Scottish Stroke Improvement Programme - 2019 report - NSS Information and Intelligence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NSS Information and Intelligence
Scottish Stroke
Improvement
Programme
2019 report.
© NHS National Services Scotland/Crown Copyright 2019 Brief extracts from this publication may be reproduced provided the source is fully acknowledged. Proposals for reproduction of large extracts should be addressed to: PHI Digital Support Information Services Division NHS National Services Scotland Gyle Square 1 South Gyle Crescent Edinburgh EH12 9EB phone: +44 (0)131 275 6233 email: NSS.PHIgraphics@nhs.net Designed and typeset by PHI Digital Support Translation Service If you would like this leaflet in a different language, large print or Braille (English only), or would like information on how it can be translated into your community language, please phone 0845 310 9900 quoting reference 287407.

2019 National Report - Scottish Stroke Improvement Programme
Contents
Introduction.......................................................................................................................... ii
1 Scottish Stroke Improvement Programme.................................................................. 1
2 Scottish Ambulance Service Stroke Improvement Plan............................................. 5
3 Inpatients........................................................................................................................ 6
4 Outpatients................................................................................................................... 18
Summary and key findings relating to outpatient data.................................................. 18
5 Atrial Fibrillation........................................................................................................... 23
6 Thrombolysis and Thrombectomy.............................................................................. 25
Emergency treatments to unblock arteries causing ischaemic stroke........................... 25
Thrombolysis.................................................................................................................. 25
Thrombectomy............................................................................................................... 30
7 Carotid Intervention..................................................................................................... 31
8 Rehabilitation................................................................................................................ 35
9 Outcomes after admission with stroke...................................................................... 36
10 Using SSCA data for research.................................................................................... 40
11 Where Next?................................................................................................................. 41
List of References............................................................................................................. 42
Appendix A: Responses from Chief Executives............................................................. 43
NHS Ayrshire & Arran..................................................................................................... 43
NHS Borders.................................................................................................................. 44
NHS Dumfries & Galloway............................................................................................. 44
NHS Fife......................................................................................................................... 45
NHS Forth Valley ........................................................................................................... 46
NHS Grampian............................................................................................................... 47
NHS Greater Glasgow & Clyde...................................................................................... 48
NHS Highland................................................................................................................. 48
NHS Lanarkshire............................................................................................................ 49
NHS Lothian................................................................................................................... 50
NHS Orkney................................................................................................................... 51
NHS Shetland................................................................................................................. 51
NHS Tayside................................................................................................................... 52
NHS Western Isles......................................................................................................... 52
Appendix B: List of Tables and Charts............................................................................ 54
Appendix C: Stroke Improvement Plan Priorities & Actions RAG................................. 56
Appendix D: Additional Information................................................................................. 63
Acknowledgements........................................................................................................ 63
i2019 National Report - Scottish Stroke Improvement Programme
Introduction
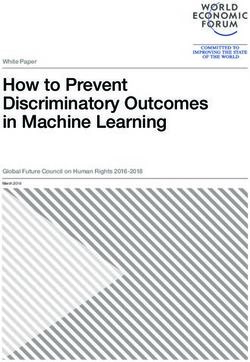
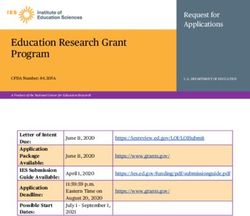
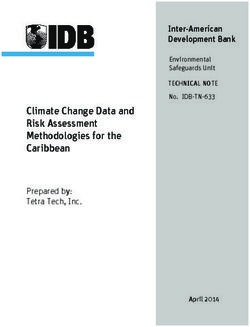
Map of Scotland showing all hospitals in NHS boards contributing to the
Scottish Stroke Care Audit
Gilbert Bain
Hospital
NHS
Shetland
Balfour Hospital
Raigmore Hospital
Belford Hospital NHS
Orkney
Caithness Hospital
Lorn and Islands Hospital
Western Isles Hospital
Uist & Barra Hospital
NHS
Western Isles
Aberdeen Royal Infirmary
Dr Gray’s, Elgin
NHS
NHS Grampian
Highland
Ninewells Hospital Dundee
Perth Royal Infirmary
Stracathro Hospital
Queen Margaret Hospital
NHS
Tayside
Victoria Hospital,
Kirkcaldy
Forth Valley Royal Hospital
Stirling Community Hospital NHS
Royal Infirmary of Edinburgh
Falkirk Community Hospital Fife
NHS
Forth Valley
St Johns Hospital Livingston
Western General Hospital
NHS
NHS Lothian
Queen Elizabeth University Hospital Greater Glasgow
and Clyde
Glasgow Royal Infirmary NHS
Lanarkshire
Stobhill Hospital
Royal Alexandra Hospital NHS
NHS
Borders
Vale of Leven Hospital Ayrshire Borders General
and Arran
Inverclyde Royal Hospital Hospital
NHS
University Hospital Ayr Dumfries
and Galloway
University Hospital Crosshouse
University Hospital Hairmyres
University Hospital Monklands
Dumfries and Galloway Royal Infirmary University Hospital Wishaw
Galloway Community Hospital
ii2019 National Report - Scottish Stroke Improvement Programme
This year the report continues to move in the direction of online only reporting, which will produce a
more interactive experience. As always, feedback on the layout and content of the Scottish Stroke
Improvement Programme (SSIP) Annual Report would be much appreciated.
Stroke is a key health issue for the people of Scotland and the Scottish NHS. It is the third commonest
cause of death in Scotland and the most common cause of severe physical disability amongst
Scottish adults. Over nine and a half thousand stroke patients were admitted to Scottish hospitals in
2018. A further thousand stroke cases were seen at neurovascular (TIA) clinics and many cases may
never present to medical attention. Stroke has a significant impact on NHS resources, accounting for
approximately 5% of total NHS costs2. Societal costs are even higher. The economic cost of stroke to
Scotland in terms of lost employment and the cost of support in the community are significant, whilst
the impact on family members or friends who care for stroke survivors is massive. For these reasons it is
important that all NHS boards across Scotland deliver high quality and equitable stroke care.
Table 1.1: Numbers of confirmed stroke patients by NHS Board of Residence, showing
percentage by age, sex, stroke type, case mix and deprivation category, 2018
data (final diagnosis).
Confirmed Crude rate Mean Age Mean Age Males Ischaemic Case Mix Scottish Index of Multiple Deprivation
NHS board of Residence Strokes per 100,000 Males Females Strokes
admitted residents (years) (years) Independent Lived alone Can talk Orientated to Can lift both Can walk SIMD 1 SIMD 2 SIMD 3 SIMD 4 SIMD 5
during 2018 in Activities at normal at first time, place arms off the without help (Most (Least
of Daily place of assessment? and person bed at first from another deprived) deprived)
Living? residence? at first assessment? person?
assessment?
Percentage of Confirmed Strokes
Total 9 641 178 71 76 51 87 83 37 74 64 60 42 24 22 19 18 15
Ayrshire & Arran 856 232 70 75 50 88 79 36 67 63 68 46 34 24 18 13 12
Borders 191 166 74 77 53 86 83 32 74 54 71 66 8 16 30 40 6
Dumfries & Galloway 244 164 74 78 52 84 84 39 70 65 57 32 12 26 38 20 4
Fife 865 233 71 76 51 90 82 38 81 65 69 47 23 25 22 15 16
Forth Valley 502 164 72 76 56 87 93 37 78 63 41 39 20 30 17 19 14
Grampian 820 140 73 76 53 84 85 35 66 64 57 32 6 16 20 30 27
Greater Glasgow & Clyde 2 062 175 69 74 51 89 80 38 73 64 62 50 45 18 11 11 14
Highland 509 158 72 76 52 85 84 37 69 67 54 44 8 23 30 30 9
Lanarkshire 1 097 166 70 75 52 90 81 34 75 65 55 44 30 30 19 13 8
Lothian 1 398 156 71 77 48 83 83 39 80 60 65 33 14 24 17 17 28
Orkney 35 158 74 75 51 80 86 29 71 63 51 37 0 37 26 31 6
Shetland 34 148 67 80 65 71 88 29 65 35 53 24 0 6 29 65 0
Tayside 717 172 71 77 52 82 89 35 82 76 49 34 18 18 23 27 15
Western Isles 42 157 68 80 45 79 69 43 62 43 31 21 0 38 57 5 0
Outside Scotland/ 269 - 69 75 56 88 88 27 71 71 55 42 - - - - -
Not Known/ Other
Notes regarding Table 1.1:
1 NHS board of residence derived from postcode. A small proportion of records cannot be assigned to specific NHS boards because of
insufficient information (e.g. part postcode) or because patient was a non-Scottish resident.
2 Some patients may not be treated within their resident NHS board and may travel to other NHS boards for treatment.
3 The column ‘Confirmed strokes’ excludes a small proportion of records for in-hospital wake-up strokes (where the patient was already in
hospital for other reasons and had a stroke during their hospital stay but with doubt about whether they woke from sleep with symptoms of
stroke).
4 For further information on the Scottish Index of Multiple Deprivation (SIMD) see the Scottish Government web site at http://www.gov.scot/
Topics/Statistics/SIMD and http://www.gov.scot/Resource/0050/00504809.pdf.
Table 1.1 provides information on stroke admissions across Scotland including details on age, stroke
type, deprivation and other case mix factors.
Table 3.1 describes the provision of stroke unit beds across Scotland. The vast majority of patients are
managed in integrated stroke units which provide both acute care and rehabilitation. In the developed
world many areas have developed comprehensive stroke centres (centres that deliver all aspects of
stroke care, including stroke thrombectomy). Currently there are no comprehensive stroke centres in
Scotland.
iii2019 National Report - Scottish Stroke Improvement Programme
The Scottish Stroke Care Audit (SSCA) has been collecting information about stroke care since 2002.
Since its inception the SSCA has helped to drive evidence-based improvements in stroke care which
have contributed to falling mortality rates and improved outcomes for Scottish stroke patients. The
SSCA has moved its focus more towards service improvement and safety over the last few years. As
improvements in performance against most of the Scottish Stroke Care Standards have occurred across
Scotland, the focus has moved towards measuring stroke care ‘bundles’. Instead of measuring how an
individual fares against any one stroke standard, bundles measure how that individual fares against all
relevant Scottish Stroke Care Standards. Achieving this care bundle is associated with reduced mortality
and increased likelihood of discharge to usual residence after stroke10.
Across Scotland Stroke Bundle compliance has improved from 65% in 2017 to 68% in 2018. This is
some way short of the 80% standard. The majority of NHS boards have seen improvement over this
time, with both Tayside and Dumfries and Galloway making statistically significant gains. However,
performance in NHS Highland continues to give rise to concern. With a change in the CT Standard
beginning from the start of 2019, it will be challenging to maintain or even improve on Bundle
performance in next year’s report.
The numbers of patients being thrombolysed has now stabilised at around 13% of all ischaemic stroke
admission. Unfortunately improvements in door to needle times against the 30 and 60 minute standards
have stalled over the last 12 months, emphasizing the need for more work here in preparation for the
development of a thrombectomy services in Scotland.
iv2019 National Report - Scottish Stroke Improvement Programme
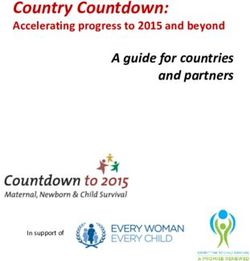
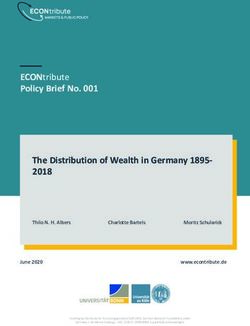
Chart 1.1: (Health Board) Percentage of stroke patients receiving an ‘appropriate’ Stroke
Care Bundle (i.e. Stroke Unit admission, swallow screen, brain scan and
aspirin), 2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2016) of 80% of stroke patients to receive the appropriate elements of the stroke care
bundle (i.e. Stroke Unit admission, swallow screen, brain scan and aspirin).
100
90
80
2017 (%)
70
2018 (%)
statistically
60 significant
improvement
% 50
2018 (%)
no statistically
40 significant
change
30
2018 (%)
statistically
20 significant
decline
10
Stroke Standard
(2016)
0
Lothian
Galloway
Highland
Scotland
Orkney
Fife
Borders
Tayside
Shetland
& Clyde
Forth Valley
Ayrshire & Arran
Western Isles
Grampian
Lanarkshire
Greater Glasgow
Dumfries &
Notes regarding Chart 1.1:
1. A ‘bundle’ involves a group of specific interventions/ processes of care that significantly improve patient outcome if done together
rather than separately and this also improves the consistency with which patients are managed.
The Stroke Care Bundle involves four components: admission to a Stroke Unit, swallow screen, brain scan and aspirin. Not all patients are
eligible for all four components. An aspirin allergy, for example, would preclude the prescribing of aspirin, so the term ‘appropriate’ refers to
patients receiving the components for which they were eligible. A flow chart in section 1 of this report describes the different categories of
bundle depending on patients’ eligibility.
For the specific components, exclusions are as follows: (1) Stroke Unit admission excludes patients with in-hospital strokes, patients
transferred in from another acute hospital or patients discharged within 1 day of admission to hospital (2) aspirin excludes patients with valid
contraindications to aspirin and also those receiving a ‘non-stroke’ final diagnosis who are discharged within 1 day of admission to hospital.
In measuring the proportion of patients receiving an ‘appropriate’ bundle, patients ineligible for, and therefore not receiving, specific
components of the bundle are counted as having received their appropriate bundle provided they received the remaining components for
which they were eligible.
2. Due to the number of beds within some hospitals indicated and the small numbers of stroke admissions to these hospitals it is not
practical to have a defined Stroke Unit. We have confirmed however that a defined stroke pathway is in place in these hospitals and that
the Scottish Stroke Care Standard criteria are established within that pathway.
3. Uist & Barra Hospital, NHS Western Isles does not have a CT scanner but patients are airlifted to Western Isles Hospital and a
proportion may arrive in sufficient time to have brain imaging within 24 hours of admission.
4. During 2017 NHS Dumfries & Galloway opened the new Dumfries & Galloway Royal Infirmary.
v2019 National Report - Scottish Stroke Improvement Programme
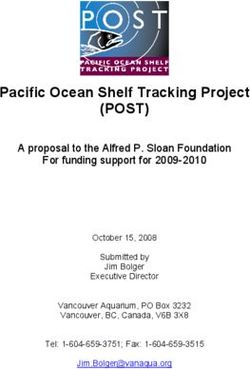
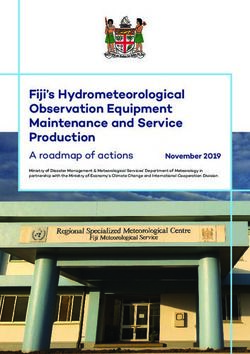
Chart 1.2: (Hospital) Percentage of stroke patients receiving an ‘appropriate’ Stroke
Care Bundle (i.e. Stroke Unit admission, swallow screen, brain scan and
aspirin), 2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2016) of 80% of stroke patients to receive the appropriate elements of the stroke care
bundle (i.e. Stroke Unit admission, swallow screen, brain scan and aspirin).
100
90
80
2017 (%)
70
2018 (%)
60 statistically
significant
improvement
% 50
2018 (%)
no statistically
40 significant
change
30
2018 (%)
statistically
20 significant
decline
10
Stroke Standard
(2016)
0
Scotland
GCH*
Crosshouse
IRH
Hairmyres
Western Isles
GRI
ARI
Monklands
SJH
Ninewells
Borders
Caithness*
Gilbert Bain*
Wishaw
QUEH
FVRH
Dr Grays
RIE
PRI
DGRI
Belford*
RAH
L&I
Raigmore
WGH
Balfour
Ayr
VHK
Notes regarding Chart 1.2:
1. A ‘bundle’ involves a group of specific interventions/ processes of care that significantly improve patient outcome if done together
rather than separately and this also improves the consistency with which patients are managed.
The Stroke Care Bundle involves four components: admission to a Stroke Unit, swallow screen, brain scan and aspirin. Not all patients are
eligible for all four components. An aspirin allergy, for example, would preclude the prescribing of aspirin, so the term ‘appropriate’ refers to
patients receiving the components for which they were eligible. A flow chart in section 1 of this report describes the different categories of
bundle depending on patients’ eligibility.
For the specific components, exclusions are as follows: (1) Stroke Unit admission excludes patients with in-hospital strokes, patients
transferred in from another acute hospital or patients discharged within 1 day of admission to hospital (2) aspirin excludes patients with valid
contraindications to aspirin and also those receiving a ‘non-stroke’ final diagnosis who are discharged within 1 day of admission to hospital.
In measuring the proportion of patients receiving an ‘appropriate’ bundle, patients ineligible for, and therefore not receiving, specific
components of the bundle are counted as having received their appropriate bundle provided they received the remaining components for
which they were eligible.
2. Due to the number of beds within some hospitals indicated (*) and the small numbers of stroke admissions to these hospitals it is not
practical to have a defined Stroke Unit. We have confirmed however that a defined stroke pathway is in place in these hospitals and that
the Scottish Stroke Care Standard criteria are established within that pathway.
3. Uist & Barra Hospital, NHS Western Isles does not have a CT scanner but patients are airlifted to Western Isles Hospital and a
proportion may arrive in sufficient time to have brain imaging within 24 hours of admission.
4. During 2017 NHS Dumfries & Galloway opened the new Dumfries & Galloway Royal Infirmary.
5. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
vi2019 National Report - Scottish Stroke Improvement Programme
1 Scottish Stroke Improvement Programme
The NHS Scotland Quality Strategy1 is the NHS Scotland
Blueprint for improving the quality of care that patients and
carers receive from the NHS across Scotland. It sets out
an ambition for health care that is person centred, safe and
effective, underpinned by the need to “embed the mutual
approach of shared rights and responsibilities into every
interaction between patients, their families and those providing
health services.” The Scottish Stroke Improvement Programme
(SSIP) works with stroke Managed Clinical Networks (MCNs)/
NHS boards to focus on building capacity for all staff to ensure
that they have the knowledge, skills and attitudes necessary to
deliver high quality services. Stroke remains the third biggest
killer in Scotland and the leading cause of disability. Further
reducing the number of deaths from stroke has been a clinical
priority for NHS Scotland since the mid 1990s. Scotland
continues to have exceptionally high levels of stroke related
deaths compared to the rest of Western Europe. The SSIP has
set out ambitions to deliver world-leading stroke care which
is consistently person-centred, clinically effective and safe.
One of the key factors for success is that there is commitment
to patient safety and, in particular, to avoiding infection and harm, using consistent and reliable
improvement methods. One of the triple aims of the 2020 vision2 is to further improve the quality of care
provided, with one of the focuses being to improve the approach to supporting and treating people with
stroke.
To improve services effectively the SSIP recognises the need to set clear aims which have been
established through the Scottish Stroke Care Standards (2016) and the priority actions from the Stroke
Improvement Plan4. Through the Scottish Stroke Care Audit (SSCA) and the regular monitoring against
the priority actions, performance is mapped and the Stroke MCNs develop action plans, test change and
implement improvement methodologies. The Stroke Improvement Programme Lead and SSCA National
Clinical Coordinator work closely with the NHS boards to ensure the key priorities from the Improvement
Plan and the Scottish Stroke Care Standards are implemented and monitored. However, it is ultimately
the responsibility of each NHS board’s Chief Executive to ensure that services improve
Scottish Stroke Care Standards Implemented 1st April 2016
(Following review of Scottish Stroke Care Standards 2013)
Topic Standard
Access to Stroke Unit 90% within 1 day of admission (Day 0 and 1).
Brain imaging 95% within 24 hours of admission.
Swallow screen 100% within 4 hours of arrival at hospital
Aspirin administration 95% of ischaemic strokes within 1 day of admission (Days 0 and 1).
Delay from receipt of referral to 80% are assessed within 4 days of receipt of referral (Day 0 being day of receipt of referral).
specialist stroke/TIA clinic
Thrombolysis 50% of patients receive the bolus within 30 mins of arrival.
80% of patients receive the bolus within one hour of arrival.
Carotid Intervention 80% undergoing carotid endarterectomy for symptomatic carotid stenosis have the operation within 14
days of the event that first led them to seek medical assistance.
12019 National Report - Scottish Stroke Improvement Programme
The national standards are recommended by the SSCA steering group and ratified by the National
Advisory Committee for Stroke. The standards should not be used to guide the care of individual
patients since there may be very legitimate reasons for NOT treating a patient according to the standard.
The standards are used to assess the performance of stroke services, at a Scotland wide, NHS board or
individual hospital level, not at the level of the individual patients.
The standards are set at a level which aims to be both challenging but potentially achievable by some
hospitals. This is done to encourage improvements in performance. Once a standard is routinely
exceeded by all hospitals then it is likely that the SSCA group will recommend that the standard is
raised, or if already at an ideal level, it may actually be removed from the audit. It is therefore inevitable
that many stroke services will not meet some of the standards. Stroke services need to use appropriate
Quality Improvement methods to optimise their own performance. The audit aims to focus its resources
on those areas where improvement will enhance patient outcomes and experience.
The following table represents the self evaluated performance of NHS boards when benchmarking
themselves against the Stroke Improvement Plan priorities, displayed in Red, Amber, Green (RAG), Blue
or Black with further detailed information in Appendix C.
Generic key for RAG chart and RAG status pages 3 and 4:
Complete and embedded in practice
Implemented but not delivered consistently
Plan to implement or partially implemented
Available but not implemented
No process or pathway in place
22019 National Report - Scottish Stroke Improvement Programme
NHS Board Priority Area / Action
1.1 1.2 2.1 2.3 3 4 5.1 5.2
Public FAST Early Scottish Thrombolysis Stroke Bundle Trained Early Diagnosis: Early Diagnosis:
campaign identification of Ambulance Process & Delivery: Workforce: TIA Access TIA Imaging
stroke by SAS/ Service (SAS) Pathway Intermittent Education
Primary Care/ Pre-Alert Pneumatic Template &
Emergency Dept Compression Training
Ayrshire and
GREEN GREEN GREEN GREEN GREEN GREEN BLUE BLUE
Arran
Borders GREEN GREEN GREEN AMBER GREEN GREEN AMBER BLUE
Dumfries and
GREEN GREEN GREEN AMBER GREEN GREEN GREEN GREEN
Galloway
Fife BLUE GREEN AMBER AMBER GREEN GREEN AMBER AMBER
Forth Valley AMBER AMBER AMBER AMBER GREEN GREEN GREEN GREEN
Grampian BLUE GREEN AMBER GREEN GREEN GREEN BLUE BLUE
Greater Glasgow
GREEN GREEN AMBER AMBER GREEN GREEN AMBER RED
and Clyde
Highland GREEN GREEN AMBER AMBER GREEN GREEN AMBER AMBER
Lanarkshire BLUE BLUE AMBER GREEN GREEN BLUE AMBER AMBER
Lothian GREEN GREEN GREEN GREEN GREEN GREEN BLUE BLUE
Orkney GREEN AMBER GREEN GREEN GREEN AMBER BLUE GREEN
Shetland BLUE GREEN GREEN AMBER GREEN GREEN AMBER AMBER
Tayside GREEN GREEN GREEN AMBER GREEN GREEN AMBER AMBER
Western Isles BLUE GREEN AMBER GREEN GREEN GREEN AMBER AMBER
32019 National Report - Scottish Stroke Improvement Programme
NHS Board Priority Area / Action
6 7.1.1 7.1.2 7.2 7.3.1 7.3.2 7.3.3 8.1 8.2 8.3 8.4
Secondary Transition to Transition to Transition Transition to Transition to Transition to Living with Living with Living Living
Prevention: Community: Community: to Commu- Community: Community: Community: Stroke: Self Stroke: with with
Anticoagula- Access Access nity: Goal Specialist Access to Specialist Manage- Access to Stroke: Stroke:
tion for AF to Stroke to Stroke Setting Visual Specialist Driving ment sup- Exercise Access to Stroke
Therapy Rehabilitation Assessment Clinical Neuro- Assessment port after support after vocational Spasticity
Services and psychological discharge discharge rehabilita- Manage-
Rehabilitation Services tion ment
Ayrshire and
AMBER GREEN AMBER AMBER BLUE AMBER BLUE GREEN BLUE GREEN AMBER
Arran
Borders AMBER GREEN AMBER GREEN BLUE RED BLUE AMBER AMBER AMBER GREEN
Dumfries and
AMBER BLUE AMBER AMBER BLUE GREEN BLUE GREEN AMBER GREEN AMBER
Galloway
Fife GREEN AMBER GREEN GREEN GREEN AMBER GREEN GREEN BLUE BLUE AMBER
Forth Valley AMBER GREEN GREEN AMBER BLUE RED BLUE AMBER GREEN AMBER GREEN
Grampian AMBER AMBER AMBER AMBER BLUE AMBER BLUE GREEN GREEN AMBER GREEN
Greater Glasgow
AMBER GREEN GREEN GREEN BLUE AMBER GREEN GREEN BLUE AMBER AMBER
and Clyde
Highland AMBER AMBER AMBER GREEN GREEN AMBER BLUE BLUE BLUE AMBER GREEN
Lanarkshire AMBER GREEN GREEN AMBER BLUE GREEN BLUE BLUE BLUE BLUE BLUE
Lothian RED AMBER AMBER BLUE AMBER GREEN BLUE GREEN GREEN GREEN GREEN
Orkney AMBER AMBER GREEN BLUE BLUE BLUE BLUE AMBER GREEN BLUE GREEN
Shetland BLUE AMBER AMBER BLUE RED RED AMBER GREEN BLUE BLUE GREEN
Tayside GREEN AMBER AMBER GREEN GREEN GREEN GREEN GREEN BLUE AMBER AMBER
Western Isles GREEN GREEN AMBER GREEN GREEN AMBER GREEN AMBER GREEN AMBER AMBER
Clearly there is variability across the country and NHS boards should strive to improve access to high
quality services to ensure the best treatment and support is available to people living with stroke.
42019 National Report - Scottish Stroke Improvement Programme
2 Scottish Ambulance Service Stroke
Improvement Plan
The Scottish Ambulance Service triaged 3,643 suspected Hyper Acute Stroke patients of which the
Service achieved a median 96.3% compliance rate with the pre-hospital stroke bundle.
The pre-hospital stroke bundle ensures that ambulance clinicians across the country are meeting at a
minimum, set clinical quality indicators in all occurrences of suspected hyper acute stroke.
The Scottish Ambulance Service is divided into three distinct regional areas, North, East and West which
traverses the fourteen health boards across Scotland. Each region is facilitated with a clinical manager
with co-responsibility for stroke alongside a Clinical Lead and Associate Medical Director within the
National Clinical Directorate.
Health Board Locality/Council Ward Number of Suspected Hyper % of Pre-hospital Median time from resource
area of incident Acute Strokes Stroke Bundle compliance allocation to ED admission
(mins)
Ayrshire and Arran 274 95.3 51
Borders 85 97.6 65
Dumfries and Galloway 113 93.8 54
Fife 362 96.7 44
Forth Valley 189 93.1 51
Grampian 383 97.4 57
Greater Glasgow & Clyde 718 95.8 47
Grampian 216 94.9 71
Lanarkshire 349 96.6 49
Lothian 630 98.1 50
Orkney 7 100.0 70
Shetland 12 100.0 40
Tayside 256 94.0 51
Western Isles 16 100.0 68
Note 33 incidents are unrecorded against a geographical health board.
The patient numbers represented in the table are patients who present with signs and symptoms of
stroke and are deemed to be suitable for thrombolysis screening in the most appropriate and nearest
emergency department. These patients in our care have not had a CT scan at this stage and it is
therefore only possible to make an informed ‘working diagnosis’ of hyper acute stroke based on the
history available to them of the immediate event and the presenting ‘condition’ of the patient.
Not all of these patients will therefore be included in the Scottish Stroke Care Audit as following a CT
scan and assessment by a stroke physician, it may be deemed that the patient is not suffering from
stroke.
To further improve our Clinician’s understanding, triage, assessment and care of patients suspected of
suffering from hyper acute stroke, the Scottish Ambulance Service is embarking on an ambitious plan to
link pre-hospital data with hospital and Scottish Stroke Care Audit data through collaboration with NHS
Scotland’s Information Services Division (ISD) and the Unscheduled Care Datamart where this joint data
is held.
It is anticipated that by having this 360˚ review process of the patient journey, we will be able to
ascertain the effectiveness and sensitivity of our clinical pathways and treatment and care of our service
users. Through collaboration with our partners and colleagues across the stroke and wider health care
communities, we hope to further improve and build on the high level of care that we provide to patients
in the pre-hospital setting.
52019 National Report - Scottish Stroke Improvement Programme
3 Inpatients
During 2018 over 9,000 patients were admitted to hospital with a final diagnosis of stroke and entered
into the SSCA. This is a similar number to 2017. The characteristics of patients admitted to hospital are
shown in Table 1.1. Ischaemic stroke was identified in 87% of patients and haemorrhagic stroke in 11%.
There were similar numbers of men and women with a mean age of 71 years for men and 76 years for
women; mean ages varied across NHS boards but the mean age of stroke was always greater in women.
When patients in the audit were divided according to socio-economic factors, the areas of highest
levels of deprivation, as measured by the Scottish Index of Multiple Deprivation (SIMD), had the highest
percentage of the patient group. This reflects the recognised association between social deprivation and
risk of stroke and emphasises the need to identify and address the factors contributing to stroke risk in
this population.
Variations in case mix between NHS boards were observed as in previous years and this was particularly
marked for the variable relating to ability to walk. This apparent variation in case mix emphasises the
need to correct any patient outcome results for variations in stroke severity.
Table 3.1 lists the numbers of patients discharged from each hospital along with availability of specialist
stroke unit beds in that hospital. Glasgow Royal Infirmary and the Queen Elizabeth University Hospital
Glasgow are the only two settings to have adopted the Hyper-Acute Stroke Unit (HASU) model involving
a small number of beds with a short length of stay aiming to facilitate early assessment, diagnosis, and
treatment before moving patients to another ward. The majority of hospitals have an integrated stroke
unit, which aims to combine both acute care and ongoing rehabilitation. Several hospitals also have
stroke rehabilitation unit beds in an off-site hospital.
The most important overall indicator of the performance of stroke services within NHS Boards or
hospitals is their performance against the stroke care bundle as described in the introduction. The
cumulative proportions of patients with a final diagnosis of stroke who were managed in accordance
with all four standards, which comprised the care bundle, was 68% across Scotland, a significant
improvement on the 2017 performance of 65%. Chart 1.1 shows that Tayside, Dumfries and Galloway
and Lanarkshire Health Boards showed a significant improvement; no Boards had a significant decline in
performance.
Chart 1.2 shows similar data presented by hospital, with significant improvements in Glasgow Royal
Infirmary, University Hospital Monklands, Ninewells Hospital and Dumfries and Galloway Royal Infirmary.
The proportion of patients across Scotland with a final diagnosis of stroke who accessed a stroke unit
on the day of admission or the day after (82%) was the same in 2018 as in 2016 and 2017, and thus
continues to fall below the standard of 90% (see chart 3.1). This indicator is important because early
admission to a stroke unit has been associated with a reduced likelihood of dying after stroke. Ninewells
Hospital, Dundee and Aberdeen Royal Infirmary both achieved statistically significant improvement in
performance in 2018, with Ninewells now performing above the 90% target. It should be noted that
small hospitals such as those on the Islands and in rural NHS boards perform well against this standard
because their only medical ward fulfils our definition of a stroke unit.
For larger hospitals, the standard can be challenging because stroke patients are often boarded into
medical wards and stroke unit beds filled with non-stroke patients particularly during periods of high bed
demand. The number of stroke unit beds appears to be an important determinant of performance but
there is also considerable variation in how well hospitals can manage these stroke beds. The degree of
priority attached to achieving this standard appears to vary between hospitals.
A stroke often affects the patient’s ability to swallow food, fluids and medication safely so if a patient
is identified as having a possible stroke a swallow assessment should be done as soon as possible
and clearly recorded in the patient’s case-notes. Previous research has suggested that the greater
the delay to swallow screen the higher the risk of stroke-associated pneumonia. Chart 3.2 shows the
proportion of patients with a final diagnosis of stroke in Scotland who had a swallow screen within 4
hours of admission with the hospitals ranked from the highest to the lowest. Overall, 80% of patients
62019 National Report - Scottish Stroke Improvement Programme
were treated in accordance with this standard which is a small but significant improvement since 2017
(76%). However, this still falls short of the target of 100%. University Hospital Crosshouse, University
Hospital Monklands and Glasgow Royal Infirmary all showed a statistically significant improvement;
elsewhere performance remained static. Chart 3.5 shows the percentage of patients who had a swallow
screen within 4, 12, and 24 hours of admission which allows assessment of the extent to which units are
missing the target – in some units there are many ‘near misses’ which might be fairly readily addressed.
Important measures to improve swallow screen performance include early identification of stroke
patients and ensuring nurses are trained to undertake a swallow screen promptly and record the result
clearly in the notes in the admission wards.
An early brain scan is required to exclude alternative causes of stroke symptoms such as brain tumours
and to distinguish stroke due to bleeding into the brain from those caused by blocked arteries. This
is important to allow treatment with thrombolysis, anticoagulants, and antiplatelet drugs. In 2018,
95% of stroke patients received a brain scan within 24 hours of admission, which was similar to 2017
(93%). The national standard is currently 95% of stroke patients receiving a brain scan within 24 hours
of admission (chart 3.3). 12 individual hospitals met or exceeded the standard, including Dumfries
and Galloway Royal Infirmary which achieved a significant improvement from 89% to 98%. Very early
scanning is an important factor for patients who can benefit from thrombolysis and thrombectomy. Most
hospitals operate a fast track brain scanning process for patients potentially suitable for thrombolysis.
After a brain scan has excluded bleeding on the brain patients should receive aspirin as soon as possible
since this has been shown to improve outcomes. Exceptions are those who are given thrombolysis, or
taking an anticoagulant, or are on an alternative antiplatelet drug, and also those who are allergic to
aspirin. 95% of patients without contra-indications should receive aspirin on the day of admission or
the day after. In 2018 92% of patients with a final diagnosis of ischaemic stroke and no clear contra-
indication received aspirin on the day of admission or the day after compared with 91% in 2017.
72019 National Report - Scottish Stroke Improvement Programme
Chart 3.1: Percentage of stroke patients admitted to a Stroke Unit within 1 day of
admission to hospital, 2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2013) of 90% of stroke patients admitted to a Stroke Unit within 1 day of admission.
100
90
80
2017 (%)
70
2018 (%)
60 statistically
significant
% 50 improvement
2018 (%)
40 no statistically
significant
30 change
2018 (%)
20 statistically
significant
10 decline
Stroke Standard
0 (2013)
Scotland
Belford*
Caithness*
GCH*
Gilbert Bain*
Crosshouse
Ninewells
Western Isles
Monklands
IRH
Hairmyres
ARI
QUEH
GRI
Wishaw
FVRH
PRI
DGRI
SJH
Dr Grays
Borders
RIE
RAH
L&I
Raigmore
WGH
Balfour
Ayr
VHK
Notes regarding Chart 3.1:
1. The denominator for the admission to Stroke Unit excludes: in-hospital strokes, patients discharged within 1 day and transfers in from
another hospital.
2. Due to the number of beds within some of the hospitals indicated (*) and the small numbers of stroke admissions to these hospitals it is not
practical to have a defined Stroke Unit. We have confirmed however that a defined stroke pathway is in place in these hospitals and that the
Scottish Stroke Care Standards criteria are established within that pathway.
3. The data included in Chart 3.1 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar years 2017 and 2018 (i.e. 1
January - 31 December).
4. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
5. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
6. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
82019 National Report - Scottish Stroke Improvement Programme
Chart 3.2: Percentage of stroke patients with a swallow screening within 4 hours of
admission, 2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2016) of 100% of stroke patients swallow screened within 4 hours of admission.
100
90
80
2017 (%)
70
2018 (%)
statistically
60 significant
improvement
% 50
2018 (%)
no statistically
40 significant
change
30
2018 (%)
statistically
20 significant
decline
10
Stroke Standard
(2016)
0
Scotland
L&I
Crosshouse
IRH
Borders
SJH
GCH
Dr Grays
GRI
RAH
RIE
Western Isles
Monklands
ARI
FVRH
Hairmyres
Caithness
Raigmore
Ninewells
Wishaw
Gilbert Bain
QUEH
PRI
DGRI
WGH
Belford
Balfour
Ayr
VHK
Notes regarding Chart 3.2:
1. The data included in Chart 3.2 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar years 2017 and 2018
(i.e. 1 January - 31 December).
2. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
3. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
4. A small proportion of patients with query in-hospital wake-up strokes are excluded from the chart.
5. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
6. Excludes a small proportion of in-hospital events where the date of onset is recorded but the time of onset is missing.
92019 National Report - Scottish Stroke Improvement Programme
Chart 3.3: Percentage of stroke patients with a brain scan within 24 hours of admission,
2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2016) of 95% of stroke patients to receive a brain scan within 24 hours of admission. *
The Scottish Stroke Care Standard for swallow screen within 4 hours was introduced from April 2016 and complete data are unavailable prior to
this date because swallow screen time was only recorded from April 2016. Prior to April 2016 only swallow screen date was recorded.
100
90
80
2017 (%)
70
2018 (%)
statistically
60 significant
improvement
% 50
2018 (%)
no statistically
40 significant
change
30
2018 (%)
statistically
20 significant
decline
10
Stroke Standard
(2016)
0
Scotland
Belford
Wishaw
Hairmyres
Borders
GCH
Western Isles
DGRI
QUEH
SJH
FVRH
ARI
IRH
Dr Grays
Raigmore
WGH
Monklands
GRI
RIE
Crosshouse
Caithness
PRI
Gilbert Bain
RAH
Ninewells
L&I
Balfour
Ayr
VHK
Notes regarding Chart 3.3:
1. Uist & Barra Hospital, NHS Western Isles does not have a CT scanner but patients are airlifted to Western Isles Hospital and a proportion may
arrive in sufficient time to have brain imaging within 24 hours of admission.
2. The data included in Chart 3.3 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar years 2017 and 2018 (i.e. 1
January - 31 December).
3. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
4. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
5. A small proportion of patients with query in-hospital wake-up strokes are excluded from the chart.
6. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
7. Excludes a small proportion of in-hospital events where the date of onset is recorded but the time of onset is missing
102019 National Report - Scottish Stroke Improvement Programme
Chart 3.4: Percentage of acute ischaemic stroke patients given aspirin in hospital within
1 day of admission, 2017 and 2018 data (based on final diagnosis).
Horizontal line reflects Scottish Stroke Care Standard (2013) of 95% ischaemic stroke patients to receive aspirin within 1 day of admission.
100
90
80
2017 (%)
70
2018 (%)
statistically
60 significant
improvement
% 50
2018 (%)
no statistically
40 significant
change
30
2018 (%)
statistically
20 significant
decline
10
Stroke Standard
(2013)
0
Scotland
Gilbert Bain
Western Isles
GCH
Wishaw
FVRH
Borders
SJH
IRH
Monklands
Hairmyres
GRI
Caithness
QUEH
ARI
Dr Grays
Raigmore
Crosshouse
Belford
Ninewells
DGRI
PRI
RAH
RIE
WGH
L&I
Ayr
Balfour
VHK
Notes regarding Chart 3.4:
1. The denominator for the percentages excludes patients with valid reasons not to give early aspirin (e.g. contraindications) and those in receipt
of thrombolysis where aspirin may be delayed for clinical reasons. A small proportion of patients with query in-hospital wake-up strokes are
also excluded.
2. The data included in Chart 3.4 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar years 2017 and 2018 (i.e. 1
January - 31 December).
3. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
4. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
112019 National Report - Scottish Stroke Improvement Programme
Chart 3.5: Percentage of stroke patients with a swallow screen by number of hours to
swallow screen, 2018 data (based on final diagnosis).
Vertical line reflects Scottish Stroke Care Standard (2016) of 100% of stroke patients to receive a swallow screen within 4 hours of admission.
Scotland
Borders
Western Isles
L&I
SJH
Dr Grays
IRH
Crosshouse Within 4 hours
VHK Within 12 hours
Monklands Within 24 hours
Wishaw Stroke Standard
Gilbert Bain (2016)
GRI
RIE
GCH
RAH
Ninewells
Hairmyres
QUEH
DGRI
ARI
Raigmore
Caithness
FVRH
PRI
WGH
Balfour
Belford
Ayr
0 20 40 60 80 100
%
Notes regarding Chart 3.5:
1. The data included in chart 3.5 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar year 2018
(i.e. 1 January - 31 December).
2. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
3. There may be some slight differences in the numerators and denominators when comparing Chart 3.5 to Chart 3.3 because some records for
in-hospital stroke patients may have been assigned to their year of admission rather than their year of onset. This principally affects records
around the period of December of one year and January of the next year where the date of admission is in one year and the date of onset is in
the next year.
4. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
5. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
6. Excludes a small proportion of in-hospital events where the date of onset is recorded but the time of onset is missing.
122019 National Report - Scottish Stroke Improvement Programme
Chart 3.6: Percentage of stroke patients with a brain scan by number of hours to scan,
2018 data (based on final diagnosis).
Vertical line reflects Scottish Stroke Care Standard (2016) of 95% of stroke patients to receive a brain scan within 24 hours of admission.
* The Scottish Stroke Care Standard for swallow screen within 4 hours was introduced from April 2016 and complete data are unavailable prior to
this date because swallow screen time was only recorded from April 2016. Prior to April 2016 only swallow screen date was recorded.
Note that the Scotland column in the chart is coloured light green and dark green simply to differentiate it from the hospital columns and
the colours are not indicative of performance. Light green corresponds to ‘Within 24 Hours’ and dark green corresponds to ‘Within 4
Hours’.
Scotland
Belford
Wishaw
Hairmyres
Borders
GCH
Western Isles
DGRI
QUEH Within 12 hours
VHK Within 24 hours
SJH Stroke Standard
FVRH (2016)
ARI
IRH
Dr Grays
Raigmore
WGH
Monklands
Balfour
GRI
RIE
Crosshouse
Caithness
PRI
Gilbert Bain
RAH
Ninewells
Ayr
L&I
0 20 40 60 80 100
%
Notes regarding Chart 3.6:
1. The data included in chart 3.6 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar year 2018 (i.e. 1 January - 31
December).
2. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
3. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
4. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
5. There may be some slight differences in the numerators and denominators when comparing Chart 3.6 to Chart 3.4 because some records for
in-hospital stroke patients may have been assigned to their year of admission rather than their year of onset. This principally affects records
around the period of December of one year and January of the next year where the date of admission is in one year and the date of onset is in
the next year.
6. Excludes a small proportion of in-hospital events where the date of onset is recorded but the time of onset is missing.
132019 National Report - Scottish Stroke Improvement Programme
Chart 3.7: Percentage of acute ischaemic stroke patients given aspirin in hospital by
number of days to receipt, 2018 data (based on final diagnosis).
Vertical line reflects Scottish Stroke Care Standard (2013) of 95% of acute ischaemic stroke patients to receive aspirin within 1 day of admission.
Note that the Scotland column in the chart is coloured light green and dark green simply to differentiate it from the hospital columns and
the colours are not indicative of performance. Light green corresponds to ‘Within 24 Hours’ and dark green corresponds to ‘Within 4
Hours’.
Scotland
Western Isles
Gilbert Bain
GCH
Wishaw
FVRH
Borders
SJH Same Day
IRH 1 Day
Monklands 2 Days
Hairmyres
Stroke Standard
GRI (2013)
Caithness
QUEH
ARI
Dr Grays
VHK
Raigmore
Crosshouse
Belford
Ninewells
DGRI
Ayr
PRI
RAH
RIE
WGH
L&I
Balfour
0 20 40 60 80 100
%
Notes regarding Chart 3.7:
1. The data included in chart 3.6 were extracted from eSSCA on the 21st March 2019. Changes/ updates to the data following this date will
therefore not feature in this analysis. The data relate to patients with final diagnosis of stroke and are for calendar year 2018 (i.e. 1 January - 31
December).
2. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
3. The denominator for the percentages excludes patients with valid contraindications to aspirin and those in receipt of thrombolysis where aspirin
may be delayed for clinical reasons.
4. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
5. Uist and Barra Hospital has been excluded from this chart due to very low patient numbers.
6. There may be some slight differences in the numerators and denominators when comparing Chart 3.7 to Chart 3.5 because some records for
in-hospital stroke patients may have been assigned to their year of admission rather than their year of onset. This principally affects records
around the period of December of one year and January of the next year where the date of admission is in one year and the date of onset is in
the next year.
One group of patients in whom it is particularly challenging to meet the standards are the patients who
have a stroke whilst an inpatient. Early recognition of the diagnosis is often difficult because patients
may have the stroke whilst under anaesthetic, or during an intensive care admission, or on a background
of complex co-morbidities. There are sometimes delays in referral to the stroke service. About 5% of
strokes in Scotland occur whilst the patient is an inpatient but this varies between hospitals and probably
reflects the services they provide.
142019 National Report - Scottish Stroke Improvement Programme
Chart 3.8: Comparison of initial diagnosis of stroke versus final diagnosis of stroke,
2018 data).
Note that the Scotland column in the chart is coloured green and red simply to differentiate it from the hospital columns and the colours are
not indicative of performance. Light green corresponds to ‘Final Only’, red corresponds to ‘Initial & Final’ and dark green corresponds to
‘Initial Only’.
100%
90%
80%
70%
60%
Final Only
50% Initial AND Final
40% Initial Only
30%
20%
10%
0%
Scotland
Crosshouse
Borders
DGRI
GCH
FVRH
ARI
Dr Grays
GRI
IRH
QEUH
RAH
Belford
Caithness
L&I
Raigmore
Hairmyres
Monklands
Wishaw
RIE
SJH
WGH
Gilbert Bain
Ninewells
PRI
Uist & Barra
Western Isles
Ayr
Balfour
VHK
Notes regarding Chart 3.8:
1. Both initial diagnosis and final diagnosis may be recorded in the SSCA data relating, respectively, to whether a patient may be suspected of
having had a stroke and whether the stroke diagnosis is confirmed on investigation. Chart 3.8 presents information on three groups of patients,
those with:
- an initial diagnosis of stroke i.e. possible stroke patients who may turn out to have another diagnosis once investigations are complete;
- a final diagnosis of stroke i.e. patients confirmed as having had strokes when their initial diagnosis may have been considered as something
else;
- an initial diagnosis and final diagnosis of stroke i.e. patients suspected of having had a stroke who have this diagnosis confirmed on
investigation.
2. In some instances, data entered into eSSCA are assigned to admitting hospitals other than the main acute hospitals participating in the
Scottish Stroke Care Audit. Data for these hospitals are combined with data for their respective main acute hospitals.
3. During 2017 NHS Dumfries & Galloway opened the New Dumfries & Galloway Royal Infirmary.
152019 National Report - Scottish Stroke Improvement Programme
Table 3.1: Stroke Unit Information.
Hospital Name Number Hyper Acute Integrated Stroke Comments
of acute Acute Stroke Stroke Rehabilitation (e.g. Off-site Locations)
strokes Stroke Unit (ASU) Unit (ISU) Unit (SRU)
discharged Unit beds beds beds on
in 2018 (HASU) acute site
beds
Ayr Hospital 37 0 0 0 24 24 stroke rehab beds within Station 16
Crosshouse Hospital, 791 0 24 0 0 20 stroke rehab beds within 30 bed Redburn
Kilmarnock Rehabilitation ward, Ayrshire Central Hospital.
Borders General 196 0 0 12 0
Hospital, Melrose
Dumfries & Galloway 202 0 0 14 0
Royal Infirmary (DGRI)
Galloway Community 47 0 0 0 0 20 bedded unit with mix of medical and
Hospital (GCH) sugical admissions. It includes hyperacute &
acute stroke bed.
Victoria Hospital, 786 0 0 24 0 QMH Ward 6 - 15 beds within a stroke and
Kirkcaldy (VHK) general rehabilitation ward.
Letham ward Cameron Hospital - 12 funded
beds but currently operating 14 with increase
to 15/16 beds as necessary (rehabilitation for
over 65).
Sir George Sharp Unit (rehabilitation for
under 65) 6 to 7 out of 12 beds.
Forth Valley Royal 509 0 0 30 0 Stirling Community Hospital - 26 beds
Hospital in total - 10 stroke rehabilitation and 16
for patients with generic rehabilitation
requirements
Aberdeen Royal 686 0 16 0 0 Currently operating as stroke unit with 4
Infirmary (ARI) additional beds. Woodend - SRU: 34beds.
Fraserburgh - SRU: 6 beds
Dr Gray's Hospital, Elgin 160 0 0 8 0
Glasgow Royal 660 5 0 0 38 24 off-site rehab beds at Stobhill
Infirmary (GRI)
Inverclyde Royal 216 0 0 17 0
Hospital, Greenock
(IRH)
Queen Elizabeth 1 075 26 0 60 0
University Hospital
(QEUH), Glasgow
Royal Alexandra 443 0 0 30 0 Off site stroke rehab at Vale of Leven, 6 beds
Hospital, Paisley
(RAH)
Belford Hospital, Fort 24 0 0 0 0 Stroke beds within an acute medical ward
William
Caithness General 47 0 0 0 0 Stroke beds within an acute medical ward
Hospital, Wick
Lorn & Islands 34 0 0 0 0 6 stroke beds within another ward
Hospital, Oban
Raigmore Hospital, 334 0 0 22 0
Inverness
Hairmyres Hospital, 320 0 0 18 0
East Kilbride
Monklands Hospital, 285 0 0 20 0
Airdrie
Wishaw General 408 0 0 25 0
Hospital
Royal Infirmary of 981 0 0 44 0 Astley Ainslie Charles Bell Pavilion 40 beds
Edinburgh and East Pavilion 6 beds = 46 All are neuro
rehab beds (none are ring fenced for stroke).
St John's Hospital, 277 0 0 22 0
Livingston (SJH)
16You can also read