COMMUNITY HEALTH NEEDS ASSESSMENT - University of Utah Health Hospitals and Clinics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

University of Utah Health Hospitals and Clinics
COMMUNITY HEALTH
NEEDS ASSESSMENT
Table of Contents
1 E X E C U T I V E N OT E S
Letter from CEO Gordon Crabtree
3
4
5
Life Expectancy at Birth
Population Count and Race/Ethnicity Table by County, Utah and US 6
2 A B O U T U N I V E R S I T Y O F U TA H H E A LT H
Mission, Vision, Values
7
8
3 COMMUNITY NEED AND COMMUNITY BENEFIT
Multiple approaches to address health and wellbeing
9
10
4 2021 CHNA ASSESSMENT BACKGROUND
Process planning, governance and collaboration
11
12
13
Community Input
Health Indicators 14
Priority Selection 15
Defining Hospital Community 16
5 I M P L E M E N TAT I O N G O A L S
Goal 1 Diabetes and Obesity
17
18
23
Goal 2 Mental Health and Suicide
Goal 3 Reducing Prescription Drug Misuse, Abuse, and Overdose 26
Goal 4 Racism and Inequality 29
Statewide Reach 34
6 S U M M A RY
Letter from RyLee Curtis and Steve Eliason
35
36
2
EXECUTIVE NOTES

FROM THE CEO
What makes up
a community?
Is it the homes that make up neighborhoods, and the families
that reside within them? Or the schools, non-profits, businesses,
and places of worship that help build culture? Is it the diversity
of the people?
I believe a community is made up of the bonds that tie all of these together.
Never has it been more apparent what makes up a community than
during the COVID-19 pandemic. We have seen communities come together
not only to distribute masks to families in need, but to sew 5 million masks for
their neighbors, and for health care workers. We’ve seen community
leaders translate complicated health messages into several languages.
Religious leaders encouraging their congregants to follow
recommended health guidelines to keep their members safe.
As CEO of University of Utah Health Hospitals and Clinics, I am moved by the
outpouring of our community’s gratitude for our frontline health
care workers. At the end of the day, each and every one of our 12,000+
employees does what they do for the health and well-being of our
community. They do this for you.
In the pages that follow, you will read about our strategies to address
pressing community needs. Some strategies will improve internal
processes to best serve community members who may become our
patients. Others will highlight areas where we can work with community
outside the hospital’s four walls and provide outreach, education, and the
expertise of our care teams.
Thank you,
Gordon Crabtree, CPA, MBA
Chief Executive Officer
University of Utah Health, Hospitals and Clinics
4 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
T H E D ATA
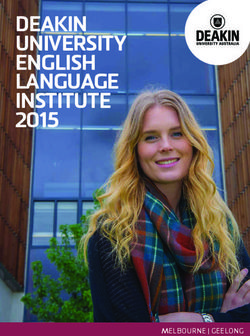
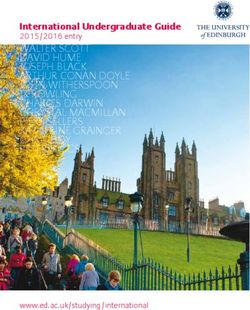
LIFE EXPECTANCY AT BIRTH BY LOCAL HEALTH DISTRICT,
2014-2018 AND U.S. 2017
Local Health Life Small Area Lowest Life Small Area Highest Difference
District Expectancy Expectancy Life Expectancy Based on
at Birth Zip Code
(years)
Davis 80.5 Clearfield/Hooper Kaysville/Fruit Heights & 5.3 years
County LHD at 77 North Salt Lake at 82.3
Salt Lake 79.5 South Salt Lake Salt Lake City (Avenues) 12.1 years
County LHD at 73.7 at 85.8
Tooele 78.2 Tooele Valley Tooele County (Other) 0.7 years
County LHD at 78.1 at 78.8
Utah 80.4 Orem (North) Provo/BYU 6 years
County LHD at 77.1 at 83.1
Weber- 78.2 Ogden (Downtown) Weber County (East) 6.6 years
Morgan LHD at 75 at 81.6
UTAH 79.8
Nation 78.6
Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Life Expectancy at Birth
78.2
80.5
78.2 WEBER
AN
RG
DAVIS MO
SALT
79.5
TOOELE LAKE
78.2 80.4
UTAH
80.5
78.2 WEBER
AN
RG
DAVIS MO
SALT 79.5
TOOELE
LAKE
80.4
UTAH
Source: Public Health Indicator Based Information System (IBIS) Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Life Expectancy at Birth Complete Health Indicator Report of Life Expectancy at Birth
5 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
T H E D ATA
AREA DEMOGRAPHICS
County Population Count
Davis County 355,481
Salt Lake County 1,160,437
Tooele County 72,259
Utah County 636,235
Weber County 260,213
UTAH 3,205,958
Nation 328,239,523
Source: U.S. Census Bureau
QuickFacts: 2019
RACE/ETHNICITY POPULATION AS PERCENT OF COUNTY
County White Black or American Asian Native Two or Hispanic White
Alone African Indian and Alone Hawaiian More or Latino alone, not
American Alaska and Other Races Hispanic
Alone Native Pacific or Latino
Alone Islander
Alone
Davis 92% 1% 1% 2% 1% 3% 10% 83%
County
Salt Lake 87% 2% 1% 5% 2% 3% 19% 70%
County
Tooele 94% 1% 1% 1% 1% 2% 13% 83%
County
Utah 93% 1% 1% 2% 1% 3% 12% 82%
County
Weber 92% 2% 1% 2% 0% 3% 19% 76%
County
UTAH 91% 2% 2% 3% 1% 3% 14% 78%
Nation 76% 13% 1% 6% 0% 3% 19% 60%
Source: U.S. Census Bureau
QuickFacts: 2019
6 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
ABOUT UNIVERSITY OF UTAH HEALTH

U N I V E R S I T Y O F U TA H H E A LT H
Our Mission University of Utah Health, which includes Academics as well as Hospitals
and Clinics, serves the people of Utah and beyond by continually
improving individual and community health and quality of life. This is
achieved through excellence in patient care, education, and research;
each is vital to our mission and each makes the others stronger.
• We provide compassionate care without compromise.
• We educate scientists and health care professionals for the future.
• We engage in research to advance knowledge and well-being.
Our Vision A patient-focused Health Sciences Center distinguished by
collaboration, excellence, leadership, and respect.
Our Values Compassion
Collaboration
Responsibility
Diversity
Quality
Trust
Innovation Integrity
U of U Health is the Mountain As part of that system, U of U Health Hospitals and Clinics is staffed by
West's only academic health care more than 5,000 practicing clinicians, including 1,700 physicians who
system, combining excellence in support five hospitals:
patient care, the latest in medical • University Hospital,
research, and teaching to • Huntsman Cancer Institute,
provide leading-edge medicine • Neilsen Rehabilitation Hospital,
in a caring and personal • University Orthopaedic Center, and
• Huntsman Mental Health Institute (HMHI) previously known as University
setting. The system provides
Neuropsychiatric Institute (UNI).
care for Utahns and residents
of five surrounding states in a
U of U Health Hospitals and Clinics also has 12 community clinics, nine
referral area encompassing
urgent care locations, and several specialty centers, which include:
more than 10 percent of the
• Cardiovascular Center,
continental United States.
• Clinical Neurosciences Center,
Whether it's for routine • John A. Moran Eye Center,
care or highly specialized • University Orthopaedic Center, and
treatment in orthopedics, • Utah Diabetes Center.
stroke, ophthalmology, cancer,
radiology, fertility, cardiology, U of U Health Hospitals and Clinics physicians also provide all the
genetic-related diseases, organ pediatric care at the Primary Children’s Hospital on campus, which is a
transplant, or more than 200 joint venture with Intermountain Healthcare.
other medical specialties, U
of U Health offers the latest Consistently ranked #1 in quality in the nation among academic medical
technology and advancements, centers, our academic partners at University of Utah Health include the
including some services available School of Medicine and Dentistry, and Colleges of Nursing, Pharmacy,
nowhere else in the region. and Health, which are internationally regarded research and teaching
institutions.
Our health care system is integrated with University of Utah
Health Plans which serves over 200,000 members through the
administration of medical, mental health, and pharmacy benefits
for self-funded employer groups as well as government programs
including Medicare and Medicaid.
8 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
& COMMUNITY NEED & COMMUNITY BENEFIT

THE COMMUNITY
Approaches University of Utah Health uses multiple
approaches to identify and address the
to identifying
health and wellbeing needs of our immediate
and regional communities.
and addressing • U of U Health supports patients in need through the
direct provision of charity care and through debt
the health
write-offs for those unable to complete payment due
to hardship.
and wellbeing
• In the 2019 fiscal year, U of U Health provided over
$190.6 million in uncompensated care, which includes
hospitals and clinics and the School of Medicine.
needs of our • U of U Health provides direct service to residents with
special health needs and to those living in under-
community served communities through education efforts,
telemedicine and outreach clinics, free screenings,
and direct patient care through partnerships with
multiple community agencies.
The Patient Protection and Affordable Care Act
(ACA), signed into law in March 2010, requires
each nonprofit hospital to conduct a Community
Health Needs Assessment (CHNA) every three
years. After identifying and prioritizing unmet
needs, each hospital is required to develop a
three-year implementation strategy to address
one or more identified community health needs.
This report documents the process through
which U of U Health conducted the CHNA, the
key findings, the identified priorities, and the
implementation strategies; this document will
also be posted online, fulfilling the requirement to
make the CHNA results available to the public.
10 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment11
T H E B A C KG R O U N D
Process planning,
governance and
collaboration
The CHNA process was led by U of U Health • Summit County Health Department
Hospitals and Clinics leadership and staff, • Tooele County Health Department
and was done in partnership with the Utah
CHNA Collaboration. This collaboration has • TriCounty Health Department
representatives from: • Uintah Basin Healthcare
• University of Utah Health
• Bear River Health Department
• Utah County Health Department
• Beaver Valley and Milford Hospitals
• Utah Department of Health
• Blue Mountain Hospital
• Utah Health Information Network
• Central Utah Public Health Department
• Utah Hospital Association
• Comagine Health
• Wasatch County Health Department
• Davis Behavioral Health
• Weber Human Services
• Davis County Health Department
• Weber-Morgan Health Department
• Get Healthy Utah
• Intermountain Healthcare
• Kem C. Gardner Policy Institute By partnering with the Utah CHNA Collaboration,
we are better able to access community health
• MountainStar Healthcare
data; reduce duplication of efforts; share
• Salt Lake County Health Department
expertise and resources in order to accomplish
• San Juan Health Department required tasks; and increase our ability to effect
• Shriner’s Hospital for Children change by identifying areas of overlap and of
• Southeast Health Department opportunities to work together.
• Southwest Health Department
12 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E B A C KG R O U N D
Community Input
MEETINGS
The Utah CHNA Collaboration hosted 20 different community input meetings throughout 2018 and 2019,
where attendees were invited to share their perspectives on the health needs of their community. Topics
included chronic disease, air quality, mental health, and substance use.
Invitees included representatives from the following groups:
• Food pantries • Local government
• Groups representing underrepresented • Low-income, uninsured, and underserved
populations populations
• Health advocacy organizations • Mental health service providers
• Health care providers • Safety net clinics
• Human service agencies • School districts
• Law enforcement • State and local health departments
• Local businesses
ONLINE SURVEY
An online survey was sent to those who could not attend the community input meeting in person, which
encouraged more representative feedback. Not all the people who received the invitation or follow-up
survey responded to the request. Transcripts of each meeting and the survey results were reviewed to
identify themes.
Overarching themes included:
• Chronic diseases associated with unhealthy weight • Immunizations;
and behaviors;
• Affordable housing;
• Mental health and suicide; • Substance use; and
• Air quality; • Social determinants of health and health equity.
13 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E B A C KG R O U N D Health Indicators For our CHNA, we used the Utah CHNA Collaboration’s approved list of health indicators, which includes over 100 health indicators and accompanying data sets. After identifying common themes from all of the community input meetings, we narrowed down the health indicator list by identified themes to provide a profile for each of the five identified communities. HEALTH INDICATORS USED TO BUILD COMMUNITY HEALTH PROFILES INCLUDE: Demographics: • Population Count by County • Race/Ethnicity Population as Percent of County Reducing Obesity & Obesity-Related Chronic Conditions (Carryover from previous CHNA) • Percentage of Adolescents who were Obese by Local Health District; Grades 8, 10, 12 (2019) • Adult Obesity by Local Health District, Utah 2018 • Fruit Consumed Two or More Times per Day by Local Health District 2017 • Vegetables Consumed Three or More Times per Day by Local Health District 2015 and 2017 • Food Insecurity, Limited Access to Healthy Food • SNAP Data by Local Health District • Senior Meals Data by County • Diabetes as an Underlying Cause of Death by Local Health District (2015-2018) • Coronary Heart Disease Deaths by Local Health District 2017-2018 Improving Mental Health and Reducing Suicide (Carryover from previous CHNA) • Suicide by Local Health District • SHARPS Self-Reported Suicide Indicators and Self Harm Data; Grades 6, 8, 10, 12 (2019) • SHARPS Self-Reported Depression Data; Grades 6, 8, 10, 12 (2019) • Estimated Utah Adults with Serious Mental Illness 2018 • Seven or More Days of Poor Mental Health in the Past 30 Days 2018 Reducing Prescription Drug Misuse, Abuse and Overdose (Carryover from previous CHNA) • Naloxone Doses Distributed in Utah by Distribution Program 2016-2019 • Opioid Deaths by Drug Category 2013-2018 • Opioid-Related Emergency Department Visits per 10,000 Population 2016-2018 • Opioid Prescriptions Dispensed per 1,000 Population 2014-2018 • Drug Death By Local Health District 2016-2018 • Drug Deaths by Local Health District Involving Opioids 2019 Reducing Inequities Caused by Social, Economic, and Structural Determinants of Health (NEW) • Poverty Rate by Race/Ethnicity by County, 5 Year Average 2013-2017 • Education Attainment by County 2014-2018 • Insurance, Median Household Income, and Poverty Percentage by Local Health District • Unemployment Rate by County in 2019 • Number of Small Areas by Health Improvement Index Scores • Percent Racial/Ethnic Minorities in Small Areas with HII Score of “High” and “Very High” 14 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
T H E B A C KG R O U N D Priority Selection Priorities for U of U Health’s Hospitals and Clinics CHNA were determined after: • analyzing the aforementioned data; • reflecting on feedback from the Utah CHNA Collaboration; • reviewing qualitative themes from the community input meetings and surveys conducted in Salt Lake, Davis, Utah, Tooele, and Weber counties; • reviewing the availability of known and effective interventions; • determining which areas were un-addressed or under-addressed; • and by considering which objectives synergized with other U of U Health initiatives including U of U Health’s Strategy Refresh and U of U Health’s Value Roadmap. Three-year plans have been outlined and implementation teams identified for each of the priorities which include: • Addressing diabetes, and reducing obesity and obesity-related chronic conditions; • Improving mental health and reducing suicide; • Reducing prescription drug misuse, abuse, and overdose; and • Addressing racism to reduce inequities caused by social, economic, and structural determinants of health. Three of the four priorities are carried over from our previous CHNA. • These three issues (obesity and obesity-related chronic conditions, mental health and suicide, and prescription drug misuse and abuse) were still top concerns for our community members. • You can find the impact assessment of U of U Health Hospital and Clinics' strategies to address these areas over the last three years in the 2018-2020 Implementation Plan & Completion Report. • We will adjust our strategies based on the data in this report, and further deepen our work in these areas over the next three years. 15 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment
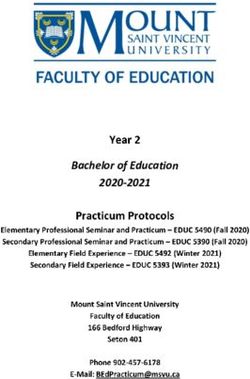
T H E B A C KG R O U N D
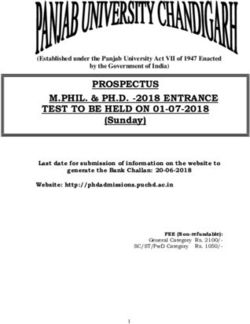
Defining the Hospital Community
U of U Health Hospitals and Clinics provides care for
Utahns and residents of five surrounding states in a CHNA TARGET COMMUNITIES
referral area encompassing more than 10 percent
Salt Lake County: With just over 1.1 million
of the continental United States. Due to our location
residents, Salt Lake County is Utah’s most
in the heart of Salt Lake City, and after a review of
populous and home to 36% of the state’s
the geographic origins of the hospital’s discharges
population. Its most populated cities are Salt
in fiscal years 2017-2019, we have chosen to focus
Lake City and West Valley City with populations
on five counties in Utah as our target communities
of 204,383 and 137,658, respectively. Salt
for the Community Health Needs Assessment—Salt
Lake City has a 32% Ethnic/Racial minority
Lake, Davis, Utah, Tooele, and Weber—which make
population and West Valley City has a 51%
up 78% of Utah’s total population.
Ethnic/Racial minority population. Salt Lake
City is home to the University of Utah.
Utah County: Utah County’s population of
636,235 makes it Utah’s second most populated
county, with 20% of the state’s residents. The most
populated cities in Utah County are Provo and
Orem, which are home to 123,027 and 98,040
residents, respectively. Provo has a 25.2% Ethnic/
Racial minority population and Orem has a 23.1%
Ethnic/Racial minority population. Provo is home
to Brigham Young University.
Davis County: At 355,481, the population of Davis
County makes up 11% of Utah’s population. Layton/
South Weber and Clearfield Area/Hooper are the
most populated cities in Davis County which are
Source: Tableau
home to 83,944 and 72,508 residents, respectively.
Layton/South Weber have a 20.1% Ethnic/Racial
minority population and Clearfield Area/Hooper
have a 22.0% Ethnic/Racial minority population.
County U of U Health Population Weber County: Weber County is home to
260,213 residents, making up 8% of the state’s
Salt Lake County 63% population. Ogden and Ben Lomand are the
most populated cities in Weber County which
Davis County 10%
are home to 77,669 and 62,407 residents,
Utah County 6% respectively. Ogden has a 29.1% Ethnic/Racial
Tooele County 5% minority population and Ben Lomand has a
28.9% Ethnic/Racial minority population. Weber
Weber County 4% County is home to Weber State University.
Source: Tableau
Tooele County: Tooele County’s population of
72,259 makes up 2% of Utah’s population. Tooele
has a 17.4% Ethnic/Racial minority population.
16 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentIMPLEMENTATION GOALS 17
I M P L E M E N TAT I O N G O A L
Addressing Below are specific strategies and initiatives
related to diabetes, obesity and obesity-related
chronic conditions which University of Utah
Diabetes and Hospitals and Clinics commits to as part of the
Community Health Needs Assessment process
Reducing Obesity and will work towards over the next three years.
and Obesity- STRATEGIES & INITIATIVES
Related Chronic Strengthen and support community-focused
programs for addressing obesity & diabetes
Conditions prevention
• Increase the number of encounters between
community members and The Wellness Bus by 5%
each year for the next 3 years
• Increase participation in both the Crush Diabetes
and the Team Thrive childhood diabetes prevention
programs by 5% each year for the next 3 years
• Increase the reach of evidence-based programs for
individuals with obesity in underserved populations
• Create an obesity & diabetes prevention, education,
and outreach taskforce to coordinate efforts to reach
out to and learn from underrepresented populations
Improve access to healthy food
• Research and create a food pharmacy that could be
piloted in a minimum of two U of U Health clinics
• Increase participation in the Food Movement and You
Addressing obesity and diabetes were elements program by 5% each year for the next 3 years
included in U of U Health’s Strategy Refresh.
We have committed as a system to continue to Increase screenings, referrals, and treatment
for obesity and diabetes programs
advocate for clear, science-supported policy
recommendations on public health needs related to • Increase the number of patients that can access care
through Utah Diabetes and Endocrinology center
obesity and diabetes. We will continue advancing
• Increase the number of patients who participate in
work to successfully manage obesity-related
the Intensive Diabetes Education And Support (IDEAS)
chronic conditions in longitudinal, value-based program
payment care programs. Leveraging our integrated • Increase the number of patients who participate in a
health system we will continue working alongside Comprehensive Weight Management Program
our partners and patients with chronic conditions
Encourage our 12,000+ Hospital & Clinic
to better coordinate their care and expand health employees to participate in employee health
coaching to more patients with chronic conditions. and wellness programs
• Implement a diabetes initiative to help our employees
and their families prevent and manage diabetes
• Encourage participation in programs available to
employees
University of Utah and University of Utah Health have come together as a community with renewed vision and the human
talent needed for our institutions to navigate an increasingly complex and dynamic landscape. This process allowed
our systems to refresh their strategies and address Utah’s growing and changing demographics, adapt to 21st-century
workforce needs, enhance lifelong education opportunities, and find new ways to leverage unique strengths of University
of Utah. The Strategy Refresh summarizes the great work ahead, starting now and continuing through 2025. The CHNA is
a complimentary document and allows for alignment between community needs and Strategy Refresh Priorities.
18 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
“So if you're a low income individual, you
cannot afford to eat healthy. [You] just can't.
Community Profile And [our] cooking skills, that is something
that we have lost in this community. I mean
we can have great produce and great
Area Diabetes, Obesity and Obesity-Related Chronic
healthy items in the pantry, and nobody
Conditions Information: knows what to do with it.”
– attendee at Ogden Community Input Meeting
OBESE ADOLESCENTS BY LOCAL ADULT OBESITY BY LOCAL HEALTH
HEALTH DISTRICT, GRADES 8, 10, DISTRICT, UTAH, 2018
AND 12, UTAH, 2019
Local Health District Percentage of
Local Health District Percentage of Adolescents
Adolescents
Davis County LHD 26.30%
Davis County LHD 8.50% Salt Lake County LHD 28.40%
Salt Lake County LHD 11.10% Tooele County LHD 43.00%
Tooele County LHD 12.20% Utah County LHD 28.50%
Utah County LHD 8.60% Weber-Morgan LHD 30.30%
Weber-Morgan LHD 12.10%
UTAH 28.40%
UTAH 9.80% Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Obesity Among Adults
Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Obesity Among
Children and Adolescents
FRUIT CONSUMED TWO OR MORE VEGETABLES CONSUMED THREE
TIMES PER DAY BY LOCAL HEALTH OR MORE TIMES PER DAY BY
DISTRICT, UTAH, 2017 LOCAL HEALTH DISTRICT, UTAH,
2018
Local Health District Age-Adjusted
Percentage of Local Health District Age-Adjusted
Adults 18+ Percentage of
Adults 18+
Davis County LHD 37.00%
Salt Lake County LHD 33.50% Davis County LHD 14%
Tooele County LHD 27.60% Salt Lake County LHD 15.30%
Utah County LHD 39.40% Tooele County LHD 11.80%
Weber-Morgan LHD 32.50% Utah County LHD 17.80%
Weber-Morgan LHD 15.50%
UTAH 34.70%
Source: Public Health Indicator Based Information System (IBIS)
UTAH 15.30%
Complete Health Indicator Report of Daily Fruit Consumption
Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Daily Vegetable Consumption
19 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
FOOD INSECURITY, LIMITED ACCESS TO HEALTHY FOOD BY COUNTY, 2017
County Percentage of Number of Percentage of Number of
Individuals Food Individuals Food Children Food Children Food
Insecure Insecure Insecure Insecure
Davis County 11% 36,310 14% 15,140
Salt Lake 12% 130,130 15% 45,360
County
Tooele County 11% 6,880 14% 3,040
Utah County 13% 73,640 14% 28,620
Weber County 12% 29,680 16% 11,260
UTAH 11% - - -
County Percentage of Percentage of Percentage of Number of
Households Households Individuals in Individuals in
reporting “yes” to reporting “yes” to County with County with
the statement: the statement: Limited Access Limited Access
“The food that I “I couldn't afford to to Grocery Store to Grocery Store
bought just didn't eat balanced meals, (Low-income & (Low-income &
last, and I don't often or sometimes”
have money to Low Access) Low Access)
get more, often or
sometimes”
Davis County 13% 18% 6% 18,820
Salt Lake 13% 16% 3% 28,999
County
Tooele County 17% 19% 10% 5,774
Utah County 14% 16% 7% 35,678
Weber County 15% 17% 6% 14,371
UTAH - - - -
Source: Utahns Fight Against Hunger
County Food Access Profiles
20 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
SNAP UTILIZATION BY COUNTY
County Number Number Percent Number of Number of Estimated
of SNAP of SNAP of County Average Low-income Number of
Households Individuals, Population Monthly Individuals Low-income
April 2019 Participating SNAP Enrolled in Individuals
in SNAP, Households, SNAP, 2017 NOT Enrolled
April 2019 SFY, 2018 in SNAP, 2017
Davis 5,699 14,107 4.12% 6,289 16,595 7,961
County
Salt Lake 31,090 68,556 6.11% 34,014 80,924 65,414
County
Tooele 1,824 4,384 6.76% 1,949 5,618 882
County
Utah 8,905 24,407 4.12% 9,780 29,317 53,272
County
Weber 8,972 19,163 7.74% 9,679 21,949 17,022
County
Source: Utahns Fight Against Hunger
County Food Access Profiles
SENIOR MEALS BY COUNTY, 2018
County Number of Congregate Congregate Meals on Meals on Senior Food Senior
Congregate Meals Meals Wheels Wheels Boxes Food Boxes
Meal Sites | People | Meals | People | Meals | Number of | Number
Served Served Served Served Participants of Pickup
Sites
Davis 3 1,256 28,243 684 83,406 55 3
County
Salt Lake 19 8,514 198,345 2,334 334,538 1,989 56
County
Tooele 4 813 16,546 230 26,203 64 1
County
Utah 15 12 2,899 1,218 122,294 132 6
County
Weber 13 12 2,316 951 138,984 476 9
County
Source: Utahns Fight Against Hunger
County Food Access Profiles
21 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
DIABETES AS AN UNDERLYING CORONARY HEART DISEASE
CAUSE OF DEATH BY LOCAL DEATHS BY LOCAL HEALTH
HEALTH DISTRICT, 2015-2018 DISTRICT, 2017-2018
Local Health District Age-Adjusted Local Health District Age-Adjusted
Rate per 100k Rate per 100k
Population Population
Davis County LHD 23% Davis County LHD 67.1%
Salt Lake County LHD 26% Salt Lake County LHD 62.5%
Tooele County LHD 30% Tooele County LHD 66.6%
Utah County LHD 22% Utah County LHD 63.5%
Weber-Morgan LHD 26% Weber-Morgan LHD 74.1%
UTAH 24% UTAH 64.8%
Source: Public Health Indicator Based Information System (IBIS) Source: Public Health Indicator Based Information System (IBIS)
Health Indicator Report of Deaths due to Diabetes as Underlying Cause Health Indicator Report of Coronary Heart Disease (CHD) Deaths
22 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentI M P L E M E N TAT I O N G O A L
Improving Mental Below are specific strategies and initiatives
related to improving mental health and reducing
suicide which University of Utah Hospitals and
Health and Clinics commits to as part of the Community
Health Needs Assessment process and will work
Reducing Suicide towards over the next three years.
STRATEGIES & INITIATIVES
Increase screenings, referrals, and treatment
coordination between mental health and
primary care providers:
• Implement Collaborative Care for patients with major
depressive disorders in order to improve health
outcomes, with a goal to see a 50% improvement in
PHQ-9/PROMIS depression scores
• Improve screenings for suicide risk and increase
access to effective behavioral health treatment by
implementing the Zero Suicide programming of the
Columbia Suicide Severity Screening (C-SSRS) in
Improving mental health and reducing suicide primary care settings
• Integrate substance abuse screening, brief
were elements included in U of U Health’s Strategy
intervention, and referral and treatment (SBIRT)
Refresh. Our vision is that access to and the quality practices into primary care settings
of mental health services in Utah are materially • Increasing access to and use of the SafeUT app and of
improved statewide, and the mental health of school-based mental health (with referral supports)
Utah’s population is better than it is today. Over • Improve transitions of care from inpatient Psychiatry to
the next few years we will be launching initiatives Primary Care and from Community Crisis Encounters
to Primary Care
for the Huntsman Mental Health Institute and
• Expand Call-Up, the Psychiatrist Consultation Program
we will continue to expand the reach of mental that provides primary care providers with access to
health services through programs like SafeUT, telehealth psychiatric consultations (peer-to-peer
statewide crisis call center, and Call-Up. consulting)
Improve access to mental health services:
In 2019, the Huntsman family announced a • Extend 24/7 mobile crisis outreach teams (MCOT)
historic gift of $150 million to establish the across the entire state – UNI provides dispatch
Huntsman Mental Health Institute with an initial services to all MCOT teams
• Enhance the statewide crisis call center to serve as
focus on advancing knowledge and relieving
the centralized hub for coordinating behavioral health
suffering through research-informed treatment
and crisis support services
of mental illness with a strong focus on improving • Create the Salt Lake County community-based
mental health services for college-age adults, behavioral health receiving center
increasing access to mental health services in
rural communities across Utah, and identifying
the genetic underpinnings of mental illness.
University of Utah and University of Utah Health have come together as a community with renewed vision and the human
talent needed for our institutions to navigate an increasingly complex and dynamic landscape. This process allowed
our systems to refresh their strategies and address Utah’s growing and changing demographics, adapt to 21st-century
workforce needs, enhance lifelong education opportunities, and find new ways to leverage unique strengths of University
of Utah. The Strategy Refresh summarizes the great work ahead, starting now and continuing through 2025. The CHNA is
a complimentary document and allows for alignment between community needs and Strategy Refresh Priorities.
23 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
SUICIDE RATES BY LOCAL HEALTH ESTIMATED UTAH ADULTS WITH
DISTRICT SERIOUS MENTAL ILLNESS, 2018
Local Health District Age-Adjusted Local Health District Percent of Number
Rate Per 100k Population with
Population UT with SMI SMI
2016-2018
Davis County LHD 4.6% 10,238
U.S. 2015-2017
Salt Lake County 4.8% 38,364
Davis County LHD 19.9
LHD
Salt Lake County LHD 22.1
Tooele County LHD 5.2% 2,164
Tooele County LHD 23.6
Utah County LHD 16.6 Utah County LHD 5.6% 21,221
Weber-Morgan LHD 28.9 Weber-Morgan 4.8% 8,698
LHD
UTAH 22.2
Source: FY 2018 Mental Health Scorecard for Audits. (2018, November)
Nation 13.6 Department of Substance Abuse and Mental Health
Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Suicide
ESTIMATED UTAH ADULTS WITH
SEVEN OR MORE DAYS OF POOR
MENTAL HEALTH IN THE PAST 30
DAYS, 2018
Local Health District Age-Adjusted
Percentage of
Adults
Davis County LHD 17%
Salt Lake County LHD 19%
Tooele County LHD 21%
Utah County LHD 18%
Weber-Morgan LHD 20%
UTAH 18%
Nation 19%
Source: Public Health Indicator Based Information System (IBIS)
Health Indicator Report of Health Status: Mental Health Past 30 Days
24 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
SELF REPORTED SUICIDE INDICATORS AND SELF HARM DATA;
GRADES 6, 8, 10, 12; 2019
County During the During the Past 12 During the Past 12 Purposeful Self Harm
Past 12 Months, Months, Did You Months, How (Without Suicidal
Did You Ever Make a Plan About Many Times Did Intention, e.g.
Seriously Consider How You Would You Actually Cutting or Burning)
Attempting Suicide Attempt Suicide? Attempt Suicide? (Answered 1 or
(Answered 'Yes') (Answered 'Yes') (Answered 1 or More Times During
More Times) the Past 12 Months)
Davis County 16% 11% 6% 15%
Salt Lake 18% 13% 8% 17%
County
Tooele 19% 16% 9% 19%
County
Utah County 15% 11% 5% 14%
Weber 17% 13% 8% 16%
County
UTAH 16% 12% 7% 15%
Source: Utah Dept. of Human Services, SHARP Survey
2019 SHARP Survey Reports
SELF REPORTED DEPRESSION DATA, GRADES 6, 8, 10, 12; 2019
County High Moderate No Felt Sad or Hopeless for
Depressive Depressive Depressive Two Weeks or More in a Row
Symptoms Symptoms Symptoms During the Past Year
Davis County 9% 58% 33% 26%
Salt Lake County 16% 13% 8% 17%
Tooele County 11% 61% 28% 29%
Utah County 8% 63% 29% 26%
Weber County 9% 62% 29% 30%
UTAH 9% 62% 29% 28%
Source: Utah Dept. of Human Services, SHARP Survey
2019 SHARP Survey Reports
25 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentI M P L E M E N TAT I O N G O A L
Reducing Below are specific strategies and initiatives
related to reducing prescription drug misuse,
abuse, and overdose which University of Utah
Prescription Hospitals and Clinics commits to as part of the
Community Health Needs Assessment process
Drug Misuse, and will work towards over the next three years.
Abuse, and STRATEGIES & INITIATIVES
Overdose Increase prevention efforts through education
and community outreach:
• Improve and increase patient education about proper
drug disposal
• Increase community outreach and access to pain
management education materials
• Increase community education regarding substance
use awareness
Measure prescribing practices within U of U
Health to identify and create best practices:
• Measure the current patterns of controlled substance
prescribing for patients with acute versus chronic
disease and develop best practices in a patient-
centered manner
• Measure Buprenorphine-specific prescribing rates
Reducing prescription drug misuse, abuse, and • Measure how U of U Health Hospitals and Clinics
clinicians co-prescribe controlled substances
overdose were elements included in U of U
alongside opioids
Health’s Strategy Refresh. We have committed as a
system to continue to advocate for clear, science- Expand access to treatment through trainings
supported policy recommendations on public and standardization of processes:
health needs related to opioids. And we will work • Expand Naloxone trainings throughout the community
with patients with chronic conditions to learn how to and within the U of U Health system
better coordinate care for them, and expand health • Expand Buprenorphine waiver trainings throughout
the community and within the U of U Health system
coaching to more patients with chronic conditions.
• Leverage our electronic medical record platform, EPIC,
to encourage best prescribing practices through the
use of care coordination and standardization
University of Utah and University of Utah Health have come together as a community with renewed vision and the human
talent needed for our institutions to navigate an increasingly complex and dynamic landscape. This process allowed
our systems to refresh their strategies and address Utah’s growing and changing demographics, adapt to 21st-century
workforce needs, enhance lifelong education opportunities, and find new ways to leverage unique strengths of University
of Utah. The Strategy Refresh summarizes the great work ahead, starting now and continuing through 2025. The CHNA is
a complimentary document and allows for alignment between community needs and Strategy Refresh Priorities.
26 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
“…what I'm seeing a lot of is the socioeconomic
disadvantages these families have, are
Community Profile creating all types of mental health issues from
food insecurities, improper early childhood
intervention, and it just moves up…socioeconomic
status is part of it can be part of the loneliness,
OPIOID DEATHS BY DRUG part of the drug abuse, part of those things. I
have families who are struggling because of the
CATEGORY socioeconomic disadvantages due to someone
who has an addiction in their family. Or the food
insecurities because of an addiction in their
family. So I just think it all ties so closely.”
– attendee at Ogden Community Input Meeting
NALOXONE DOSES DISTRIBUTED IN
UTAH BY DISTRIBUTION PROGRAM
Source: Utah Department of Health
Opioid Data Dashboard
NEWBORNS WITH NAS
Source: Utah Department of Health
Opioid Data Dashboard
Source: Utah Department of Health
Opioid Data Dashboard
27 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
OPIOID-RELATED EMERGENCY DRUG DEATHS BY LOCAL HEALTH
DEPARTMENT VISITS PER 10,000 DISTRICT, 2016-2018*
POPULATION
Local Health District Age-Adjusted
Rate Per 100k
Population
Davis County LHD 17
Salt Lake County LHD 23.3
Tooele County LHD 21.4
Utah County LHD 20.2
Weber-Morgan LHD 25.4
UTAH 21.9
*The Consensus Recommendations for National and State Poisoning Surveillance
definition of a drug is as follows: A drug is any chemical compound that is chiefly
used by or administered to humans or animals as an aid in the diagnosis, treatment,
or prevention of disease or injury, for the relief of pain or suffering, to control or
improve any physiologic or pathologic condition, or for the feeling it causes.
Source: Public Health Indicator Based Information System (IBIS)
Complete Health Indicator Report of Drug Overdose
Source: Utah Department of Health
and Poisoning Incidents
Opioid Data Dashboard
OPIOID PRESCRIPTIONS DRUG OVERDOSE DEATHS
DISPENSED PER 1,000 POPULATION INVOLVING OPIOIDS BY LOCAL
HEALTH DISTRICT, 2019
Local Health District Age-Adjusted
Rate Per 100k
Population
Davis County LHD 9.9
Salt Lake County LHD 20.3
Tooele County LHD 17.4
Utah County LHD 13.3
Weber-Morgan LHD 19.7
UTAH 16.7
Source: Utah Department of Health
Opioid Data Dashboard
Source: Utah Department of Health
Opioid Data Dashboard
28 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentI M P L E M E N TAT I O N G O A L
Below are specific strategies and initiatives
related to reducing inequities caused by social,
Addressing
economic, and structural determinants of health
which University of Utah Hospitals and Clinics
commits to as part of the Community Health
Racism to Reduce Needs Assessment process and will work towards
over the next three years.
Inequities STRATEGIES & INITIATIVES
Implement impact hiring programs:
• Develop and implement U of U Health diversity and
inclusion strategies, including recruitment, performance
management, staff development, engagement, and
retention
• Create and fill the position of Senior Director of HR for
Equity, Diversity, and Inclusion
Implement a system-based approach to
understanding our patients’ social determinants
of health (SDOH):
• Convene a U of U Health workgroup to develop system-
based approaches to screening and referrals for SDOH
• Actively participate in ongoing community-led
meetings about community and statewide initiatives to
We recognize racism as a public health crisis and address SDOH
believe anti-Black racism is one major cause of • Increase the capture rate of sexual orientation, gender
health disparities that we observe in our society. identity, pronouns, and chosen name fields
Addressing racism to reduce inequities caused
Encourage enrollment in health insurance
by social, economic, and structural determinants
programs:
of health were elements included in U of U
• Create community-based partnerships to assist
Health’s Strategy Refresh. Our vision is to actively
uninsured individuals with the health insurance
value equity, diversity, and inclusion and see application process
the reflection and impact of these values at all • Create outreach and education materials to encourage
levels of the organization—by recruiting and uninsured individuals to enroll in health care coverage
retaining diverse faculty, trainees, students, and to seek primary and preventive care services
and employees. We will ensure Utahns who seek
Help clinicians and staff provide culturally
care from U of U Health have easy and direct responsive care:
access to our services. And we will finalize an
• Improve access to foundational health resources in
integrated, comprehensive care plan for patients languages other than English
with elevated socioeconomic and clinical risks. • Create learning modules available to all staff
highlighting best practices in caring for LGBTQIA+
patients
• Improve access to the Intensive Outpatient Clinic for
qualifying patients
University of Utah and University of Utah Health have come together as a community with renewed vision and the human
talent needed for our institutions to navigate an increasingly complex and dynamic landscape. This process allowed
our systems to refresh their strategies and address Utah’s growing and changing demographics, adapt to 21st-century
workforce needs, enhance lifelong education opportunities, and find new ways to leverage unique strengths of University
of Utah. The Strategy Refresh summarizes the great work ahead, starting now and continuing through 2025. The CHNA is
a complimentary document and allows for alignment between community needs and Strategy Refresh Priorities.
29 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
Area Inequities Caused by Social, Economic, and Structural Determinants of Health
POVERTY RATE BY RACE/ETHNICITY BY COUNTY, 5 YEAR AVERAGE 2013-2017
County White Black or American Asian Native Some Two or Hispanic White
Alone African Indian alone Hawaiian other more or Latino alone,
American and and Other race races Origin not
Alone Alaska Pacific alone (of any Hispanic
Native Islander race) or Latino
alone alone
Davis 5.5% 23% n/a n/a n/a 12% 9% 17% 5%
County
Salt Lake 8% 29% 25% 14% 14% 23% 13% 20% 7%
County
Tooele 10% 27% 30% 15% 15% 23% 14% 20% 9%
County
Utah 11% 24% 19% 23% 13% 26% 15% 19% 10%
County
Weber 11% 15.5% 22% n/a n/a 22% 22% 23% 9%
County
Source: Utahns Fight Against Hunger
County Food Access Profiles
EDUCATION ATTAINMENT BY COUNTY (PERCENT
OF PERSONS AGE 25 YEARS+)
County High School Bachelor's Degree
Graduate
Davis County 96% 38%
Salt Lake County 90% 35%
Tooele County 91% 23%
Utah County 94% 40%
Weber County 90% 24%
UTAH 92% 33%
Nation 88% 32%
Source: U.S. Census Bureau
QuickFacts: 2019
30 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA
Community Profile
Area Inequities Caused by Social, Economic, and Structural Determinants of Health
UNEMPLOYMENT RATE BY KEY SOCIOECONOMIC FACTORS BY LOCAL
COUNTY, 2019 HEALTH DISTRICT
County Unemployment Local Health Persons Median Persons in
Rate District without health household poverty,
insurance, income in percent
Davis County 2.60% under age 65 2018 dollars
Salt Lake 2.73%
Davis 7% 79,690 6%
County
County LHD
Tooele County 3.05%
Salt Lake 12% 71,230 9%
Utah County 2.55% County LHD
Weber County 3.22% Tooele 10% 71,020 7%
County LHD
UTAH 2.90%
Utah 9% 70,408 9%
Source: Utahns Against Hunger
County Food Access Profiles
County LHD
Weber- 10% 64,636 9%
Morgan
LHD
UTAH 11% 68,374 9%
Nation 10% 60,293 11%
Source: Public Health Indicator Based Information System (IBIS)
IBIS-PH Indicator Reports Introduction
31 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentT H E D ATA Community Profile The Utah Department of Health recently created a composite measure of social determinants of health by geographic area called the Health Improvement Index (HII). The ten indicators included in the HII describe important determinants of health information: 1. Population aged ≥25 years 5. Owner-occupied housing 8. Population below 150% of the with
T H E D ATA Community Profile The HII report allows us to quickly identify areas where addressing social determinants of health through a health equity lens can move the needle on health disparities and ultimately adverse health outcomes. The HII report underscores the need to implement interventions with a focus on health equity, as this will be more effective because the areas with “High” and “Very High” HII scores tend to have a higher percentage of racial/ethnic minorities. How to use this classification: Very High HII >120; geographically, this is a very high health disparities area; SUBSTANTIAL IMPROVEMENTS are needed to advance health equity and reduce health disparities in the area. High HII >105 and 94 and 80 and
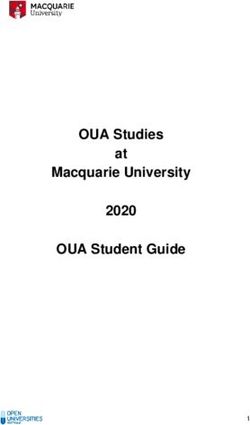
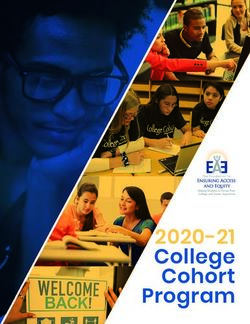
CLINICAL REACH
S T R AT E GY
Statewide Reach
Since University of Utah Hospital opened its doors
in Salt Lake City, Utah, in 1965, U of U Health has
grown from a single county hospital to an exemplary
regional health care system that includes five
hospitals, 12 community health centers, several
specialty centers, and an extensive network of affiliate
partners throughout the Mountain West region.
Additionally, 81 telehealth sites offer on-demand
access for both referring providers and patients.
A number of the strategies and tactics U of U Health
Hospitals and Clinics will take to address our four CLINICAL REACH
main Community Health Needs Assessment goals will ● Affiliate Partners ◆ Outreach Clinics ● Telehealth Sites
not only benefit our five target communities, but could
also have a statewide and even regional impact. Source: FY19 System Summary
IMPLEMENTATION GOAL: ADDRESSING DIABETES IMPLEMENTATION GOAL: REDUCING
AND REDUCING OBESITY AND OBESITY-RELATED PRESCRIPTION DRUG MISUSE, ABUSE, AND
CHRONIC CONDITIONS OVERDOSE
Strengthen and support community-focused Increase prevention efforts through education
programs for addressing obesity & diabetes and community outreach:
prevention • Increase community outreach and access to pain
• Increase participation in both the Crush Diabetes management education materials.
and the Team Thrive childhood diabetes prevention • Increase community education regarding substance
programs by 5% each year for the next 3 years. use awareness.
• Increase the reach of evidence-based programs for Expand access to treatment through trainings
individuals with obesity in underserved populations.
and standardization of processes:
• Create an obesity & diabetes prevention, education,
and outreach taskforce to coordinate efforts to reach • Expand naloxone trainings throughout the community
out to, and learn from, underrepresented populations. and within the U of U Health system.
• Expand Buprenorphine waiver trainings throughout
the community and within the U of U Health system.
IMPLEMENTATION GOAL: IMPROVING MENTAL
HEALTH AND REDUCING SUICIDE
Increase screenings, referrals, and treatment IMPLEMENTATION GOAL: ADDRESSING RACISM
coordination between mental health and TO REDUCE INEQUITIES
primary care providers: Implement a system-based approach
to understanding our patients’ social
• Increasing access to and use of the SafeUT app and of
determinants of health (SDOH):
school-based mental health (with referral supports).
• Expand Call-Up, the Psychiatrist Consultation Program • Actively participate in ongoing community-led
that provides primary care providers with access to meetings about community and statewide initiatives to
telehealth psychiatric consultations (peer-to-peer address SDOH.
consulting). Encourage enrollment in health insurance
Improve access to mental health services: programs:
• Extend 24/7 mobile crisis outreach teams (MCOT) • Create community-based partnerships to assist
across the entire state – UNI provides dispatch uninsured individuals with the health insurance
services to all MCOT teams. application process.
• Enhance the statewide crisis call center to serve as
the centralized hub for coordinating behavioral health
and crisis support services.
34 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs AssessmentSUMMARY
S U M M A RY
Community matters.
University of Utah Health is a proud member of our community. We strive to be an equal
partner, both offering our expertise, and listening to the experiences of the individuals
who make up our community. It is our commitment to collaborate with the intent to better
understand community needs, and work to address those needs both through internal
process improvement and by offering support outside our hospital’s four walls.
The COVID-19 pandemic has shown just how interconnected we all really are. It has
opened our eyes to health inequities that have existed long before COVID-19, and the
importance of addressing them going forward. It’s underscored the significance of
addressing chronic conditions earlier, to avoid co-morbidities and help individuals live
longer. We’ve forged new partnerships, and strengthened old ones. As a community that
is bonded together after going through a pandemic—we will survive, and we will thrive.
We would love to hear from you about how we can work together to make our community
healthier and stronger. Let’s connect.
RyLee Curtis Steve Eliason
Director, Community Engagement Sr. Director, Finance and Strategic Project
Rylee.Curtis@utah.edu Management
Steven.Eliason@hsc.utah.edu
36 2021-2023 University of Utah Health Hospitals and Clinics Community Health Needs Assessment50 N. Medical Drive
Salt Lake City, UT 84132
801-581-2121You can also read