Terapia anticoagulante Update 2023 - Marco Rebecchi, MD Aritmologia Clinica ed Interventistica
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Terapia anticoagulante
Update 2023
Marco Rebecchi, MD
Aritmologia Clinica ed Interventistica
Policlinico Casilino, Roma
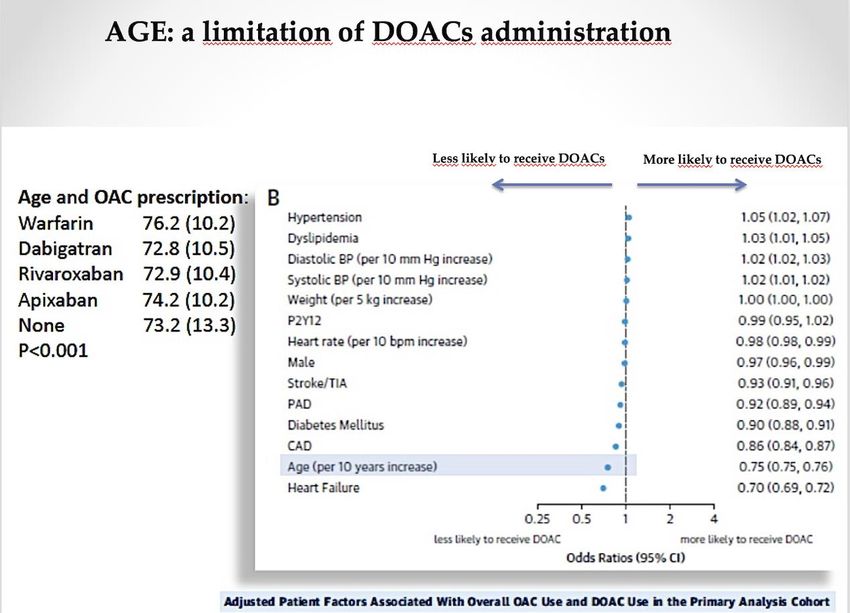
ofAnalysis
NOACs, many
of data from patients
global and at riskobservational
European prospective, of stroke do
registries
nothasreceive OACs
shown an increasing uptake of NOACs, but many patients with AF who
are at risk of stroke do not receive OACs 1–4
GLORIATM-AF (10 675 patients)1 GARFIELD-AF (17 475 European patients)2
GLORIA™-AF (% receiving)
20% 31%
VKA 32.3 Anti- Anti-
Dabigatran 32.2 Receiving OAC
thrombotic thrombotic
rivaroxaban 12
treatment treatment
Apixaban 3.5
ASA 11.5 at baseline Not receiving OAC at baseline
AP (not ASA) 0.9
none 7.6
other 0.1 80% 69%
Similar proportions of patients did not receive OACs in
the PREFER in AF (17.7%) and EORP-AF (20.0%) registries3,4
1. Huisman MV et al. Am J Med 2015; 2. Camm AJ et al. Poster P85323, ESC 2015; 3.
Kirchhof P et al. Europace 2014;
4. Lip GHY et al. Europace 2014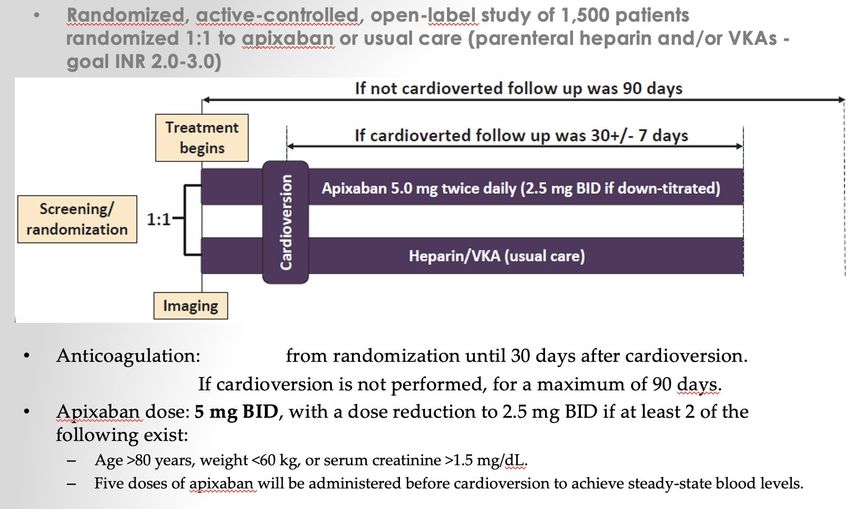
The perfect Anticoagulant STROKE PREVENTION BLEEDING RISK
Kidney and DOAC
Still an actual
problem?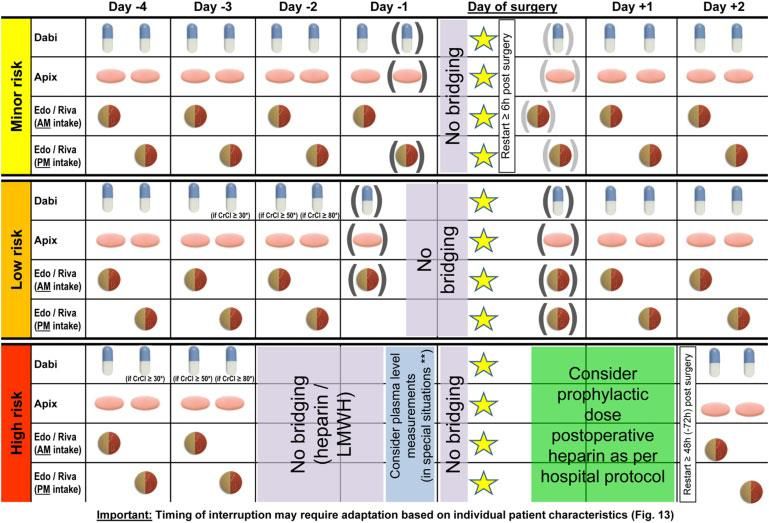
30% 80%
50%
70%
50%
20%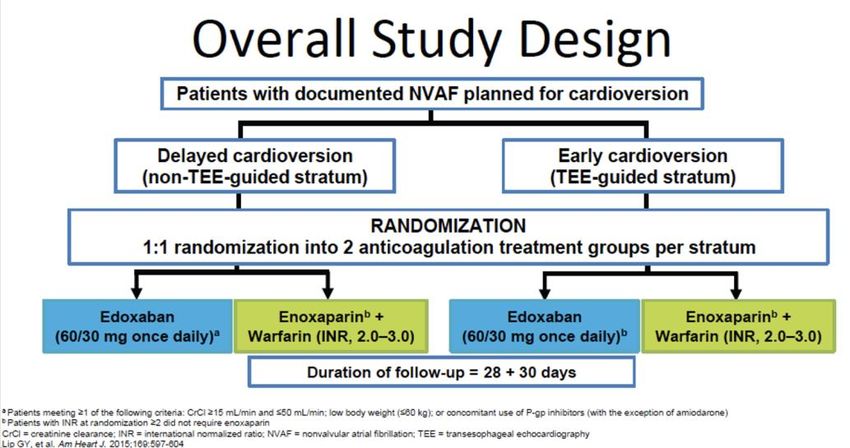
Many patients with mild-to-moderate CKD (i.e. CrCl 30 – 89 mL/ min) have been enrolled in the NOAC trials.
Data from Phase III trials in patients with moderate renal
impairment (CrCl 30–49 mL/min)
Stroke and systemic embolism
Study drug Warfarin
HR
(%/yr) (%/yr)
RE-LY®:
1.52 2.78 0.55
Dabigatran 150 mg*1,2
RE-LY®:
2.15 2.78 0.77
Dabigatran 110 mg*1,2
ROCKET AF: Rivaroxaban3 2.95 3.44 0.86
ARISTOTLE: Apixaban*4 2.11 2.67 0.79
Efficacia dei NOACS
indipendentemente dalla IR
moderata, soprattutto il Dabigatran 0.5 1 1.5
Favours NOAC Favours warfarin
150 riduce del 45% il rischio di ictus!!
*Includes patients with CrCl
RE-LY®: analisi di sottogruppo per funzionalità renale
– pazienti con CrCl= 30-50 mL/min
Ictus ed embolia sistemica
Trattamento Warfarin
HR*
(%/anno) (%/anno)
Dabigatran 150 mg 1.52 2.78 0.55
Dabigatran 110 mg 2.15 2.78 0.77
0.5 1 1.5
A favore di Dabigatran A favore di warfarin
Sanguinamenti maggiori
Trattamento Warfarin
HR*
(%/anno) (%/anno)
Dabigatran 150 mg 5.44 5.41 1.01
Dabigatran 110 mg 5.29 5.41 0.98
0.5 1 1.5
A favore di Dabigatran A favore di warfarin
HR = hazard ratio; *= 95% intervalli di confidenza
Connolly S et al. NEJM 2009; 361:1139–51; Eikelboom J et al. Circulation 2011;123:2363–72JASN 2011
Significantly less decline in renal function in patients treated with dabigatran
vs warfarin
Dabigatran 110 mg Dabigatran 150 mg
BID BID Warfarin
Mean decline from baseline in
0
-1
GFR* ± SE
-2
-2,57 -2,46
-3
-3,68
-4
-5
P=0.0002
P=0.0008
Post hoc analysis of renal function in RE-LY® showed significantly lower mean
decline in GFR over 30 months with dabigatran vs warfarin
*According to the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation
Böhm et al. ESC 2014EHRA UPDATE 2018 AND EHRA UPDATE 2021
Creatinine
≥ 1.5 mg/dL
Weight ≤ 60 Kg Weight ≤ 60 Kg
Age ≥ 80 y
≤DOACs in with AF and with ESRD on hemodialysis
The 1-year rates for major or clinically relevant
nonmajor bleeding were 32% and 26% in apixaban
and warfarin groups, respectively (hazard ratio,
1.20 [95% CI, 0.63–2.30]),
1-year rates for stroke or systemic embolism
were 3.0% and 3.3% in apixaban and warfarin
groups, respectively.
Clinically relevant bleeding events were ≈10-fold more frequent than stroke or systemic embolism
among this population on anticoagulation, highlighting the need for future randomized studies
evaluating the risks versus benefits of anticoagulation among patients with AF and end-stage kidney
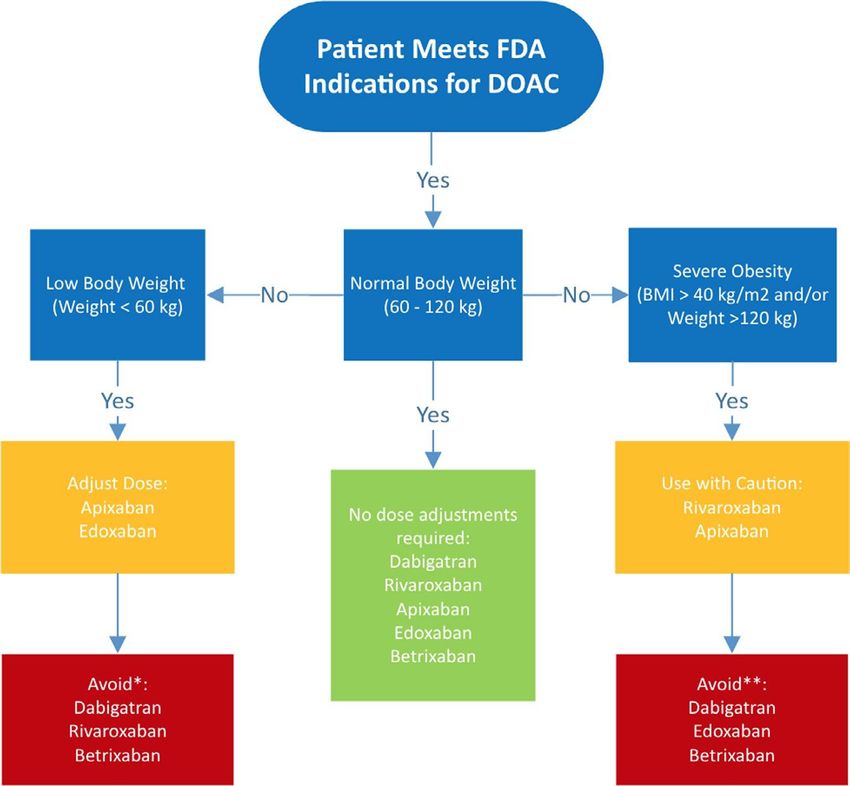
disease on hemodialysis.DOACs Distribution volume
Evaluation of Higher dose edoxaban regimen (HDER) in several setting of GFR (30 mg in GFR
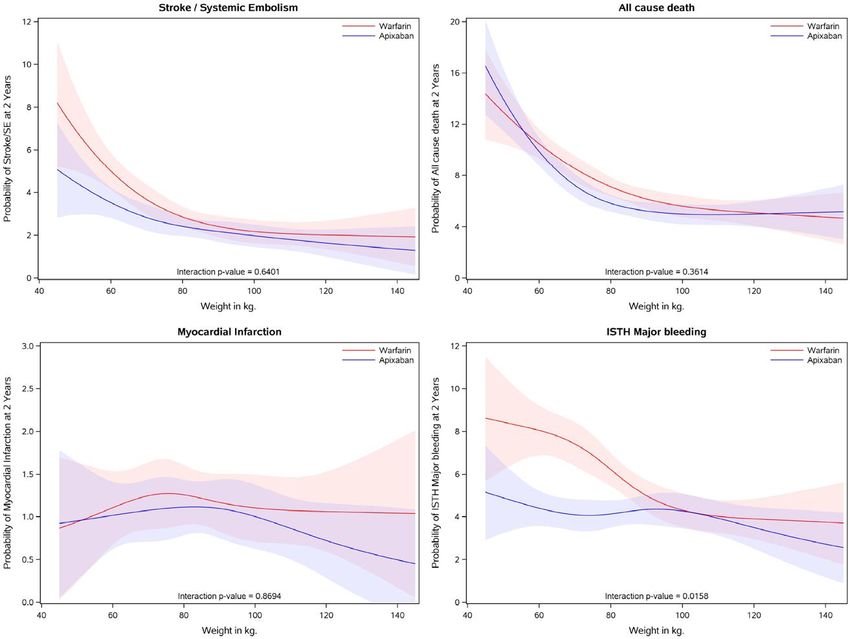
……apixaban is efficacious and safe across the spectrum of weight, including in low- (≤60 kg) and highweight patients (>120 kg). The superiority on efficacy and safety outcomes of apixaban compared with warfarin persists across weight groups, with even greater reductions in major bleeding in patients with atrial fibrillation with low to normal weight as compared with high weight. ………….Thus, apixaban appears to be appropriate for patients with atrial fibrillation irrespective of body weight
DOAC in under and overweight patients
2020
When is raccomanded a dose optimization Pharmacological interactions
Follow up
Proposed Blood sampling
Beginning DOAC
Blood count, creatinine, total and
fractionated bilirubin, AST / ALT, GGT
3 ms 6 ms-12 ms
Age >75 y, CKD, Fragile pts Stable pts
Blood count, creatinine, total and Blood count, creatinine, total and
fractionated bilirubin, AST / ALT, GGT, iron fractionated bilirubin, AST / ALT, GGT, iron
serum levels serum levelsDOACs
&
Non cardiac
surgery2022 2018
AF Ablation
DOACs
&
Electrical CVAfib CV in NOACs trials
Limited data
ROCKET AF: similar data in both study arms (VKA and
Rivaroxaban) patients undergone ablation and CV in
terms of long term stroke rates and survival
RE-LY: Dabigatran had similar rates of stroke/SE and
major bleeding compared with warfarin within 30 days
of cardioversion (about 600 pts)
ARISTOTLE: Apixaban and warfarin had similar rates of
major cardiovascular events after cardioversion (540
pts)Imaging and Doacs (results from Emanate-Apixaban)
• Thrombus identification in left atrial appendage in 61
pts. Every patient continued anticoagulation therapy.
Non events occurred
• Among pts undergone to a new TEE (37±11days),
thrombus regression has been found in:
-52% of apixaban arm
-56 % of Eparin/VKA armDOACs for thrombus therapy
Resolution rate (most pts in VKA therapy): 55%-90%
Study Study design, location LA/LAA thrombus resolution rate*
% n/N
Collins et al, 19951 Observational, US 86.0 12/14
Corrado et al, 19992 Observational, Italy 81.8 9/11
Jaber et al, 20003 Single-centre observational, US 80.0 129/161
Seidl et al, 20024 Single-centre observational, 55.0 30/55
Germany
Akdeniz et al, 20055 Observational, Turkey 63.6 7/11
Saeed et al, 20066 Single-centre observational, US 90.0 (LMWH) 18/20
Hammerstingl et al, Single-centre, Germany 18.0 9/50
2015 ACC7 58.0 (NOACs) 18/31
*Receiving VKA therapy unless otherwise specified
1. Collins LJ et al, Circulation 1995;92:160–163; 2. Corrado G et al, Chest 1999;115:140–143;
3. Jaber WA et al, Am Heart J 2000;140:150–156; 4. Seidl K et al, J Am Coll Cardiol 2002;39:1436–1442;
5. Akdeniz B et al, Int J Card Imaging 2005;98:49–55; 6. Saeed M et al, Int J Cardiol 2006;113:401–406;
7. Hammerstingl C et al, Poster Presented at: ACC Scientific Sessions 2015X-TRa Study Design
• X-TRa was a prospective, single-arm, multi-centre study
Rivaroxaban 20 mg od Standard of care
Patients with non-valvular
(CrCl 15–49 ml/min: 15 mg od)
AF or atrial flutter with a
LA/LAA thrombus detected
on a TEE 6 weeks 30 day follow-up
EOT TEE End of
Treatment assignment (baseline)
(outcome evaluation) follow-up
• Primary outcome variable: complete LA/LAA thrombus resolution rate
confirmed by the 6-week EOT TEE
1. Lip GYH et al, Am Heart J. 2015;169:464–471Results
X-TRA: resolved or reduced clot resolution in 60% of patients
70% 60,4%
Percentage of patients (95% CI)
(46.0–73.6)
60%
50% 41,5%
(28.1–55.9)
40%
30%
20%
10%
0%
Complete thrombus Resolved or reduced
resolution thrombus
1. Lip GYH et al, Am Heart J. 2016;178:126–134
L.IT.MA.01.2017.2142 AD ESCLUSIVO USO DEL MEDICALCLOT- AF Study Design
• European regional, multi-centre, retrospective, non-interventional study
Retrospective
Registry design*
Start of observational 3–12 weeks Data collection
period follow-up (May 2013–
May 2014)
3–12 weeks SOC
anticoagulation therapy
Per patient
TEE-confirmed diagnosis EOT TEE#
of LA/LAA thrombus
*FPFV = 1 January 2010; LPFV = 31 December 2012; LPLV = 31 March 2013; #if no EOT TEE was performed, the observational
period ended at 12 weeks after diagnosis at the latest. If more than one TEE was performed during treatment the thrombus
outcome was collected from the last TEE performed within 12 weeks of treatment start
Lip GYH et al, Am Heart J 2015;169:464–471
L.IT.MA.01.2017.2142 AD ESCLUSIVO USO DEL MEDICALThe thrombus resolution rate (62.5%) was
similar to results seen previously (55–90%)
80%
68,0%
Percentage of patients (95% CI)
70% 62,5% (53.3–80.5)
(52.0–72.2) 56,5%
60% (41.1–71.1)
50%
40%
30%
20%
10%
0%
All patients Eastern Europe Western Europe
Reported thrombus resolution
1. Lip GYH et al, Am Heart J. 2016;178:126–134
L.IT.MA.01.2017.2142 AD ESCLUSIVO USO DEL MEDICALIf a thrombus persists during follow-up despite confirmed good ad-herence to the NOAC regimen an individualized management strategy is required. This may include switching to a different type of NOAC or INR-tailored VKA-therapy. Some centres have reported LAA closure in patients with a persistent thrombus. Finally, long-standing thrombi may become organized and fixed, allowing cardioversion if regaining sinus rhythm is considered to be of substantial benefit for the patient……….
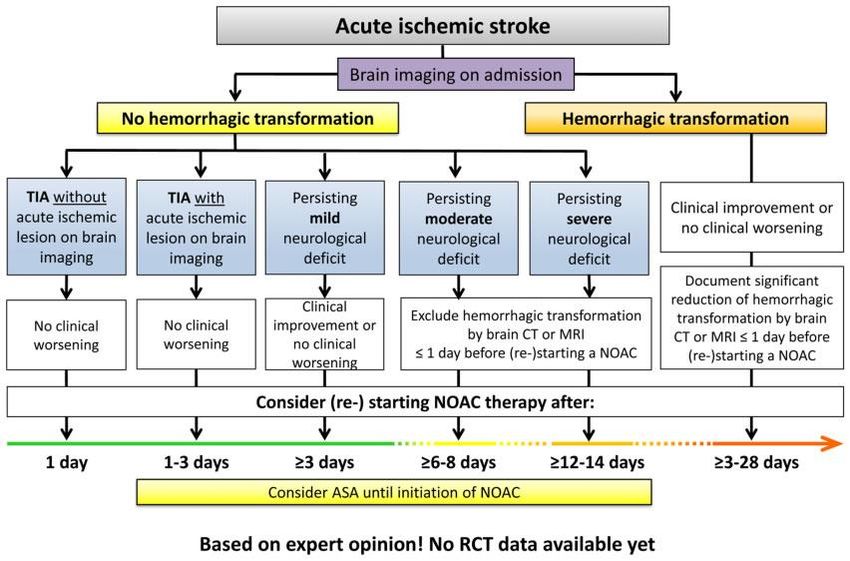
Stroke during Doacs Therapy Time of DOAC restarting? Changing DOACs?
66 y, male
GFR 85 ml/min, Weight: 80 kg
2021: 1 AF episode (September 2021)Apixaban 5 mg/bid
2022: 1 AF recurrence (March 2022)
4 episodes of profuse nosebleeds with the need for nasal swab but non indications to surgery
--Rivaroxaban 20 mg---new nosebleed recurrence
General doctor: STOP DOAC (Rivaroxaban 20 mg)Enoxaparine 6000/die
Change DOAC?
In office clinical visit May 2022: what solutions
Reduced dose?66 y, male
GFR 85 ml/min, Weight: 80 kg
2021: 1 AF episode (Dicember 2021)
2022: 1 AF recurrence (March 2022)
CHa2DS2 Vasc Score: 2 (Hypertension, Age)
Rivaroxaban 15 mg/die
(an off label choice?)Scegli sempre il cammino che sembra il migliore anche se sembra il più difficile: l’abitudine lo renderà presto piacevole. (Pitagora)
Ricordiamoci sempre di somministrazione
THE HIGHER DOSE
…Cioe’ non la piu alta quantitativamente
, ma la migliore per quel paziente…
Altrimenti saremo
Off LABELYou can also read