Validation of the ABCD Score in Identifying Individuals at High Early Risk of Stroke After a Transient Ischemic Attack
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Validation of the ABCD Score in Identifying Individuals at
High Early Risk of Stroke After a Transient
Ischemic Attack
A Hospital-Based Case Series Study
Georgios Tsivgoulis, MD; Konstantinos Spengos, MD; Panagiota Manta, MD;
Nikolaos Karandreas, MD; Thomas Zambelis, MD; Nikolaos Zakopoulos, MD;
Demetrios Vassilopoulos, MD, PhD
Background and Purpose—A simple score derived in the Oxfordshire Community Stroke Project (ABCD score) was able
to identify individuals at high early risk of stroke after a transient ischemic attack (TIA) both in a population-based and
a hospital-referred clinic cohort. We aimed to further validate the former score in a cohort of hospitalized TIA patients.
Methods—We retrospectively reviewed the emergency room and hospital records of consecutive patients hospitalized in
our neurological department with a definite TIA according to the World Health Organization (WHO) criteria during a
5-year period. The 6-point ABCD score (age [⬍60 years⫽0, ⱖ60 years⫽1]; blood pressure [systolic ⱕ140 mm Hg and
diastolic ⱕ90 mm Hg⫽0, systolic ⬎140 mm Hg and/or diastolic ⬎90 mm Hg⫽1]; clinical features [unilateral
weakness⫽2, speech disturbance without weakness⫽1, other symptom⫽0]; duration of symptoms [⬍10 minutes⫽0, 10
to 59 minutes⫽1, ⱖ60 minutes⫽2]) was used to stratify the 30-day stroke risk.
Results—The 30-day risk of stroke in the present case series (n⫽226) was 9.7% (95% CI, 5.8% to 13.6%). The ABCD
score was highly predictive of 30-day risk of stroke (ABCD⫽0 to 2: 0%, ABCD⫽3: 3.5% [95% CI, 0% to 8.2%],
ABCD⫽4: 7.6% [95% CI, 1.2% to 14.0%], ABCD⫽5: 21.3% [95% CI, 10.4% to 33.0%], ABCD⫽6: 31.3% [95% CI,
8.6% to 54.0%]; log-rank test⫽23.09; df⫽6; P⫽0.0008; P for linear trend across the ABCD score levels ⬍0.00001).
After adjustment for stroke risk factors, history of previous TIA, medication use before the index TIA, and secondary
prevention treatment strategies, an ABCD score of 5 to 6 was independently (P⬍0.001) associated with an 8-fold greater
30-day risk of stroke (hazard ratio, 8.01; 95% CI, 3.21 to 19.98).
Conclusions—Our findings validate the predictive value of the ABCD score in identifying hospitalized TIA patients with
a high risk of early stroke and provide further evidence for its potential applicability in clinical practice. (Stroke. 2006;
37:2892-2897.)
Key Words: ABCD score 䡲 prognosis 䡲 stroke 䡲 transient ischemic attack
R ecent population-based studies have documented that
transient ischemic attacks (TIAs) constitute a strong
predictor of subsequent stroke, with the 90-day stroke risk
identify individuals at high early risk for stroke after a TIA.7
Aim of the present hospital-based case series study was to
further validate the former score in a cohort of hospitalized
following a TIA ranging from 9.5% to 14.6%.1– 4 However, a TIA patients.
substantial international variation in the acute management of
individuals presenting to the emergency room (ER) with TIA Methods
(emergency inpatient care versus nonemergency outpatient Patient Selection
clinic assessment) exists because of the inability to identify A series of 238 consecutive patients hospitalized in our institution
the patients who are at highest risk for early stroke.5,6 A between January 2000 and December 2004 with a diagnosis of
simple score derived in the Oxfordshire Community Stroke definite TIA according to the World Health Organization standard
Project (OCSP) on the basis of age, blood pressure (BP), definition8 were initially screened.
All patients presenting at the ER of the Neurology Department of
clinical features, and duration of TIA symptoms (ABCD our institution are primarily screened by the attending neurologist.
score) was validated both in a population-based and a An initial brain CT scan is routinely performed in all TIA patients at
hospital-referred clinic cohort as a practical tool able to the ER or within 24 hours from hospital admission. The diagnostic
Received June 4, 2006; final revision received July 29, 2006; accepted August 11, 2006.
From Departments of Neurology (G.T., K.S., P.M., N.K., T.Z., D.V.) and Clinical Therapeutics (N.Z.), University of Athens School of Medicine,
Athens, Greece.
Correspondence to Georgios Tsivgoulis, Iofontos 2, 11634-Athens, Greece. E-mail tsivgoulisgiorg@yahoo.gr
© 2006 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000249007.12256.4a
2892
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 2015Tsivgoulis et al ABCD Score and Stroke Risk in TIA Patients 2893
work-up of the TIA patients during hospitalization includes extracra- Statistical Analysis
nial Doppler/duplex ultrasonography in nearly all cases, whereas Statistical comparisons were performed between subgroups of pa-
brain MRI, transthoracic or transesophageal echocardiography, and tients using the 2 test (or the Fisher exact test) and the unpaired t test
magnetic resonance or digital subtraction angiography and 24-hour (or Mann-Whitney U test) as indicated. The Kaplan-Meier product-
heart rate monitoring are performed in selected cases. All TIA and limit method was used to estimate the cumulative probability of
stroke patients hospitalized in our Neurology Department are in- subsequent stroke after 1 month from the index TIA. Differences in
cluded in a computerized observational data bank and their demo- stroke-free survival between groups stratified by the ABCD score
graphic characteristics, risk factors, history of previous TIA, pre- were assessed for statistical significance with the log-rank test.
vious medications, and secondary prevention therapies during Sensitivities and specificities of prediction were determined at each
hospitalization and after discharge are documented as elsewhere cut-off of the score and the receiver operating characteristic curve
described.9,10 More specifically, patients were diagnosed as having was plotted. Cox proportional hazards regression modeling was used
a history of hypertension, if they had evidence of systolic BP to identify factors that increased the risk of subsequent stroke after a
ⱖ140 mm Hg or diastolic BP ⱖ90 mm Hg or if they had received TIA. In the initial univariate analyses the association of demographic
any antihypertensive medication at any time before presentation to characteristics, stroke risk factors, previous medication use, second-
the ED.11 Diabetes mellitus was specified as fasting serum glucose ary prevention therapies, and the ABCD score with the 30-day risk
ⱖ7.0 mmol/L, nonfasting serum glucose ⱖ11.1 mmol/L, or use of of stroke was investigated. All factors that contributed to the
oral blood sugar-lowering drugs or insulin.12 Hypercholesterolemia outcome in the initial univariate analyses at P⬍0.1 were included in
was defined as total cholesterol ⬎6.2 mmol/L or use of lipid- the multivariate model as candidate variables and then removed by
backward stepwise selection procedure. In the final multivariate
lowering drugs.13 Smoking status was defined as current use. History
analyses, statistical significance was achieved if P⬍0.05. To confirm
of myocardial infarction, angioplasty, coronary artery bypass sur-
the robustness of multivariate models, we repeated all multivariate
gery, and angina pectoris was recorded. A positive history of
analyses using a forward-selection procedure. Associations are present-
coronary artery disease was defined by the presence of any of the ed as hazard ratios (HR) with corresponding 95% confidence intervals
previous conditions. Finally, atrial fibrillation was diagnosed on the (95% CI). The Statistical Package for Social Science (version 10.0 for
basis of at least one ECG before or during hospitalization. Windows; SPSS Inc) was used for statistical analyses.
ABCD Score Results
For the needs of the present study, 2 investigators (G.T. and K.S.) The final studied population consisted of 226 patients hospi-
blinded to the follow-up events retrospectively reviewed both the ER
and hospital records of all 238 patients. The 6-point ABCD score talized with a diagnosis of TIA. The elapsed time from
(age [⬍60 years⫽0, ⱖ60 years⫽1]; BP [systolic ⱕ140 mm Hg and symptom onset to hospital admission was ⬍48 hours in all
diastolic ⱕ90 mm Hg⫽0, systolic ⬎140 mm Hg and/or diastolic cases (87.6% within 24 hours). Demographic characteristics,
⬎90 mm Hg⫽1]; clinical features [unilateral weakness⫽2, speech stroke risk factors, medications before hospitalization, and
disturbance without weakness⫽1, other symptom⫽0]; duration of secondary prevention therapies during hospital stay and after
symptoms [⬍10 minutes⫽0, 10 to 59 minutes⫽1, ⱖ60 min- hospital discharge are presented in Table 1. The distribution
utes⫽2])7 was computed in 231 cases. BP measurements at the ER
were performed using standard mercury sphygmomanometer by the
of the ABCD scores at the time of presentation at the ER is
attending physicians. Clinical features were categorized as motor shown in Table 2. The median length of hospitalization was
weakness (focal, usually unilateral, weakness of one or more of face, 8 days (interquartile range, 7 days). The diagnostic evaluation
arm, hand, or leg) versus speech disturbance (defined as dysarthria or of TIA patients at the ER and during hospital stay included a
dysphasia or both) versus all other symptoms (numbness, change in brain CT scan (100% of cases within 24 hours after presen-
vision, dizziness or vertigo, gait disturbance) according to the OCSP tation to the ER), extracranial Doppler/duplex ultrasonogra-
definition of the ABCD score.7 Seven patients with unavailable BP
recordings (n⫽5) or duration of TIA symptoms (n⫽2) at the ER
phy (96.9%), transthoracic or transesophageal echocardiog-
records were excluded from further evaluation. raphy (38.1%), cerebral magnetic resonance or digital
subtraction angiography (14.6%), and 24-hour heart rate
Patient Outcome monitoring (33.6%). Evidence of cerebral infarction was
All surviving stroke or TIA patients hospitalized in our institution identified on admission CT scan in 31 patients (13.7%),
were followed-up prospectively at 1 month, as previously described.10 whereas ultrasonography disclosed carotid stenosis (ⱖ50%
Follow-up was routinely performed at the outpatient clinics of our reduction in lumen diameter) relevant to the patient’s pres-
department. The outcome events of interest in case of stroke and TIA
enting symptoms in 16 cases (7.1%). Patients with ABCD
patients were recurrent and subsequent strokes respectively, defined
as a cerebrovascular events of sudden onset, lasting for ⬎24 hours, score ⬍5 had fewer (P⬍0.05, Fisher exact test) ischemic
clearly resulting in an increase of an existing or in a new neurological lesions on brain CT scan (10.4%) and less carotid stenoses
deficit.14 They were determined after evaluation of all the available (4.9%) than patients with an ABCD score of 5 to 6 (22.2%
information obtained from our and other hospital records, physi- and 12.7%, respectively). Carotid endarterectomy was per-
cians’ notes in private practice, necropsy findings, or death certifi- formed in 2 patients (12.5%) with symptomatic carotid
cates, and the patients’ clinical presentation at the regular follow-up
disease during the follow-up period.
assessments. Brain imaging visualizing a new lesion involving an
anatomic site or vascular territory that was unaffected on the Within 30 days of the index TIA, 22 (9.7%) patients had a
admission CT scan was mandatory to support the diagnosis of subsequent stroke (18 during hospitalization and 4 after
subsequent stroke in TIA patients. According to the Trial of Org discharge), 16 (7.1%) experienced a recurrent TIA, and 13
10172 in Acute Stroke Treatment (TOAST) criteria, ischemic stroke were dead (n⫽2, 0.9%) or dependent (n⫽11, 4.9%). The
was classified based on etiopathogenetic mechanisms into the subtypes of ischemic stroke (IS) had the following distribu-
following groups: large artery atherosclerotic stroke, cardioembolic
tion: large artery atherosclerotic stroke (45.5%, n⫽10), car-
stroke, small artery occlusion or lacunar infarction, infarction of
other determined origin, and infarction of undetermined cause.14 A dioembolic stroke (13.6%, n⫽3), lacunar infarction (22.7%,
total of 5 patients who were lost from follow-up were excluded from n⫽5), and infarction of undetermined cause (18.2%, n⫽4).
further evaluation. During the follow-up period no hemorrhagic cerebral events
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 20152894 Stroke December 2006
TABLE 1. Baseline Characteristics, Stroke Risk Factors, TIA (ABCD⫽0 to 2: 0%, ABCD⫽3: 3.5% [95% CI, 0% to 8.2%],
Characteristics, and Medications Before and ABCD⫽4: 7.6% [95% CI, 1.2% to 14.0%], ABCD⫽5:
During Hospitalization 21.3% [95% CI, 10.4% to 33.0%], ABCD⫽6: 31.3% [95%
Variable % CI, 8.6% to 54.0%]; log-rank test⫽23.09; df⫽6; P⫽0.0008;
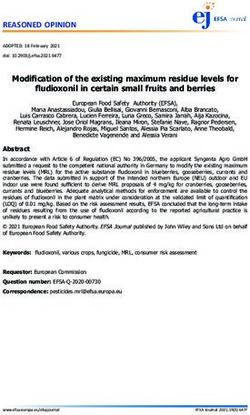
P for linear trend across the ABCD score levels ⬍0.00001)
Baseline characteristics and stroke risk factors
risk of stroke (Table 2). The area under the receiver operating
Mean age (SD, years) 63.9 (12.3)
characteristic curve (Figure 1) was 0.78 (95% CI, 0.69 to
Age ⬎60 years 61.5 0.87; P⬍0.001).
Male 58.8 The association of demographic characteristics, stroke risk
Hypertension 56.6 factors, previous medications, secondary prevention therapies
Diabetes mellitus 25.2 during hospitalization and after discharge, and ABCD score
Hypercholesterolemia 51.3 at the time of presentation at the ER with the risk of
Current smoking 26.1 subsequent stroke was evaluated using univariate Cox pro-
portional hazards analyses. The following variables were
Coronary artery disease 12.8
significantly (P⬍0.1) related to stroke recurrence and were
Atrial fibrillation 11.9
therefore selected for entry into the final multiple-variable
Previous TIAs in the past month 35.4 model: ABCD score ⬎4 (HR, 6.12; 95% CI, 2.49 to 15.02),
TIA characteristics hypercholesterolemia (HR, 4.22; 95% CI, 1.80 to 9.89),
Median duration (IQR, minutes) 50 (227) diabetes mellitus (HR, 3.01; 95% CI, 1.27 to 6.77), arterial
Duration ⬍10 minutes 16.8 hypertension (HR, 2.65; 95% CI, 0.98 to 7.19), lipid-lowering
Duration ⱖ10 minutes and ⬍59 minutes 36.7 medications during hospitalization and/or after discharge
Duration ⱖ60 minutes 46.5 (HR, 0.38; 95% CI, 0.15 to 0.96), and antihypertensive
medications during hospitalization and/or after discharge
Unilateral weakness 46.5
(HR, 0.46; 95% CI, 0.19 to 1.09). The multivariate Cox
Speech disturbance 42.5
regression analyses (performed both with the backward-
Numbness 37.6 selection and forward-selection procedure) revealed only an
Dizziness or vertigo 7.5 ABCD score of 5 to 6, hypercholesterolemia, and diabetes
Gait disturbance 5.8 mellitus as independent predictors of the 30-day risk of stroke
Change in vision 4.4 (Table 3). More specifically, an ABCD score of 5 to 6 at the
Mean systolic BP (SD, mm Hg) 147.0 (27.9) ED was associated (P⬍0.001) with an 8-fold greater 30-day
Systolic BP ⬎140 mm Hg 51.3 risk of stroke (HR, 8.01; 95% CI, 3.21 to 19.98; Figure 2).
Furthermore, an ABCD score of 5 to 6 was also indepen-
Mean diastolic BP (SD, mm Hg) 84.4 (15.1)
dently (P⬍0.001) associated with the 7-day risk of stroke
Diastolic BP ⬎90 mm Hg 33.2
(HR, 8.94; 95% CI, 2.72 to 29.32).
Medications before hospitalization Because evidence for infarction on CT-scans of TIA pa-
Antiplatelet agents 15.9 tients had been associated with an increased risk of subse-
Oral anticoagulants 5.3 quent stroke, we repeated the analyses after including this
Anthypertensive medications 42.0 potential confounder in the multivariable model. An ABCD
Lipid-lowering medications 7.5 score of 5 to 6 remained an independent (P⬍0.001) predictor
Antidiabetic medications 17.3 of the 30-day risk of stroke (HR, 7.31; 95% CI, 2.98 to
17.94). In addition, the exclusion of the TIA patients who
Medications during hospitalization and/or
after discharge experienced a recurrent stroke within 24 hours after hospital
admission (n⫽3), did not attenuate the predictive value of the
Antiplatelet agents 85.4
ABCD score (HR, 12.59; 95% CI, 4.43 to 35.80; P⬍0.001).
Oral anticoagulants 14.6
Finally, we included the patients who were lost during the
Antihypertesnive medications 54.4 follow-up period in our dataset and performed the Cox
Lipid-lowering medications 26.5 regression analyses based on the worst-case scenario (assum-
Antidiabetic medications 21.7 ing that all 5 patients had experienced a subsequent stroke).
LMWH 4.4 The association between ABCD score and risk of stroke
IQR indicates interquartile range; LMWH, low molecular weight heparins. recurrence retained its statistical significance (HR, 4.86; 95%
CI, 2.23 to 10.66; P⬍0.001).
were documented. A total of 3 (1.3%) and 18 (8.0%) stroke
events occurred within 1 and 7 days after hospital admission. Discussion
The ABCD score was highly predictive of both the 7-day The findings of the current hospital-based case series of TIA
(ABCD⫽0 to 2: 0%, ABCD⫽3: 1.7% [95% CI, 0% to 5.1%], patients add to the mounting evidence of an early risk of
ABCD⫽4: 7.6% [95% CI,1.2% to 14.0%], ABCD⫽5: 19.1% subsequent stroke following the index TIA. The rate of IS
[95% CI, 7.8% to 30.4%], ABCD⫽6: 18.8% [95% CI, 0% to during hospitalization in our study (7.9%) was practically
37.9%]; log-rank test⫽17.46; df⫽6; P⫽0.0077; P for linear identical to the in-hospital stroke incidence (8.0%) recorded
trend across the ABCD score levels⫽0.0003) and the 30-day in a multicenter prospective observational study.15 In addi-
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 2015Tsivgoulis et al ABCD Score and Stroke Risk in TIA Patients 2895
TABLE 2. The 7- and 30-Day Risks of Stroke Stratified According to the ABCD Score
7 Days 30 Days
ABCD Score Patients Strokes Risk (%, 95% CI)* Strokes Risk (%, 95% CI)†
0 5 (2.2%) 0 0 0 0
1 12 (5.3%) 0 0 0 0
2 22 (9.7%) 0 0 0 0
3 58 (25.7%) 1 (5.6%) 1.7 (0–5.1) 2 (9.1%) 3.5 (0–8.2)
4 66 (29.2%) 5 (27.8%) 7.6 (1.2–14.0) 5 (22.7%) 7.6 (1.2–14.0)
5 47 (20.8%) 9 (50.0%) 19.1 (7.8–30.4) 10 (45.5%) 21.3 (10.4–33.0)
6 16 (7.1%) 3 (16.7%) 18.8 (0–37.9) 5 (22.7%) 31.3 (8.6–54.0)
Total 226 (100%) 18 (100%) 8.0 (4.5–11.5) 22 (100%) 9.7 (5.8–13.6)
*Log-rank test⫽17.46; df⫽6; P⫽0.0077; P for linear trend across the ABCD score levels⫽0.0003; †Log-rank
test⫽23.09; df⫽6; P⫽0.0008; P for linear trend across the ABCD score levels⬍0.00001.
tion, the 30-day risk of stroke in our cohort was substantially well as in the current hospital-based cases series, underlines
high (9.7%) and only slightly lower to the equivalent risk the high reliability of the score for the prediction of stroke
documented in population-based studies conducted in Ox- risk after a TIA in different clinical settings. In contrast to our
fordshire (11.5%)2 and the greater Cincinnati metropolitan findings, Cucchiara et al after assessing the ABCD score in a
region (11.2%).4 Hence, our data underscore the brief time North American series of hospitalized TIA patients (n⫽117)
window available for stroke prevention in TIA patients and found little predictive value of the ABCD risk score and
emphasize the importance of urgent assessment and effective concluded that its discriminatory capacity was not optimal.16
management in this specific subgroup of patients. Of note, though, is that the outcome chosen in the former
Because TIA patients are a highly heterogeneous group in study was a composite one including stroke, death, ipsilateral
terms of symptoms, risk factors, underlying pathology, and carotid stenosis ⬎50%, or a cardioembolic source warranting
early prognosis, different models for the stratification of coagulation. Notably, only 2 patients experienced a stroke
stroke risk have been recently developed.1,7 Our results event during the 90-day follow-up period and consequently
provide for the first time evidence for the external validity of the risk of stroke was substantially low (⬍2%).
the OCSP-derived ABCD score. More specifically, an ABCD We also documented a higher prevalence of cerebral
score of 5 to 6 was associated with 8-fold greater 30-day risk infarction and ipsilateral carotid stenosis in patients with an
ABCD score of 5 to 6 than in subjects with an ABCD score
of stroke after adjustment for potential confounders including
ⱕ4. Interestingly, evidence of ischemic lesions on baseline
stroke risk factors and secondary prevention therapies. How-
brain CT scan has been previously associated with an adverse
ever, only 7 strokes (4.3%) were documented in the subgroup
outcome in hospitalized TIA patients,15 whereas the early
of patients with an ABCD score ⱕ4. The consistency of the
(90-day) risk of stroke was particularly high (20.1%) in TIA
predictive power of the ABCD score both in a population-
patients with internal carotid artery disease.17
based and hospital-referred clinic cohort of TIA patients,7 as
Given that the ABCD score seems to constitute a valuable
tool able to identify in the ED the subgroup of TIA patients
which is at greatest need for emergent evaluation and effec-
tive treatment, the applicability of the former score in clinical
practice may raise certain potential therapeutic implications.
A recent meta-analysis of individual patient data from ran-
domized control trials of carotid endarterectomy versus med-
ical treatment alone showed that the benefit from surgery was
time-dependent and demonstrated that carotid endarterecto-
my was most effective when performed within 2 weeks from
the qualifying ischemic event (stroke/TIA).18 However, only
12.5% of cases with symptomatic carotid disease underwent
carotid revascularization during the first month after the
TABLE 3. Multivariate Cox Regression Analysis of Predictors
of 30-Day Risk of Stroke
Dependent Variable Comparison HR (95% CI) P
ABCD score 5–6 vs 0–4 8.01 (3.21–19.98) ⬍0.001
Hypercholesterolemia Yes vs no 3.83 (1.47–9.96) 0.006
Figure 1. Receiver operating characteristic curves (ROC) for
Diabetes mellitus Yes vs no 2.98 (1.28–6.94) 0.015
predictive value of ABCD score.
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 20152896 Stroke December 2006
Figure 2. Kaplan-Meier curves of patients sur-
viving free from stroke from time of presenting
TIA stratified according to ABCD score.
index TIA in our cohort, whereas the results of a recent treated within a few minutes of ictus. The results of the German
population-based study are more alarming, because they multicenter hospital-based observational study that had identi-
indicate that carotid surgery was performed within 2 weeks fied admission to stroke unit as a valid predictor for survival and
from TIA/stroke onset in 6% of patients with symptomatic functional independence both in IS and TIA patients,15 lend
carotid stenosis.19 Furthermore, among patients who were support to the former assumption.
enrolled within 1 week in the MATCH (Management of Certain methodological limitations of the present report
ATherothrombosis with Clopidogrel in High-risk patients) should be addressed. First, the ABCD score of the studied
trial, the risk of recurrent stroke appeared to be substantially patients at the time of their presentation at the ER was
(but not significantly because of small numbers) reduced with identified retrospectively from inspection of medical records
combination therapy (clopidogrel plus aspirin) versus clopi- and thus the risk of incomplete case ascertainment cannot be
dogrel alone, compared with the lack of risk reduction in the excluded. Second, we were unable to complete follow-up in
subgroup of patients who were enrolled later.20 The former all patients. However, our additional analyses have already
observation suggests that the risk-benefit ratio of combination addressed this potential shortcoming and indicate that it is
therapy compared with monotherapy may be greatest when unlikely that patients lost to follow-up may have biased the
double antiplatelet therapy is initiated early and continued documented association between the ABCD score and the
only for a short period after the ischemic event. Notably, such risk of stroke. Third, there is accruing evidence confirming
a policy was associated with promising results in the recently that TIA patients with diffusion-weighted imaging ischemic
published CARESS (Clopidogrel and Aspirin for Reduction lesions on MRI are at substantially higher risk of stroke than
of Emboli in Symptomatic Carotid Stenosis) trial.21 those without.26 Because diffusion-weighted brain MRI was
Additionally, in the MIRACL (Myocardial Ischemia Reduc- available in an extremely limited number of patients in our
tion with Acute Cholesterol Lowering trial), statin treatment cohort (5.7%), this potential confounder was not included in
initiated immediately after an unstable angina or a non-Q wave the multivariable Cox-regression model. Fourth, because we
myocardial infarction was associated with a significant reduction evaluated only hospitalized patients, it should be acknowl-
of stroke.22 Because statins seem to reduce the incidence of all edged that the present study validated the ABCD score in a
strokes and the progression of carotid intima-media thickening,23 different cohort of patients from those for which the model
it was postulated that aggressive cholesterol reduction with was intended to be used. More specifically, the ABCD model
statins in patients with recent IS or TIA may decrease stroke was developed in the outpatient setting, to predict risk for all
recurrence. This hypothesis was supported by the shortly pre- TIA patients. Thus, further validation of this score is needed
sented final results of the SPARCL (Stroke Prevention by especially in patients with TIA that were referred to the ED
Aggressive Reduction in Cholesterol Levels) trial.24 Finally, in but not hospitalized.
view of the extremely high (31.3%) early risk of stroke in the In conclusion, the present study validates the predictive
TIA patients of our cohort with an ABCD score of 6, admission value of the ABCD score in identifying hospitalized TIA
of this TIA subgroup to a stroke unit with a ready access to patients with a high risk of early stroke and provides further
immediate thrombolysis in case of subsequent stroke appears to evidence for its potential applicability in clinical practice. Our
be another aggressive albeit potentially effective treatment op- findings advocate the use of the simple and practical ABCD
tion. The substantial benefit of thrombolysis when given within score in the emergency setting to triage TIA patients that may
1 hour of stroke onset25 could be amplified in stroke patients benefit the most from hospital admission, expedited diagnos-
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 2015Tsivgoulis et al ABCD Score and Stroke Risk in TIA Patients 2897
tic evaluation, and early instigation of effective treatment 14. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL,
strategies such as early carotid endarterectomy, close moni- Marsh EE 3rd. Classification of subtype of acute ischemic stroke. Defi-
nitions for use in a multicenter clinical trial. TOAST (Trial of Org 10172
toring in a stroke unit with ready access to thrombolysis, and in Acute Stroke Treatment). Stroke. 1993;24:35– 41.
more aggressive risk factor modification. 15. Daffertshofer M, Mielke O, Pullwitt A, Felsenstein M, Hennerici M.
Transient ischemic attacks are more than “ministrokes”. Stroke. 2004;35:
Disclosures 2453–2458.
16. Cucchiara BL, Messe SR, Taylor RA, Pacelli J, Maus D, Shah Q, Kasner
None.
SE. Is the ABCD score useful for risk stratification of patients with acute
transient ischemic attack? Stroke. 2006;37:1710 –1714.
References 17. Eliasziw M, Kennedy J, Hill MD, Buchan AM, Barnett HJ; North
1. Johnston SC, Gress DR, Browner WS, Sidney S. Short-term prognosis American Symptomatic Carotid Endarterectomy Trial Group. Early risk
after emergency department diagnosis of TIA. JAMA. 2000;284: of stroke after a transient ischemic attack in patients with internal carotid
2901–2906. artery disease. CMAJ. 2004;170:1105–1109.
2. Coull AJ, Lovett JK, Rothwell PM; Oxford Vascular Study. Population 18. Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJ;
based study of early risk of stroke after transient ischaemic attack or Carotid Endarterectomy Trialists Collaboration. Endarterectomy for
minor stroke: implications for public education and organisation of symptomatic carotid stenosis in relation to clinical subgroups and timing
services. BMJ. 2004;328:326 –328. of surgery. Lancet. 2004;363:915–924.
3. Hill MD, Yiannakoulias N, Jeerakathil T, Tu JV, Svenson LW, Schop- 19. Fairhead JF, Mehta Z, Rothwell PM. Population-based study of delays in
flocher DP. The high risk of stroke immediately after transient ischemic carotid imaging and surgery and the risk of recurrent stroke. Neurology.
attack: a population-based study. Neurology. 2004;62:2015–2020. 2005;65:371–375.
4. Kleindorfer D, Panagos P, Pancioli A, Khoury J, Kissela B, Woo D, 20. Diener HC, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste
Schneider A, Alwell K, Jauch E, Miller R, Moomaw C, Shukla R, M, Leys D, Matias-Guiu J, Rupprecht HJ; MATCH investigators. Aspirin
Broderick JP. Incidence and short-term prognosis of transient ischemic and clopidogrel compared with clopidogrel alone after recent ischaemic
attack in a population-based study. Stroke. 2005;36:720 –723. stroke or transient ischaemic attack in high-risk patients (MATCH):
5. Johnston SC, Smith WS. Practice variability in management of transient randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:
ischemic attacks. Eur Neurol. 1999;42:105–108. 331–337.
6. Goldstein LB, Bian J, Samsa GP, Bonito AJ, Lux LJ, Matchar DB New 21. Markus HS, Droste DW, Kaps M, Larrue V, Lees KR, Siebler M,
transient ischemic attack and stroke: outpatient management by primary
Ringelstein EB. Dual antiplatelet therapy with clopidogrel and aspirin in
care physicians. Arch Intern Med. 2000;160:2941–2946.
symptomatic carotid stenosis evaluated using doppler embolic signal
7. Rothwell PM, Giles MF, Flossmann E, Lovelock CE, Redgrave JN,
detection: the Clopidogrel and Aspirin for Reduction of Emboli in Symp-
Warlow CP, Mehta Z. A simple score (ABCD) to identify individuals at
tomatic Carotid Stenosis (CARESS) trial. Circulation. 2005;111:
high early risk of stroke after transient ischaemic attack. Lancet. 2005;
2233–2240.
366:29 –36.
22. Schwartz GG, Olsson AG, Ezekowitz MD, Ganz P, Oliver MF, Waters D,
8. WHO MONICA Project Principal Investigators. The World Health Orga-
Zeiher A, Chaitman BR, Leslie S, Stern T; Myocardial Ischemia
nization MONICA Project (monitoring trends and determinants in car-
diovascular disease): a major international collaboration. J Clin Epi- Reduction with Aggressive Cholesterol Lowering (MIRACL) Study
demiol. 1988;41:105–114. Investigators. Effects of atorvastatin on early recurrent ischemic events in
9. Tsivgoulis G, Vemmos KN, Spengos K, Papamichael CM, Cimboneriu acute coronary syndromes: the MIRACL study: a randomized controlled
A, Zis V, Zakopoulos N, Mavrikakis M. Common carotid artery trial. JAMA. 2001;285:1711–1718.
intima-media thickness for the risk assessment of lacunar infarction 23. Amarenco P, Labreuche J, Lavallee P, Touboul PJ. Statins in stroke
versus intracerebral haemorrhage. J Neurol. 2005;252:1093–1100. prevention and carotid atherosclerosis: systematic review and up-to-date
10. Tsivgoulis G, Spengos K, Zakopoulos N, Manios E, Xinos K, Vassilo- meta-analysis. Stroke. 2004;35:2902–2909.
poulos D, Vemmos KN. Twenty four hour pulse pressure predicts long 24. The SPARCL Investigators. The Stroke Prevention by Aggressive
term recurrence in acute stroke patients. J Neurol Neurosurg Psychiatry. Reduction in Cholesterol Levels (SPARCL) Study. Cerebrovasc Dis.
2005;76:1360 –1365. 2006;21(suppl 4):1.
11. 1999 World Health Organization-International Society of Hypertension 25. Hacke W, Donnan G, Fieschi C, Kaste M, von Kummer R, Broderick JP,
Guidelines for the Management of Hypertension Guidelines Subcom- Brott T, Frankel M, Grotta JC, Haley EC Jr, Kwiatkowski T, Levine SR,
mittee. J Hypertens. 1999;17:151–183. Lewandowski C, Lu M, Lyden P, Marler JR, Patel S, Tilley BC, Albers
12. Expert Committee on the Diagnosis and Classification of Diabetes G, Bluhmki E, Wilhelm M, Hamilton S; ATLANTIS Trials Investigators;
Mellitus. Report of the Expert Committee on the Diagnosis and Classi- ECASS Trials Investigators; NINDS rt-PA Study Group Investigators.
fication of Diabetes Mellitus. Diabetes Care. 1997;20:1183–1197. Association of outcome with early stroke treatment: pooled analysis of
13. Expert Panel on Detection, Evaluation, and Treatment of High Blood ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:
Cholesterol in Adults. Executive Summary of The Third Report of The 768 –774.
National Cholesterol Education Program (NCEP) Expert Panel on 26. Ay H, Koroshetz WJ, Benner T, Vangel MG, Wu O, Schwamm LH,
Detection, Evaluation, And Treatment of High Blood Cholesterol In Sorensen AG. Transient ischemic attack with infarction: a unique
Adults (Adult Treatment Panel III). JAMA. 2001;285:2486 –2497. syndrome? Ann Neurol. 2005;57:679 – 686.
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 2015Validation of the ABCD Score in Identifying Individuals at High Early Risk of Stroke
After a Transient Ischemic Attack: A Hospital-Based Case Series Study
Georgios Tsivgoulis, Konstantinos Spengos, Panagiota Manta, Nikolaos Karandreas, Thomas
Zambelis, Nikolaos Zakopoulos and Demetrios Vassilopoulos
Stroke. 2006;37:2892-2897; originally published online October 19, 2006;
doi: 10.1161/01.STR.0000249007.12256.4a
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2006 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/37/12/2892
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/
Downloaded from http://stroke.ahajournals.org/ by guest on November 7, 2015You can also read