Results in 95 Hemorrhagic Stroke Patients Included in CLASS, a Controlled Trial of Clomethiazole Versus Placebo in Acute Stroke Patients
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Results in 95 Hemorrhagic Stroke Patients Included in
CLASS, a Controlled Trial of Clomethiazole Versus Placebo
in Acute Stroke Patients
N.G. Wahlgren, MD, PhD; E. Dı́ez-Tejedor, MD, PhD; J. Teitelbaum, MD FRCP(C); A. Arboix, MD;
D. Leys, MD; T. Ashwood, PhD; E. Grossman, MD;
for the CLASS (CLomethiazole Acute Stroke Study) Study Group
Background and Purpose—Clomethiazole is a neuroprotective drug that enhances g-aminobutyrate type A (GABAA)
receptor activity. Its efficacy and safety were tested in the CLomethiazole Acute Stroke Study (CLASS). The
protocol allowed a CT scan to be done after randomization but within 7 days of stroke onset to minimize delays
before start of treatment. Ninety-five of the 1360 patients randomized were diagnosed as having intracranial
hemorrhage rather than ischemic stroke. Safety results for clomethiazole compared with placebo in this group
are reported.
Methods—The study included patients with a clinical diagnosis of acute hemispheric cerebral infarction. Treatment was
a 24-hour intravenous infusion of 75 mg/kg clomethiazole or placebo. Patients with intracranial hemorrhage discovered
on a postrandomization CT were withdrawn from study treatment if treatment was ongoing, and all patients were
followed up to 90 days.
Results—Ninety-four patients received treatment, 47 in each group. The hemorrhage was classified as intracerebral
in 89 patients (94%). Mortality at 90 days was 19.1% in the clomethiazole group and 23.4% in the placebo group.
Sedation was the most common adverse event, occurring at a higher incidence in clomethiazole-treated patients
(clomethiazole 53%, placebo 17%), followed by rhinitis and coughing. The incidence and pattern of serious
adverse events was similar between the treatment groups. The percentage of patients reaching relative functional
independence on the Barthel Index (score $60) at 90 days was 59.6% in the clomethiazole group and 53.2% in
the placebo group.
Conclusions—Clomethiazole appears safe to administer to hemorrhagic stroke patients compared with placebo.
These results would obviate the need for a CT scan before therapy is initiated in acute stroke. The safety of
clomethiazole in hemorrhagic stroke patients will be further evaluated in a prospective study that is under way in
North America. (Stroke. 2000;31:82-85.)
Key Words: cerebral ischemia n clinical trials n clomethiazole n hemorrhage n neuroprotection
C lomethiazole (Zendra, AstraZeneca) is a neuroprotective
drug that has been shown to be effective in several
animal models of cerebral ischemia.1– 6 The compound en-
patients treated.10 However, for 545 patients classified before
randomization as having total anterior circulation syndrome,
the percentage who reached relative functional independence
hances g-aminobutyrate type A (GABAA) receptor activity,7–9 (Barthel Index score $60) was 40.8% for clomethiazole and
and this is a plausible mechanism for its neuroprotective 29.8% for placebo, a relative benefit of 37% (nominal
effect. The efficacy and safety of clomethiazole were tested in P50.008).11 It is widely believed that it is important to start
a double-blind, placebo-controlled study that recruited 1360 acute stroke treatment as soon as possible after onset of the
patients with a clinical diagnosis of acute hemispheric cere- stroke. To minimize delays in the hospital, the study did not
bral infarction (CLomethiazole Acute Stroke Study require a CT scan before randomization; however, one had to
[CLASS]). There was no statistically significant difference be performed within the first 7 days after randomization. This
between the treatment groups in functional outcome for all resulted in the inclusion of patients with a diagnosis of
Received July 6, 1999; final revision received October 5, 1999; accepted October 8, 1999.
From the Stroke Research Unit, Department of Neurology, Karolinska Hospital, Stockholm, Sweden (N.G.W.); Stroke Unit, Department of Neurology,
University Hospital La Paz, Universidad Autónoma de Madrid, Spain (E.D.-T.); Hopital Maisonneuve Rosemont, Montreal, Canada (J.T.); Quinta de
Salud la Alianza, Servicio de Neurologia, Barcelona, Spain (A.A.); Service de Neurologie Vasculaire, Hôpital Roger Salengro, Lille, France (D.L.); and
AstraZeneca, Södertälje, Sweden (T.A., E.G.).
AstraZeneca, the manufacturer of Zendra (clomethiazole), provided funding for this study.
Correspondence to N.G. Wahlgren, MD, The Stroke Research Unit, Department of Neurology, Karolinska Hospital, S-171 76 Stockholm, Sweden.
E-mail nilsgw@neuro.ks.se
© 2000 American Heart Association, Inc.
Stroke is available at http://www.strokeaha.org
82
Downloaded from http://stroke.ahajournals.org/ by guest on November 4, 2015Wahlgren et al Results for Clomethiazole in Hemorrhagic Stroke 83
TABLE 1. Demographic and Baseline Characteristics TABLE 2. Adverse Events of Any Severity (Mild, Moderate,
Severe) Occurring at >5% Incidence During Treatment
Clomethiazole Placebo
Characteristics (n548) (n547) Clomethiazole Placebo
Age, y, mean6SD 73.368.5 74.069.8 Preferred Term (n547) (n547)
Weight, kg, mean6SD 70.4614.4 68.0614.8 Somnolence (including sedation) 25 (53.2) 8 (17.0)
Height, cm, mean6SD 167.6610.3 165.967.9 Rhinitis 9 (19.1) 1 (2.1)
Male sex, n (%) 21 (44) 22 (47) Fever 6 (12.8) 7 (14.9)
Smoker, n (%) 6 (13) 4 (9) Coughing 4 (8.5) 0 (0)
Diabetes, n (%) 5 (10) 7 (15) Agitation 3 (6.4) 2 (4.3)
Hypertension, n (%) 20 (42) 16 (34) Headache 2 (4.3) 3 (6.4)
Atrial fibrillation, n (%) 3 (6) 3 (6) Hypertension 2 (4.3) 6 (12.8)
Myocardial infarction, n (%) 4 (8) 3 (6) Vomiting 2 (4.3) 8 (17)
Angina, n (%) 8 (17) 3 (6) Tachycardia 0 4 (8.5)
Cardiac failure, n (%) 4 (8) 3 (6) Bradycardia 0 3 (6.4)
Previous stroke, n (%) 3 (6) 6 (13) Coma 0 3 (6.4)
Previous TIA, n (%) 4 (8) 6 (13) Values are n (%).
Baseline blood pressure, mm Hg,
mean6SD infusion. Patients were assessed at baseline and regularly during the
infusion for adverse events, blood pressure, and level of sedation.
Systolic 169.9624.9 163.2624.4
Sedation was assessed by use of a sedation scale used in a previous
Diastolic 93.0615.1 91.6614.4 dose-escalation trial.13 Serious adverse events (SAEs) were defined
Median baseline SSS-58 score as those that resulted in death, hospitalization, or permanent or
(interquartile range) 27.5 (17–34) 26 (16–32) significant disability or that were life threatening or required medical
or surgical intervention. Information on all SAEs was collected up to
Randomized to stratum 0–6 h, n (%) 35 (73) 24 (51)
7 days after randomization, and data on those SAEs that were
Time since onset, h, mean6SD 5.662.8 6.763.1 believed to be related to treatment were collected for 90 days during
the first half of the study recruitment period. The protocol was then
amended owing to regulatory requirements, and all data on SAEs
intracranial hemorrhage. We report here on the safety of were collected up to day 90. Functional and neurological outcomes
clomethiazole versus placebo in patients with intracranial were assessed with the Barthel Index14 and the SSS,12 respectively,
hemorrhage. at 7, 30, 60, and 90 days. The primary end point was the percentage
of patients scoring $60 on the Barthel Index (relative functional
independence) at 90 days.
Subjects and Methods
The study was performed in accordance with the Declaration of
Helsinki, and the protocol was approved by the local ethics commit- Results
tees. All patients or their relatives gave informed consent. A full Recruitment and Baseline Characteristics
description of the study design, inclusion and exclusion criteria, Ninety-five (7%) of the 1360 patients randomized to CLASS
treatment regimen, assessments, statistical methods, and study group
members has been given elsewhere.10 In brief, 1360 patients were were classified as having intracranial hemorrhage. One pa-
recruited at 85 centers in 7 European countries and Canada. Patients tient randomized to the clomethiazole group did not receive
were included if they were aged 40 to 90 years and were conscious, treatment because an intracerebral hemorrhage was found on
with a clinical diagnosis of acute hemispheric cerebral infarction and the CT scan before treatment could be started. Therefore, 94
onset of symptoms in the 12 hours before randomization. They had
patients were included in the analysis of all patients treated
to score #40 on the sum of the Scandinavian Neurological Stroke
Scale (SSS) long-term items12 and #14 for the sum of the SSS motor (47 in each treatment group). All but 1 of these patients (in
items of arm, hand, and leg at baseline. Patients were randomized to the clomethiazole group) were randomized before the results
either clomethiazole or placebo (75 mg/kg), which was administered of the CT scans were known.
as a 15-minute loading infusion (8% of total dose) followed by a The hemorrhage was classified as intracerebral in 89
maintenance infusion to 24 hours. If patients became excessively
patients (94%). Of the remaining patients, 2 had subdural
sedated, the infusion was interrupted and then resumed at half the
previous rate. hematomas, 1 had subarachnoid hemorrhage, and 1 had
A CT scan was required within 7 days of stroke onset. When this mixed intracerebral and subarachnoid hemorrhage in the
was done before randomization, patients with a diagnosis of intra- clomethiazole group, and 1 patient in the placebo group had
cranial hemorrhage were excluded. Patients diagnosed with intracra- mixed intracerebral and subarachnoid hemorrhage.
nial hemorrhage after a postrandomization CT scan were withdrawn
from treatment if treatment was ongoing. All patients were followed
The mean age of patients classified as having an intracranial
up to 90 days. hemorrhage was 73.669.1 years compared with 71.2611.2
Hemorrhage on the CT scan was classified as subdural hematoma, years for the ischemic stroke patients (n51254), and these
intracerebral hemorrhage, or subarachnoid hemorrhage. More than 1 patients had slightly worse scores on the SSS-58 scale (hemor-
category could be recorded. Patients with CT evidence of infarction rhagic: median 26 points, interquartile range 17 to 33; ischemic:
and hemorrhagic transformation (as judged by the investigator) were
not classified as having intracranial hemorrhage. median 28 points, interquartile range 19 to 38).
Assessments of body temperature, ECG, laboratory tests, and The demographic and baseline characteristics of patients in the 2
plasma sampling were made at baseline and at the end of the treatment groups were reasonably well balanced for age and
Downloaded from http://stroke.ahajournals.org/ by guest on November 4, 201584 Stroke January 2000
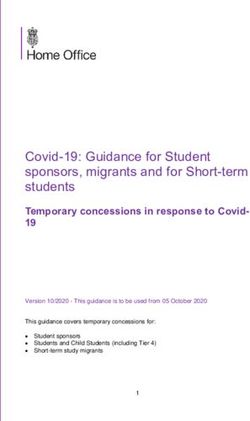
Distribution of Barthel Index scores for clomethia-
zole and placebo groups at 90 days.
severity on the SSS-58 scale. Mean time since onset of symptoms patients and 25 (53.2%) of 47 placebo patients scored $60 on
was 1 hour shorter in the clomethiazole group, and there were some the Barthel Index, an absolute difference of 6.4% (OR51.3,
differences in the medical history (Table 1). Mean blood pressure 95% CI 0.57 to 2.94). At the $95 cutpoint, the difference
was slightly higher in the clomethiazole group (Table 1). between the groups was 14.9 percentage units to the advan-
tage of clomethiazole. On the SSS-48 scale, the median
Dose Administered absolute change from baseline to last rating was 16 points for
The mean dose administered in the clomethiazole group was
clomethiazole patients and 13 points for placebo patients.
58.1 mg/kg compared with 62.4 mg/kg for the placebo group.
The latter was calculated from the volume administered. There
were 15 withdrawals (32%) from each treatment group. The
Discussion
Stroke patients with a diagnosis of intracranial hemorrhage
main reason for withdrawal was diagnosis of hemorrhage during
the 24-hour treatment period, which was a protocol-specified are usually excluded from clinical trials of putative acute
criterion for withdrawal. This occurred in 10 clomethiazole stroke therapies. This was also done in CLASS if a preran-
patients (21%) and 12 placebo patients (20%). The second most domization CT scan was performed, but a prerandomization
common reason for withdrawal was the occurrence of adverse scan was not a requirement. As a result, 7% of the patients
events, which occurred in 4 clomethiazole patients (9%) and 3 randomized had intracranial hemorrhage. This is the first
placebo patients (6%). All of these adverse events were related report of the safety and tolerability of a neuroprotective drug
to reduced consciousness, eg, sedation or coma. compared with placebo in patients with acute hemorrhagic
stroke.
Safety The patients included in the study were slightly older and
Mortality at 90 days was slightly lower for patients treated scored only 2 points worse on the SSS than the ischemic
with clomethiazole than for those treated with placebo stroke group. Correspondingly, the 90-day mortality rate of
(clomethiazole 19.1%, placebo 23.4%), but the difference 23.4% in the placebo group was similar to that for patients
between groups was not statistically significant (OR 0.78, with ischemic stroke who received placebo (19.4%).10 The
95% CI 0.29 to 2.09; P50.614), and there was no difference
30-day mortality rate of '15% in the hemorrhagic stroke
between the Kaplan-Meier estimates of the survival distribu-
group is relatively low compared with most series of these
tion (data not shown). The most common primary cause of
patients, in whom the mortality rate at '1 month ranges from
death was damage due to initial stroke (6 patients in the
clomethiazole group and 4 in the placebo group). Mortality at 35% to 50%.15–17 Similarly, functional outcome in this study
30 days was 17.0% in the clomethiazole group and 14.9% in was relatively good, with '53% of hemorrhagic patients who
the placebo group. The incidence of adverse events during were treated with placebo reaching relative functional inde-
treatment is shown in Table 2. Somnolence (which includes pendence at 90 days, in contrast to a figure of 25% reported
the term sedation), rhinitis, and coughing were the most in previous series after 4 months of follow up.17 It is likely
common adverse events, and these occurred at a higher rate in that the better outcome in the present study is due to a large
the clomethiazole group. The incidence of SAEs was similar extent to the exclusion of patients with reduced consciousness
in both treatment groups (8 clomethiazole patients, 5 placebo and symptoms of brain stem stroke.17
patients), and there was no obvious difference between the Sedation was the most common adverse event produced by
treatment groups in the type of adverse events reported. The clomethiazole, but the incidence of some respiratory adverse
most common event was cerebral hemorrhage (3 clomethia- events was also increased. The pattern and incidence of
zole patients, 1 placebo patient), and these cases corre- adverse events was very similar to that reported for all
sponded with the initial diagnosis of the illness. Clomethia- patients.10 Clomethiazole also produced a mild lowering of
zole produced a mild lowering of systolic blood pressure systolic blood pressure. This was similar to what was seen in
during treatment compared with placebo. The mean differ- all patients in whom it was not associated with a worse
ence between the treatment groups for the change from
outcome.18 The incidence of SAEs was similar between the
baseline to the minimum value at any time during treatment
treatment groups, and there was no difference in mortality.
was 7 mm Hg (SE 4.3; P50.105) for systolic and 0 mm Hg
Hemorrhagic patients constituted a small subgroup of all
(SE 2.6) for diastolic blood pressure. There were no differ-
ences between the treatment groups for mean laboratory test patients randomized, and the study was not powered to detect
values, including coagulation tests, or mean ECG times. a difference between treatment groups in functional outcome
for this subgroup. There were indications of a better func-
Functional and Neurological Outcomes tional outcome in hemorrhagic stroke patients treated with
The outcome on the Barthel Index at 90 days is shown in the clomethiazole compared with placebo, but this might be due
Figure. Twenty-eight (59.6%) of 47 clomethiazole-treated to imbalances in severity and prognostic factors at baseline. A
Downloaded from http://stroke.ahajournals.org/ by guest on November 4, 2015Wahlgren et al Results for Clomethiazole in Hemorrhagic Stroke 85
much larger study is required to test the efficacy of clome- 8. Hales TB, Lambert JJ. Modulation of GABAA and glycine receptors by
thiazole in hemorrhagic stroke. chlormethiazole. Eur Pharmacol. 1992;210:239 –246.
9. Moody EJ, Skolnick P. Clomethiazole: neurochemical actions at the
We conclude that clomethiazole appears safe to administer gamma-aminobutyric acid complex. Br J Pharmacol. 1989;164:
to hemorrhagic stroke patients, and in contrast to 153–158.
thrombolytics, it should not be necessary to obtain the results 10. Wahlgren NG, Ranasinha KW, Rosolacci T, Franke CL, von Erven
of a CT scan before clomethiazole treatment for acute stroke PMM, Ashwood T, Claesson L, for the CLASS Study Group. Clome-
thiazole Acute Stroke Study (CLASS): results of a randomised controlled
is begun. The safety of the drug is being further studied in a
trial of clomethiazole versus placebo in 1360 acute stroke patients. Stroke.
prospective study that is under way in North America in 1999;30:21–28.
which the volume of hemorrhage is also being measured.19 11. Wahlgren NG, Bornhov S, Sharma A, Cederin B, Rosolacci T, Ashwood T,
Claesson L, for the CLASS Study Group. The Clomethiazole Acute Stroke
Acknowledgment Study (CLASS): efficacy results in 545 patients classified as total anterior
circulation syndrome (TACS). J Stroke Cerebrovasc Dis. 1999;8:1–10.
This trial was sponsored by Astra Arcus AB, Södertälje, Sweden, the
12. Scandinavian Stroke Study Group. Multicenter trial of hemodilution in ischemic
manufacturer of Zendra (clomethiazole).
stroke, I: results in the total study population. Stroke. 1987;18:691–699.
13. Wester P, Strand T, Wahlgren NG, Ashwood T, Osswald G. An open
References study of clomethiazole in patients with acute cerebral infarction. Cere-
1. Cross AJ, Jones JA, Baldwin Ma, Green AR. Neuroprotective activity of brovasc Dis. 1998;8:188 –190.
clomethiazole following transient forebrain ischemia in the gerbil. Br J 14. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md
Pharmacol. 1991;104:406 – 411. Med J. 1965;14:61– 65.
2. Cross AJ, Jones JA, Snares M, Jostell K-G, Bredberg U, Green AR. The 15. Fogelholm R, Nuutila M, Vuorela A-L. Primary haemorrhage in the
protective action of chlormethiazole against ischaemia-induced neurogen- Jyväskulä region, Central Finland, 1985– 89: incidence, case fatality rate,
eration in gerbils when infused at doses having little sedative or anticon- and functional outcome. J Neurol Neurosurg Psychiatry. 1992;55:
vulsant activity. Br J Pharmacol. 1995;114:1625–1630. 546 –552.
3. Sydserff SG, Cross AJ, Green AR. The neuroprotective effect of chlorme-
16. Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral
thiazole on ischaemic neuronal damage following permanent middle
haemorrhage more than twice as common as subarachnoid hemorrhage.
cerebral artery ischaemia in the rat. Neurodegeneration. 1995;4:323–328.
J Neurosurg. 1993;78:188 –191.
4. Sydserff SG, Cross AJ, West KJ, Green AR. The effect of chlorme-
17. Anderson CS, Chakera TMH, Stewart-Wynne EG, Jamrozik KD.
thiazole on ischaemic neuronal damage in a model of transient focal
ischaemia. Br J Pharmacol. 1995;114:1631–1635. Spectrum of primary intracerebral haemorrhage in Perth, Western Aus-
5. Snape MF, Baldwin HA, Cross AJ, Green AR. The effects of chlorme- tralia, 1989 –90: incidence and outcome. J Neurol Neurosurg Psychiatry.
thiazole and nimodipine on cortical infarct area after focal cerebral 1994;57:936 –940.
ischaemia in the rat. Neuroscience. 1993;53:837– 844. 18. Wahlgren NG. The Clomethiazole Acute Stroke Study (CLASS): safety
6. Marshall JWB, Cross AJ, Murray TK, Ridley RM. Functional benefit results in 1356 patients with acute hemispheric stroke. Neurology. 1998;
from clomethiazole treatment after focal cerebral ischaemia in a 50(suppl 4):A212.
non-human primate species. Stroke. 1998;29:330. Abstract. 19. Lyden PD, Ashwood T, Claesson L, Odergren T, Friday GH, Martin-
7. Cross AJ, Stirling JM, Robinson TN, Bowen DM, Francis PT, Green AR. Munley S. The clomethiazole acute stroke study in ischemic, hemorrhagic
The modulation by clomethiazole of the GABAA receptor complex in rat and t-PA treated stroke: design of a phase III trial in the U.S. and Canada.
brain. Br J Pharmacol. 1989;98:284 –290. J Stroke Cerebrovasc Dis. 1998;7:435– 441.
Downloaded from http://stroke.ahajournals.org/ by guest on November 4, 2015Results in 95 Hemorrhagic Stroke Patients Included in CLASS, a Controlled Trial of
Clomethiazole Versus Placebo in Acute Stroke Patients
N. G. Wahlgren, E. Díez-Tejedor, J. Teitelbaum, A. Arboix, D. Leys, T. Ashwood and E.
Grossman
for the CLASS (CLomethiazole Acute Stroke Study) Study Group
Stroke. 2000;31:82-85
doi: 10.1161/01.STR.31.1.82
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2000 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/31/1/82
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/
Downloaded from http://stroke.ahajournals.org/ by guest on November 4, 2015You can also read