2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Stroke
AHA/ASA GUIDELINE
2022 Guideline for the Management of Patients
With Spontaneous Intracerebral Hemorrhage:
A Guideline From the American Heart
Association/American Stroke Association
Reviewed for evidence-based integrity and endorsed by the American Association of Neurological Surgeons and Congress of
Neurological Surgeons.
Endorsed by the Society of Vascular and Interventional Neurology
The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists.
Endorsed by the Neurocritical Care Society
Steven M. Greenberg, MD, PhD, FAHA, Chair; Wendy C. Ziai, MD, MPH, FAHA, Vice Chair; Charlotte Cordonnier, MD, PhD;
Dar Dowlatshahi, MD, PhD, FAHA; Brandon Francis, MD, MPH; Joshua N. Goldstein, MD, PhD, FAHA;
J. Claude Hemphill III, MD, MAS, FAHA; Ronda Johnson, MBA; Kiffon M. Keigher, MSN, ACNP-BC, RN, SCRN;
William J. Mack, MD, MS, FAHA*; J. Mocco, MD, MS, FAHA†; Eileena J. Newton, MD; Ilana M. Ruff, MD‡;
Lauren H. Sansing, MD, MS, FAHA; Sam Schulman, MD, PhD; Magdy H. Selim, MD, PhD, FAHA; Kevin N. Sheth, MD, FAHA*§;
Nikola Sprigg, MD; Katharina S. Sunnerhagen, MD, PhD; on behalf of the American Heart Association/American Stroke Association
Downloaded from http://ahajournals.org by on May 18, 2022
Key Words: AHA Scientific Statements ◼ cerebral amyloid angiopathy ◼ cerebral hemorrhage ◼ intracranial hemorrhage ◼ prevention
◼ recovery ◼ treatment
TOP 10 TAKE-HOME MESSAGES FOR agents, help to predict the risk of hematoma expan-
sion. These neuroimaging markers include signs
THE MANAGEMENT OF PATIENTS WITH detectable by noncontrast computed tomography,
SPONTANEOUS INTRACEREBRAL the most widely used neuroimaging modality for ICH.
HEMORRHAGE GUIDELINE 3. ICHs, like other forms of stroke, occur as the con-
1. The organization of health care systems is increas- sequence of a defined set of vascular patholo-
ingly recognized as a key component of optimal gies. This guideline emphasizes the importance
stroke care. This guideline recommends develop- of, and approaches to, identifying markers of both
ment of regional systems that provide initial intra- microvascular and macrovascular hemorrhage
cerebral hemorrhage (ICH) care and the capacity, pathogeneses.
when appropriate, for rapid transfer to facilities with 4. When implementing acute blood pressure lowering
neurocritical care and neurosurgical capabilities. after mild to moderate ICH, treatment regimens that
2. Hematoma expansion is associated with worse limit blood pressure variability and achieve smooth,
ICH outcome. There is now a range of neuroimag- sustained blood pressure control appear to reduce
ing markers that, along with clinical markers such as hematoma expansion and yield better functional
time since stroke onset and use of antithrombotic outcome.
*AHA Stroke Council Scientific Statement Oversight Committee on Clinical Practice Guideline liaison. †AANS/CNS liaison. ‡AHA Stroke Council Stroke Performance
Measures Oversight Committee liaison. §AAN representative.
AHA Stroke Council Scientific Statement Oversight Committee members, see page e•••.
Supplemental material is available at https://www.ahajournals.org/doi/suppl/10.1161/STR.0000000000000407
© 2022 American Heart Association, Inc.
Stroke is available at www.ahajournals.org/journal/str
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e1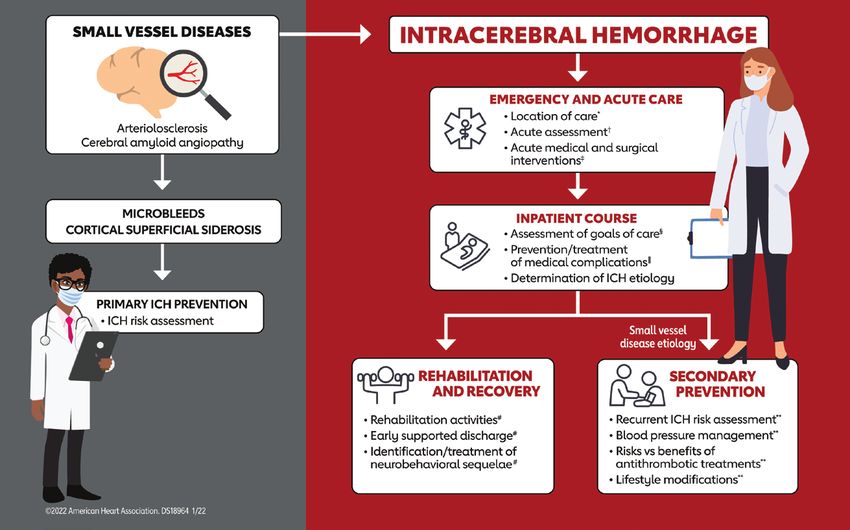
Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
5. ICH while anticoagulated has extremely high inpatient team care with early assessment of dis-
CLINICAL STATEMENTS
mortality and morbidity. This guideline provides charge planning and a goal of early supported dis-
AND GUIDELINES
updated recommendations for acute reversal of charge for mild to moderate ICH. Implementation
anticoagulation after ICH, highlighting use of pro- of rehabilitation activities such as stretching and
tein complex concentrate for reversal of vitamin functional task training may be considered 24 to 48
K antagonists such as warfarin, idarucizumab for hours after moderate ICH; however, early aggres-
reversal of the thrombin inhibitor dabigatran, and sive mobilization within the first 24 hours after ICH
andexanet alfa for reversal of factor Xa inhibitors appears to worsen 14-day mortality. Multiple ran-
such as rivaroxaban, apixaban, and edoxaban. domized trials did not confirm an earlier suggestion
6. Several in-hospital therapies that have histori- that fluoxetine might improve functional recovery
cally been used to treat patients with ICH appear after ICH. Fluoxetine reduced depression in these
to confer either no benefit or harm. For emergency trials but also increased the incidence of fractures.
or critical care treatment of ICH, prophylactic cor- 10. A key and sometimes overlooked member of the
ticosteroids or continuous hyperosmolar therapy ICH care team is the patient’s home caregiver.
appears to have no benefit for outcome, whereas This guideline recommends psychosocial educa-
the use of platelet transfusions outside the setting tion, practical support, and training for the care-
of emergency surgery or severe thrombocytopenia giver to improve the patient’s balance, activity
appears to worsen outcome. Similar considerations level, and overall quality of life.
apply to some prophylactic treatments historically
used to prevent medical complications after ICH.
Use of graduated knee- or thigh-high compres- PREAMBLE
sion stockings alone is not an effective prophylactic Since 1990, the American Heart Association (AHA)/
therapy for prevention of deep vein thrombosis, and American Stroke Association (ASA) has translated sci-
prophylactic antiseizure medications in the absence entific evidence into clinical practice guidelines with rec-
of evidence for seizures do not improve long-term ommendations to improve cerebrovascular health. These
seizure control or functional outcome. guidelines, which are based on systematic methods to
7. Minimally invasive approaches for evacuation of evaluate and classify evidence, provide a foundation for
supratentorial ICHs and intraventricular hemor- the delivery of quality cerebrovascular care. The AHA/
rhages‚ compared with medical management alone‚ ASA sponsors the development and publication of clini-
Downloaded from http://ahajournals.org by on May 18, 2022
have demonstrated reductions in mortality. The clini- cal practice guidelines without commercial support, and
cal trial evidence for improvement of functional out- members volunteer their time to the writing and review
come with these procedures is neutral, however. For efforts.
patients with cerebellar hemorrhage, indications for Clinical practice guidelines for stroke provide recommen-
immediate surgical evacuation with or without an dations applicable to patients with or at risk of developing
external ventricular drain to reduce mortality now cerebrovascular disease. The focus is on medical practice in
include larger volume (>15 mL) in addition to previ- the United States, but many aspects are relevant to patients
ously recommended indications of neurological dete- throughout the world. Although it must be acknowledged
rioration, brainstem compression, and hydrocephalus. that guidelines may be used to inform regulatory or payer
8. The decision of when and how to limit life-sus- decisions, the core intent is to improve quality of care and
taining treatments after ICH remains complex and align with patients’ interests. Guidelines are intended to
highly dependent on individual preference. This define practices meeting the needs of patients in most, but
guideline emphasizes that the decision to assign not all, circumstances and should not replace clinical judg-
do not attempt resuscitation status is entirely dis- ment; furthermore, the recommendations set forth should
tinct from the decision to limit other medical and be considered in the context of individual patient values,
surgical interventions and should not be used to preferences, and associated conditions.
do so. On the other hand, the decision to imple- The AHA/ASA strives to ensure that guideline writing
ment an intervention should be shared between groups contain requisite expertise and are representative of
the physician and patient or surrogate and should the broader medical community by selecting experts from
reflect the patient’s wishes as best as can be dis- a broad array of backgrounds, representing different sexes,
cerned. Baseline severity scales can be useful to races, ethnicities, intellectual perspectives, geographic
provide an overall measure of hemorrhage severity regions, and scopes of clinical practice and by inviting
but should not be used as the sole basis for limiting organizations and professional societies with related inter-
life-sustaining treatments. ests and expertise to participate as endorsers. The AHA/
9. Rehabilitation and recovery are important determi- ASA has rigorous policies and methods for development
nants of ICH outcome and quality of life. This guide- of guidelines that limit bias and prevent improper influence.
line recommends use of coordinated multidisciplinary The complete policy on relationships with industry and
e2 TBD Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407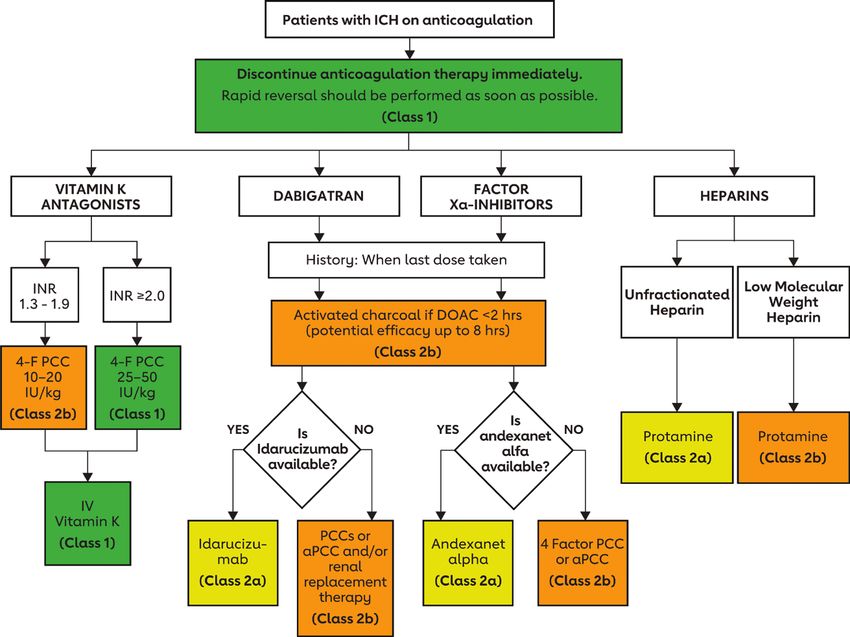
Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
other entities (RWI) can be found at https://professional. the ICH field into practical recommendations for clinical
CLINICAL STATEMENTS
heart.org/-/media/phd-files/guidelines-and-statements/ practice.
AND GUIDELINES
policies-devolopment/aha-asa-disclosure-rwi-policy-5118.
pdf?la=en.
1.1. Methodology and Evidence Review
Beginning in 2017, numerous modifications to AHA/
ASA guidelines have been implemented to make guide- The recommendations listed in this guideline are, when-
lines shorter and enhance user-friendliness. Guidelines ever possible, evidence based and supported by exten-
are written and presented in a modular knowledge chunk sive evidence review. A search for literature derived from
format; each chunk includes a table of recommendations, research principally involving human subjects, published
a brief synopsis, recommendation-specific supportive in English, and indexed in MEDLINE, PubMed, Cochrane
text, and, when appropriate, flow diagrams or additional Library, and other selected databases relevant to this
tables. Hyperlinked references are provided to facilitate guideline was conducted between October 2020 and
quick access and review. Other modifications to the guide- March 2021. Additional trials published between March
lines include the addition of Knowledge Gaps and Future 2021 and November 2021 that affected the content,
Research segments in some sections and a web guideline Class of Recommendation (COR), or Level of Evidence
supplement (Online Data Supplement) for useful but non- (LOE) of a recommendation were included when appro-
critical tables and figures. priate. For specific search terms used‚ readers are
Joseph P. Broderick, MD, FAHA referred to the Online Data Supplement, which contains
Chair, AHA Stroke Council Scientific Statement the final evidence tables summarizing the evidence used
Oversight Committee by the guideline writing group to formulate recommenda-
tions. In addition, the guideline writing group reviewed
documents related to subject matter previously pub-
1. INTRODUCTION lished by the AHA/ASA. References selected and pub-
Approximately 10% of the 795 000 strokes per year in lished in the present document are representative and
the United States are intracerebral hemorrhages (ICHs),1 not all inclusive.
defined by brain injury attributable to acute blood extrav- Each topic area was assigned a primary writer and a pri-
asation into the brain parenchyma from a ruptured cere- mary and sometimes secondary reviewer. Author assign-
bral blood vessel. The clinical impact of ICH appears ments were based on the areas of expertise of the
disproportionately high among lower-resource popu- members of the guideline writing group and their lack of
Downloaded from http://ahajournals.org by on May 18, 2022
lations both in the United States and internationally. In any RWI related to the section material. All recommen-
US-based studies, ICH incidence has been reported to dations were fully reviewed and discussed among the
be ≈1.6-fold greater among Black than White people2 full guideline writing group to allow diverse perspectives
and 1.6-fold greater among Mexican American than non- and considerations for this guideline. Recommendations
Hispanic White people.3 Internationally, ICH incidence is were then voted on, and a modified Delphi process was
substantially higher in low- and middle-income versus used to reach consensus. Guideline writing group mem-
high-income countries, both as a proportion of all strokes bers who had RWI that were relevant to certain recom-
and in absolute incidence rates.4,5 mendations were recused from voting on those particular
Several additional features of ICH make it a greater recommendations. All recommendations in this guideline
public health threat than conveyed by incidence numbers were agreed to by between 88.9% and 100% of the vot-
alone. ICH is arguably the deadliest form of acute stroke, ing guideline writing group members.
with early-term mortality about 30% to 40% and no or
minimal trend toward improvement over more recent
time epochs.6–9 Incidence of ICH increases sharply with 1.2. Organization of the Writing Group
age and is therefore expected to remain substantial as The guideline writing group consisted of vascular neurolo-
the population ages, even with counterbalancing public gists, neurocritical care specialists, neurological surgeons,
health improvements in blood pressure (BP) control.8 an emergency physician, a hematologist, a rehabilitation
Another growing source of ICH is more widespread use medicine physician, a board-certified acute care nurse
of anticoagulants,10 a trend likely to counterbalance the practitioner, a fellow-in-training, and a lay/patient repre-
reduced ICH risk associated with increasing prescription sentative. The writing group included representatives from
of direct oral anticoagulants (DOACs) relative to vitamin the AHA/ASA, the American Association of Neurological
K antagonists (VKAs).11 Surgeons/Congress of Neurological Surgeons, and the
ICH thus remains in need of novel treatments and American Academy of Neurology. Appendix 1 of this doc-
improved application of established approaches for every ument lists guideline writing group members’ relevant RWI
aspect of the disease: primary and secondary preven- and other entities. For the purposes of full transparency,
tion, acute inpatient care, and poststroke rehabilitation the guideline writing group members’ comprehensive dis-
and recovery. This guideline seeks to synthesize data in closure information is available online.
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e3
Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
CLINICAL STATEMENTS
AND GUIDELINES
Figure 1. Guideline overview for primary ICH.
ICH indicates intracerebral hemorrhage. Recommendations on the topics above can be found in the guideline in the sections indicated: *Sections
3 and 5. †Section 4. ‡Sections 5 and 6. §Section 7. ∥Section 5. #Section 8. **Section 9.
Downloaded from http://ahajournals.org by on May 18, 2022
1.3. Document Review and Approval aneurysmal subarachnoid hemorrhage,14 or unruptured
saccular aneurysms.13,15 This guideline does, however,
This document was reviewed by the AHA Stroke Coun-
address imaging approaches to ICH that help differenti-
cil Scientific Statement Oversight Committee, the AHA
ate primary ICH from these secondary causes.
Science Advisory and Coordinating Committee, and the
This guideline aims to cover the full course of primary
AHA Executive Committee; reviewers from the Ameri-
ICH (Figure 1), from the location and organization of emer-
can Academy of Neurology, the Society of Vascular
gency care (Section 3), initial diagnosis and assessment
and Interventional Neurology, and the American Asso-
(Section 4), and acute medical and surgical interventions
ciation of Neurological Surgeons/Congress of Neuro-
(Sections 5.1, 5.2, and 6) to further inpatient care of post-
logical Surgeons; and 53 individual content reviewers.
ICH complications (Sections 5.3–5.5), goals of care assess-
Appendix 2 lists reviewers’ comprehensive disclosure
ment (Section 7), rehabilitation and recovery (Section 8), and
information.
secondary prevention of recurrent ICH (Section 9). Because
of the substantial differences in pathogenesis and course
1.4. Scope of the Guideline between ICH and ischemic stroke, the writing group sought,
This guideline addresses the diagnosis, treatment, and when possible, to base its recommendations on data derived
prevention of ICH in adults and is intended to update specifically from ICH patient groups. Some aspects of inpa-
and replace the AHA/ASA 2015 ICH guideline.12 This tient medical care and post-ICH rehabilitation are likely
2022 guideline is limited explicitly to spontaneous ICHs to be similar between patients with ICH and patients with
that are not caused by head trauma and do not have a ischemic stroke, however. Readers are therefore referred to
visualized structural cause such as vascular malforma- relevant AHA/ASA guidelines and scientific statements for
tion, saccular aneurysm, or hemorrhage-prone neoplasm. ischemic stroke in these overlapping areas.16,17 Table 1 is a
These hemorrhages without a demonstrated structural list of associated AHA/ASA guidelines and scientific state-
or traumatic cause are often referred to as primary ICH ments that may be of interest to the reader.
(see further comment on this terminology in Section 2.1, Another area where this ICH guideline interfaces with
Small Vessel Disease Types). This guideline thus does prior ischemic stroke guidelines is the challenging area
not overlap with AHA/ASA guidelines or scientific state- of antithrombotic agent use in patients after ICH who
ments on the treatment of arteriovenous malformations,13 are at risk for both recurrent ICH and ischemic stroke
e4 TBD Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
Table 1. Associated AHA/ASA Guidelines and Statements
CLINICAL STATEMENTS
Publication
AND GUIDELINES
Title Organization year
AHA/ASA guidelines
2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From AHA/ASA 2021
the American Heart Association/American Stroke Association
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, ACC/AHA/AAPA/ 2017
Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/ ABC/ACPM/AGS/
American Heart Association Task Force on Clinical Practice Guidelines APhA/ASH/ASPC/
NMA/PCNA
uidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals From the Ameri-
G AHA/ASA 2016
can Heart Association/American Stroke Association
Guidelines for the Management of Patients With Unruptured Intracranial Aneurysms: A Guideline for Healthcare AHA/ASA 2015
Professionals From the American Heart Association/American Stroke Association
Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals AHA/ASA 2015
From the American Heart Association/American Stroke Association
Guidelines for the Primary Prevention of Stroke: A Statement for Healthcare Professionals From the American Heart AHA/ASA 2014
Association/American Stroke Association
Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage: A Guideline for Healthcare Professionals AHA/ASA 2012
From the American Heart Association/American Stroke Association
AHA/ASA scientific statements
Care of the Patient With Acute Ischemic Stroke (Prehospital and Acute Phase of Care): Update to the 2009 Compre- AHA/ASA 2021
hensive Nursing Care Scientific Statement: A Scientific Statement From the American Heart Association
Management of Brain Arteriovenous Malformations: A Scientific Statement for Healthcare Professionals From the AHA/ASA 2017
American Heart Association/American Stroke Association
Prevention of Stroke in Patients With Silent Cerebrovascular Disease: A Scientific Statement for Healthcare Profes- AHA/ASA 2017
sionals From the American Heart Association/American Stroke Association
Palliative and End-of-Life Care in Stroke: A Statement for Healthcare Professionals From the American Heart Associa- AHA/ASA 2014
tion/American Stroke Association
AAPA indicates American Association of Physician Assistants; ABC, Association of Black Cardiologists; ACC, American College of Cardiology; ACPM, American
Downloaded from http://ahajournals.org by on May 18, 2022
College of Preventive Medicine; AGS, American Geriatrics Society; AHA, American Heart Association; APhA, American Pharmacists Association; ASA, American Stroke
Association; ASH, American Society of Hypertension; ASPC, American Society for Preventive Cardiology; NMA, National Medical Association; and PCNA, Preventive
Cardiovascular Nurses Association.
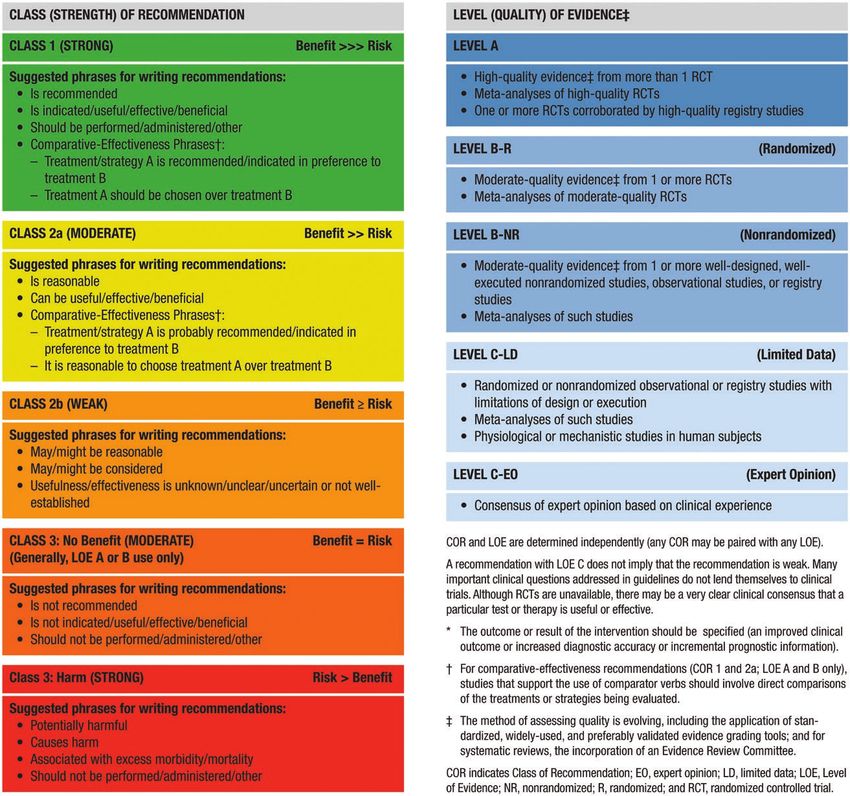
(Section 9.1.3, Management of Antithrombotic Agents). 1.5. COR and LOE
This guideline does not attempt to reassess the extensive
Recommendations are designated with both a COR and
literature on assessment of future ischemic stroke risk
an LOE. The COR indicates the strength of recommen-
and instead refers the reader to existing AHA guidelines
dation, encompassing the estimated magnitude and cer-
on primary and secondary ischemic stroke prevention.18,19
tainty of benefit in proportion to risk. The LOE rates the
This ICH guideline has a new section on assess-
quality of scientific evidence supporting the intervention
ment of ICH risk in individuals with no prior ICH but with
on the basis of the type, quantity, and consistency of data
neuroimaging findings such as cerebral microbleeds or
from clinical trials and other sources (Table 2).
cortical superficial siderosis suggestive of a hemorrhage-
prone microvasculopathy. This topic, which was also pre-
viously discussed in an AHA scientific statement on the Abbreviations
wider area of silent cerebrovascular disease,20 does not
fall strictly under the heading of ICH management. This Abbreviation Meaning/Phrase
guideline writing group nonetheless included the section ADL activities of daily living
(9.2, Primary ICH Prevention in Individuals With High-Risk AF atrial fibrillation
Imaging Findings) because of its close relationship to the AHA American Heart Association
considerations used for secondary prevention of recurrent aPCC activated prothrombin complex concentrate
ICH (Section 9.1, Secondary Prevention) and the high fre- ASA American Stroke Association
quency with which these small hemorrhagic lesions are
ATACH-2 Antihypertensive Treatment of Acute Cerebral Hemorrhage II
detected as incidental findings on magnetic resonance
AVERT A Very Early Rehabilitation Trial
imaging (MRI) performed for other indications. Evidence
BP blood pressure
on how to interpret and act on incidental hemorrhagic
lesions remains limited but is likely to grow with the wide- CAA cerebral amyloid angiopathy
spread incorporation of blood-sensitive MRI methods into CLEAR III Clot Lysis: Evaluating Accelerated Resolution of Intraven-
tricular Hemorrhage Phase III
research studies and clinical practice.
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e5Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
Abbreviation Meaning/Phrase Abbreviation Meaning/Phrase
CLINICAL STATEMENTS
CLOTS Clots in Legs or Stockings After Stroke PCC prothrombin complex concentrate
AND GUIDELINES
COR Class of Recommendation PE pulmonary embolism
CPP cerebral perfusion pressure PREVAIL Evaluation of the WATCHMAN Left Atrial Appendage
[LAA] Closure Device in Patients With Atrial Fibrillation
CT computed tomography
Versus Long Term Warfarin Therapy
CTA computed tomography angiography
PRoFESS Prevention Regimen for Effectively Avoiding Second
DBP diastolic blood pressure Strokes
DIAGRAM Diagnostic Angiography to Find Vascular Malformations PROGRESS Perindopril Protection Against Recurrent Stroke Study
DNAR do not attempt resuscitation PROTECT-AF WATCHMAN Left Atrial Appendage System for Embolic
Protection in Patients With Atrial Fibrillation
DOAC direct oral anticoagulant
QASC Quality in Acute Stroke Care
DSA digital subtraction angiography
RCT randomized controlled trial
DVT deep vein thrombosis
RRT renal replacement therapy
ED emergency department
RWI relationships with industry and other entities
EIBPL early intensive blood pressure lowering
SAE serious adverse event
EMS emergency medical services
SBP systolic blood pressure
ERICH Ethnic/Racial Variations of Intracerebral Hemorrhage
SPARCL Stroke Prevention by Aggressive Reduction in Cholesterol
EVD external ventricular drain/drainage
Levels
FFP fresh-frozen plasma
SSRIs selective serotonin reuptake inhibitors
4-F PCC 4-factor prothrombin complex concentrate
STICH Surgical Trial in Intracerebral Hemorrhage
GCS Glasgow Coma Scale
TBI traumatic brain injury
HE hematoma expansion
TXA tranexamic acid
HR hazard ratio
UFH unfractionated heparin
ICH intracerebral hemorrhage
VKA vitamin K antagonist
ICP intracranial pressure
VTE venous thromboembolism
ICU intensive care unit
INCH International Normalized Ratio (INR) Normalization in
Downloaded from http://ahajournals.org by on May 18, 2022
Coumadin Associated Intracerebral Hemorrhage 2. GENERAL CONCEPTS
INR international normalized ratio
2.1. Small Vessel Disease Types
INTERACT2 The Second Intensive Blood Pressure Reduction in Acute
Cerebral Hemorrhage Trial Despite our use of the term primary ICH to distinguish
IPC intermittent pneumatic compression from ICH with a demonstrated structural cause (Section
IVC inferior vena cava
1.4, Scope of the Guideline), these seemingly spontaneous
IVH intraventricular hemorrhage
hemorrhages are not truly primary but rather represent the
consequence of defined underlying (and often co-occurring)
IVT intraventricular thrombolysis
vascular pathologies. The 2 common cerebral small vessel
LMWH low-molecular-weight heparin
pathologies that account for the overwhelming majority
LOE Level of Evidence of primary ICH are arteriolosclerosis and cerebral amyloid
LOS length of stay angiopathy (CAA). Each is a common age-related pathol-
LVAD left ventricular assist device ogy, appearing at autopsy at moderate to severe extents in
MIS minimally invasive surgery 30% to 35% of individuals enrolled in a longitudinal study of
MISTIE III Minimally Invasive Surgery Plus rt-PA for Intracerebral aging.21 Arteriolosclerosis (also referred to as lipohyalinosis)
Hemorrhage Evacuation is detected as concentric hyalinized vascular wall thicken-
MRA magnetic resonance angiography ing favoring the penetrating arterioles of the basal ganglia,
MRI magnetic resonance imaging thalamus, brainstem, and deep cerebellar nuclei (collectively
mRS modified Rankin Scale referred to as deep territories). Its major associated risk fac-
MSU mobile stroke unit
tors are hypertension, diabetes, and age. CAA is defined by
NCCT noncontrast computed tomography
deposition primarily of the β-amyloid peptide in the walls
of arterioles and capillaries in the leptomeninges, cerebral
ND neurological deterioration
cortex, and cerebellar hemispheres (lobar territories). The
NICE-SUGAR Normoglycemia in Intensive Care Evaluation and Survival
Using Glucose Algorithm Regulation
primary risk factors for CAA are age and apolipoprotein E
genotypes containing the ε2 or ε4 alleles.
NIHSS National Institutes of Health Stroke Scale
ICH occurs in a relatively small subset of those brains
NSAID nonsteroidal anti-inflammatory drug
with advanced arteriolosclerosis or CAA, typically in deep
OR odds ratio
territories for arteriolosclerosis and lobar territories for CAA,
e6 TBD Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
Table 2. Applying Class of Recommendation and Level of Evidence to Clinical Strategies, Interventions, Treatments, or Diag-
nostic Testing in Patient Care (Updated May 2019)*
CLINICAL STATEMENTS
AND GUIDELINES
Downloaded from http://ahajournals.org by on May 18, 2022
the brain locations favored by the underlying pathologies. of ICH.25 It is important to note, however, that the small
Small, often asymptomatic cerebral microbleeds in these vessel pathologies that underlie ICH are also associated
compartments are substantially more common, occurring with increased risk of ischemic stroke,26 highlighting the
in >20% of population-based individuals >60 years of age complexity and importance of balancing the risks versus
scanned with sensitive T2*-weighted MRI methods.22,23 The benefits of antithrombotic treatment. Among the cerebral
presence of multiple strictly lobar ICHs, microbleeds, or cor- small vessel diseases, CAA inferred by the Boston crite-
tical superficial siderosis (chronic blood products over the ria appears to confer substantially greater risk for recur-
cerebral subpial surface) has been pathologically validated rent hemorrhage than arteriolosclerosis (recurrent ICH
as part of the Boston criteria to detect CAA-related hem- rates in a pooled analysis of 7.39%/y after CAA-related
orrhage with reasonably high specificity and sensitivity.24 ICH versus 1.11%/y after non–CAA-related ICH).27
Microbleeds associated with arteriolosclerosis tend to occur
in deep territories but can appear in lobar territories as well.
The underlying small vessel types of ICH have several 2.2. Mechanisms for ICH-Related Brain Injury
practical implications for the formulation of ICH guide- ICH is understood to injure surrounding brain tissue
lines. They establish a hemorrhage-prone environment in through the direct pressure effects of an acutely expand-
which use of antithrombotic agents creates increased risk ing mass lesion and through secondary physiological
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e7Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
and cellular pathways triggered by the hematoma and its Recommendations for Organization of Prehospital and Initial Systems
CLINICAL STATEMENTS
metabolized blood products.28 Direct pressure effects can of Care (Continued)
AND GUIDELINES
include both local compression of immediately surrounding COR LOE Recommendations
brain tissue and more widespread mechanical injury caused 2. In patients with sudden onset of neurological
by increased intracranial pressure (ICP), hydrocephalus, or symptoms or signs attributable to potential
spontaneous ICH, use of stroke recogni-
herniation. Early HE, possibly driven by mechanical shearing
tion and severity tools is recommended for
of surrounding vessels by the initial hematoma,29 is common 1 B-R
dispatch personnel and first responders to
and a consistent predictor of worse ICH outcome.30 identify potential stroke and facilitate rapid
transport to reduce time to diagnosis and
Secondary physiological and cellular injury mecha-
treatment.36–41
nisms postulated to be triggered by ICH include cere-
3. In patients with stroke symptoms attributable
bral edema, inflammation, and biochemical toxicity of to potential spontaneous ICH, immediate
blood products such as hemoglobin, iron, and thrombin.28 1 B-NR activation of the emergency response system
Although it is plausible that the underlying small vessel (9-1-1 in North America) is recommended to
reduce time to diagnosis and treatment.32,42
disease type may affect the mechanism and severity
4. In patients with potential spontaneous ICH,
of ICH-related brain injury, there is currently no strong early notification by emergency medical ser-
evidence for substantial differences between the acute 1 B-NR vices (EMS) staff to the receiving hospital is
course of arteriolosclerosis-related and CAA-related ICH recommended to improve time to diagnosis
and treatment.43,44
other than differences attributable to ICH location.
Several of the major medical therapies for ICH such as BP 5. In patients with spontaneous ICH, regional
systems of stroke care are recommended
lowering and reversal of anticoagulation are aimed at limiting so all potentially beneficial therapies can
HE. The search for effective medical treatments for protect- be made available when appropriate as
ing tissue from secondary post-ICH injury, like the search for rapidly as possible‚ including, at minimum,
1 C-LD
(a) health care facilities that provide initial
effective neuroprotectants for ischemic stroke, has to date spontaneous ICH care, including diagnosis
been unsuccessful. Surgical hematoma evacuation through and treatment, and (b) health care facilities
craniotomy, minimally invasive approaches, or ventriculostomy with neurocritical care and neurosurgical
capabilities.45
is aimed at both preventing further pressure-related injury
6. In patients with potential stroke, including
and protecting against secondary physiological and cellu- spontaneous ICH, in geographic regions
lar injury. One complexity that arises in the interpretation of where mobile stroke units (MSUs) operate,
results of surgical ICH trials is the possibility that mortality 2a B-R such mobile units are reasonable to enable
Downloaded from http://ahajournals.org by on May 18, 2022
more rapid diagnosis and treatment than
might be prevented without improvement in functional out- achievable by ambulance transfer to the clos-
come, an issue addressed explicitly in the current guidelines. est stroke-capable facility.46,47
7. In patients with potential spontaneous ICH,
first responder training in stroke evaluation
2.3. Limits to Generalizability 2a C-LD
and care with the ability to provide airway and
circulatory support when necessary is reason-
A key limitation that runs through all sections of this able to detect and manage prehospital neuro-
guideline is that much of the data come from high- logical deterioration (ND).48,49
resource countries and from more affluent demographic
groups within those countries. The potential limitations Synopsis
of generalizability to lower-resource settings and popu- Much of the data for prehospital care and stroke sys-
lations noted to be disproportionately at risk of ICH tems of care are derived from studies of stroke of
(Section 1, Introduction), highlight the need for future all types (including ICH). Furthermore, it is generally
guidelines based explicitly on data from these under- not possible for prehospital clinicians to distinguish
served and underrepresented groups. between patients with ICH and those with other types
of stroke. As a result, the recommendations for pre-
hospital care of patients with hemorrhagic stroke are
3. ORGANIZATION OF PREHOSPITAL AND essentially identical to those recommended for any
INITIAL SYSTEMS OF CARE patient with stroke: early recognition, expedient trans-
port to the most appropriate facility, and prenotification
Recommendations for Organization of Prehospital and Initial Systems
of Care before hospital arrival to expedite the in-hospital stroke
Referenced studies that support recommendations are summarized in response. Although it can be difficult to measure the
Data Supplements 1 through 12.
precise time to onset of ICH treatment, it is reason-
COR LOE Recommendations able to infer that earlier diagnosis will be closely linked
1. In patients with stroke, including spontaneous to earlier treatment. To facilitate rapid diagnosis and
ICH, design and implementation of stroke
public education programs for diverse popula-
treatment of ICH, we recommend public health mea-
1 B-R sures to educate the public, build and maintain orga-
tions focused on early recognition and the
need to seek emergency care rapidly is useful nized systems of care, and ensure appropriate training
to reduce time to diagnosis and treatment.31–35
of first responders.
e8 TBD Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
Recommendation-Specific Supportive Text associated with earlier emergency department
CLINICAL STATEMENTS
(ED) arrival (adjusted odds ratio [OR], 2.00 [95%
1. Early symptom recognition is essential for timely ICH
AND GUIDELINES
CI, 1.93–2.08]), quicker ED evaluation (adjusted
care. In the United States, ≈67% of adults know the OR, 1.89 [95% CI, 1.78–2.00]), and more rapid
signs and symptoms of stroke and the need to call treatment for ischemic stroke (adjusted OR, 1.44
EMS; stroke knowledge increased almost 15 per- [95% CI, 1.28–1.63]).32,42 For ICH specifically, a
centage points between 2009 and 2017.33 Public large multicenter cohort study found that time from
education campaigns can improve stroke knowl- symptom onset to ED was 63 minutes versus 227
edge,35,50 increase the use of EMS for stroke,31 and minutes in patients who used EMS versus those
use of EMS is associated with shorter time to diag- who did not use EMS, and time to hospital admis-
nosis.32 In the largest cluster randomized controlled sion was 167 minutes versus 537 minutes.55 Thus,
study of >75 000 subjects, an educational inter- persistent efforts to ensure activation of the 9-1-1
vention reduced time to hospital arrival in women or a similar emergency system by patients or other
(median, 328 minutes versus 559 minutes) but not members of the public for suspected stroke are
men.34 Although some smaller studies have dem- warranted.
onstrated modest benefits, others have shown no 4. Many observational studies in patients with stroke
or only transient benefits.51–54 Knowledge of stroke (including both ischemic and ICH) have found that
warning signs varies by race, sex, ethnicity, age, edu- use of prehospital notification to the destination ED
cation, and urbanicity,33 which may contribute to dis- is associated with faster time to neuroimaging and
parities in outcomes. Public education campaigns shorter time to alteplase in ischemic stroke.56–59 For
should make every attempt to address underserved example, a large registry found that after adjustment
groups and those with the largest opportunities to for covariates, EMS use (with prenotification) was
improve awareness. associated with faster door-to-CT times than both
2. No existing clinical decision scale can differenti- private transport and EMS without prenotification.44
ate ICH from other diseases with high sensitiv- In the AHA Get With The Guidelines–Stroke registry,
ity or specificity in the absence of neuroimaging. EMS personnel provided prearrival notification to the
Prehospital scales such as FAST (Face, Arm, Speech, destination ED for 67% of transported patients with
Time to call 911), LAPSS (Los Angeles Prehospital stroke.43 EMS prenotification was associated with
Stroke Scale), CPSS (Cincinnati Prehospital Stroke shorter door-to-imaging times and shorter symptom
Downloaded from http://ahajournals.org by on May 18, 2022
Scale), and ROSIER (Recognition of Stroke in the onset–to–needle times. One group found that for
Emergency Room) are available and typically are ICH, early stroke team activation was associated
validated in all stroke rather than ICH specifically.41 with faster door-to-CT times (24 minutes versus 48
Differences include whether they focus on sensitiv- minutes) and faster time to hemostatic medication
ity or specificity and whether they screen for stroke when used (63 minutes versus 99 minutes).60
severity as well as presence. For dispatch, a group 5. Many regions have developed stroke systems of
found that a specific dispatch stroke assessment care and stratify hospitals according to their ability
tool was associated with shorter time to diagno- to deliver intravenous thrombolytics or endovascular
sis,37 and a clinical trial found that a dispatch stroke therapy for ischemic stroke. Triage algorithms sug-
screen reduced time to both hospital arrival and gest routing patients on the basis of the results of
stroke unit admission (although only 5% had ICH).36 prehospital stroke severity scales. These scales
One group analyzed ICH specifically39 and found an often indicate high severity in the case of ICH, which
association between documented stroke scale use would direct patients with potential ICH preferen-
and ICH recognition. The sensitivity for ICH was tially to advanced stroke centers such as a com-
84%, and stroke scale documentation was indepen- prehensive stroke center. Whether patients with
dently associated with ICH recognition and shorter ICH benefit from the higher level of care versus
door–to–computed tomography (CT) times (20 earlier temporizing at regional facilities remains to
minutes versus 47 minutes). Most studies of stroke be seen and should be studied. One observational
scale use in practice inadequately account for false- study found that Canadian provinces that had imple-
negative cases, thereby likely artificially boosting mented stroke systems of care had reduced mortal-
performance. One group developed a clinical predic- ity for the entire cohort (including ICH, ≈10% of the
tion rule to classify stroke subtypes, including ICH, cohort; adjusted incidence rate ratios, 0.85 [95% CI,
in the prehospital setting; however, neither the sen- 0.79–0.92]).45
sitivity nor positive predictive value was published.40 6. Most studies of MSUs have focused on time to
3. One group found that in a large national cohort thrombolysis for stroke, and subgroup analyses of
of patients with stroke, EMS use compared with those diagnosed with ICH are small and underpow-
arrival to hospital by other means is independently ered. One group randomized their geographic region
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e9Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
to weeks on/off for MSU availability and found that life support yields better ICH outcomes. Data on
CLINICAL STATEMENTS
those patients treated in MSUs had faster times the impact of MSUs on ICH are also limited.
AND GUIDELINES
from symptom onset to laboratory results and to • Much of the data for prehospital care and stroke
CT.47 No MSU diagnosis of ICH (or lack of ICH) systems of care were derived from studies of sus-
required revision during follow-up. Another study in pected stroke (including ICH), diagnosed stroke of
2 regions of Germany found similar reductions in all types (including ICH), or ischemic stroke. As a
time to CT.46 The MSU reduced the use of interfa- result, the recommendations for prehospital care are
cility transfer to zero for ICH because those with typically based on those for ischemic stroke or all
ICH were taken to a comprehensive stroke cen- strokes. Future research should evaluate whether
ter as the initial hospital. Forty-one percent of the particular systems of care are specifically beneficial
MSU patient group and none of the standard care to ICH, as well as the impact of regionalized large
group received BP management in the field after vessel occlusion stroke care on ICH outcomes and
diagnosis, suggesting that MSU led to earlier initia- the impact of EMS bypass of primary stroke centers
tion of treatment. Issues of logistics, feasibility, and for suspicion of large vessel occlusion.
cost currently appear to restrict MSU use to certain • Existing tools to stratify or diagnose ICH in the pre-
regions and facilities, and all studies are currently hospital setting are limited. It remains unclear which,
underpowered to evaluate any association with if any, tool is best or whether stroke scales that incor-
clinical outcome after ICH. porate severity, rather than just stroke presence,
7. No clinical trials of different EMS response strategies are useful for ICH prehospital assessment. Further
were found to have been conducted in ICH. Some study of test characteristics of existing stroke sever-
have been published in traumatic brain injury (TBI). ity scores in identifying patients with ICH is needed,
One large clinical trial of TBI found that in patients whether the destination of patients with potential ICH
with Glasgow Coma Scale (GCS) scoreGreenberg et al 2022 Guideline for the Management of Spontaneous ICH
Table 3. Initial History, Physical Examination and Laboratory Workup in Patients With ICH
CLINICAL STATEMENTS
Assessment type Comments
AND GUIDELINES
History
Time of symptom onset (or time patient was last normal)
Symptoms Headache
Thunderclap: Aneurysm, RCVS, some instances of CVST
Slower onset: Mass lesion, some instances of CVST, ischemic stroke with hemorrhagic
transformation
Focal neurologic deficits
Seizures
Decreased level of consciousness
Vascular risk factors Ischemic stroke
Prior ICH
Hypertension (Section 9.1.2)
Hyperlipidemia
Diabetes
Metabolic syndrome
Imaging biomarkers (eg, cerebral microbleeds; Section 9.1.1)
Medications Antithrombotics:
Anticoagulants (Section 5.2.1), thrombolytics, antiplatelet agents (Section 5.2.2), NSAIDs
(9.1.4), dose and time of last ingestion
Vasoconstrictive agents (associated with RCVS):
Triptans, SSRIs (Section 8.2), decongestants, stimulants, phentermine, sympathomimetic
drugs
Antihypertensives (as a marker of chronic hypertension)
Estrogen-containing oral contraceptives (hemorrhage attributable to CVST)
Cognitive impairment or dementia Associated with (but not specific for) amyloid angiopathy
Substance use (Section 9.1.5) Smoking
Alcohol use
Downloaded from http://ahajournals.org by on May 18, 2022
Marijuana (associated with RCVS)
Sympathomimetic drugs (amphetamines, methamphetamines, cocaine)
Liver disease, uremia, malignancy, and hematologic disorders May be associated with coagulopathy
Physical examination
Vital signs Including assessment of airway, breathing, circulation
A general physical examination focusing on the head, heart,
lungs, abdomen, and extremities
A focused neurological examination A structured examination (such as the NIHSS) can be completed in minutes and provides a
quantification that allows easy communication of the severity of the event to other caregivers.
GCS is relevant to patients with impaired level of consciousness.
Serum and urine tests
Complete blood count, blood urea nitrogen and creatinine, Anemia is associated with poor outcomes and hemorrhagic expansion.73,74
liver function tests, glucose, inflammatory markers (ESR and/ Thrombocytopenia is associated with increased mortality.75
or CRP)
Acute kidney injury and hyperglycemia are associated with worse outcomes and mortality.68–71,76–81
Inflammatory markers are associated with infective endocarditis.82
GFR influences clearance of DOACs.83
Prothrombin time (with INR) and an activated partial thrombo- Anticoagulant-related hemorrhages are associated with an increased hematoma volume,
plastin time, specific tests for DOACs when appropriate greater volume and time interval of expansion, and increased morbidity and mortality.84–86
Specific tests for DOACs (including dilute thrombin time, anti-Xa activity) may be useful for
considering reanticoagulation.87
Cardiac-specific troponin and ECG Elevated troponin levels are associated with increased mortality. Signs of left ventricular hyper-
trophy and other abnormalities on ECG can identify chronic hypertension, myocardial ischemia,
or prior cardiac injury.
Urine toxicology screen Cocaine and other sympathomimetic drugs are associated with ICH.
Pregnancy test in a woman of childbearing age Peripartum angiopathy, eclampsia, HELLP syndrome, and sinus venous thrombosis can cause
ICH in pregnant women.
CRP indicates C-reactive protein; CVST, cerebral venous sinus thrombosis; DOAC, direct oral anticoagulant; ECG, electrocardiogram; ESR, erythrocyte sedimenta-
tion rate; GCS, Glasgow Coma Scale; GFR, glomerular filtration rate; HELLP, hemolysis, elevated liver enzymes, and low platelets; ICH, intracerebral hemorrhage; INR,
international normalized ratio; NIHSS, National Institutes of Health Stroke Scale; NSAID, nonsteroidal anti-inflammatory drug; RCVS, reversible cerebral vasoconstriction
syndrome; and SSRI, selective serotonin reuptake inhibitor.
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e11Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
complete blood count and coagulation profile can help of DOAC medications, these studies are not reliable
CLINICAL STATEMENTS
to diagnose coagulopathy attributable to medications enough to determine the level of anticoagulation at
AND GUIDELINES
or underlying medical conditions such as hematologic the time of presentation with DOAC-related ICH.
malignancies.72 This could lead to targeted therapies that Specific factor Xa inhibition levels have been devel-
can improve outcome. For surgical patients, coagulation oped for the factor Xa inhibitors and thrombin-based
status is important to determine whether external ven- assays for dabigatran, but these studies are not
tricular drainage (EVD) or craniotomy can be performed widely available and often are not able to be run in
safely. Electrolyte disturbances, renal dysfunction, and an emergency setting quickly enough for decision-
acute cardiac syndromes can confound the clinical making. Specific reliable measurements of these
picture and require treatments that should be initiated anticoagulants could determine which patients may
urgently on hospital arrival. benefit from reversal of anticoagulation.
• Viscoelastic hemostatic assays, including throm-
Recommendation-Specific Supportive Text
boelastography and rotational thromboelastog-
1. Complete blood count and coagulopathy studies
raphy, allow measurement of both cellular and
(prothrombin time/partial thromboplastin time/INR)
plasma components of clot formation and fibri-
can help determine hemorrhage type, including
nolysis, unlike traditional coagulation tests (pro-
spontaneous ICH attributable to extreme thrombo-
thrombin time/partial thromboplastin time/INR)
cytopenia (eg, plateletsGreenberg et al 2022 Guideline for the Management of Spontaneous ICH
Recommendations for Neuroimaging for ICH Diagnosis and Acute a baseline CT within 3 hours of ICH onset and a
CLINICAL STATEMENTS
Course (Continued) repeat CT at 1 and 20 hours after baseline scan
AND GUIDELINES
COR LOE Recommendations found that substantial HE occurred in 26% of
4. In patients with spontaneous ICH, CT angiog- patients on the 1-hour scans and in an additional
2b B-NR
raphy (CTA) within the first few hours of ICH 12% of patients on the 20-hour scans.97 HE was
onset may be reasonable to identify patients
associated with ND. In another study, the frequency
at risk for subsequent HE.103–108
of HE was greatest among those who underwent
5. In patients with spontaneous ICH, using non-
contrast computed tomography (NCCT) mark-
the initial CT scan within 3 hours of ICH onset and
2b B-NR
ers of HE to identify patients at risk for HE progressively declined as the time to initial scan
may be reasonable.106 was prolonged; 15% of patients exhibited HE
Synopsis between 6 and 12 hours and 6% between 12 and
24 hours. HE after 24 hours was extremely rare
Brain imaging is essential to distinguish ICH from isch- (0%).98 However, delayed IVH has been reported in
emic stroke and determine ICH volume (often estimated 21% of patients with no initial IVH, and infrequently
in practice with the ABC/2 formula109). CT is the most beyond 24 hours,99 delayed IVH is more likely to
widely used imaging modality to confirm (or rule out) the be associated with delayed HE, is independently
presence of ICH because of its widespread availability, associated with mortality and poor outcomes, and
rapidity, high diagnostic accuracy, and ease. However, often requires emergency surgical intervention.
MRI with echo-planar gradient echo or susceptibility- Incorporating new IVH appearance and IVH expan-
weighted sequences also can detect hyperacute ICH sion into the definition of HE appears to improve
with high accuracy.94,95,110 Brain imaging during the prediction of poor neurological outcome.113,114 In
acute phase of ICH can provide prognostic information patients with ICH with stable examination and pre-
and aid in monitoring the evolution of ICH. HE tends to served level of consciousness, follow-up CT scans
occur early after ICH (typically within 24 hours of ICH at ≈6 and 24 hours after onset appear adequate to
onset) and is associated with poor outcome and mortal- exclude HE and document final ICH volume.
ity.30,97,98,111 Identification of a spot sign on CTA or con- 3. This recommendation pertains to indications for
trast-enhanced CT104,107,108 or certain imaging features repeat imaging to detect other downstream effects
on NCCT such as heterogeneous densities within the of recent hemorrhage that may occur beyond
hematoma or irregularities at its margins106,112 may help the first 24-hour period. Evidence derived from
Downloaded from http://ahajournals.org by on May 18, 2022
to identify patients at risk for HE. These markers could patients with mild TBI, defined as a GCS score
influence the triage, monitoring intensity, and outcome ≥13, suggested that routine repeat head CT in
prognostication for such patients. Repeating the CT neurologically stable patients is of low yield and
after the initial scan to evaluate for development of HE, often unnecessary,100,115 whereas other evidence
hydrocephalus, or perihematomal edema can be useful, indicated that routine serial neuroimaging may
particularly in patients whose neurological status deterio- have some value in patients with moderate or
rates and in those with impaired level of consciousness severe TBI.101 However, these studies included few
in whom examination is limited. subjects with ICH (most patients had subarach-
Recommendation-Specific Supportive Text noid, subdural, or epidural hemorrhages), and the
1. A prospective, multicenter, observational study of physiological differences between traumatic and
62 patients presenting within 6 hours of sponta- nontraumatic hemorrhage limit the generalizabil-
neous ICH reported that the sensitivity, specificity, ity of these data to primary ICH. A single-center
predictive value, and accuracy of detecting ICH on observational study in 239 patients with spontane-
MRI by experienced readers were 100%.94 A simi- ous ICH admitted to a neurological intensive care
lar study in 200 patients in which MRI was done unit (ICU) with a standardized order set, including
first followed by CT found that MRI and CT were serial CT at 6, 24, and 48 hours and hourly neuro-
equivalent for detecting acute ICH and that MRI logical assessments, found that 35% of patients
was more accurate for detecting chronic ICH.95 required emergency neurosurgical interventions
A prospective, single-center study in patients after admission; 46% were instigated by imaging
with spontaneous ICH reported that MRI was findings versus 54% by a change in neurologi-
slightly more sensitive than CT for detecting small cal examination,102 suggesting that routine serial
IVH‚ where MRI sensitivity was 100% compared imaging might be of supplemental value to neu-
with 97% for CT.96 rological assessments. Beyond the first 24 hours,
2. HE occurs early after ICH and is an independent serial imaging is generally guided by the clinical
predictor of ND, mortality, and poor functional picture of the patient.
outcome.30,111 A prospective, observational study 4. Although benefits of therapies that target HE have cur-
in 103 patients with spontaneous ICH who had rently not been demonstrated, stratification of patients
Stroke. 2022;53:00–00. DOI: 10.1161/STR.0000000000000407 TBD e13Greenberg et al 2022 Guideline for the Management of Spontaneous ICH
at risk of HE can influence the triage and intensity appealing, particularly in low-resource settings where
CLINICAL STATEMENTS
of monitoring of these patients and their prognosis. A immediate performance and interpretation of CTA
AND GUIDELINES
prospective, multicenter, observational study reported are challenging. However, the prognostic yield and
that HE was more frequent in patients with a CTA- clinical relevance of these NCCT signs and scores
positive spot sign than in those without it, although the are yet to be adequately examined in prospective
negative and positive predictive values of the spot sign large studies. An important goal of future research is
were not robust.104 Mortality and poor modified Rankin to refine the utility of NCCT signs (defined by stan-
Scale (mRS) score at 90 days were greater in patients dardized criteria) and HE scores to maximize their
with CTA-positive spot sign. Subsequent meta-analy- diagnostic and predictive capabilities and validity.
ses106–108 also suggested that CTA-positive spot sign
can predict HE and mortality, although interpretation 4.2. Diagnostic Assessment for ICH
of these analyses is limited by high heterogeneity of
Pathogenesis
the included studies. A meta-analysis of individual data
Recommendations for Diagnostic Assessment for ICH Pathogenesis
from 5435 patients reported that the addition of the Referenced studies that support recommendations are summarized in
spot sign provided small improvement in the discrimi- Data Supplement 15.
nation of an HE prediction model composed of simple COR LOE Recommendations
clinical variables (ICH volume, time from ICH onset to 1. In patients with lobar spontaneous ICH and
imaging, and use of antithrombotic drugs).103 The sen- ageYou can also read