Trombolisi sistemica: nuove evidenze (nuovi protocolli, nuovi farmaci, nuove finestre terapeutiche) - Siss Ictus
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Trombolisi sistemica: nuove
evidenze (nuovi protocolli,
nuovi farmaci, nuove finestre
terapeutiche)
Dott.ssa Marialuisa Zedde, MD, FESO
SC Neurologia, Stroke Unit
Azienda Unità Sanitaria Locale - IRCCS
Reggio Emilia (Italy)
Disclosures Consulting and conference fees from TAKEDA, SANOFI-GENZYME, AMICUS, BAYER, GE Advisory Board membership from Daiichi Sankyo and AMICUS
Pathways
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
During the past three decades, acute stroke reperfusion strategies have evolved from nihilism to thrombolytic therapy followed by endovascular therapy and recently to next generation endovascular devices and thrombolytic agents. The eligibility criteria and the drugs/devices for these two approved therapies have further evolved over the past two decades.
Time clock Tissue clock
TIME IS BRAIN In un minuto vengono persi circa 1.9 milioni di neuroni Saver J. Time is brain--quantified. Stroke. 2006 Jan;37(1):263-6
3 ore 4.5 ore
Time is brain is a fact in major artery occlusion stroke with small ischemic core but likely fiction in small distal artery stroke.
https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.04.001
https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.04.001
Slow progressors Fast progressors
Stroke. 2019;50:34-37TIME IS BRAIN COLLATERALS ARE THE PACE
TIME IS BRAIN ALSO FOR EVT
Longer OTR time was associated with a reduced likelihood of good outcome (OR for 30-minute delay,
0.74; 95% confidence interval [CI], 0.59–0.93).
Time to reperfusion is negatively associated with favorable outcome, being CT to reperfusion, as
opposed to onset to CT, the main determinant of this association. In addition, OTR was strongly
associated to outcome in patients with low ASPECTS scores but not in patients with high ASPECTS
scores.
Stroke. 2016;47:999-1004Endovascular therapy for ischemic stroke
Save a minute—save a week
Each minute saved in onset-to-treatment time
granted on average 4.2 days of extra healthy
life, with a 95% prediction interval 2.3–5.4.
Women gained slightly more than men due to
their longer life expectancies. Patients
younger than 55 years with severe strokes of
NIH Stroke Scale score above 10 gained more
than a week per each minute saved.
In the whole cohort, every 20 minutes
decrease in treatment delays led to a gain of
average equivalent of 3 months of disability-
free life.
Neurology 2017;88:2123–2127BUT MAINLY IN FAST PROGRESSORS
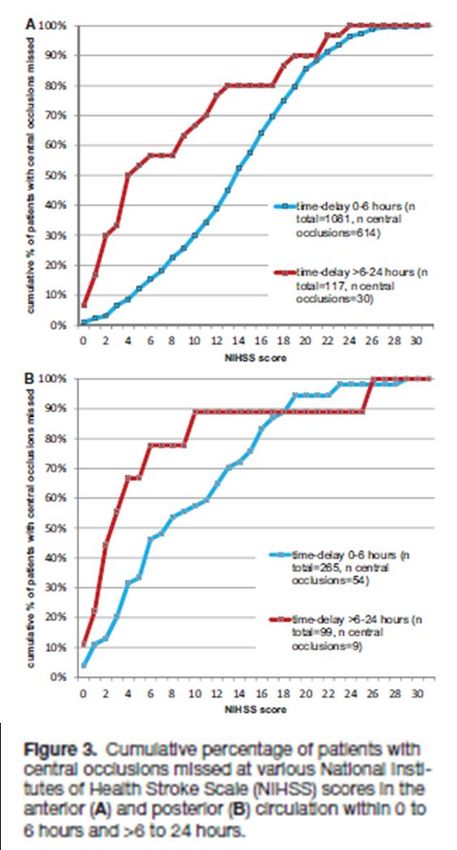
Which is the proportion of acute stroke
patients with LVO ?1043 patients (48.5%) showed a VO on MRA or CTA, 887 in the AC and 156 in the PC. 860 (82.45%) VOs were central, 775 in the AC and 85 in the PC.
CSC
Within 6 hours
EVT
10.5% according to AHA/ASA criteria
17.7% according to criteria reembling RCTs
IVT
36.2%What about «tissue clock» also for IVT?
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
Int J Stroke, Vol 10, October 2015, 1119–1129
Int J Stroke, Vol 10, October 2015, 1119–1129
• The proportion of eligible patients who are eventually treated with intravenous thrombolysis (IVT) is not known. • We prospectively analyzed data from 1184 consecutive ischemic stroke patients admitted to the 22 Stroke Units (SUs) of the Veneto region in order to assess the proportion of ischemic strokes potentially eligible and actually treated with IVT, and to explore the reasons for not administering IVT. • Out of 841 (71%) patients who presented within 4.5 h of stroke onset, 704 (59%) had no other absolute exclusion criteria and were therefore potentially eligible for IVT according to the current guidelines; however, only 323 (27%) patients were eventually treated with IVT. • Only 46% (323/704) of the potentially eligible patients were actually treated with IVT in the SUs of the Veneto region.
European Journal of Neurology 2019, 26: 1091– 1097
ANN NEUROL 2019;86:770–779
In acute ischemic stroke, EVT and IVT appear similarly effective in achieving favorable outcome at 3
months for patients with LVO and mild neurologic symptoms. EVT might be marginally inferior to IVT
regarding outcome across all levels of disability and mortality.
FurtherstudiesarerequiredtodeterminewhethercertainsubgroupsofpatientswithLVOand mild symptoms
benefit from EVT.
Neurology® 2019;93:e1618-e1626OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
Telecteplase vs alteplase
< 6 hours
Alteplase (N=25) or TNK 0.1 mg/kg (N=25)
or 0.25 mg/kg (N=25)
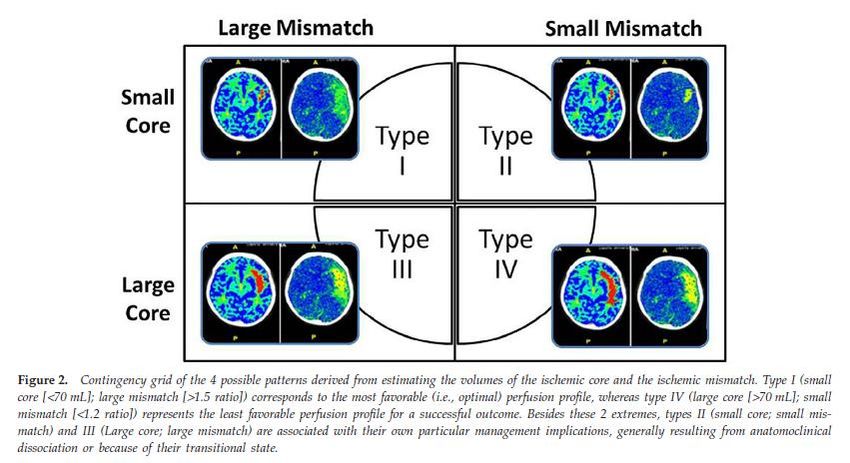
the eligibility criteria were a perfusion
lesion at least 20% greater than the
infarct core on computed tomographic
(CT) perfusion imaging at baseline and
an associated vessel occlusion on CT
angiography.
Of the 2768 patients who were screened
for participation in the study, 75
underwent randomization to the three
treatment groups.
N Engl J Med 2012;366:1099-107The Alteplase-Tenecteplase Trial Evaluation for Stroke Thrombolysis (ATTEST) trial of 0.25 mg/kg
of tenecteplase compared to 0.9 mg/kg alteplase was completed and collected perfusion
and angiographic imaging as a biomarker for clinical outcome and enrolled patients
clinically eligible for thrombolysis and failed to demonstrate a significant clinical
improvement in patients treated with tenecteplase.
Lancet Neurol 2015;14:368–376
The Australian-TNK trial required a large vessel occlusion on baseline CT angiography (CTA)
and substantial mismatch on baseline CT perfusion (CTP) imaging for study enrollment and
compared tenecteplase doses of 0.1 mg/kg and 0.25–0.9 mg/kg alteplase. The Australian-
TNK trial noted similar imaging and clinical outcomes recanalization between the 0.1 mg/kg
tenecteplase arm and the 0.9 mg/kg alteplase arms.
However, better early clinical improvement, recanalization, and higher rates of favorable
day 90 outcome were seen with 0.25 mg/kg of tenecteplase.
N Engl J Med 2012;366:1099–1107Tenecteplase in ischemic stroke offers improved recanalization
Analysis of 2 trialsNeurology 2017;89:1–6
Lancet Neurol 2017; 16: 781–88
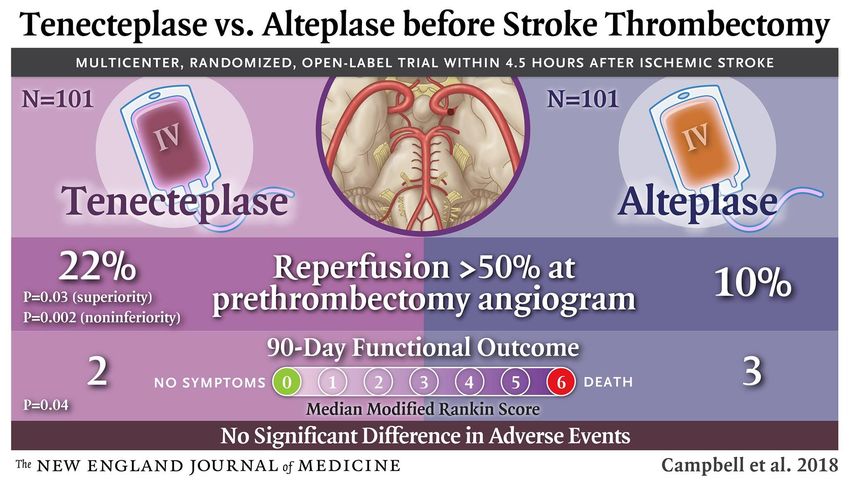
N Engl J Med 2018;378:1573-82
mRS 0-1
mRS 0-2
Future evidence
International Journal of Stroke 2018, Vol. 13(9) 885–892International Journal of Stroke 0(0) 1–6
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
Lancet Neurol 2015: 14: 575–84
Lancet 2018; 392: 1247–56
N Engl J Med 2018;378:11-21
N Engl J Med 2018;378:708-18
Turc G, et al. J NeuroIntervent Surg 2019;0:1–30
Stroke. 2019;50:00-00
< 80 years
mRS 0-1
Stroke < 1/3 MCA
territory on MRI
NIHSS < 25
No indications for
EVT
N Engl J Med 2018;379:611-22Patients were eligible for inclusion if they were at least 18 years of age; had excellent functional status before enrollment (mRS
International Journal of Stroke 0(0) 1–8
Lancet 2019; 394: 139–47
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
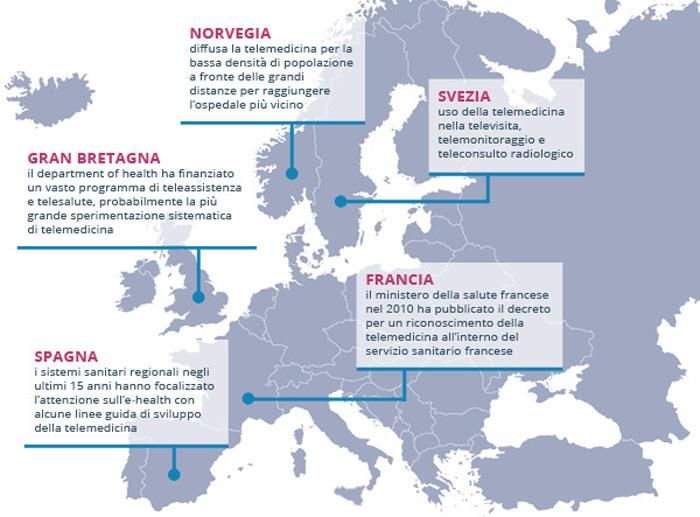
Telestroke: gli scenari possibili
Two years of Finnish Telestroke
Thrombolysis at spokes equal to that at the hub
Thus the patients treated with thrombolysis based on teleconsultation had similar outcome with
those treated at HUCH (mRS 0–2: 49.1% vs 58.1%, p 0.214 and mRS 0–1: 17/57 [29.4%] vs 352/957
[36.8%], p 0.289).
Neurology 2011;76:1145–1152OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
OUTLINE 1. Premessa: «time is brain» rivisitato 2. Trombolisi sistemica: certezze e aree grigie 3. Nuovi trombolitici 4. Finestra temporale estesa 5. Telestroke 6. Linee guida 7. Impatto sull’organizzazione dei percorsi
Evolution of Acute Ischemic Stroke (AIS) Care
over two decades 2015
< 4.5 hr < 24 hr DAWN, DEFUSE 3
Endovascular 4.5-24hr
CTA-CTP selected
DEFUSE
Alteplase 3-6hrs IMS III, MR MR-WITNESS
ASK
MRI-selected RESCUE, Alteplase 4.5-24hr
Streptokinase
SYNTHESIS MRI-selected
0-4 hrs
DIAS / DEDAS DIAS-2 Endovascular NOR-TEST
NINDS IV tPA Desmoteplase 3- Desmoteplase 3- Early Devices Tenecteplase WAKE-UP
Alteplase 0-3 hrs 9hrs MRI-selected 9hrs MRI-selected < 5-8hr 0-4.5hr Alteplase > 4.5hr
MRI-selected
1996 2005-2006 2009 2013 2017
1995 1998 2008 2012 2015 2018
ECASS I ATLANTIS ECASS-3 Tenecteplase MR CLEAN, ESCAPE, EXTEND-IA, EXTEND-IA TNK
Alteplase 0-6hr Alteplase 3-5 hrs Alteplase 3-4.5hr vs. Alteplase 0- SWIFT-PRIME, REVASCAT Tenectoplase 0-6hr
4.5hr CTP- Endovascular New Devices < 6-12hr CTP-selected + LVO
ECASS II EPITHET selected + LVO
Alteplase 3-6 hrs Alteplase 3-6hr PRISMS
MRI-selected Alteplase 0-3hr
Non-DisablingAcute ischemic stroke decision-making
1988
Stroke Symptoms
Head CT
Acute Ischemic Stroke
AdmitAcute ischemic stroke decision-making
Stroke Symptoms < 3 hrs from
1998 time Last Known Normal (LKN)
Head CT
Acute Ischemic Stroke
Go to IV tPA protocol -
Eligible for IV tPA?
No
Yes Admit
Give IV tPAAcute ischemic stroke decision-making
Stroke Symptoms < 4.5 hrs from
time Last Known Normal (LKN) 2008
Head CT
Acute Ischemic Stroke
Go to IV tPA protocol -
Eligible for IV tPA?
No
Yes Admit
Give IV tPAStroke Symptoms < 24 hrs from time Last
Acute ischemic stroke decision-making
Go to Wake-up /
Unwitnessed
Known Normal (LKN) and Head CT without ICH
Onset hMRI
Stroke Protocol
Acute Ischemic Stroke Mimic vs. AIS Stroke Mimic
Yes
Yes Go to HyperAcute MRI No
Wake-up / Protocol; DWI c/w AIS?
Unwitnessed stroke
> 4.5 hr from LKN, Triage per
can get hMRI and be Prelim. Dx
Go to IV tPA protocol: LKN <
treated with IV tPA < 4.5 hr and eligible for IV tPA? Yes
4.5 hr from sx
discovery? No Give IV tPA
No (and has not
received tPA) NIHSS ≥ 6 and LKNStroke Symptoms < 24 hrs from time Last
Known Normal (LKN) and Head CT without ICH
Go to Wake-up /
Unwitnessed
Onset hMRI
Stroke Protocol
Acute Ischemic Stroke Mimic vs. AIS Stroke Mimic
Yes Education
Yes Go to HyperAcute MRI No - Neurology MD
Wake-up / Protocol; DWI c/w AIS?
Unwitnessed stroke - EM MD/RN
> 4.5 hr from LKN, Triage per
can get hMRI and be Prelim. Dx - Radiology MD
Go to IV tPA protocol: LKN <
treated with IV tPA < 4.5 hr and eligible for IV tPA? Yes - MRI techs
4.5 hr from sx
discovery? Give IV tPA
No
No (and has not
received tPA) NIHSS ≥ 6 and LKN3 ore 24 ore
Thank you for your attention
Emerg Med Clin N Am 37 (2019) 365–379
You can also read