The Dream Team: A New Twist on Care
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Dream Team: A New Twist on Care
Management Design (Title/Presentation #359)
• Paula Spears, DNSc, RN, NEA-BC, VP Professional Practice, Research and
Magnet
• Darla Banks, MS, BSN, RN, CCRN, CNL, Director CNL Program
• Sherry Petrillo, MS, RN, CCM, Senior Director Care Transition Management
AONE Annual Meeting
April 2015
Disclosure
Today’s presenters do not have any relevant financial interests presenting a conflict of interest to disclose.
Participants must attend the entire session(s) in order to earn contact hour credit. Continuing Nursing Education credit can be
earned by completing the online session evaluation.
The American Organization of Nurse Executives is accredited as a provider of continuing nursing
education by the American Nurses Credentialing Center’s Commission on Accreditation.
AONE is authorized to award one hour of pre-approved ACHE Qualified Education credit (non-ACHE) for this program toward
advancement, or recertification in the American College of Healthcare Executives.
Objectives 1. Participants will describe the role of nurse leaders to effectively develop a new delivery model for the acute care setting. 2. Participants will critically analyze a care delivery model that creates a nurse led team to optimize the functions of care coordination within redesigned and integrated care management processes.

Our Story: Background Information

• Total of 25 acute-care and short-stay hospitals that are owned, operated, joint-ventured or affiliated with the System. • 14 Hospitals are wholly owned • 18 Outpatient Facilities • 250 Community access points • 3,800 Licensed hospital beds • 22,500 Employees • 6700 Registered Nurses • 5500 Physicians

“There is no more powerful engine driving an organization toward excellence and long-range success than an attractive, worthwhile, achievable vision for the future, widely shared.” — Burt Nanus, Visionary Leadership

Alignment with AONE AONE’s Future Care Delivery Models AONE’s Nurse Executive Competencies. Managing the Journey Competency: Knowledge of the Health Care • Nurses integrate all contributions to patient care Environment and serve as managers of the patient’s journey – Delivery Models/Work Design not only their piece but also the interdisciplinary • Maintain current knowledge of patient care hand-offs throughout the patient care process. delivery systems and innovations. • Integrated teams achieve patient outcomes. As • Articulate various delivery systems and patient care managers of the patient’s journey, nurses are models and the advantages/disadvantages of each. responsible for clarifying, integrating and • Serve as change agent when patient care coordinating the roles of the interdisciplinary team. work/workflow is redesigned. • The role of manager ensures that what the patient • Determine when new delivery models are has negotiated with his/her caregivers is carried out appropriate, and then envision and develop them. appropriately and that the nurse-patient team stands above all as the model for care delivery.

Alignment with THR Objectives
• Quality Measures • Nursing and Physician Engagement
– Nursing Core Measures • Nursing Retention
• Pay for Performance Documentation – First Year Retention
– Present on Admission Indicators (POA) – Nurse Vacancy
• Value Based Purchasing Indicators • Improved Patient Throughput
– HCAHPS – Average Discharge Time
– Hospital Acquired Conditions – 11AM and 2PM Discharge
• Prevention of Complications/ • Cost savings
Risk Avoidance – Variable Cost Opportunities
– DVT – LOS
– Nosocomial Infections
– Decreased Overtime
– Readmissions
Triple Aim
Goals Tools Outcomes
Prevention
Population Disease Registry
Health Clinical Outcomes
Disease Quality Measure • Disease specific
Management Disease Managers (Diabetes, Cardio,
Resp)
• Preventive care
Access • Care coordination
(all cause
readmission,
Care Providers admission for
Member Care ambulatory sensitive
Triple Aim Care Transition Mgmt
Experience Coordination conditions)
• Member experience
Navigation
Resource
Stewardship
Total Cost of Robust reporting
Care Dashboards Financial Outcomes
High Value Clinical Review • Total medical PMPM
Network
Business Model
Expense reduction Revenue
Decrease unit cost Decrease utilization Growth
Appropriate
Delivery Efficiency
Utilization Revenue
(service/care)
(level/type)
• All care team • Population health • Total population
members risk management risk and global
practicing at the strategies budget
top of their license • Care coordination arrangements
• Streamlined work and navigation • Bundle services
flow • Decrease and payment for
• Process variation in episodes of care
automation diagnosis and or chronic health
• Decrease care treatment conditions
process variation
… while increasing quality and member experienceCare Management Redesign Initiative
The Case for Change
The need for change:
Over the next few years, we expect health care costs to rise, reimbursements to
decrease and a large growth in the number of patients we will serve. To succeed in this
new environment, THR has to deliver care differently. One of the ways THR will do this is
in care management.
There is a great variety in how THR cares for patients from hospital to hospital, making it
difficult to consistently deliver evidence-based care system wide and across the
continuum.
The vision:
Over the next few years, we will create a new care management model, adopt new
technologies, workflows and processes.The New Definition of Care Management
Acute Care Coordination
• Nurse Manager
Improve outcomes by reliably • Charge Nurse
applying medical science to each • Advanced Practice Nurses
patient. • CNL/PCF
• Direct Care Nurse
Denials & Appeals Management Care Transition
• Clinical Review Denials & Management
Appeals RNs • CTM RN
• Clinical Review Specialists
Care Management • CTM SW
• Post-acute Care Managers
Utilization Management
• Clinical Review Utilization Management
RNs
• Clinical Review SpecialistsCare Management Redesign Initiative
Corporate Level Organization Structure
EVP, President of Population Management SVP, Chief Nursing Executive
(Dr. Joan Clark)
Chief Accountable Care Care Management VP of Professional Practice
Physician Advisors Officer Program Ownership and Research
(Dr. Paula Spears)
CBO Leader Entity CMOs
Blue Care Transition CNL/PCF Director
Clinical Review Director Green Care Transition
Management Senior Director Management Senior Director (Darla Banks)
(Sherry Petrillo)
• Texas Health Presbyterian • Texas Health Harris Methodist All Entity CNLs/PCFs
Hospital Dallas Hospital Fort Worth
• Texas Health Presbyterian • Texas Health Harris Methodist
Hospital Plano Hospital H-E-B
• Texas Health Arlington Memorial • Texas Health Harris Methodist
Hospital Hospital Southwest FW
• Texas Health Presbyterian • Texas Health Harris Methodist
Hospital Denton Alliance
• Texas Health Presbyterian • Texas Health Harris Methodist
Direct Reporting Relationship Hospital Allen Hospital Stephenville
• Texas Health Presbyterian • Texas Health Harris Methodist
. . . . . . . . . . . . . Collaborative Relationship Hospital Kaufman Hospital Cleburne
• Texas Health Harris Methodist
Hospital AzleWhat were the GAPs in accountability and what roles would we need in a new redesigned care delivery model.
Accountability at “POC”
• Needed a standard role to assume accountability for patient-care outcomes
• Someone to OWN the patient’s experience
• Needed a provider and coordinator of care at the point of care (not a manager)
• Available, consistent, reliable, and across the patient’s stay
• Needed POC application of EBP and PI to design, implement, evaluate, and improve
patient-care processes
• Additional issues:
– Not meeting the desired mark
– Lack of innovation for new roles / CDMs
– Move to 12 hour shift
– HospitalistsClinical Nurse Leader
• Master’s prepared advance clinician who functions as a
clinical leader for RNs and other staff, not as manager.
• Advances professional practice, accountability and reduces
costs.
• Major partner to nursing supervisors/managers.
• Knows about each patient in their microsystem.
• Acts as consistent figure for patient in the hospital to offset
fragmentation.
• Acts in the role of ‘traffic control’ or “quarterback” or
“attending nurse” in coordinating rollout of the plan for care.
• Acts as the primary liaison for physicians, other disciplines,
and families.
• Monitors competency and mentors team members.
• “Advanced Generalist” is role needed.
• Responsible 24/7.Twelve Bed Hospital©
• Model for coordinating patient care
• Breaks a patient care unit into small, 12 Bed 12 Bed 12 Bed
manageable segments of 12 or more beds,
depending on physical layout of the patient
care unit
• Places a nurse facilitator in the “lead” role for 12 Bed 12 Bed
all the patients in the hospital
17Twelve Bed Hospital©
One
Clinical Nurse Leader
per 12-16 patientsMountain.jpg
PATIENT ROUNDING
Operational Standards
The CNL PAVES the way to great patient outcomes©
Patient ADIET Assessing their understanding of Assess understanding of Validate Understanding Evaluate Discharge Planning. Safety Surveillance Address Pain, Potty, Anything Explain
their plan of Care their illness of education Home situation Position, Possession else we can continuity of
Management do for Care/Give Card
you?
P A V E S ©
What is the plan of care? Health Decision Health Literacy What type of care will you Fall Risk
Planning. Screening need when you go home? Central Line
Discuss Diagnosis, procedure, Foley
health care team, meds and What happened during Management plan When are you going home? Chest Tube
labs. this admission? CHF Dressings
Coumadin Where are you going when VTE
Begin discharge planning? How long has it been Diabetic discharged? Med Reconciliation
since your last Inhalers Restraints
Use leading questions? admission? Diet Who is their support person? Isolation
Stroke Seizure Precautions
Pt. journal Do you have primary Core Measures How will you get your Suicide Precautions
physician – when was the Pain meds? Depression Screening
last time you’ve seen
them?Facilitates Daily Care Briefings
CNL Dashboard: > 30 Indicators
Action Plan
Transformational Theme: Improve Quality Max Par Threshold FY10 FY11 FY12 YTD 13 Q1 FY13 Q2 FY13
Unit Acquired Pressure Ulcer - Premier per Clinical Advisor 0 1 2 3 Goal: Reduce Pressure Ulcers Occurrence
By Cost Center CC# CNL 0 0 0 0 0 0
Patient Falls - NDNQI Goal: Reduce Patient Falls
Total Falls/1000 Patient Days 2.4 2.9 1.8 3.3 4.1 2.5
By Cost Center CC# CNL 3.0 3.4 2.9 2.4 3.4 1.4
DVT Frequency - Premier per Clinical Advisor Goal: Reduce DVT Frequency
By Cost Center CC# CNL 7 3 1 1 0 1
Failure to Rescue - Premier per Clinical Advisor Goal: Reduce Failure to Rescue Frequency
By Cost Center CC# CNL 1 0 0 1 0 0
Catheter Associated UTI - NDNQI Goal: Reduce CAUTI Rate
Total CAUTI/1000 Patient Days N/A N/A 0 0 0 0
By Cost Center CC# CNL N/A N/A 1.33 0 0 0
Core Measure: Pneumonia Vaccine Goal: Decrease Missed Pneumonia Vaccine
By Cost Center CC# CNL 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Core Measure: Influenza Vaccine
By Cost Center CC# CNL 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Core Measure: HF 30 day Readmission Rate
By Cost Center CC# CNL 33.33% 0.00% 0.00% 0.00% 0.00%PCFs and CNLs - THR
• 14 wholly owned entities
• 124 budgeted positions
• 105 filled positions (March 2015)
• CNL Director is operational leader
• Resources are centralized and
deployed to entity.Academic-Practice Model
• Partnered locally with Texas Christian University.
– First cohort of CNL students began in fall of 2009.
– Two tracks:
• Advanced Practice nurses post masters’ certificate course.
• Generic CNL degree.
• TCU provides:
– CNL certification preparation and host testing.
– TCU provides philanthropic financial assistance to discount
tuition.
• THR covers costs for THR nurses through tuition reimbursement
and additional funding through THR’s Nursing Excellence Fund.Redesign of Case Management to Care Transitions Management
Care Transitions Management
• Take patient through the continuum, not just to the front door at
discharge
• Significant process variation through 13 hospitals
• Abolishment of monthly CTM lead meetingsCTM Department/Processes
Collaboration
Silos
• Refocus CTM Functions
- Moving patient through system, including post-acute
• Change Documentation Processes
– Ease of use
– Ease of real-time information finding
– Ease of metric retrieval
• Separate out UR-Denials/AppealsCare Management
Ownership Matrix
Function CTMs CNLs CR Facility
Nursing Admission Assessment o X
“Low-Risk” & No Transition Need Patients X
“Low-Risk” & Transition Need Patients X
“High-Risk” & Transition or No Transition Need Patients X
Readmission Assessment o X 0
Application of Readmission Risk Indicator (“RRI”) tool X
Initial Estimated Transition Date (“ETD”) X
Updated ETD, if necessary o X
Discharge Instructions and Summary of Care X
Concurrent Reviews o X
Registration X
Identification of PCP X o o
Post-Transition Planning X o
Health Decision Planning o X o
Daily Patient Care Briefings Facilitation o X o
KEY
X – Indicates primary responsibility o – Indicates a role in facilitating the process/functionCollaboration
Importance of the Role of the Unit Nursing Leaders
• Share information and set performance
expectations regarding the new
Communicator process for your Nursing staff
Nursing Initiative
Advocate Champion
• Act as “voice” for acute care
Nursing staff • Facilitate adoption of new processes
and inter-disciplinary collaboration for
your areaCare Transition Management
Implementation Timeline
HIGH-LEVEL IMPLEMENTATION PLAN FOR CARE TRANSITION MANAGEMENT
I M P L E M E N TAT I O N March 2014 April 2014 May 2014 June 2014 July 2014
Care Transition Management
M ILESTONES 3/24 3/31 4/7 4/14 4/21 4/28 5/5 5/12 5/19 5/26 6/2 6/9 6/16 6/23 6/30 7/7 7/14 7/21 7/28
Implementation
Implementation Timeline
System Wide IT
THP – 2 units
THSW – 4 units
THFW – 3 units
THK – 2 units
THD – 1 unit
THAL – 1 unit
THAZ – 1 unit
THHEB – 2 units
THC – 1 unit
THDN
THA
Dates to be determined – dependent on recruitment/hiring of CNLs in upcoming 2 months
THS
THAM
Key
Implementation Activities
Go-LiveCommunication/Education • CTM Documentation change before any roll out the units CTM Navigator CNL Navigator Superusers for each group • Physicians, Hospital Leaders, Nurse Directors/Managers informed of the overall initiative, education approach, and implementation approach • Charge Nurses and Direct Care Nurses educated through WBT; modules released (2-4 weeks prior to their unit go-live date) -- Supplemental Q&A sessions as needed using the CNLs/PCFs as Super Users to answer questions
Major Changes in Historical
Roles/Responsibilities
CTMs are both RNs and SWs
- No longer react to referrals, instead proactive stance.
- Each have a definite, discrete set of patients for which they are accountable.Required New Model
Components
• DCB (daily care briefing)
• Risk for admission
• ETD
• Transition Evaluation
• Completion of DC Plan
• PCP appointment
• Readmission evaluation, if applicable
• Post DC follow-up
• Regulatory complianceCritical Success Factor
The success of the daily care briefings process relies on recognition of the
interdependencies between all members of the Interdisciplinary Team.
Communication must be timely to improve the overall process.Daily Care Briefings
Daily Care Briefings Are…
• Brief (average of one minute per patient)
• Focused on patient progress and movement to transition, identifying any barriers and offering solutions
• A high-level review of each patient’s needs for the next 24 hours
• Led by a facilitator (i.e. Clinical Nurse Leader/Patient Care Facilitator/Charge Nurse/House Supervisor)
• Inclusive of various members of the interdisciplinary team who bring information pertinent to their role
Daily Care Briefings Are Not …
• Patient care rounds
• Shift report
• Teaching roundsDaily Care Briefing Questionnaire
Care Transition Manager
Daily Care Briefing Questionnaire – Care Transition Manager (RN & SW)
What is the patient’s payor source?
What is the appropriate patient status (IP, Observation, OP) and level of care (CC, Step-down, Acute, etc.)?
Does the patient continue to meet medical necessity criteria for current patient status and level of care?
What is the transition plan and plan progression for referred patients? Contingency plan(s)?
What are the patient transition needs/barriers (Financial, Psycho/Social, etc.) for referred patients?
Is this a high or low risk for readmission patient (based on RRP)?
What is keeping this patient in the hospital (medical necessity)?
What are the patient’s post-acute handover and follow-up care needs?
Communication by exceptionReadmit Risk Tool
• Use LACE + tool that is part of CareConnect/EPIC
• “Validated index to predict early death or urgent readmission after
hospital discharge using administrative data”
• Score (red/yellow/green) shows on census list and also in
patient banners
• GOAL: To reduce readmissions by collaborative team
action for high risk patientsPCP Appointment
• Within 3-7 days post acute care DC
• PCP, Free Clinic, Transitions House CallsPurpose of Assigning an
Estimated Transition Date (ETD)
• Ensures the patient has a smooth transition to the next care setting
• Provides a goal for the interdisciplinary team to work towards
• Enables proactive coordination of acute care services
• Provides clarity to the patient/caregivers about when the patient is going home so they
can prepare transportation and home arrangements
• Prevents clinical complications (i.e. nosocomial infections, pressure ulcers, general
debilitation, etc.)
• Prevents denials for unnecessary daysTransition Evaluation
Purpose
• Initial patient screening that will serve as the foundation for the Transition Plan
Who
• Unit Care Transition Manager (for referred patients)
When
• Occurs within 24 hours of receiving the CTM referral
• Transition planning begins upon admission and therefore the Transition Evaluation must be conducted early in the patient’s stay in order
to maximize health outcomes
How
• Using the standardized Transition Evaluation template in CareConnect
• Review ED CTM notes or previous acute stay notes to gather any pertinent information on patient background if ableMetrics • Readmissions • HCAPS scores/R/T Care Transitions • # of unique patients touched by CTM • # PCP appointments made • Completion of T.E./DC plan • Regulatory Compliance.
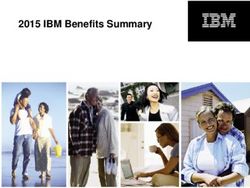
Average Length of Stay
Systemwide
Care Management Redesign Average LOS
All In-Scope Units - 24 month Trend
5.40
5.20 5.19
5.11
5.02
5.00
4.90 4.92 4.90 4.92 4.90
4.85 4.83 4.85
4.81 4.79 4.81 4.79
4.80 4.76
4.73
4.68 4.67 4.66 4.67 4.67 4.67
4.64
4.60
4.40
4.20
4.00
3.80
ALOS Mean UCL LCL Linear (ALOS)
Systemwide ALOS was calculated using all patients, all in-scope units, and all wholly owned entities (excluding THSH and THHVH). ALOS
analysis excludes inpatient rehab, psych, mother/baby, and expired patients.
Confidential And Proprietary – All Rights Reserved – For Internal Use Only Texas
Health Resources
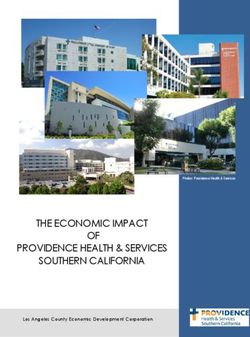
43Readmission Rate
Systemwide
Care Management Redesign Readmission Rate
All In-Scope Units - 24 month Trend
11.5%
11.0%
10.6%
10.5% 10.3%
10.0% 9.9% 9.9% 9.9%
9.7% 9.8%
9.7%
9.6%
9.5% 9.5% 9.4% 9.5%
9.5% 9.4%
9.3% 9.3%
9.3%
9.1%
8.9% 9.0%
9.0% 8.9% 8.9%
8.8%
8.5%
8.0%
7.5%
Readmit Rate Mean UCL LCL Linear (Readmit Rate)
All-cause readmission rates were calculated using total 1 – 30 day readmits as the numerator, and total all-cause, all-readmission cases as the denominator.
Includes all wholly-owned entities, excluding THSH and THHVHA.Clinical Review Data Trend
Systemwide
Systemwide Clinical Review Performance
24 month Trend
7.00%
6.00%
5.20% 5.19%
5.00% 4.89% 4.85% 4.85%
4.44% 4.47%
4.30%
3.99% 4.02% 4.01% 4.06%
3.89%
4.00% 3.70%
3.62%
3.47% 3.40% 3.47%
3.28% 3.26% 3.34%
3.18% 3.18%
3.00% 2.69%
2.00%
1.00%
0.06% 0.05% 0.07% 0.07% 0.07% 0.05% 0.05% 0.07% 0.09% 0.11% 0.14%
0.12% 0.09% 0.10% 0.10% 0.12% 0.11% 0.10% 0.05% 0.07% 0.07%
0.00%
Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14
% or Total IP Registrations with an initial Denial % or Total IP Registrations actually written-off
Mean UCL
LCL Linear (% or Total IP Registrations with an initial Denial)
Source: Executive Dashboard metrics; XNET PXPWC1 AND PXPWC2
Includes clinical and technical denials.
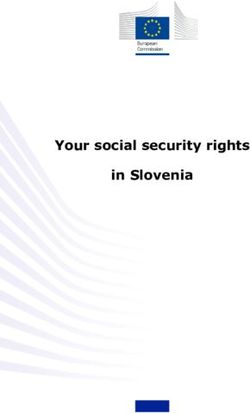
Includes all wholly-owned entities.HCAHPS – Care Transitions
Systemwide
Care Management Redesign HCAHPS Care Transitions
All In-Scope Units - 12 month Trend
64
61.8
62
61 61 60.9
90th %
60
58 57.3 57.2
Care Transitions Top
56.7 56.9
75th % 55.8
56 55.4
Box Score
53.7 53.9
54
THR
52 52.9 52.9
52.6
50th % 52.2
50
48
46
2014 Q1 2014 Q2 2014 Q3 2014 Q4
THR 50th %ile 75th %ile 90th %ile Linear (THR)HCAHPS – Nurse Communication
Systemwide
Care Management Redesign HCAHPS Nurse Communication
All In-Scope Units - 24 month Trend
88
85.6 85.7 85.6
86 85.3 85.3 85.2 85.3
84.4
84
90th % 82.7 82.5 82.5
Nurse Communication Box
82.3 82.3 82.4
82.1
82 81.4
75th %
79.5 79.7
80 79.3 79.4 79.4
79.1 79
78.3 79.5
Top Score
79
78 78.7
50th % 77.9
77.4 77.4
77
76
THR
75.6
74
72
70
2013 Q1 2013 Q2 2013 Q3 2013 Q4 2014 Q1 2014 Q2 2014 Q3 2014 Q4
THR 50th %ile 75th %ile 90th %ile Linear (THR)HCAHPS – Discharge Information
Systemwide
Care Management Redesign HCAHPS Discharge Information
All In-Scope Units - 24 month Trend
94
92 91.4 91.4
91.2 91.2 91.1
90.5 90.5
90.1
Discharge Information Top
90 89.4
90th % 88.8 88.7 88.7 88.8
88.1 88.2 88.4
88 87.5 88
86.7 86.5 86.7
75th %
Box Score
85.7 86.9
86 85.3 86.2 86.3
86 86.3
84.8
85.6
85.2
50th %
84
THR
83.2
82
80
78
2013 Q1 2013 Q2 2013 Q3 2013 Q4 2014 Q1 2014 Q2 2014 Q3 2014 Q4
THR 50th %ile 75th %ile 90th %ile Linear (THR)Implications for Future Care
Delivery
1. Accountable care
– CNL playing direct role in improvement workstreams with third party
payers for diabetes, CHF, pneumonia and AMI patients to improve
outcomes and reduce readmission on the inpatient units
– Continue to evaluate the use of the CNL role to coordinate care and
collaborate across three zones of hospitals and health care providers in
over 250 physician practice settings.
– Determine balance between using case managers, navigators, social
workers, coaches and other roles
– Continued innovation in care delivery models at micro-level2. Value based purchasing and Pay for Performance
– Retention of masters prepared generalists at the point of care and actively
engaged in patient management
– Focus of the CNL role is on patient advocacy and continuity
– CNLs lead and improve interprofessional team coordination and
communication
– CNLs directly intervene to prevent complications and assure appropriate
documentation of care
– CNLs can impact quality and performance outcomes
– CNLs promote evidence based care at the point of care and directly with
staff3. Cost containment and reduction
• Coordination of care to enhance the flow and delivery of services, reduction
in unnecessary work (or rework) and cost
• Partner with the nurse manager and leadership team to tackle operational
improvements at the point of care
• Provide direct feedback on staff effectiveness, staffing and care delivery
appropriateness and barriers to effective staff nurse performanceFuture Plans • Continued partnership • Development of options for CNLs to matriculate to DNP • Identification of new environments for CNL practice • Continued collaborative professional activities • Focus on disseminating value of CNL role through demonstration of enhanced patient outcomes
Questions & Discussion
"Vision without execution is hallucination.”
— Thomas Edison
Dr. Paula Spears: paulaspears@texashealth.org
682-236-6205
Darla Banks: darlabanks@texashealth.org
682-236-7146
Sherry Petrillo: sherrypetrillo@texashealth.org
682-236-6749You can also read