Surge - FALL 2021 hopkinschildren's - Johns Hopkins Medicine
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
hopkinschildren’s
FALL 2021 THE JOHNS HOPKINS CHILDREN’S CENTER MAGAZINE
The
Second
Surge
How did critical care
specialist Meghan Bernier
The Draw of Pediatrics
Residents and veteran
physicians share what
attracted them and
and other staff manage the how they’ve evolved.
pandemic, themselves and each
other, the second time around? Photo Journal
Kids giving back in
surprising ways.
FamilyMatters
As Always,
Supporting Families
“WHAT I WISH YOU KNEW” is a catch because of the pandemic. We joked that
phrase used often over the last 11 years this was likely the “Last Supper.” Little
by parent members of the Pediatric did we know then! But COVID-19 by Sue Mead,
Family Advisory Council (PFAC). We didn’t stop the council from continuing Parent Advisor
find that message even more important to assist both staff and families. We did
now, as we continue to search for effec- our best to support staff with food and
tive ways to support families during the snacks, while volunteering at the ware-
COVID-19 pandemic. house to help make face shields, bottle
Interestingly, the realities
Interestingly, the realities of living hand sanitizers and fold reusable heavy of living during a pandemic
during a pandemic are not unlike what gowns.
are not unlike what our
our families deal with while caring for a As the months wore on, we soon
critically ill child in the hospital: different realized how difficult it was for only one families deal with while
circumstances, yet similar feelings. Each parent to be permitted at the bedside. caring for a critically ill child
day, we receive new insights, but often, We tried to decrease their social isolation
there are no concrete answers. There’s by introducing activities like parent in the hospital.
worry, fear, exhaustion, added expenses bingo on Tuesdays via CCTV, hoping On Thursdays we continued our free
and isolation. Yet, like these brave fami- to provide a little entertainment and meals for parents program, providing
lies, we keep pushing forward and gain distraction — not to mention gift-card individually packaged lunches from local
strength as we confront this crisis. prizes. Similarly, an artist-in-residence restaurants. We helped to orchestrate
It was only a little more than a year ago Child Life specialist now works with virtual town halls from every pediatric
when, as we served our traditional Thurs- parents on art projects to engage them division, so that patients and families
day night meal to Children’s Center in a medium that can help them process could hear directly from our physicians
families, the governor held a press confer- what they are going through and about COVID-19, its effects and how
ence to announce the closure of schools normalize their lives (see page 60). to protect themselves. We also launched
a food pantry in the Pediatric Intensive
Care Unit and in Oncology to provide
Family inspiration boards, like this
one in the pediatric intensive care grab-and-go meals and snacks, so that
unit, help to calm parents’ worries, families don’t have to leave the unit to
fears and isolation.
purchase food or to feed family at home.
All Johns Hopkins Family Advisory
Councils continue to meet monthly via
Zoom — with better attendance than
ever. We continue to advise and offer
feedback about visitation, marketing and
patient education surrounding COVID-
19 and the vaccine. We have also created
our own social media page for families to
follow while they’re in the hospital. That
way, they can receive daily updates on
special virtual activities on CCTV. In the
spirit of “What I wish you knew,” we
continue to solicit ideas from parents to
support them and their families, espe-
cially during this difficult time. Please let
us know your ideas, too. Thank you.
H O P K INS C H IL D REN’ S | hopkinschildrens.org
FALL 2021
42 Organ Transplant Surgeon Betsy King
The daughter of a bricklayer, King knew since childhood that
she wanted to do something with her hands. Little did she
know it would be saving the lives of children D E P A R T M E N T S
needing new kidneys and livers. 2 Directors’ View
Aiming for Health Equity
F E A T U R E S T O R I E S 3 Spotlight
Pediatric Chaplain Matt Norvell
4 The Second Surge
This time staff faced more 16 Photo Journal
Kids Giving Back: Patients and their Fundraisers!
daunting challenges and greater
stress. How did they do? 32 Pediatric Rounds
Mat Edelson Treating Obesity Related Hypertension
A Sly Spinal Cord Tumor
22 T
he Draw of Pediatrics
A Nursing Trifecta
Bridge Builder John Campo
What attracted them to taking
care of children and how they’ve 46 Research Roundup
evolved doing so. Reducing Readmissions for Nephrotic Syndrome
A Game-Changer Grant for Managing MIS-C
Karen Blum
50 People & Philanthropy
Play Games, Heal Kids
A Giant Impact
Radiothon: The Show Goes On
60 In Memoriam
Cover photo: Keith Weller
FAL L 2 02 1 1
The Directors' View
Aiming for Health Hopkins Children’s is published
by the Johns Hopkins
Equity
Children’s Center Office of
Communications & Public Affairs
901 S. Bond St., Suite 550
It has been quite a year. In addition to grappling with racial injustice Baltimore, MD 21231
and increasing urban unemployment and poverty — among other hopkinschildrens.org
stressors — we and our patients and families have faced a pandemic 410-502-9428
that has claimed half a million lives in this country. Children have
not gotten as sick as adults, but, as Pediatric Hospital Medicine Shannon Ciconte
Division Director Eric Biondi noted this winter, “We can no Senior Director,
longer say that children are not affected by COVID-19.” Read “The Interactive Marketing
Second Surge” feature story in this issue (pages 4-15). Gary Logan
Similarly, issues such as racial disparities have motivated us to work Editor
harder to ensure health equity for all of our patients. That means
promoting equal access to health care and, especially during these Helen Grafton
times, providing vaccines against COVID-19. Another concern Molly Saint-James
is the need for greater awareness by our staff about unconscious Assistant Editors
discrimination in working with our patients and families — as well
Cozumel Pruette, m.d.
as each other. See our interview on implicit bias with Maria Trent,
Medical Editors
chief of the Division of Adolescent and Young Adult Medicine, and
her colleagues (pages 30-31). Waun'Shae Blount
Being aware of how we as pediatricians communicate with our Karen Blum
patients and their families, colleagues and staff is one trait of a Julie Weingarden Dubin
superb pediatrician. Compassion, curiosity, empathy — seeing Mat Edelson
medicine through the patient’s lens — are equally vital attributes. Leslie Feldman
How do we support these goals? Learn what pediatricians Barry Christina Frank
Solomon, Hoover Adger and Nicole Shilkofski, among Rachel Hackam
others, have to say on the subject, in “The Draw of Pediatrics” Amanda Leininger
(pages 22-29). Michael E. Newman
An innovative mind is yet another characteristic we aspire to — Contributing Writers
and remains at the heart of much of what we do here. Whether
through the delicate resection of a spinal cord tumor with Rachel Sweeney
neurosurgeon Alan Cohen or the building of a new congenital Graphic Designer
heart center with cardiac surgeon Bret Mettler, cardiologist Kathryn Dulny
Shelby Kutty and intensivist Jamie McElrath Schwartz, Keith Weller
we continue to advance care for children (see “Pediatric Rounds” Photography
pages 32-45).
Printed in the U.S.A.
Thank you, and enjoy this issue. ©The Johns Hopkins University 2021
Margaret “Maggie” Moon, M.D., M.P.H.
Co-Director and Pediatrician-in-Chief,
Johns Hopkins Children’s Center Give us feedback
Send letters to Gary Logan at
the above address, or email
glogan@jhmi.edu.
For more information
David Hackam, M.D., Ph.D. To read more on the clinical services and
Co-Director and Surgeon-in-Chief, Johns programs covered in Hopkins
Hopkins Children’s Center Children’s, visit hopkinschildrens.org.
How you can help
Call 410-361-6493
2 H O PK INS C H IL D REN’ S | hopkinschildrens.org
Spotlight
Pediatric Chaplain
Matt Norvell
Following training, he sought a
place where the pace was fast
and the stakes higher.
by Julie Weingarden Dubin
M
att Norvell pulls into the hospital in 2007 as a chaplain resident in pediatrics, Norvell had to make such connections
parking garage during the early and he was then hired as a pediatric in new ways: Walking the halls and
morning and receives a page: palliative care support specialist. When making eye contact above all the masks.
A young patient unexpectedly went into funding came through for a Department Comforting patients by talking by phone
surgery and the mother is crying, afraid of Pediatrics chaplain, he landed the job through glass doors. Sending the entire
that her child may not survive. Norvell sits following a national search. staff weekly inspirational emails to ease
for hours with her in the surgical waiting In addition to supporting patients and anxiety.
area, reminding himself this is why he families, Norvell tends to the spiritual and “Most of the world was being told to stay
chose to become a minister and pastoral emotional health of Children’s Center staff home and health care workers were told to
counselor. members: “A challenge for health workers come to work,” says Norvell. “That worry
“In high school, people said I was a taking care of sick, vulnerable children, of putting their lives and their families at
really good listener and that shaped me,” is there isn’t a place built into their risk layered on top of trying to teach kids
he says. “A piece of my inspiration toward professional role to deal with emotions.” at home, see a sick parent and somehow
professional ministry was the desire to Norvell lets them know that he’s find toilet paper, was too much.”
be with people and understand their available when they need to talk. If the One resource for staff is the RISE
relationship with themselves, with other stress they face isn’t addressed, Norvell says, (Resilience in Stressful Events) program,
people and with God.” there may be consequences that interfere co-developed by Norvell. It provides
Norvell was always drawn to the one- with their mental health and their ability emergency psychological and emotional
on-one counseling of ministry, but he to do their job. first aid to employees — if something
found through his early intern work that goes wrong with a patient and the staff
the pace and intensity of the medical world member doesn’t want to talk about it with
was a better fit. “When you get a call in coworkers, the employee can talk to a peer
the hospital, there’s an acute need to help A challenge for health responder.
someone, where in a church setting it’s “When COVID hit, RISE went from
more sporadic,” says Norvell, pediatric
workers taking care of sick, about four calls a week in January to 30
chaplain at Johns Hopkins Children’s vulnerable children, is there calls a week March through May,” says
Center. isn’t a place built into their Norvell. “RISE is now in 65 hospitals
Why the focus on children and their across the country.”
families? “The stakes feel a little higher
professional role to deal For his own emotional stability, Norvell
working with sick kids,” he says. “Nobody with emotions. focuses on his family and hobbies like
ever says, ‘He lived a good life’ when a kid gardening, golf and bluegrass jam sessions.
dies. It’s always a bad thing.” “They tell me they haven’t slept because “When I’m playing the banjo,” he says, “I
Norvell received a Master of Divinity of stress,” he explains. “I say, ‘Dude, this can immerse myself in the music and not
from Duke Divinity School and a Master is a real thing. You should pay attention think about health care or COVID.”
of Pastoral Counseling from Loyola to this.’”
University. He started at Johns Hopkins When the pandemic hit, however,
FAL L 2 0 2 1 3
Facing the
Second
Surge
BY MAT EDELSON
4 H O PK INS C H IL D REN’ S | hopkinschildrens.org
Pediatric infectious disease specialists
Anna Sick-Samuels and Aaron Milstone.
“SUDDENLY WE WERE WORKING 100-HOUR WEEKS FOR SIX STRAIGHT WEEKS
IN THE COMMAND CENTER, BECAUSE IN THE FIRST WAVE PROVIDERS WERE
SCARED. THERE WAS SO MUCH TO FIGURE OUT ON THE FLY—THINGS LIKE
HOW TO TEST PATIENTS COMING INTO THE HOSPITAL, WHAT KIND OF PPE
WORKED BEST, ANYTHING AND EVERYTHING REGARDING INFECTION SPREAD.”
— AARON MILSTONE
FAL L 2 0 2 1 5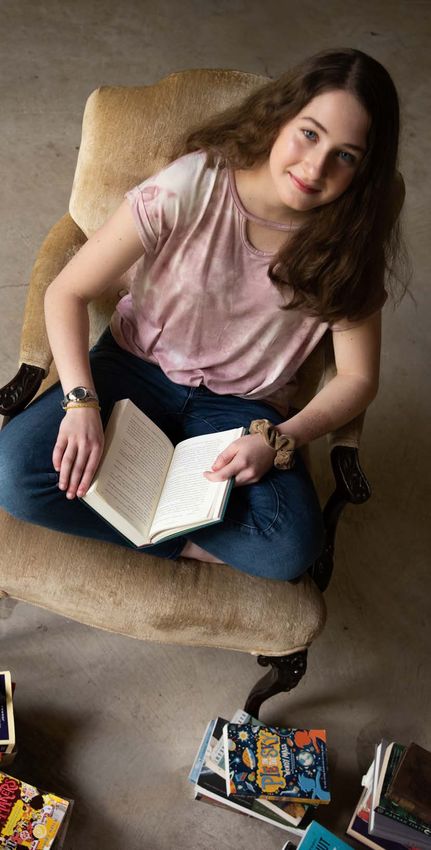
This was
definitively
not a drill.
In early March 2020, the newly formed dren’s Center to remain open and care into the pandemic’s
Incident Command Center at Johns for patients, staff and the community as vortex like wind being
Hopkins Children’s Center (JHCC) the second surge of COVID-19 engulfs sucked through a jet engine.
convened for the first time. After nearly Baltimore. This dynamic tension between sharing
three months of rumors, chatter and precious resources serving the highly
terrifying news reports, SARS-CoV-2, impacted adult population while still
H
the virus that causes COVID-19, had ow does one describe the carrying out the Children’s Center’s
made the 7,573-mile journey from unprecedented 18 months mission to safely treat children is the
Wuhan, China, to Johns Hopkins’ since the pandemic assaulted continuing through-line in this tale. It
front door. Charm City? For the staff — and we is a story of great self-sacrifice, a shelv-
The mood in the Command Center talked with more than 20 for this story ing of egos, and a marshaling of talents
was concern tinged with fear; the scene, — there’s the daily dichotomy of liv- and skills that have so far met — and
frankly, a bit chaotic. Some in the ing inside a plague of seemingly bibli- perhaps even stayed a step ahead — of
overcrowded small room wore masks, cal proportions. They’ve been awed by the greatest medical emergency Johns
others did not. Open platters of food their fellow staff members, describing Hopkins has ever faced.
were scattered about the conference them as “heroic,” “brilliant,” “creative” On a functional level, there have
table, as if this was just another catered and “innovative.” But individually, been huge alterations in day-to-day
meeting. With little official guidance they admit to feeling “frustrated,” “ex- operations. Part of the pediatric inten-
yet on what to do — this was before hausted,” “soul-crushed” and “help- sive care unit (PICU) was retrofitted
the words “physical distancing” and less,” from the experience. to admit and care for adult patients
“mask” became as ubiquitous as “um” Even as vaccines reach outstretched with COVID-19. Necessary nega-
— everyone was ad-libbing, and no one arms across Johns Hopkins, the fin- tive pressure rooms for patients with
was pleased. Said one participant, “We ish line remains hazy. Virus variants COVID-19 were built nearly over-
were all looking at each other like ‘this muddy the view as death tolls climb night. Telemedicine (Zoom-like video
doesn’t feel OK.’” well past the half-million mark na- outpatient consults with patients and
But from this initial tumult emerged tionally, with more than 8,000 dead families in their homes) soared. A
a coordinated effort unprecedented in in Maryland. Fortunately, childhood scarce resources allocation group was
the Children’s Center’s history. Hun- deaths make up a very small percentage convened to ensure all staff had proper
dreds of faculty and staff united to solve of that number, but that doesn’t mean PPE (personal protective equipment).
daily crises. In a time calling for the ul- pediatric staff have sat on the sidelines Child Life expanded from the bed-
timate in fluidity and flow, the can-do during the crisis. side to the car side, developing coping
spirit that has so often permeated the Far from it. Because of its physical plans that nurses could use to comfort
walls of Johns Hopkins led to a “get ’er and institutional connection to the anxious children as they got tested for
done, titles-be-damned” mentality. adult side of Johns Hopkins Medicine, coronavirus in drive-up sites. Work
And it paved the way for the Chil- the Children’s Center has been pulled schedules were revamped when the
6 H OP K I NS C HILD REN’ S | hopkinschildrens.org
Rebecca Trexler, (left), project
administrator for patient- and family-
centered care, and pediatric nurse
Cathy Garger went beyond their
traditional roles to communicate “need
to know” COVID-care updates to staff.
governor banned elective procedures Yet those same distancing policies, daily to make decisions,” says Maggie
for roughly two months beginning last and the social isolation they impose, are Moon, co-director of Johns Hopkins
March. Even pediatric medical resi- difficult to bear for months on end for Children’s Center, “but a big part was
dents felt the impact, deploying into patients, families and staff. Not surpris- informing everybody affected by those
adult care across Johns Hopkins. In the ingly, calls from staff to Johns Hopkins decisions to help them anticipate and
Children’s Center, overseeing it all was RISE (Resilience in Stressful Events) feel engaged and confident about what’s
its Incident Command Center, which teams have soared, as has outreach to coming next as much as anyone else.”
met daily for weeks, coordinating the pastoral care and other psychological Between in-person and Zoom at-
crisis and pumping out a steady stream services. tendees, several dozen people often
of science-solid information to an un- In other words, everyone’s helping, took part in the daily briefings, includ-
derstandably uneasy staff. and everyone’s hurting. ing division heads, charge nurses and
And make no mistake — keeping top administrators. Even for those
the staff safe and healthy, both physi- with previous disaster training, this
I
cally and psychologically, has been as t ’ s not an overstatement to was suddenly the real deal unpredict-
daunting as maintaining premium stan- say that in the first days of the pan- ably unfolding in real time. As one fac-
dards of patient care. In the first surge, demic, people were desperate for ulty member put it, “COVID was like
nearly 100 staff members tested positive information. With treatment and PPE playing whack-a-mole, where stuff just
for COVID-19, but that number has protocols and the Centers for Disease pops up and we all had to jump on it.”
dropped drastically as the Children’s Control and Prevention recommenda- Each day’s briefing included a COVID
Center successfully created a “bubble” tions changing sometimes hourly, get- case and PPE count, along with robust
environment. By instituting a one- ting up-to-the-minute info to the front discussions of how to put out the latest
parent visitor policy, and urging non- lines was critical. That task fell to the COVID-related brush fires. Recording
front-line staff to work at home when JHCC Incident Command Center. “A and distilling all that conversation into
possible, the Children’s Center feels crisis situation requires an all-hands- easily digestible all-staff emails and texts
like an awfully quiet but far safer place on-deck community where everybody fell to Cathy Garger and Rebecca
these days, at least when it comes to has a voice, and the Incident Com- Trexler. As was common with many
COVID spread. mand Center got people together staff during the crisis, Garger, a pedi-
FAL L 2 0 2 1 7
“IT’S A MOMENT IN
TIME WHEN A GROUP
OF PEOPLE IDENTIFY A
SUDDENLY EMERGING
PROBLEM AND RAPIDLY
COMBINE BRAINPOWER
TO FREELANCE A
SOLUTION. TEAMING
THRIVES ON TRUSTING
YOUR TEAMMATES AND
IMPLEMENTING RAPID
ITERATIONS.”
–DANIEL HINDMAN
atric nurse with disaster-coordinating starting asymptomatic COVID testing calls “teaming,” borrowed from the
experience, and Trexler, the project for hospitalized patients every seven book Teaming by Amy Edmonson.
administrator for patient- and family- days of their stay, and another Power- “It’s a moment in time when a group
centered care, went beyond their job Point featuring pediatric infectious dis- of people identify a suddenly emerging
descriptions to take on these crucial ease specialist Anna Sick-Samuels problem and rapidly combine brain-
communications duties. Trexler’s daily explaining the workings and studies of power to freelance a solution,” says
email (it’s now weekly) covered the the then-just-approved Pfizer vaccine. Hindman, who practices mostly at
basics for staff: negative pressure room This regular messaging is helping to Johns Hopkins Bayview Medical Cen-
bed availability, ICU COVID cases, keep everyone on the same page, says ter. “Teaming thrives on trusting your
the latest advice from the Hospital Moon. “The feedback I was getting teammates, and implementing rapid
Epidemiology and Infection Control from staff is that, if the rules change iterations. And when you don’t have
(HEIC) team, hospital COVID-care from yesterday to today, it’s unjustifi- an option to wait around, you decide
resources and contact info to reach the able to ask people to work in the dark; to do something knowing it won’t be
Command Center. “We were seek- the staff all said, ‘we’ll do anything we perfect, (then) figure out what doesn’t
ing consistent messaging and narrow- need to do to make this right, but we work, then try it again with some modi-
ing the info to ‘here’s what you need need to know what to do, and we need fication and keep doing that.”
to know that’s happening during the to know why.’” This idea of teaming spread through
surge,’” says Trexler. pediatric staff nearly as fast as the pan-
T
In time, Trexler’s notes, vetted by here’s an old saying, perhaps demic. It’s a delicate balance. Ethi-
Moon, have become a one-stop CO- apocryphal, that in crisis comes cally, one can’t improvise to the point
VID-awareness shop cutting through opportunity. The COVID cri- that care is compromised. But in the
the numbing amount of emails com- sis stripped Hopkins’ bureaucracy to absence of established protocols, some-
mon to any staff member’s inbox. By the core. There were simply too many times a best guess is the best (and only)
example, Trexler’s Dec. 14, 2020, problems requiring too many solutions way to go. For Hindman, that meant
all-staff email contained the JHCC too quickly for the process to be slowed handwriting a negative-pressure-care
Incident Command Center summary, by traditional medically conservative protocol for Johns Hopkins Bayview
along with a PowerPoint explaining chain of command. What occurred is the night the governor announced the
why Johns Hopkins Medicine was what pediatrician Daniel Hindman first COVID cases reached Maryland.
8 H O PK INS C H IL D REN’ S | hopkinschildrens.orgFor Residents, Uncharted Waters
N
obody enters a residency really strong team where no one cared “We created a biodome and had
expecting to confront a pan- that I was a pediatrician; I always felt
to bring in all this adult equipment;
demic, but that’s exactly what I had someone who could answer my
happened to Zach Claudio and questions, and I never felt like I was new beds, pumps, supplies, lots of
Shira Ziegler. Claudio, a third-year doing anything unsafe.” logistics for dealing with patients
resident, remembers the pandemic’s For Ziegler, a third-year pediatrics five times larger than who we’re
onset as being “in unchartered waters,” and genetics resident with an M.D./ used to taking care of.”
what with anxieties of how the disease Ph.D., COVID ground her research to – shira ziegler
spread, whether children would be af- a sudden halt. “They needed (clinical)
fected, and if residents would get sick hands, and though it’s a little cliché, I
en masse. Claudio says that unease was had this very inner desire to help,” says
quelled somewhat “as Hopkins had Ziegler, who volunteered to work in
been manufacturing some of their own the part of the PICU redesigned for
PPE, so we knew we had adequate adult patients with COVID. “We cre-
supplies versus some friends I knew ated a biodome and had to bring in
who worked in community hospitals.” all this adult equipment; new beds,
Claudio was redeployed into an pumps, supplies, lots of logistics for
adult ICU. His last adult care experi- dealing with patients five times larger
ence came in medical school, and he than who we’re used to taking care of,”
admits, “I was nervous at first, because says Ziegler. “But our team rallied and
a lot of the co-morbidities these adults just came together, focusing on giving
had I hadn’t seen in quite some time, them the best care during a novel virus
being a pediatric resident. But we had a and circumstances nobody could have
expected.”
For pediatric anesthesiologist and Koka also handled redeployment of the becoming unstable, while other young-
critical care specialists Jamie McEl- numerous pediatric anesthesiologists sters faced disrupting their scheduled
rath Schwartz and Rahul Koka, it who volunteered to work in other adult routine childhood vaccines.
meant literally taking down walls and side departments to meet the crisis. The situation might have become
reorganizing staff. “We went from a complete bureau- untenable, if not for the efforts of pe-
With the adult side of the hospital cracy and not being able to change a diatrician Helen Hughes and pediat-
getting slammed by COVID, Schwartz, lightbulb without input from nine dif- ric cardiologist and Chief Informatics
who is division chief of pediatric criti- ferent departments, to building seven Officer Philip Spevak. Hughes had
cal care medicine, worked with build- ICU beds in three days,” recalls Koka. independently started a telemedicine
ing operations and pediatric leadership “That’s amazing, and I’m proud of our pilot a few years earlier, serving a rural
to quickly create new adult ICU beds ability to become agile overnight.” Maryland community (Talbot County)
within the PICU. Koka’s role, as the That ability was sorely tested in the so they wouldn’t have the long com-
anesthetic director of the daily flow wake of the elective surgery shutdown, mute to Baltimore for routine care.
within the pediatric operating rooms, as there was an immediate ripple effect Her small outreach, roughly 10 cases,
was to work with Schwartz’s team to on the Children’s Center. Many par- along with a few scattered cases in pe-
ensure the safety of all providers and ents canceled pediatric visits, fearing diatric cardiology and other special-
patients who required emergency and that Johns Hopkins, like many hospi- ties, accounted for all of the Children’s
trauma surgeries, which were still al- tals, was a COVID hot spot. From a Center’s telemedicine cases. But when
lowed after elective surgeries were care viewpoint, this belief had poten- COVID hit, Hughes began mentor-
temporarily banned by Maryland Gov. tially dire consequences. Children with ing other faculty to get them comfort-
Larry Hogan in early March 2020. controlled chronic conditions risked able with providing telemedicine care.
FAL L 2 0 2 1 9Hughes, Spevak and Senior Business cialists and nutritionists into a patient’s outpatient Harriet Lane Clinic, faculty
Intelligence Analyst Muhammad Is- room, “Now we have our team sitting have had a good response reaching out
mail partnered with the institution’s in a conference room, and we have only to East Baltimore residents and con-
Office of Telemedicine to streamline one or two people walk around the pa- vincing them that it’s safe to bring their
the process so patients could access tient with an iPad for everyone else to children back in for well-care visits and
telemedicine video calls with just a few see and hear,” says Eric Biondi, di- scheduled vaccines.
clicks on their MyChart account. rector of pediatric hospital medicine. If the story were to stop right here,
The results have been nothing short “We’re still ‘rounding’ with the whole one might assume all was humming
of astounding. “By May and June, we team, and honestly, it’s increased our along well at the Children’s Center.
averaged over 4,000 telemedicine video efficiency quite a bit. I don’t really want But that’s not the case. Just like nearly
visits per month, accounting for about to go back to the old way of doing it.” all front-line workers, mental health
60% of our total case volume,” says There have been other innovations issues facing Children’s Center staff
Hughes, who was promoted to assis- as well. Throughout the second surge, were palpable. “At first, it was easier to
tant medical director for Johns Hop- as care protocols for adults became recognize the emotional toll because it
kins Medicine’s Office of Telemedicine standardized, the Children’s Center was based on stress and fear,” of CO-
on July 1, 2020. pitched in by creating non-ICU space VID’s communicability and lethality,
That confidence level in using video for recovering adult patients. They also says pediatric epidemiologist Aaron
has spread to the inpatient service as found they were able to treat multisys- Milstone.
well. With COVID protocols demand- tem inflammatory syndrome in chil- In the second surge, that fear has
ing the fewest people possible by the dren (MIS-C), a rare and terrifying given way to an unrelenting funk. “The
bedside, telemedicine has changed tra- disease linked to COVID. Tragically, number of calls to our RISE teams
ditional patient rounds for perhaps the one child died from MIS-C last May, has actually decreased (from the first
first time in a century. Instead of simul- but since then, the Children’s Center surge) says epidemiologist and surgeon
taneously jamming residents, fellows, has successfully cared for more than 30 Albert Wu, who directs RISE. “I
attendings, students, Child Life spe- patients with MIS-C. And over at the think people are just getting discour-
“WE WENT FROM
A COMPLETE
BUREAUCRACY AND
NOT BEING ABLE TO
CHANGE A LIGHTBULB
WITHOUT INPUT
FROM NINE DIFFERENT
DEPARTMENTS, TO
BUILDING SEVEN ICU
BEDS IN THREE DAYS.
THAT’S AMAZING, AND
I’M PROUD OF OUR
ABILITY TO BECOME
AGILE OVERNIGHT.”
–RAHUL KOKA
10 HO PK INS C H IL D REN ’S | hopkinschildrens.orgNurses: The Soldiers in the Battle
S
enior Director of Pediatric Nurs- top-notch care. “I was so proud of that cal quality officer and otolaryngologist
ing Dawn Luzetsky understands partnership, because it was truly the Emily Boss. “I felt like there was no
the stress front-line workers have voice of the pediatric front line saying, nurse not utilized, redeployed every-
felt during the pandemic. Her job has ‘we want to help,’ and leadership heard where, such as our testing sites. It was
been to quell that anxiety wherever she them,” says Luzetsky. a massive effort on their parts, and so I
can. When nurses were asked to go to Just staying employed was another feel we can’t thank our nurses enough
the adult side of the hospital to provide major concern for nurses. Inpatient for being the soldiers in this battle.”
overflow care, they were torn; they cases plummeted when the governor
wanted to help, but preferred to do it banned elective surgeries in March
in a familiar location. So Luzetsky and 2020 for two months, and outpatient
other pediatric administrators lobbied visits dropped precipitously as well. But
hospital leadership for a new unit within between some early retirements and
the pediatric intensive care unit (PICU) creative scheduling, Luzetsky and Assis-
that could handle adults with COVID. tant Director of Pediatric Nursing Lisa
In essence, a new team was created; Fratino have kept nurses working and
PICU nurses on their home turf work- their paychecks rolling, and their efforts
ing side by side with a medical intensive didn’t go unnoticed.
care unit (MICU) adult intensivist and “The nurses are really the heroes of
a MICU nurse consultant to provide this pandemic,” says former chief surgi-
“The nurses are really the heroes of this pandemic. I felt like there
was no nurse not utilized, redeployed everywhere, such as our
testing sites. It was a massive effort on their parts, and so I feel we
can’t thank our nurses enough for being the soldiers in this battle.”
-former chief surgical quality officer emily boss
aged. Even when we do respond to a patients and staff. By example, Child visiting restriction meant parents were
call, more people are silent; they’re just Life has long had a closed-circuit TV rarely in the room together with their
emotionally and physically fatigued.” channel for children. With COVID child until the very end.
Still, RISE and other staff commit- infection prevention efforts eliminat- Still, Kowalski was determined to re-
ted to offering psychological help have ing play visits with siblings and friends, main that constant reassurance in these
done their best to keep the demons at Child Life has tried filling that void by parents’ lives, even if she is now often
bay. Carisa Parrish, who co-directs rapidly expanding live programming to physically off-site to keep patients and
pediatric medical psychology, launched five days a week, broadcasting enter- their families safe. “I’ve been able to do
an initiative for employees dealing with taining and educational shows for kids a lot of teleministering this year, and I
home-schooling challenges. She admits eight hours a day. think it’s actually been very effective,”
it’s not always an easy sell. “For many Similarly, limited parental visitation she says. “It was a natural segue, re-
people, prioritizing their mental health has affected the neonatal intensive care ally, because I’m already working with
is the last thing they do after they have unit. Consider that one of the most a lot of outpatient pregnant moms in
covered every other priority, regardless stressful events for parents and staff is the perinatal program. It’s always been
of the positive influence it might make dealing with a terminally ill baby; in re- easy for me to text a mom and say, ‘I’m
for them,” she says. sponse, Reverend Kat Kowalski had thinking about you,’ and then I can
And yet there are breakthroughs, previously created a perinatal palliative come in and provide in-person sup-
both big and small. Johns Hopkins, un- care program, helping parents from port during really tough times, hav-
like many institutions, deemed Child when they first receive pre-term news ing already established a relationship
Life and Pastoral Care staff as essen- about their baby’s condition through (through teleministry).”
tial workers, which greatly benefited end-of-life care. But when COVID hit, Kowalski adds that staff members
FAL L 2 0 2 1 11“FOR MANY PEOPLE,
PRIORITIZING THEIR
MENTAL HEALTH IS
THE LAST THING THEY
DO AFTER THEY HAVE
COVERED EVERY OTHER
PRIORITY, REGARDLESS
OF THE POSITIVE
INFLUENCE IT MIGHT
MAKE FOR THEM.”
–CARISA PARRISH
have also been reaching out to her in MESH — protecting our staff’s mental, ship doesn’t expect that there will be
increased numbers throughout the emotional and spiritual health.” additional elective procedures or clini-
pandemic. “There was a huge uptick cal shutdowns. There’s also a sense that
in prayer requests. Whether it was ‘My many of the initiatives (such as tele-
S
grandfather has COVID and I’m really o where , exactly , does the medicine) implemented throughout
worried about him,’ or ‘I’m pregnant Children’s Center stand as it the pandemic will become a permanent
and I’m afraid to be at work’ … vari- endures this second surge? It’s part of clinical care.
ous things people would send me, and tempting to think that as vaccination But in the meantime, many staff
it was reaching out in a different way rates rise across Johns Hopkins (the in- members believe there’s still a psycho-
for help.” stitution has been lauded for the fair- logical toll to be paid, a shock that may
COVID’s greatest long-term institu- ness with which they’ve disseminated set in when the pandemic has suppos-
tional impact may be that the psycho- vaccines to front-line workers), the edly passed. Call it pandemic PTSD.
logical resources available around Johns pandemic will eventually recede into Some have already succumbed, retir-
Hopkins are working together in new memory, overtaken by whatever is the ing or resigning when possible, calling
ways. “We’ve coordinated for the first “new normal.” And indeed, that may in sick for days or weeks on end when
time very closely with the other help- eventually happen; barring some un- that’s not an option.
ing services at the hospital,” says RISE’s foreseen circumstance like the spread “There’s a mental health tsunami
Albert Wu, pointing to programs avail- of a new, uncontrolled variant, leader- coming at us, and it’s tough to know
able to all Children’s Center staff. These
include the Healthy at Hopkins initia-
tive as well as outpatient psychiatric ser-
“WE KNOW WHAT WE’RE DOING NOW; IT’S NOT
vices, which brought back retired and THE SAME PANIC SITUATION AS DURING THE FIRST
semiretired staff to handle the mental
health crisis. “As an institution, I think
SURGE. YES, IT’S A BURDEN, BUT WE ARE CALM
there’s a new appreciation for staff resil- NOW, WE UNDERSTAND IT, AND WE’RE CAPABLE
iency and their ability to execute their
mission,” says Wu. “Our leadership
OF A VERY NIMBLE RESPONSE.”
has really embraced the services we call –MAGGIE MOON
12 HO PK INS C H IL D REN ’S | hopkinschildrens.orgwhen it’s going to hit,” says Parrish. ter Surgeon-in-Chief David Hackam, It should, at least, be a more manage-
“It’ll be when people can actually un- who notes that while the Children’s able lift, thanks to what the Children’s
clench and think about what they went Center ceased elective surgeries early Center has learned over the past year-
through, the losses. There’s going to be in the pandemic, its need to perform plus. The JHCC Incident Command
a lot of PTSD and depression. It’s not emergency surgery, especially in new- Center is still convening and commu-
surprising; people have been operating borns, never slowed down significantly. nicating, although virtually now, ex-
on hypervigilance 12 hours a day for “Multiple teams operating in space- panding the content of its Friday email
so long.” suit-like, battery-powered protective summary and Wednesday Zoom up-
As with all wars, pandemics do end, gear came together and showed an in- date. “We know what we’re doing now;
whether it’s after this second surge or credible amount of creativity, flexibil- it’s not the same panic situation as dur-
additional aftershocks. Either way, ity and expertise in providing complex ing the first surge,” says Maggie Moon.
there’s the sense that the Children’s pediatric care,” says Hackam. Compar- “Yes, it’s a burden, but we are calm
Center will come out of this a better ing the second surge with a marathon, now, we understand it, and we’re ca-
institution, even more deft and with far he adds, “We will get through this to- pable of a very nimble response.”
greater resilience than anybody could gether, and those who are struggling,
have expected or asked for. That’s al- the rest of us will pick them up — and
ready happening, says Children’s Cen- we will carry them forward.”
Infection Control:
100-Hour Weeks on the Fly
I
t’s rare that infectious disease spe- like being a traffic cop. You’re trying to more PPE, more testing.”
cialists are a hospital’s most sought- protect people, but you’re unpopular,” Now with COVID care becoming
out physicians, but COVID-19 has says Milstone. more routine in the second surge, Mil-
spotlighted the work of faculty such That all changed when COVID hit. stone worries that, even with vaccina-
as epidemiologist Aaron Milstone. “Suddenly we were working 100-hour tions, staff are letting down their guard.
A member of the Children’s Center weeks for six straight weeks in the “We’re beginning to get that resent-
Hospital Epidemiology and Infection Command Center, because in the first ment again,” regarding their infection-
Control (HEIC) team, Milstone, along wave providers were scared,” says Mil- protection advice. “This is not the time
with Lisa Maragakis, Anna Sick- stone. “There was so much to figure to be complacent. This is when it mat-
Samuels, Taylor McIlquham and out on the fly—things like how to test ters most.”
other HEIC members were the go-to patients coming into the hospital, what
consortium for keeping hospital staff kind of PPE worked best, anything and
and patients COVID-safe. everything regarding infection spread.”
For Milstone, suddenly being high Millstone adds, “Usually, we’re told “We're beginning to get that
profile and in demand was a career we’re doing too much (regarding nor- resentment again. This is not the
first. He agrees that, in normal times, mal infection protocols),” says Milstone. time to be complacent. This is
infectious disease docs are often seen “But in the beginning of the pandemic, when it matters most.”
as a bit of a pain in the neck, always we ironically got criticized for not being – aaron milstone
reminding people of basic hygiene. “It’s conservative enough; people wanted
FAL L 2 0 2 1 13In the pediatric intensive care unit,
from left, Meghan Bernier, Amanda
Levin and Katherine Hoops.
Battling Multisystem Inflammatory Disease
BY GARY LOGAN
After a year in the trenches an outside hospital or our transport admit MIS-C patients, agrees: “In the
team about a patient with certain signs beginning, so many patients came in
facing the pandemic’s most and symptoms and can say with pretty with vague symptoms, really sick and
lethal threat to children, significant acumen this child has MIS-C we weren’t sure why, or seemed to
intensivists cite significant until proven otherwise.” manifest MIS-C with a predilection for
gains in diagnosing and Many children with MIS-C, Bernier ex- one or two organs involved as the pri-
plains, typically present with abdominal mary problem. Early on, and even now,
treating this new disease — pain, difficulty breathing, fevers, gastro- people are not always recognizing that
and saving lives. intestinal issues, inflammation, neuro- it might be MIS-C, even though we’re
logic manifestations such as seizures, and getting more and more savvy. We see
F
ollowing the arrival of the coronavi- skin rashes — all signs and symptoms the whole gamut.”
rus in early 2020, a new mysterious that can also mimic many other diseases. Further complicating diagnosis and
and serious — and in some cases, “What makes MIS-C such a chal- treatment, however, is how quickly
deadly — related disease appeared. lenging diagnosis is that it has so much these intensivists have seen patients de-
Called multisystem inflammatory syn- in common with other clinical syn- cline due to a tsunami of inflammation
drome in children (MIS-C), its symp- dromes that we see, like sepsis or even attacking multiple organ systems.
toms initially confounded diagnosis and a GI illness,” says intensivist Katherine “Rapid diagnosis and rapid initiation
treatment by critical care intensivists like Hoops. of treatment is really important be-
Meghan Bernier — but not so much On the other hand, Hoops adds, the cause kids can get very ill very fast,” says
today. signs can be really subtle — a challenge Hoops. “They may have progressive
“Back in May and June 2020 we were for families and clinicians to see the for- multisystem failure with heart failure,
struggling with how to treat these pa- est through the trees. respiratory failure needing mechanical
tients and what protocol to use,” says “It looks like a lot of things but the ef- ventilation, and kidney failure needing
Bernier. “Now, we’re 12 months into fects can be devastating,” says Hoops. dialysis.”
MIS-C and have developed a lot of ex- Intensivist Amanda Levin, who Adds Bernier, “They can go from
perience. Today I can hear a story from leads one of two PICU teams that walking into the ED to needing life sup-
14 HO PK INS C H IL D REN ’S | hopkinschildrens.org“I was drawn to the PICU
because I like caring for and
thinking about the whole child
and the interaction of all of
port within hours.” “you have to go with your gut instinct the body’s systems. I love our
Initially, Hoops says, there was a lot and your best idea of what is going on work caring for critically ill
of fear among health professionals about with the child.” and injured children — they
how to respond to MIS-C. At the same To help fill in any holes in care — like challenge us all to be our best.”
time, she adds, intensivists do not like to an unrelenting fast heart rate that despite
– katherine hoops
be put on their heels, which prompted fluid or antipyretics cannot be brought
an aggressive fast-paced learning pro- down — they reach out to their subspe-
cess in the PICU to work collaboratively cialist colleagues in cardiology and rheu- to their baseline level of functioning in
to understand how MIS-C presented matology, among other disciplines, for a week, a month, a year. However, we
and what treatments could best tame it. speedy remedies and input on workup, are encouraged that kids are leaving
They have seen enough cases to always possible causes and treatment. Collabo- the ICU faster and responding to those
have a high index of suspicion for MIS-C ration and communication, stresses Ber- therapies.”
if a critically ill child comes in with symp- nier, are essential. So, the learning curve continues?
toms consistent with sepsis. “We’re still generalists in the ICU — “Oh sure, we’re still refining these
In addition, garnering 12 months of we can do 80% to 90% of the work, but algorithms as we learn about new
experience encountering the signs and we need the help of our specialists to therapies shown to be effective by our
symptoms of MIS-C, they have built refine the last 10% to think of presen- colleagues here at Johns Hopkins and
— seemingly brick by brick with each tations and diseases and workup we around the world,” says Hoops. “Our
patient they’ve seen or case they’ve re- hadn’t thought of,” says Bernier. practice is constantly evolving with the
viewed — a diagnostic and treatment Hoops agrees: “Through this process evidence — that is how we in critical
algorithm with their pediatric subspecial- we’ve been grateful for a lot of collabor- care manage anything.”
ist colleagues in cardiology, hematology, ative work from a multidisciplinary team Managing MIS-C, the intensivists con-
infectious disease and rheumatology. As to better understand the disease pro- clude, is not by any means easy work.
cardiac and respiratory functions are the cess and also to develop diagnostic and The alarm-bell, all-hands-on-deck
highest priority concerns in their proto- treatment protocols so we can rapidly moments when everybody swoops in
col, the intensivists adhere to the ABC identify new cases and quickly intervene to quickly reverse the inflammation and
formula — airway, breathing, circula- to give our patients the best evidence- potentially save a life is both exciting and
tion — they’ve been trained to follow based therapies.” rewarding. But not all patients survive,
for life-threatening conditions. One such proven targeted therapy which takes an intense toll on the team
“Our main role is to help stabilize the is intravenous immune globulin (IVIG), members as well, as they see firsthand
critical functions of the body, to make which Bernier describes as applying the struggles and distress families face —
sure the child’s blood pressure is staying white noise to the immune system: “It’s which they also face.
stable, the heart rates and function are amazing to watch this listless child lying The rewards they cite are seeing a
working appropriately, and the patient is in bed febrile and tachycardic, then get child turnaround following treatment, in
breathing and exchanging air acceptably the infusion of IVIG to quiet the im- some cases dramatically, and getting to
with whatever medicines and interven- mune system, and six to 10 hours later know a patient and the family at the bed-
tions are needed,” says Bernier. that child has perked up and is playing in side or on twice-daily, family-centered
This stabilizing step relies on a team of the parent’s lap or walking around the rounds. They also cite intrinsic rewards.
faculty physicians, fellows, residents and room. The parents are like, ‘I have my “I was drawn to the PICU because I
nurse practitioners — a tailored MIS-C baby back.’” like caring for and thinking about the
group of specialists within the PICU — That, however, has not and will not whole child and the interaction of all of
working 24/7 to constantly evaluate and always be the case, says Hoops, noting the body’s systems,” says Hoops. “I love
initiate therapies to prevent worsening that each child’s recovery is different: our work caring for critically ill and in-
of illness. Meanwhile, at times because “When you see a child in the PICU, it’s jured children — they challenge us all to
time is of the essence, Bernier adds, hard to predict if they’re going to return be our best.”
FAL L 2 0 2 1 15P H OTO J O U R N A L
KIDS
GIVING
BACK
IN SURPRISING WAYS
Most children, teens or parents never imagine
finding themselves at Johns Hopkins Children’s Center.
Whether for a broken bone, a cancer diagnosis or a chronic
illness, patients, families and friends alike are afraid of the
unknown and look to their care team for answers.
For many, the care providers become like family, and the hospital
feels like a second home. This connection extends even deeper
for some who decide to give back to Johns Hopkins to show
their gratitude. Some people who don’t visit the Children’s
Center firsthand, but are touched by the experience of their
family and friends, feel inspired to contribute, as well.
Meet five patients and friends of the Children’s Center who,
through their compassion and resiliency, provide invaluable
resources to help kids and teens like them.
PHOTOGRAPHY BY KATHRYN DULNY
TEXT BY AMANDA LEININGER
16 HO PK INS C H IL D REN ’S | hopkinschildrens.orgJULIA
ALEXANDER, 14
Grade II Ependymoma
Diagnosed with a brain tumor
at age 8, Julia has undergone
three brain surgeries, five minor
surgeries, eight rounds of
chemotherapy and two months
of radiation at the Children’s
Center. Julia and the Sparklettes
regularly participate in Team
Hopkins Kids during the Baltimore
Running Festival, the Children’s
Center’s Radiothon, and Baltimore
Boogie dance marathon. The
performances raise funds for Child
Life services and other programs
that provide fun play opportunities
for kids in the hospital.
“
"Johns Hopkins means so
much to me and my family,”
Julia says. “They saved my
life. Miss Mollie is my Child
Life specialist, and she makes
my time at the hospital
as enjoyable as it can be.
Because of her, I am looking
into being a Child Life
specialist or an art therapist."
FAL L 2 0 2 1 17TEDDY
MOSHER, 14
Traumatic Injury,
Commotio Cordis
14-year-old Teddy, a goalie, was
struck in the chest by a shot on
goal during a lacrosse tournament.
The impact triggered a disruption
in the rhythm of his heart, caus-
ing it to stop, and Teddy collapsed
on the field. After follow-up care
at the Children’s Center, he was
playing lacrosse again within weeks.
Today he is happily “back in the
cage” with the Looney’s Lacrosse
Club, and he plans to play at Loyola
Blakefield in Towson, Maryland
next year as a freshman.
Teddy passionately advocates for
player safety, and promotes use
of new required chest protec-
tors through social media. He also
designed a wristband that reads
“HeartStrong” on one side and
“#Looneys2025” on the other
side, and he donates all proceeds
from their sale to support pediatric
cardiology at the Children’s Center.
“
"I want to raise awareness
for what happened to me and
for all athletes to wear the
proper equipment,” Teddy
says. “I just want to make
sure that nothing like this
happens to anyone else."
18 HO PK INS C H IL D REN ’S | hopkinschildrens.orgHANNAH
VINITSKY, 14
E. Coli Poisoning,
Kidney Disease
At 4-years-old, Hannah was
admitted to the Children’s Center
with E. coli poisoning. In addition
to dehydration, she suffered severe
kidney damage. Hannah underwent
two surgeries and three blood
transfusions at the Children’s
Center, and she is now regularly
seen there for kidney disease
caused by the E. coli poisoning.
While waiting for appointments
in the renal clinic over the years,
Hannah has always loved to read,
and she wanted to help provide
books to other patients. Hannah
collected over 120 books to give to
the clinic.
“
"Johns Hopkins Children’s
Center means a lot to
me, and I'm happy to do
something for the other
kids like me that have to go
there,” Hannah says. “I love to
read, and I wanted to help the
older kids at the Children’s
Center have something to do
while waiting to see doctors.”
FAL L 2 0 2 1 19AMBER BRISCOE, 17 Founder and President of Arts-n-STEM 4 Hearts Amber began volunteering at local hospitals at the beginning of middle school and she recalls her interac- tions with pediatric patients as the most profound and meaningful. Her creative passions led her to engage young patients through drawing, painting and other crafts. Inspired by the “moments of joy” she saw when they discovered their creativity, and with her con- viction to make the world a better place, she combined her passions for art and science and founded the Arts-n-STEM 4 Hearts foundation, which supports 32 organizations (including Johns Hopkins Children’s Center) through volunteering and by providing art and science kits. “ “To me, Johns Hopkins Children’s Center means family,” Amber says. “The resilience and courage of the patients and families continue to inspire me every day. I have an immense love for every child, and I am truly honored and blessed to be able to make a difference wherever I can. I hope to continue living a life of significance for my family at the Children’s Center.” 20 HO PK INS C H IL D REN ’S | hopkinschildrens.org
“
RUBY ROSEN, 5
Atrial Septal Defect
Diagnosed with an atrial septal defect, or hole in “When I stayed at the
her heart, at 6 months old, Ruby has been closely hospital to get my heart fixed,
followed by pediatric cardiologists at Johns Hop-
kins Children’s Center ever since. Doctors carefully I got a Frozen nightgown and
monitored her, hoping the hole would close on its toys,” Ruby says. “Now other
own. Unfortunately, it was too large and needed to
kids can get that when their
be closed surgically. At age 4, Ruby had open heart
surgery. Just 60 days later, she ran a lemonade stand heart is fixed.”
in her neighborhood to raise funds for the Children’s
Center’s Division of Pediatric Cardiology.
FAL L 2 0 2 1 21The
Draw of
Pediatrics
22 HO PK INS C H IL D REN ’S | hopkinschildrens.orgYou can also read