Building a Community of - Practice to Support Hepatitis B Birth Dose Introduction in the African Region
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Building a Community of
Practice to Support Hepatitis B
Birth Dose Introduction in the
African Region
Stakeholders Meeting #3:
Sharing NITAG Experiences with Hepatitis B
Birth Dose and NITAG Tookit | June 17, 2021
A program of
Executive Summary
In Africa, an estimated 87,890 deaths are caused by hepatitis B (HepB) each year, and the
6.1% estimated prevalence rate stands among the highest globally. Contracting HepB
during infancy conveys the highest risk of chronic infection, and only 14 countries in
Africa have implemented the HepB birth dose vaccine. Hep B surface antigen prevalence
in children under age 5 in Africa hovers at 2.53%, well above the global interim elimination
target of less than 1%. With an estimated 296 million people worldwide living with
chronic HepB and 82 million of these people in the African region, the need for effective
interventions is urgent.
How can public health and other partners support African countries in introducing
and scaling up timely HepB birth dose vaccine? In collaboration with the World Health
Organization (WHO) and the Global Immunization Division of the U.S. Centers for Disease
Control and Prevention (CDC), the Coalition for Global Hepatitis Elimination (CGHE) is
convening stakeholders in a community of practice toward the successful introduction
and scale-up of the birth dose vaccine for the WHO AFRO region. By providing evidence-
based strategies that can be applied locally, this series supports information sharing,
peer-to-peer collaboration, technical assistance, and capacity building within countries.
To date, these stakeholder meetings have drawn more than 220 unique participants with
24 African countries represented.
Source: Slide 2 from Dr. Njuguna’s presentation on Recap of Previous Meetings (March 17-18 and May 5, 2021)
Key takeaways to date for the Community of Practice series:
• Key challenges for birth dose introduction include (1) insufficient coordination
between expanded program on immunization (EPI) staff members and maternal and
child health (MCH) programs; (2) logistical and operational barriers posed by home
births.
• Greater awareness is needed among policy makers about how the birth dose helps
eliminate mother-to-child transmission (MTCT) and how cost effective it can be.
• More advocacy is needed to build local support among health care workers and to
increase grassroots demand (by mothers) for the birth dose vaccine.
2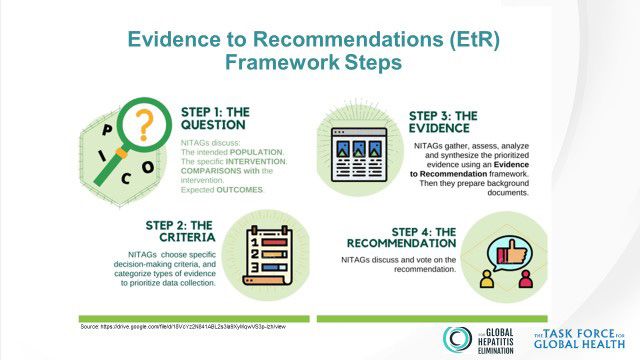
• There is an ongoing need for funding and for Gavi support to introduce and scale up
the birth dose vaccine across African countries.
The third meeting (June 17) explored the role of National Immunization Technical Advisory
Groups (NITAGs) within HepB birth dose vaccine introductions and roll-outs, highlighting
key evidence and critical information that NITAGs need to develop appropriate
recommendations for birth dose vaccine introduction. NITAG and EPI representatives
explained their countries’ recommendation processes and helped identify technical
needs for countries that wish to introduce the vaccine. Following case examples from
Senegal and Zimbabwe and a panel discussion, CGHE staff member Dr. Henry Njuguna
presented a draft toolkit for feedback. The toolkit aims to assist countries with the NITAG
process, including steps for building evidence to support the birth dose recommendation.
Key takeaways from the June 17 meeting:
• Successful NITAGs are those that provide strong evidence-based recommendations
incorporating local data wherever possible. Modeling data are also useful when local
data are difficult to obtain.
• As they compile evidence for HepB birth dose vaccine introduction, NITAGs should
think across the lifespan and work across disease areas to demonstrate the true
burden of hepatitis B. Those working in MCH and liver cancer are in different silos, so
the true costs of not vaccinating can sometimes be underestimated.
• There is a gap between a successful recommendation (by the NITAG) and successful
implementation (by the Ministry of Health). Political will and funding challenges can
contribute to this gap. Government support is essential for vaccine introduction;
reliance on Gavi and external funders alone is not sufficient for sustainability.
• Empowering NITAGs means allowing them to make independent decisions at the
country level. While there will often be multiple opinions on a given question, NITAGs
should make evidence-based recommendations that support the best interest of
their communities.
3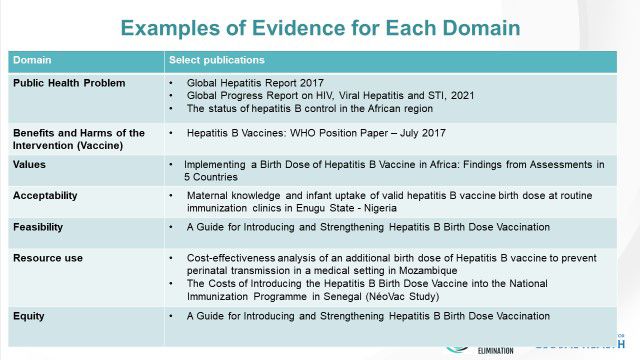
Presentation Highlights
The role of NITAG in the introduction of new vaccines
Dr. Abigail Shefer, CDC GID
NITAGs form part of the WHO Immunization Policy Advisory Framework and function
on the national level. Globally, 170 countries have established NITAGs, with 123 of these
considered functional since they have met the six WHO defined process indicators.
NITAGs serve both as a technical resource and a deliberative body; they also play an
increasing role in advising governments on approaches to address vaccine confidence
and coverage, helping recommend locally customized applications.
Benefits of involving NITAGs in policy decision making:
• Increasing credibility of governmental policy decisions by having a rigorous evidence-
based decision-making process
• Minimizing pressure from outside interest groups, including industry when needed
• Providing transparency by eliminating real or apparent personal conflicts of interest
• In case of an adverse event from immunization, NITAGs can neutralize public backlash
Immunization Agenda 2030: Vision = A world where everyone, at every age, fully benefits
from vaccines for good health and well being
• NITAGs play a key role in this effort with involvement in Strategic Priority 2,
commitment/ ownership and accountability.
• NITAGs provide input to strengthen evidence-based decision making (EBDM).
• Guidance and platforms for monitoring and evaluation are provided in part by NITAGs.
• The specifics of the 2030 agenda remain under development and are country-
specific.
4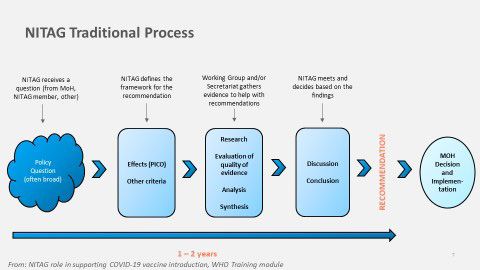
NITAGs Status in WHO AFRO Region
Dr. Sidy Ndiaye, WHO/AFRO
Currently, 37 countries have established a NITAG in the WHO AFRO region, and 25 of these
qualify as fully functional for having met the six WHO defined quality indicators. NITAGs
are evaluated annually based on these criteria. The NITAG maturity model is a new tool
under development by a working group led by US CDC that ranks a country’s NITAG
according to criteria and key indicators, with special focus on functionality, processes,
and the recognition of the NITAG in the immunization system.
Ongoing NITAG activities in the AFRO region include:
• Updating/adapting existing training materials, including online training materials on
the Evidence to Recommendation (EtR) process
• Assessment tool for advancing the NITAG Maturity Model
• COVID19 and other vaccine introductions
• Introduction of SYSVAC, a global registry launched in December 2020 that aims to
make it easier for NITAGs to identify relevant systematic reviews and access guidance
on using existing reviews (through an online course). Priority is currently given to
reviews of COVID19 (burden, risk factors, vaccine); other diseases will be added in
2021.
Current challenges facing NITAGs include:
• Addis Declaration on Immunization (ADI) road map target on NITAG establishment in
countries has not been achieved.
• Integration of the NITAGs in immunization decision-making process has not been
systematized in all countries.
• Sustainability of NITAG activities remains an uphill battle: financing is needed as well
as increased staffing.
• Local data availability remains insufficient with more evidence needed.
Recommendations for the way forward:
• Continue advocacy for NITAG establishment in the 10 remaining countries in the
African region and for effective functionality in those that already have NITAGs.
• Release new training materials and tools.
• Pilot test maturity model assessment tool.
• Implement regional scientific hub project (Vaccines for Africa / University of Cape
Town) with Wellcome Trust funding.
5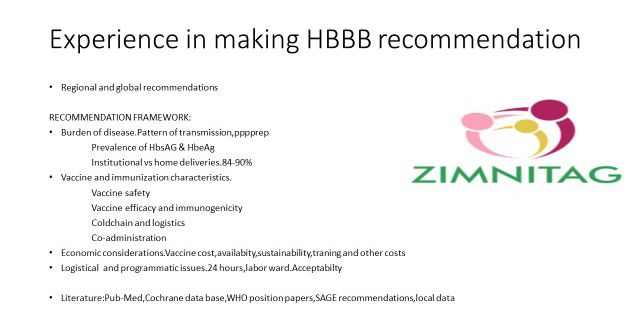
The NITAG hepatitis B birth dose process in Senegal
Professor Anta Tal Dia, Advisory Committee for Vaccination in Senegal (CCVS)
• Senegal's NITAG, the Comité Consultatif pour la Vaccination au Sénégal (Advisory
Committee for Vaccination in Senegal, or CCVS), is the advisory body responsible for
issuing scientific and technical opinions and recommendations to guide the Ministry
of Health in national vaccination policies and strategies.
• CCVS began working in 2014 to address the question of the HepB birth dose vaccine:
◦ A working group was formed to define the basis for the recommendation, to
research/analyze the evidence, and to submit a report with recommendations.
◦ The evidence search focused on HepB infection rates and transmission in
newborns, the efficacy and safety of the vaccination at birth, and the economics
of the vaccine at birth. The group also examined the administration/time period
(24 hours) and operational aspects.
• After reviewing evidence, CCVS recommended introduction of the HepB birth dose
vaccine. The committee further recommended:
◦ Making the vaccine available in all health facilities likely to house deliveries
◦ Strengthening antenatal consultations in both volume and quality
◦ In the case of home deliveries, vaccinating at the first contact with a health
facility
◦ Ensuring financial sustainability
• The recommendation process did not encounter any major difficulties. But the
exhaustive bibliographic search, particularly for articles that are not open access,
encountered pitfalls.
• Recommendations for continued implementation include:
◦ Need for MCH and EPI collaboration, as well as private sector partnerships
◦ Need to build MCH capacity to provide the vaccine through training, job aids, and
more
◦ Need to ensure the vaccine is available in all birthing facilities
6
The NITAG hepatitis B birth dose process in Zimbabwe
Dr. N.A. Gonah, ZIMNITAG
• Formed in 2011 and reestablished in 2016, Zimbabwe’s NITAG, or ZIMNITAG, made a
recommendation in 2018 to implement the HepB birth dose vaccine, but the Ministry
of Health has not yet implemented that recommendation.
• The technical process leading to the recommendation included the following
elements:
◦ Burden of disease demonstration
◦ Analysis of vaccination and immunization characteristics
◦ Economic considerations (cost, availability, sustainability, training, etc.)
◦ Consideration of logistical and programmatic issues (24-hr window, labor ward)
Source: Slide 5 from Dr. Gonah’s presentation
• Challenges leading to lack of implementation included:
◦ Complicated interactions between NITAG and the MoH; policy makers not making
the HepB BD a priority
◦ Leadership changes and transitions
◦ Burden of disease data – more needed, including seroprevalence study within first
six weeks of birth
◦ Sustainability: overreliance on Gavi support meant that officials did not want to
move forward when Gavi decided not to finance the birth dose vaccine
◦ Vaccine resources strained by the COVID19 pandemic
7Highlights from Panel Discussion
NITAG experiences with decision making for the introduction of
hepatitis B birth dose
Burkina Faso (Dr. Jean Kabore)
Ghana (Prof. George Armah)
South Africa (Prof. Rose Burnett/Dr. Melinda Suchard)
Moderators: Dr. Sidy Ndiaye/Dr. John Ward/Dr. Henry Njuguna
Burkina Faso (Dr. Jean Kabore)
• The NITAG received a request from Burkina Faso’s Ministry of Health in July 2020 to
address questions around the introduction of the HepB birth dose vaccine. The NITAG
established working groups around vaccine characteristics, disease epidemiology,
economic and operational considerations, and programmatic issues; members also
considered local studies that estimated prevalence.
• All working groups have completed their tasks; the next step is to convene a plenary
session to write a draft recommendation. This plenary has been delayed due to
challenges with member availability and competing priorities within the secretariat
(COVID19 outbreaks). Another major challenge remains lack of funding.
Ghana (Prof. George Armah)
• Ghana’s NITAG was established in 2018 and has not yet looked at the HepB birth dose
vaccine. NITAG members are working with EPI to determine what data is available.
• Evidence-based data will be a major challenge; Ghana needs to look not only at
vaccine introduction but also at data capture systems: How can we improve data
collection that is needed for effective advocacy?
• In chat discussion, it was also noted that CDC is working with Ghana’s EPI and Ghana’s
health service to implement serosurveys to estimate HepB prevalence in children and
pregnant women, and to assess the risk of MTCT in Ghana. These will help inform the
NITAG’s future deliberations.
South Africa (Prof. Rose Burnett/Dr. Melinda Suchard)
• National Advisory Group on Immunization (NAGI) made the decision not to recommend
the HepB birth dose vaccine. It is unusual for this NITAG to defer from WHO
recommendations, and not all NAGI members agreed with the decision.
• Since this recommendation, the country has seen political pushback and grassroots
advocacy for the birth dose introduction. The Minister of Health did not accept NAGI’s
recommendation, and South Africa’s 2019 national guidelines for managing viral
hepatitis do include the birth dose introduction. But the vaccine has not yet been
implemented, owing to NAGI’s recommendation against introduction and lack of
funding.
8NITAG toolkit for decision making in introduction of HepB-BD
Dr. Henry Njuguna
While the toolkit is still under development, notable components include the following:
• Adaptation of the evidence to recommendation (EtR) framework to suit the HepB
birth dose vaccine.
Source: Slide 7 from Dr. Njuguna’s presentation
• Steps for building evidence for the birth dose recommendation (show slide here: EtR
Framework Steps)
◦ Formulating and focusing the policy question: Should a birth dose of the HepB
vaccine be introduced? This broad question should be turned into specific policy
questions using the PICO (population, intervention, control, outcomes) method.
◦ Specifying evidence to be collected
◦ Gathering, assessing, and evaluating evidence
◦ Discussing and deciding on a recommendation
9Source: Slide 16 from Dr. Njuguna’s presentation
• Synthesis of available literature to help with evidence gathering (CGHE has done a
significant portion of this work already)
• Plan to share materials and seek feedback on utility of developed tools
• CGHE is available to offer technical assistance to support the NITAG process.
Resources include:
◦ Evidence base
◦ Help desk
◦ HepB Birth dose literature synthesis (ongoing)
◦ Technical support for Evidence to Recommendations framework
10Upcoming Meetings:
Meeting 4:
Next steps (July 22)
This meeting wraps up the series and finalizes plans for additional technical assistance,
including support to countries in the NITAG evidence to recommendation process to
support HepB birth dose introduction. These follow-up plans may include a Project
ECHO for EPI managers introducing and scaling up HepB birth dose vaccination and
related strategies. The agenda will be flexible and will be developed as the webinar series
progresses.
Meeting format:
Each webinar will be 1-2 days with 1 session per day, no session will last more than 3
hours.Each webinar will have a rapporteur and meeting report.
Simultaneous French translation will be provided.
Appendices
Summary of Q&A is available here.
11You can also read