Cook In' - Business School Alliance for Health Management
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Cook In’
Providing nourishing ingredients to inspire healthy Cook In’
Jennifer Eftychiou
Anna Okoniewski
Monica TraczikExecutive summary
Cook In’ aspires to reduce the healthcare costs associated with chronic conditions by
inspiring single mothers in low income neighborhoods of the South Bronx in New York City to
lead healthy lifestyles through the delivery of meal kits designed to create tasty, culturally
influenced, nutrient-dense meals. Very few Americans follow healthy living guidelines and
recommendations, and the rates of obesity and chronic illness continue to rise. Particularly in
low-income communities, access to healthy living resources, such as grocery stores and health
clubs are scarce, unaffordable, or lacking completely. For single mothers living in shelters below
the poverty line without access to a vehicle and with few grocery stores within walking distance,
cooking healthy, nutritious meals for themselves and their children can be particularly
complicated. Fast food chains advertising two for $5 value meals and including toys in kid’s
meals make healthy eating even more challenging.
Our target community is single mothers in low income neighborhoods of the South Bronx
identified as being overweight, obese, and/or diabetic. A focus group with women in this
community confirmed a strong desire and need for healthy ingredients, and highlighted the
positive experience associated with cooking at home, preferences for choice of meals, and
standards for freshness of ingredients.
Our proposed meal-kit delivery service addresses the many barriers of access to healthy
food that single mothers living in low-income communities face. This proposed solution will
begin as a grant-funded pilot program, partnering with FreshDirect for purchasing ingredients, a
consulting nutritionist for recipe development, and local primary care clinics for referring
customers. Staff hired directly from the community will prepare and deliver meal kits to
customers once per week. Data on patient outcomes will be measured during the pilot phase to
show the impact of healthy eating on chronic conditions. Significant positive outcomes can
demonstrate opportunities for funding by insurance companies. We will begin monetizing our
business after six months of grant funding by selling meal kits to mothers with families in the
South Bronx that are not part of the pilot program in order to grow into a self-sustaining
business. Scaling will occur in three phases: expanding initially within the target community,
expanding product offerings, and expanding geographically.
The Problem
Chronic diseases, such as heart disease, cancer, diabetes, and obesity are leading causes
of death in the US and are the leading drivers of the nation’s health care costs, accounting for
hundreds of billions of dollars in health care spending every year.i Current estimates for these
costs range from $147 billion to nearly $210 billion per year. In addition, chronic disease impacts
job absenteeism, costing billions of dollars annually and negatively impacting productivity.ii
Chronic diseases are often preventable or manageable and are caused by unhealthy
lifestyles and risky behaviors including smoking, poor nutrition, lack of physical activity, and
excessive alcohol use. Evidence demonstrates that healthy eating patterns and regular physical
activity can help people achieve and maintain good health and reduce the risk of chronic disease
throughout all stages of life.iii
To ensure a healthy lifestyle, the Office of Disease Prevention and Health Promotion's
2015-2020 Dietary Guidelines for Americans recommends that individuals eat several servings
of fruits, vegetables, and grains daily, and avoid foods high in saturated fat, sodium, processed
chemicals, trans fats, and added sugars. The Dietary Guidelines include recommendations to
maintain a healthy body weight and meet physical activity guidelines.ivEating patterns in the United States show that Americans are not following healthy eating
patterns. About three quarters of the population has an eating pattern that is low in vegetables,
fruits, dairy, and oils. Most Americans exceed the recommendations for added sugars, saturated
fats, and sodium, and the eating patterns of many are too high in calories.v
Furthermore, only 20 percent of adults meet the recommended physical activity
guidelines. Physical activity associated with work, home, and transportation has declined in
recent decades as a result of less active occupations; reduced physical activity for commuting to
work, school, or for errands; and increased sedentary behavior associated with television viewing
and other forms of screen time.vi
Members of low-income communities face additional challenges in adopting and
maintaining healthy behaviors, including limited resources and lack of access to healthy,
affordable foods, cycles of food deprivation and overeating, high levels of stress, anxiety and
depression, fewer opportunities for physical activity, greater exposure to marketing of obesity-
promoting products (such as sugary beverages and video games), and limited access to
healthcare.vii The financial and social impact of a hospitalization can add adds layers of
additional problems for single mothers. Low-income communities like the South Bronx are often
identified as food deserts, making access to food particularly challenging. A meal kit delivery
system providing free and low-cost meals would help to address the barrier of access to healthy
food for low-income single mothers.
The Community
The South Bronx is home to Community Districts 1 and 2 of Bronx County in New York
City, which includes the neighborhoods of Mott Haven, Melrose, Hunts Point, and Longwood.
This community has a population of 156,357. Of this population, 67 percent are Hispanic,
(predominantly Puerto Rican and Dominican), 28 percent are Black, and three percent are White.
Sixty-five percent of the population is between the ages of 18 and 64. The median household
income is $20,966, which is approximately one third of the nation-wide median household
income. Forty-four percent of persons are below the poverty line, and 59 percent of children
under the age of 18 are below the poverty line; the poverty rate is more than double the nation-
wide poverty rate. Only 59 percent of the population has a high school degree or higher, and 65.1
percent of the population speaks a language other than English at home.viii This community was
classified as having a Meal Gap (number of missing meals per capita) of more than 35 meals per
person in 2014 and had only between 1.0 and 1.7 supermarket square feet per person, which is
significantly less than the Department of City Planning’s optimal ratio of 3.0.ix
The South Bronx experiences some of the highest rates of family shelter entry and
number of single mothers with children under five years of age living in poverty in New York
City. There are between 12.2 and 19.1 per 1,000 families entering shelters annually and between
787 and 1,256 single mothers living with children under five years old earning below the federal
poverty level.x
Community health profiles published by the NYC Department of Health in 2015 indicate
that 68 percent of members of this community report their own health as “excellent,” “very
good,” or “good.” Among members of this community, 16 percent are current smokers, 38
percent drink one or more 12 once sugary drink per day, 77 percent have at least one serving of
fruits or vegetables per day, and 70 percent did some form of physical activity in the last 30 days.
Thirty-three percent of adults are obese, and 15 percent of adults have diabetes. The top three
leading causes of death in this community are heart disease, cancer, and diabetes mellitus.xi, xii Inthis community, an average of 68 percent of households receive benefits from the Supplemental
Nutrition Assistance Program (SNAP).xiii
Cook In’ is targeted at single mothers living in the South Bronx. Based on feedback from
a focus group we held, we chose to concentrate on the meal kit system as opposed to the ready-
made meals that companies like the Food Is Medicine Coalition provide. This focus group
consisted of 11 women between the ages of 29 and 43 years old that are identified as being
overweight or obese and live below the poverty line in our community. Many of the women
brought their children to the focus group.
These women are the primary providers for themselves and their children. Based on the
results of a survey completed by the participants of the focus group, the overwhelming majority
shop at grocery stores and prefer to cook as opposed to having someone else prepare their meals
for them. The participants report eating fresh fruit and vegetables every week. These fresh fruit
and vegetables are accessible in the community, but are very expensive and expire quickly.
While some of the woman report access to farmer’s markets through government programs in the
neighborhood, they are limited to where they can use their SNAP benefits, deterring some from
buying produce this way.
The women report shopping weekly for their groceries and pending between $80 and
$120 per week to feed a family of four. It was unclear if this amount accounted for the use of
SNAP benefits. The focus group participants are educated on healthy foods since most of them
are in New York State’s W.I.C. program, which mandates that they are seen by a nutritionist at
least once per year. They report understanding how healthy eating can reduce chronic illness;
however, one third reported that their doctor has never talked to them about nutrition or ways to
prevent chronic disease.
The overall take-home message from this focus group was that a meal kit system would
be preferred to a ready-made meal delivery option. The ability to choose their own meals and
cook meals themselves at home were identified as necessary factors. This reflects the strong
cultural traditions and focus on cooking at home that many of the participants hold. In addition,
freshness and cleanliness of the ingredients was identified as high priority.
The Meal Kit Delivery Industry and Trends in Healthcare Benefits
In 2007, Kicki Theander launched the first meal kit company called “Middagsfrid” in
Sweden. Today, the industry boasts over 170 businesses worldwide with over 150 of those in the
U.S. The concept of the meal kit became popular mostly amongst older millennials in urban
areas because of the convenience of the product.xiv Customers are able to pick out meals and
have the pre-measured ingredients delivered right to their doors along with recipe cards with
step-by-step directions to prepare the meal. This saves the customer time and reduces food waste.
In a 2016 report, it was estimated that meal kits reduce food waste by 62 percent.xv In addition,
consumers are able to choose from a variety of meals, including those with vegetarian, gluten
free, and low-carb options.
Cost is one of the major downfalls of the industry. Many of these companies spend
heavily on acquiring and retaining new customers in addition to their overhead costs of labor,
packaging, and shipping. Additionally, meal kits are price-prohibitive for many people who are
not able to spend the average meal kit price of $8 to $12 per serving.
The meal kit delivery industry delivers convenience but has yet to offer a low-price
option that would allow meal kits to be more accessible to a broader customer market. The
leaders of the industry, United States-based “Blue Apron” and Berlin-based “HelloFresh,” havebeen unable to turn a profit because of their high costs. As of February 2017, HelloFresh holds
approximately 33% of the market share in this $5 billion industry.xvi While the industry shows
sales growth, there is much room for innovations to broaden the customer base.
As of 2018, approximately 9 percent of Americans (10.5 million households) reported
that they had purchased a meal kit in the previous six months.xvii Another 25 percent of
consumers (30.1 million households) report that they would consider trying one.xviii This leaves a
huge opportunity for companies to gain market share if they can come up with a more innovative
way to attract and retain customers. Total spending on meal kits in the United States is expected
to increase to $11.6 billion by 2022 according to the research firm eMarketer.xix
Supermarkets and global companies have started to form alliances with meal kit
companies or provide meal kit options of their own. Albertsons, a large American supermarket
chain, recently bought the meal kit company “Plated” and plans to offer their kits in its grocery
stores. These stores have the advantage of existing supply chains, which help to minimize costs
of the ingredients.xx Peapod, an Internet grocer, supports many causes in the communities it
serves including Meals On Wheels and local food banks.xxi FreshDirect partners with (RED),
which supports people living with AIDS and regularly donates meals to various charities.xxii
These companies understand the importance of healthy eating and support those who have
limited ability to make healthy meals on their own.
Insurance companies have also started to offer recipients benefits for healthy eating.
These companies have seen that healthy eating can reduce obesity and chronic diseases such as
Diabetes Mellitus Type 2, Hypertension and Hyperlipidemia. By offering the insured an
incentive to eat healthier, companies have seen a reduction in their overall spending on
emergency room visits and inpatient hospitalizations related to chronic disease.xxiii
John Hancock life insurance offers its clients incentives and discounts when customers
“buy lots of fruits, vegetables and other healthy foods at the grocery store” using a loyalty card.
Through this program, customers can receive savings up to $50 per month or $600 a year. The
company reports that healthier clients reduce their overall spending in the long run.
Several health insurance companies, such as United Healthcare, Anthem Blue Cross, and
several state-run Medicaid programs, have implemented healthy eating incentives for their
recipients. Medicare Part C offers meal delivery at the discretion of the plan and Medicare
Advantage recipients may start to see incentives to healthy eating as a benefit as this was
recently approved by the federal government.xxiv
Since 2015, Health Partners Plan, a non-profit that runs Medicaid programs, has
partnered with a group of insurers around the country to offer prepared meals designed for
patients with chronic diseases such as diabetes, heart disease and kidney failure. The meals cost
approximately $5 per meal and Health Partners Plan covers 100% of the costs for the clients.
These meals are delivered to the plan’s recipients through a partnership with the Philadelphia
based nonprofit called MANNA (The Metropolitan Area Neighborhood Nutrition Alliance).xxv
The nonprofit organization Food Is Medicine Coalition provides medically-tailored
healthy meals to adults with serious illness and chronic disease. Currently, 18 states and the
District of Columbia are part of this organization. Aetna has added this benefit to its Medicaid
enrollees and California’s Medi-Cal Medicaid program started a 3-year pilot project in May 2018
costing $6 million to deliver meals to thousands of adults with chronic disease. Medi-Cal hopes
that if their pilot shows positive health benefits that the federal government will see the benefit of
making their idea a nationwide Medicaid benefit.xxvi The coalition’s “medically-tailored
nutrition” initiative has shown successful outcomes for those on their meal plans after sixmonths. These outcomes include a 16 percent net reduction in healthcare cost savings, 50 percent
reduction in hospitalizations, 50 percent adherence to the meal plans, and 23 percent increase in
discharges to home from the hospital for those admitted.xxvii
The Implementation
Cook In’s mission is to deliver meal kits filled with nutrient-dense ingredients and
healthy recipes to members of low-income communities at affordable prices. We aspire to reduce
the healthcare costs associated with chronic conditions by inspiring members of low-income
communities to adopt healthier lifestyles.
We will complete a one-year pilot study through grant funding from the Centers for
Medicare and Medicaid. Our target sample size is 200 female participants, taking into
consideration potential for drop-out. Participants will be recruited from local healthcare clinics
and a community hospital in the South Bronx. Inclusion criteria will be single mothers living in
the community who are identified as being overweight, obese, and/or diabetic. We will not
exclude based on age, race or other factors at this time. Once a client is identified, the healthcare
provider will meet with the patient and explain our pilot study. The client will receive our meal
kit recipe options based on their chronic disease and complete an online or phoned in order with
us. The client will have the option of either three or five dinners per week for themselves with
options to add on meals for their children at a small price of $2.50 per serving. We will deliver
all kits one time per week for each client, staggering delivery days based on order quantity.
The meals will be developed by a nutrition consultant on staff with knowledge of our
chosen chronic disease. We will partner with a company such as Peapod or FreshDirect to
purchase our ingredients and packing supplies in bulk at low cost while providing a philanthropic
opportunity for our partner. As an alternative, we will buy through a local wholesale food
market, fish market and meat market in the South Bronx that distributes to many of the local
restaurants in the area.
We will use a shared commercial kitchen space to pre-measure and package our meal
kits. We have identified a shelter system in our community that is interested in sharing their
commercial kitchen space with us at no cost. If we are unable to use their kitchen space, or if
additional kitchen space is needed, we will rent space at a local commercial kitchen facility to
supplement. The shared space allows us to reduce our costs and have a central location to help
keep our ingredients fresh and stored at the correct temperature.
Each recipe will be made up of 10 ingredients or less, 500 calories or less per serving,
and have a prep-to-table time of no more than 20 minutes. The meal kits will be delivered in a
box containing all necessary pre-measured ingredients along with a printed recipe card with step
by step instructions for preparing and cooking the meal. Recipe cards will have the nutritional
facts of each meal and will be available in English and Spanish. Ingredients used will be easy to
find in local groceries at low price so that customers can replicate the meals on days they do not
have meal kits.
Six months into the pilot program, participants will have a follow-up appointment with
their referring healthcare provider in order to check on progress, compliance, and improvement
in weight, A1C levels, blood pressure, and cholesterol levels. Additionally, at the six-month
mark, we will begin monetizing our product, offering our meal kits to additional single mothers
and their families within the community at a price of $2.50 per serving.
At the end of the pilot year, we will analyze our data to send to the insurance company
funding our program. We are confident this will lead to continued funding with an ultimate goalfor this to become a benefit for clients with Medicaid. In order for clients to receive and maintain
this benefit, they will have to consistently see their healthcare provider for an annual checkup.
This will incentivize patients to use their insurance, reducing the number of unnecessary
emergency department visits.
Our staff will include full time employees from the local community who are responsible
for preparing, packaging, and delivering all kits. We will also have a director, a development
coordinator, and a Board of Directors whose members will have a minimum annual fundraising
requirement. One member of the Board of Director will be a lawyer providing pro bono legal
counsel. By hiring employees from the local community and partnering with local kitchen
facilities Cook In’ will support the community and improve the lifestyles of many residents.
The Scaling Plan
Cook In’ will scale in three phases: expand reach in target community, expand offerings,
and expand geographically. As previously mentioned, six months into Cook In’s initial pilot
year, we will begin monetizing our product with additional single mothers in our community. We
will use the data collected during the pilot year to create additional partnerships with local clinics
and health care facilities within the South Bronx while simultaneously pursuing additional
funding opportunities from grants, largely from local Managed Medicaid insurance providers, as
well as individual and major giving campaigns. Grant funding will be used to offset operating
costs and allow us to offer free meals to those mothers and families that cannot afford our meal
kits otherwise.
As our customer base grows, we will have greater buying power and ability to purchase a
wider variety of ingredients at discounted prices. As a result, we will expand our menu of
recipes, as well as offer lunch options and flexibility in the number of meals ordered per week.
Upon building our brand and reputation in the South Bronx, we will begin to expand our
reach to clinics and healthcare facilities within New York City and in other metropolitan areas
with similar demographics. We will identify neighborhoods to serve as hubs where we will
locate shared or rented commercial kitchen space so that meal kit preparation continues to take
place within the communities we serve. Additionally, we will pursue corporate sponsorships
from local, regional, and national food distributors and lifestyle companies to further our pursuit
of our mission and vision.
The Competitive Analysis
Cook In’ combines the concept of the “medically-tailored nutrition” programs with the
meal kit delivery system to offer free and low-cost meal kits filled with nourishing ingredients
and healthy recipes to our underserved community, which does not otherwise have the luxury of
this option.
We will have a competitive advantage in the marketplace with our low-price, quality
product that is culturally sensitive to the community’s food preferences and tailored to their
chronic health conditions. Family-style meal options will open the doors to additional sources of
funding, allowing us to reach a broader audience that includes children, many of which are
insured through Children’s Health Insurance Program (CHIP). Additionally, we will be a vendor
that accepts SNAP benefits, allowing our customers to use these benefits to pay for their Cook
In’ meal kits. Currently, no companies offer a meal kit solution that is subsidized by insurance
for single mothers and their children. Subsidized meal programs are only offered as pre-prepared
meals, which does not meet the preference of our target demographic. We will combat the mealkit industry’s issues of customer acquisition and retention previously mentioned by partnering
with healthcare practitioners for referrals to our service and by continuously listening to the
needs of our customers.
As we enter the market, our supplier will have power until we have proven ourselves in
the industry. We will use the buying power of our grocery partner in order to keep our costs low.
As our company matures, we will contact food distributors for donations to further reduce costs.
The meal kit industry is currently crowded with a high threat to new entry despite
difficulty in turning a profit within the industry. By implementing an insurance-paid benefit
model, we will stand out in this crowd. There are many substitutes for healthy options, but they
are price prohibitive for our target demographic. Other alternatives are cheap, but at the cost of
nutritional value. For example, you can buy a McDonald’s “value meal” (single hamburger,
small fries, small Coca-Cola) starting at $3 with a caloric intake of 630 calories (170 calories
from fat and 48 grams of sugar).
Inherent to any business and new business models are certain risks. Competitive risk is a
concern if a cheaper cost structure or better product is developed. If this were to happen, Cook
In’ would face challenges maintaining current customers and gaining new referrals. Strategic risk
would emerge if Cook In’ fails to reach its targeted vision of improving the management of
chronic disease and promoting healthier lifestyles among low-income communities. This would
lead to financial risk as well, as funders could lose confidence in the prospect of future growth
and sustainability. Data collection and data analysis is an important element of the Cook In’
business model that will serve to assess risk and lead to proactive decision making to mitigate
risk that materializes. Economic risk may be a potential concern if the general prices of food
products and other materials rise. As the business model shifts to monetization and data
outcomes help us to secure additional funding, financial risk will be reduced.
The Revenue Model
Startup costs for this business are low at approximately $25,600. The first year of
business will be run as a pilot study of 200 single mothers and their families in our community.
Single mothers will be identified to participate by healthcare providers at our partnering clinics,
and their healthcare outcomes will be documented throughout the year. Participant women will
receive free meals kits for three or five meals per week with the option of paying $2.50 per
serving to feed their family.
Six months into the pilot year, we will begin monetizing our product by offering our meal
kits to additional single mothers and their families within the community at a price of $2.50 per
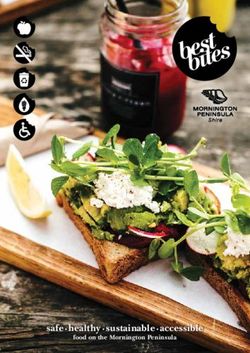
serving. Total operating costs for the first year, assuming 200 pilot participants with an average
of two children each for the duration of the year and 100 additional customer families is
approximately $750,100 with expected cash inflows of $840,400 from a combination of grant
funding, individual giving, and sales.
Entering the second year, we will be poised to receive additional grant funding as a result
of the healthcare outcome data collected from pilot participants. We will continue to offer meals
at $2.50 per serving to single mothers and their families in our community. Grant funding will be
used to offset operating costs and allow us to offer free meals to those mothers and families that
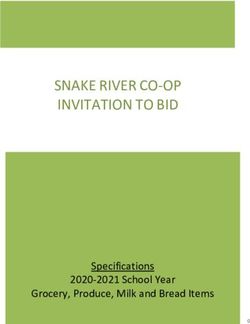
cannot afford our meal kits otherwise. (See Exhibit A)Exhibit A
Financial Assumptions
Inflows from Operations
o Grant Funding: One-year grant from government and private insurance companies
o Individual/Major Giving: From Board of Directors and fundraising campaigns
o Sales: Income from sale of the family option add-on to meal kits and from sale of
meal kits to those within the target community that can afford to pay at $2.50 per
serving. Income will come from a combination of SNAP benefits and cash.
Outflows from Operations
o Employees: Director ($100K/year), Development Coordinators ($50K/year), Food
Prep & Delivery Associates ($32K/year)
o Cost of Goods Sold: $1.96 per meal based on the assumption that the ingredients
selected will cost 75% of those that Blue Apron uses. Blue Apron’s 2017 gross
margin was 29%, with COGS approximately $2.60 per serving.
o Rent: Use of shared commercial kitchen and food storage space
o Telephone & Utilities: Cell phones for all employees
o Advertising: Targeted Facebook advertisements
o Office Supplies: Pens, paper, general office supplies, printing costs
o Vehicle: Insurance ($1,238/month), gas ($2,239/month), parking ($400/month)
o Menu Development: Development of recipes and periodic review of menu by
freelance nutritionist (40 hours every 6 months at $40/hour)
Outflows from Non-Recurring Expenses
o Vehicle: Purchase of a delivery van
o Website Development: Freelance web designer to set up website (100 hours at
$50/hour)
o Licensing: Food processing establishment licenseStatement of Cash Flow – Year 1
Projection of Income & Expense – Year One Projection of Income & Expense – Year Two
Bibliography
i
Irving, Doug. “Chronic Conditions in America: Price and Prevalence.” Rand Review. 12 Jul
2017. https://www.rand.org/blog/rand-review/2017/07/chronic-conditions-in-america-price-and-
prevalence.html. Accessed 19 Jan 2019.
ii
“The Healthcare Costs of Obesity.” The State of Obesity. https://stateofobesity.org/healthcare-
costs-obesity/. Accessed 19 Jan 2019.
iii
“Dietary Guidelines for Americans 2015-2020: Nutrition and Health are Closely Related.”
Office of Disease Prevention and Health Promotion.
https://health.gov/dietaryguidelines/2015/guidelines/introduction/nutrition-and-health-are-
closely-related/. Accessed 20 Jan 2019.
iv
“Dietary Guidelines for Americans 2015-2020: Executive Summary.” Office of Disease
Prevention and Health Promotion.
https://health.gov/dietaryguidelines/2015/guidelines/executive-summary/. Accessed 20 Jan 2019.
v
“Dietary Guidelines for Americans 2015-2020: Current Eating Patterns in the United States.”
Office of Disease Prevention and Health Promotion.
https://health.gov/dietaryguidelines/2015/guidelines/chapter-2/current-eating-patterns-in-the-
united-states/. Accessed 19 Jan 2019.
vi
“Dietary Guidelines for Americans 2015-2020: Current Eating Patterns in the United States.”
Office of Disease Prevention and Health Promotion.
https://health.gov/dietaryguidelines/2015/guidelines/chapter-2/current-eating-patterns-in-the-
united-states/. Accessed 19 Jan 2019.
vii
“Why Low-Income and Food Insecure People are Vulnerable to Poor Nutrition and Obesity.”
Food Research and Action Center. http://frac.org/obesity-health/low-income-food-insecure-
people-vulnerable-poor-nutrition-obesity. Accessed 20 Jan 2019.
viii
“American Community Survey 1-year estimates” U.S. Census Bureau. 2017.
https://censusreporter.org/profiles/79500US3603710-nyc-bronx-community-district-1-2-hunts-
point-longwood-melrose-puma-ny/. 7 Jan 2019.
ix
”Food Metrics Report 2016.” NYC Food Policy.
https://www1.nyc.gov/assets/foodpolicy/downloads/pdf/2016-Food-Metrics-Report.pdf.
Accessed 7 Jan 2019.
x
“On the Map: The Dynamics of Family Homelessness in New York City.” ICPHusa. 2016.
www.icphusa.org/wp-content/uploads/2016/04/Single-Mothers.pdf. Accessed 26 Jan 2019.
xi
King L, Hinterland K, Dragan KL, Driver CR, Harris TG, Gwynn RC, Linos N, Barbot O,
Bassett MT. “Community Health Profiles 2015, Bronx Community District 1: Mott Haven and
Melrose.” NYC Health. https://www1.nyc.gov/assets/doh/downloads/pdf/data/2015chp-bx1.pdf.
Accessed 7 Jan 2019.
xii
King L, Hinterland K, Dragan KL, Driver CR, Harris TG, Gwynn RC, Linos N, Barbot O,
Bassett MT. “Community Health Profiles 2015, Bronx Community District 2: Hunts Point and
Longwood.” NYC Health. https://www1.nyc.gov/assets/doh/downloads/pdf/data/2015chp-
bx2.pdf. Accessed 7 Jan 2019.
xiii
“SNAP (Food Stamps), Recipient: Individuals; Community District; Percent; 2016” Citizens’
Committee for Children of New York. https://data.cccnewyork.org/data/map/142/snap-food-
stamps#142/89/3/227/22/202. Retrieved 7 Jan 2019.
xiv
“Meal Kit Industry Statistics, Facts & History.” Review Chatter. 31 Jul 2018.
https://www.reviewchatter.com/statistics-facts-history/meal-kits. Accessed 11 Jan 2019.xv
Levy, Adam. “Should You Invest in Meal Kits?” The Motley Fool. 7 Jul 2018.
https://www.fool.com/investing/2018/07/07/should-you-invest-in-meal-kits.aspx. Accessed 7 Jan
2019.
xvi
Molla, Rani. “HelloFresh is now bigger than Blue Apron in the U.S.” Recode. 26 Mar 2018.
https://www.recode.net/2018/3/26/17165030/hellofresh-blue-apron-meal-kit-delivery-
marketshare-acquisition-organic-green-chef. Accessed 7 Jan 2019.
xvii
Garcia, Tonya. “People like meal kits, but their business model is unsustainable.”
MarketWatch. 6 Aug 2018. https://www.marketwatch.com/story/meal-kit-sector-is-facing-a-
shake-out-as-its-business-model-is-not-sustainable-2018-07-31. Accessed 7 Jan 2019.
xviii
Britt, Russ. “Will Investors Eat Up The Fresh New Industry of Meal Kits?” Investor’s
Business Daily. 25 June 2018. https://www.investors.com/news/meal-kits-meal-delivery-service-
review/. Accessed 7 Jan 2019.
xix
Levy, Adam. “Should You Invest in Meal Kits?” The Motley Fool. 7 Jul 2018.
https://www.fool.com/investing/2018/07/07/should-you-invest-in-meal-kits.aspx. Accessed 7 Jan
2019.
xx
“Upstart meal-kit companies may need a new recipe for growth.” The Economist. 14 Apr
2018. https://www.economist.com/business/2018/04/14/upstart-meal-kit-companies-may-need-a-
new-recipe-for-growth. Accessed 7 Jan 2019.
xxi
“Peapod in the Community.” Peapod. https://about.peapod.com/peapod-in-the-community/.
Accessed 27 Jan 2019.
xxii
Brecker, Anabelle. “Freshdirect Partners With (RED).” Sourced by FreshDirect for you. 29
May 2019. https://blog.freshdirect.com/freshdirect-partners-red/. Accessed 27 Jan 2019.
xxiii
Tobin, Tommy. “Health Insurance Coverage for Healthy Groceries? More Food-Based
Interventions May Be Coming.” Forbes. 24 May 2018.
https://www.forbes.com/sites/tommytobin/2018/05/24/health-insurance/#70208f3b459b.
Accessed 7 Jan 2019.
xxiv
Jaffe, Susan. “Medicare Advantage Plans Cleared To Go Beyond Medical Coverage – Even
Groceries.” Kaiser Health News. 3 Apr 2019. https://khn.org/news/medicare-advantage-plans-
cleared-to-go-beyond-medical-coverage-even-groceries/. Accessed 11 Jan 2019.
xxv
Kaiser Health News. “Using Nutrition as Medicine.” U.S. News. 25 Jun 2019.
https://www.usnews.com/news/healthiest-communities/articles/2018-06-25/medicaid-plan-in-
pennsylvania-offers-tailored-meals-to-combat-illnesses. Accessed 11 Jan 2019.
xxvi
Almendrala, Anna. “California Becomes The First State to Prescribe Food As Medicine.”
Huffington Post. 8 May 2018. https://www.huffingtonpost.com/entry/california-food-program-
medicaid_us_5af1ffb7e4b0ab5c3d6adae4. Accessed 7 Jan 2019.
xxvii
“Policy Priorities.” Food is Medicine Coalition.
https://static1.squarespace.com/static/580a7cb9e3df2806e84bb687/t/5bc0c310b208fc8737aa058
2/1539359504367/2-Fall+2018+FIMC+Talking+Points+one-pager.pdf. Accessed 7 Jan 2019.You can also read