Updated GP and Specialist Numbers for SA - MM3 Admin
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7
OCTOBER 2010
Updated GP and Specialist Numbers for SA
1 Introduction quoted sources that state that there 2 The Use of HPCSA Data
are 36,9123 doctors practising in
This note builds on National South Africa, we find evidence of The September 2010 ANC NHI
Health Insurance (NHI) Note 4 only 27,432 doctors practising in proposal (p. 35) uses figures from
that was published in November total (17,802 general practition- the Health Professions Council
2009.1 In that note the difficul- ers (GPs) and 9,630 specialists). of South Africa (HPCSA) to indi-
ties in obtaining accurate data on cate the total number of doctors.
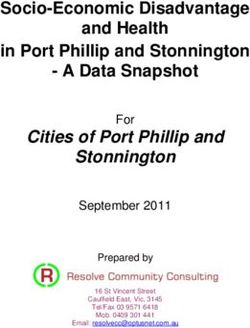
human resources in health (HRH) Furthermore, when the distribu- This data source shows a steady
in South Africa (SA) were pointed tion of these doctors between increase in medical practitioners
out. At that stage an effort was the public and private sectors (GPs and specialists) over the past
made to collect data from various is examined, our research indi- decade – data shown in Figure 1.
sources and to collate the data in cates an almost equal distribu-
order to arrive at a fair picture of tion of GPs between the two However, as previously explained
the number of doctors and nurses sectors: 2,861 people per GP in in NHI Note 4, the HPCSA fig-
in South Africa. Care was also tak- the public sector and 2,723 peo- ures overstate the number of doc-
en to emphasise the problems and ple per GP in the private sector. tors (GPs and specialists) actively
gaps in the officially available data. We find that contrary to popular working in SA. We know that the
perceptions about the spread of HPCSA figures (as given in Figure
The recent release of the resources, the majority (61.9%) 1) include doctors who are regis-
ANC’s latest NHI proposal2 in of GPs work in the public sector. tered in SA, but practise abroad or
September 2010, prompted us to While more specialists (56.2%) that have moved on to other occu-
update our initial HRH figures with work in the private sector, the pations (such as those in manage-
the latest available data. This note population ratios are also not as ment or other administrative jobs),
shows that contrary to officially skewed as commonly believed. but are still maintaining their regis-
This research note forms part of a series of notes dealing with issues of health reform in South Africa. In the interest of constructively contributing
to the NHI debate, the Hospital Association of South Africa (HASA) has commissioned this series of research notes which can be accessed on the
Econex website: www.econex.co.za.
1. Available on our website: www.econex.co.za
2. ANC National General Council 2010, Additional Discussion Documents. Released September 2010. Available at:
http://www.anc.org.za/docs/discus/2010/aditionalo.pdf (p.14)
3. See Figure 1.
1Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7 - OCTOBER 2010
Figure 1: Growth in medical practitioners (GPs and specialists), 2002-2010 doctors in SA. This note serves to
38 000 correct the misleading notion that
36 912
there are almost 37,000 doctors in
35 707
36 000 SA and aims to provide a more ac-
34 687
34 324 curate and up to date assessment.
34 000 33 220
32 198
32 000 31 214 3 Updated HRH Figures for
30 578 South Africa
29 903
30 000
Following from the above discus-
28 000 sion, Econex updated the work
2002 2003 2004 2005 2006 2007 2008 2009 2010 done in NHI Note 4 in order to
see how the situation might have
Source : HPCSA figures from ANC NHI proposal (September 2010) & Health Systems Trust changed since 2009, as well as to
provide the latest HRH figures. This
trations with the HPCSA. The HPC- non-payment, including more
should inform the ongoing debate
SA does not distinguish between than 6,300 emergency care
around the details and implemen-
doctors actively working in SA as practitioners and 1,942 medi-
tation of a NHI system in South
clinicians and those who are not cal practitioners and dentists.”
Africa. Table 1 provides the latest
practising here or are not practis- This was confirmed in a media
estimates for GPs and specialists
ing as doctors, and therefore these statement4 by the HPCSA ear-
actively working in South Africa.
numbers are inappropriate indi- lier this year, saying that, “Last
cators and over-estimate the true year the HPCSA was forced to
3.1 Data sources and scenarios
number of doctors working in SA. suspend some 12,800 practition-
ers who did not comply with In accordance with our original
Evidence of this comes from the their requirements...” (To date, methodology, we used the latest
HPCSA themselves. In the SA Health however, this reduction in the data from the government’s pub-
Review (2008: 358) there is refer- data has not been observed.) lic sector Personnel and Salary
ence to an announcement by the Administration System (PERSAL)
Registrar of the HPCSA at the Consequently, it is not appropriate as a starting point for both GPs
time that “11,500 healthcare to use these inaccurate figures, as (11,309) and specialists (4,442) in
practitioners would be erased for an estimate of the total number of the public sector in 2010. Medical
About ECONEX
ECONEX is an economics consultancy that offers in-depth economic analysis covering competition economics, international trade, strategic analysis
and regulatory work. The company was co-founded by Dr. Nicola Theron and Prof. Rachel Jafta during 2005. Both these economists have a wealth
of consulting experience in the fields of competition and trade economics. They also teach courses in competition economics and international
trade at Stellenbosch University. Director, Cobus Venter, who joined the company during 2008, is also a Senior Economist at the Bureau for
Economic Research (BER) in Stellenbosch. For more information on our services, as well as the economists and academic associates working at and
with Econex, visit our website at www.econex.co.za.
4. HPCSA Media Statement, 11 March 2010. Available at:
http://www.hpcsa.co.za/downloads/press_releases/current/hpcsa_annual_fees_now_due.pdf
2Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7 - OCTOBER 2010
scheme industry estimates (6,949 bers – especially when it comes to figures were used as is, while
GPs and 5,695 specialists) were the population ratios in section 4. the private sector estimates were
used for the updated totals in the decreased with 5% and 10% for
private sector, based on doctors When analysing Table 1, one GPs and specialists respectively.
visited by members and subse- should keep in mind that it is not
quently reimbursed by schemes. only the underlying split between 3. For the third scenario the
the private and public sectors that adjustments to the PERSAL and
In order to avoid double count- is important, but rather the abso- medical scheme industry esti-
ing, one has to exclude from lute number of doctors in the coun- mates were split between the
the public sector part-time try. That is ultimately what we are two sectors, i.e. a 2.5% decrease
and sessional doctors that trying to determine. The need for for GPs were made in the pub-
are working primarily in the doctors over the next decade or lic and the private sectors, while
private sector, but one also has to two should therefore be assessed we subtracted 5% from the spe-
exclude doctors in the private sec- based on the total number actively cialist figures in both sectors.
tor who primarily work in the pub- working in SA (as will be shown in
lic sector. Since there is no indi- the following Health Reform Note). From the figures above one can
cation in either dataset who these see that the different scenarios
doctors may be, or exactly how Three human resource sce- do not yield significantly dif-
many there are, it is a very difficult narios are created to address ferent numbers. Whilst some
adjustment to make. If one were the issue of double count- industry experts believe the in-
to make the adjustment in both ing (i.e. where doctors work in cidence of public sector doctors
sectors, one would certainly un- both public and private sectors): working part-time in the private
derestimate the number of doctors. sector is more prevalent than the
1. In the first scenario the other way around, we are cau-
Medical scheme industry esti- respective 5% and 10% de- tious not to underestimate private
mates assume that there are 5% creases for GPs and specialists sector resourcing. We therefore
of private GPs and 10% of private were made in the public sector elected to use the third scenario to
specialists in their databases who alone. Thus, the PERSAL figures determine the most likely number
are working in the public sector given above were adjusted ac- of doctors in SA, as opposed to the
as well as the private sector (and cordingly, while the private sec- second scenario. Accordingly, the
are therefore already included in tor estimates were left unadjusted. best estimates are a total of 17,802
the PERSAL data). However, we GPs and 9,630 specialists in the
do not make the adjustment in the 2. The second scenar- country, or 27,432 doctors in total.
private sector only as this meth- io assumed the same adjust-
odology may result in underes- ments, but for the private sector This total is in line with a recent
timating the private sector num- only – implying that the PERSAL statement by the South African
More Information
ECONEX regularly publishes Research Notes on various relevant issues in South African competition, trade and applied economics. For access to
previous editions of Research Notes, or other research reports and published articles, go to: www.econex.co.za
If you want to add your name to our mailing list, please send an e-mail to iris@econex.co.za
3Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7 - OCTOBER 2010
Table 1: Updated estimates of active doctors, 2010
by Wadee and Kahn8 reported in
the media, even though the au-
Public Private Total
thors acknowledge that there is a
GPs “paucity of data regarding the
true public-private distribution of
- scenario 1 10,744 6,949 17,693 HRH and the public-private split
is contested...” (2008: 143). Ac-
- scenario 2 11,309 6,602 17,911
cording to their estimates, 27.4%
- scenario 3 11,026 6,775 17,802 of GPs work in the public sector
vs. 72.6% in the private sector,
Specialists while 24.8% of specialists work
in the public sector compared
- scenario 1 3,998 5,695 9,693
to 75.2% in the private sector.
- scenario 2 4,442 5,126 9,568
However, using the updated num-
- scenario 3 4,220 5,410 9,630 bers from scenario 3 as calculated
above in Table 1, the public / pri-
Total doctors (scenario 3) 15,246 12,186 27,432 vate split looks substantially dif-
ferent from Wadee and Kahn’s es-
Source : Medical scheme industry estimates and PERSAL
timates. Table 2 gives the revised
Medical Association (SAMA) firms, “There is the need for a distribution which looks very sim-
who estimates that with 14,000 central data source on special- ilar to the most recent estimates
members they represent about ists (and all medical and dental from the CMSA. They find that
half of SA’s doctors.5 Also the professionals) which is moni- 42.1% of GPs work in the private
College of Medicines in South tored and updated annually.”7 sector and 57.9% in the public sec-
Africa (CMSA) estimated that tor, and of specialists 55.6% work
there were about 27,641 doc- in the private sector with 44.4%
tors in SA at the end of 2009.6 4 Public / Private Sector Split working in the public sector.9
The fact that one has to consider As was pointed out in NHI Note
various scenarios and use differ- 4, there is a common misconcep- 5 Population Ratios
ent data sources in order to ob- tion about the relative distribution
tain the best estimate, emphasises of doctors and specialists between Another important point is that
the danger of using the HPCSA the public and private sectors. the distribution of GPs between
figures as is. As the CMSA con- One often finds the figures given the public and private sectors
5. Kahn, T., 2010. “Plea for details of health insurance plan,” Business Day, 30 September. Available at: http://www.businessday.co.za/articles/Con-
tent.aspx?id=122325
6. Strachan, B., 2009. “Meeting South Africa’s Needs: A Preliminary Report of an Investigation into Specialist Training and Development,” The Colleges
of Medicine in South Africa.
7. See footnote 6. (p.34)
8. Wadee, H. & Kahn, F., 2008. “Human resources for health, “ Chapter 9 in the SA Health Review 2007.
9. See footnote 6.
4Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7 - OCTOBER 2010
Table 2: Updated public / private split, 2010 This is a very important result,
as the distribution of the popula-
tion between GPs in the public
Public Private
and private sectors are then almost
equal, and not as skewed as the
GPs 61.9% 38.1%
ANC proposal suggests. The reason
Specialists 43.8% 56.2% why these estimates are so differ-
ent is largely because of the use of
Source : Econex calculations the HPCSA numbers, as explained
previously. The mistake commonly
users is also different from what are based on overstated and out-of- made is to use the total number of
is commonly believed. McIn date HPCSA data from 2005. The medical practitioners registered
tyre et. al. (2007)10 estimate that proposal also does not draw from with the HPCSA as a starting point
35.8% of the population were de- other reliable sources to inform the and then subtract all GPs and spe-
pendent on the private sector for estimates. Accordingly, the indica- cialists on the PERSAL database to
primary healthcare services in tion is that there are 588 people arrive at the number of doctors in
2005. We updated this percentage per GP in the private sector (based the private sector. By using incor-
for 2010,11 and found that at least on 35.8% of the population seeing rect (and much larger) figures for
36.9% of the population currently private GPs in that year) and 4,193 the private sector specifically, one
utilise private medical services for people per GP in the public sector. would arrive at a much lower es-
their primary healthcare needs. However, our estimates show that timate for the population per GP.
This means that there are 0.37 GPs there are at least 2,723 people per
per 1,000 population in that group GP in the private sector and 2,861 Similar to the situation for GPs,
(private sector) and 0.35 GPs per people per GP in the public sec- medical scheme members are not
1,000 population for the rest of tor (see Table 3 for a comparison). the only ones seeing private sec-
the population who depend exclu-
Table 3: Population per general practitioner
sively on public sector services for
primary healthcare needs in 2010,
based on the latest figures in Table 1. Public Private
In the recent ANC NHI proposal12 ANC NHI proposal (2005 data) 4,193 588
the distribution of healthcare re-
Econex estimates (2010 data) 2,861 2,723
sources significantly differs from our
calculations, but the former figures
Source : ANC NHI proposal (September 2010) & Econex calculations
10. Mcintyre, D., Thiede, M., Nkosi, M., Mutyambizi, V., Castillo-Riquelme, M., Goudge, J., Gilson, L. & Erasmus, E., 2007. “A critical analysis of the cur-
rent South African health system,” Health Economics Unit, University of Cape Town and Centre for Health Policy, University of the Witwatersrand.
Available at: http://heu-uct.org.za/research/publications/reports-and-working-papers/
11. See methodology in Health Reform Note 4 on our website: www.econex.co.za.
12. See footnote 2. (p.14)
5Trade, Competition & Applied Economics
HEALTH REFORM NOTE 7 - OCTOBER 2010
tor specialists. Private hospital Table 4: Population per specialist
data indicate that about 15% of
their patients seeing private spe-
Public Private
cialists are not medical scheme
beneficiaries. Given that there are
ANC NHI proposal (2005 data) 10,811 470
8,126,193 medical scheme benefi-
ciaries at the moment,13 it implies Econex estimates (2010 data) 9,581 1,767
that 9,560,227 people (19.1% of
the total population) are depend- Source : ANC NHI proposal (September 2010) & Econex calculations
ent on private sector specialists,
while the remaining 80.9% sees cialist,”14 but rather a 5.4 times against the fact that the private sec-
only public sector specialists. Un- difference. tor is better resourced, it is shown
der that scenario, there are 0.57 that proportionally more GPs and
specialists per 1,000 population specialists are active in the public
in the private sector and 0.1 spe- 6 Conclusion sector than often reported. It was
cialists per 1,000 population in also shown that the population
the public sector. This translates In light of the current (proposed) per GP ratios quoted in the ANC
to the population per special- changes in the health sector in NHI proposal is incorrect, and
ist estimates shown in Table 4. SA, it is imperative that the policy that this ratio is roughly the same
debate is appropriately informed. for the private and public sectors.
Although the public sector esti- Hence, this note provided a brief
mates in Table 4 are close to each update on the HRH figures in SA. Our next note in this series will use
other, the private sector ratio still It shows that the widely used HPC- the updated HRH figures provid-
differs significantly between the SA data, which is also used in the ed here as a starting point to cal-
two sources. In other words, there ANC NHI proposal, overstates the culate different scenarios related
is not a “23 times difference in the number of doctors in this coun- to the future requirement/need for
number of people served per spe- try. Whilst there is no argument doctors and nurses, respectively.
ECONEX Services
Econex has extensive experience in competition economics, international trade and regulatory analysis. Strategic analysis was recently added as
practice area. We have an established reputation for providing expert economic advice for high profile mergers and complaints that appear before
the competition authorities. Some of the more recent highlights include the complaint against British American Tobacco, the merger between MTN
and iTalk, the complaint against Senwes and the acquisition of KayaFM by Primedia. Apart from competition work we have also been involved in
trade matters which included analyses of the effects of tariffs, export taxes and anti-dumping tariffs.
As a result of our work in competition analysis we also have invaluable experience in some of the sectors of the South African economy where
regulation continues to play a role, e.g. the telecommunications, health and energy sectors. We use economic knowledge of these sectors to
analyse specific problems for some of the larger telecommunications, health and energy companies.
13. Council for Medical Schemes, Quarterly Report for the period ended 31 March 2010. Available at:
http://www.medicalschemes.com/Publications.aspx
14. See footnote 2. (p.13)
6You can also read