEIGHT: 60 kg
BP: 135/95 mmHg Recurrent pleural effusions Diziness
HR: 91 bpm
No chest pain No syncopes
5
2PHYSICAL
EXAMINATION
Normal heart
sounds,
Rales, bilateral
regular rhythm
Carpal tunnel
surgery
Mild edema,
bilateral
5
3FAMILY HISTORY
FATHER MOTHER
Died at age 65 due to
heart failure associated Died at age 69 due to
with coronary artery myocardial infarction.
disease.
- PND III (wheel chair)
SON & DAUGHTER
Healthy.
5
4ECG
Das Bild
kann nicht
angezeigt
werden.
26
.0
7.
20
18
13
:4
9:
41
(A
HK
I2
M
R
IW
)
5
5LABORATORY
TESTING
1773 pg/mL
NT-pro BNP Troponin T
68 ng/L
5
6ECHO
5
7ECHO REPORT
- Hypertropic non-obstructive CM (IVS: 23 mm)
- Moderately reduced LVF, GLS: -11% (“apical sparing“)
- Severely enlarged LA, mildly enlarged RA
- Mildly reduced RVF
- Severe MR
- Pleural effusion, bilateral
5
8DISCUSSION PHYSICIAN #3
Bone scintigraphy!!
PHYSICIAN #1
Positive family history of CVD
and elevated Troponin T. We
need to exclude coronary artery
disease.
PHYSICIAN #2
HCM and apical sparing, we
should order a cardiac MRI.
5
9CARDIAC MRI
- LVF: 53%, RVF: 51%
- Late gadolinium enhancement
RVEDV: 148ml
- T1 time: 1161 ms
RVEF: 42%
- ECV: 66%
- Severe MR
- Pleural effusion, bilateral
- No pericardial effusion
60CORONARY ANGIOGRAPHY RIGHT
HEART CATHETERIZATION
- Normal angiography
RVEDV: 148ml
- Postcapillary PH
RVEF: 42%
- mPAP: 49 mmHg
- PCWP: 29 mmHg
- LVEDP: 29 mmHg
61BONE
SCINTIGRAPHY
- Grade 0: no cardiac uptake and normal
bone uptake
- Grade 1: cardiac uptake which is less
than bone uptake
- Grade 2: cardiac uptake with intensity Grade 3
similar to or greater than bone uptake
- Grade 3: cardiac uptake with much
reduced or absent bone signal
62
Perugini E et al. J Am Coll Cardiol. 2005 Sep 20;46(6):1076-84.DISCUSSION
It looks like an ATTR amyloidosis,
but we should perform
immunofixation of
serum and urine and check for
pathological light-chains.
63LABORATORY
TESTING
Urine immunofixation:
No pathological light chains Serum immunofixation: No paraprotein
No paraprotein
64PHYSICIAN #3
DISCUSSION Analysis of the TTR
gene!!
PHYSICIAN #1
AL amyloidosis was
excluded. She has ATTR
amyloidosis, but is only
57 year old...
PHYSICIAN #2
... and positive family
history for PNP.
65ANALYSIS OF THE
TTR GENE
Mutation: His108Arg
66TIMELINE
Atrial Afib -> 2x eCV
fibrillation Atrial
4x nsVT 2x fast VT -> fibrillation
ICD shock
24 hour ECG Single-chamber- Isthmus
(Holter) ICD-system ablation
67THANKS
68ZUSAMMENFASSUNG: DIAGNOSE UND THERAPIE DER KARDIALEN AMYLOIDOSE
DRAN DENKEN, KLINISCHE RED FLAGS, RISIKOGRUPPEN
Stabilizer:
• Tafamidis 61mg 1x1 seit Februar 2020 zugelassen, reduziert die Mortalität und
Hospitalisierungraten
• Andere Stabilizer (AG 10) derzeit in klinischer Erprobung
Silencer:
• Inotersen und Patisiran derzeit nur für familiäre PNP Stadium 1 und 2 zugelassen, Daten zur
Amyloidkardiomyopathie aus Subgruppen der Zulassungsstudien
• Beide Substanzen –zum Teil in modifizierter Formulierung- derzeit in klinischer Erprobung
Offene Fragen:
• Optimaler Behandlungsbeginn? Behandlungsabbruch? Kombinationstherapien? Kosten?DANKE FÜR IHRE AUFMERKSAMKEIT
You can also read

















































