Scientific Evidence of Interventions Using the Mediterranean Diet: A Systematic Review
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
February 2006: (II)S27–S47
Scientific Evidence of Interventions Using the Mediterranean
Diet: A Systematic Review
Lluı́s Serra-Majem, PhD, MD, Blanca Roman, MD, and Ramón Estruch, PhD, MD
The Mediterranean Diet has been associated with lated cognitive impairment, and cancer, among
greater longevity and quality of life in epidemiological others. Interventions should use food scores or pat-
studies, the majority being observational. The appli- terns to ascertain adherence to the Mediterranean
cation of evidence-based medicine to the area of diet. Further experimental research is needed to cor-
public health nutrition involves the necessity of devel- roborate the benefits of the Mediterranean diet and
oping clinical trials and systematic reviews to develop the underlying mechanisms, and in this sense the
sound recommendations. The purpose of this study methodology of the ongoing PREDIMED study is
was to analyze and review the experimental studies on explained.
Mediterranean diet and disease prevention. A system-
Key words: Mediterranean diet, prevention, evidence-
atic review was made and a total of 43 articles
based nutrition, dietary interventions, clinical trails
corresponding to 35 different experimental studies
© 2006 International Life Sciences Institute
were selected. Results were analyzed for the effects of
doi: 10.1301/nr.2006.feb.S27–S47
the Mediterranean diet on lipoproteins, endothelial
resistance, diabetes and antioxidative capacity, car-
diovascular diseases, arthritis, cancer, body compo-
sition, and psychological function. The Mediterranean INTRODUCTION
diet showed favorable effects on lipoprotein levels,
endothelium vasodilatation, insulin resistance, meta- Epidemiological studies1-3 have observed great geo-
bolic syndrome, antioxidant capacity, myocardial and graphical differences in the incidence rates of cardiovas-
cardiovascular mortality, and cancer incidence in cular disease. Compared with northern European coun-
obese patients and in those with previous myocardial tries or the United States, there is a low incidence of
infarction. Results disclose the mechanisms of the coronary heart disease (CHD) in countries of southern
Mediterranean diet in disease prevention, particularly
Europe, such as France, Spain, Greece, and Italy. The
in cardiovascular disease secondary prevention, but
Mediterranean food pattern has been the factor most
also emphasize the need to undertake experimental
frequently invoked to explain this difference. The term
research and systematic reviews in the areas of pri-
mary prevention of cardiovascular disease, hyperten- “Mediterranean diet” reflects the dietary patterns charac-
sion, diabetes, obesity, infectious diseases, age-re- teristics of several countries in the Mediterranean Basin
during the early 1960s. The association between greater
longevity and reduced mortality and morbidity for CHD
Dr. Serra-Majem is with the Department of Clinical has also been observed for certain cancers and other
Sciences. University of Las Palmas de Gran Canaria, nutrition-related diseases. The common dietary food pat-
Spain, and the Foundation for the Advancement of the terns in these countries have substantiated this con-
Mediterranean diet, University of Barcelona Science cept,4,5 although the data come mostly from observa-
Park, Spain; Dr. Roman is with the Foundation for the
Advancement of the Mediterranean Diet; Dr. Estruch is
tional studies.
with the Department of Internal Medicine, Hospital Such patterns were defined in 1993 at the Interna-
Clinic, Instituto de Investigaciones Biomédicas August tional Conference on the Diets of the Mediterranean,
Pi Sunyer (IDIBAPS), University of Barcelona, Spain having also been previously defined in other meetings.4-7
Please address all correspondence to: Profes- They are comprised of:
sor Lluı́s Serra-Majem, President, Foundation for the ● Abundant plant foods (fruits, vegetables, breads,
Advancement of the Mediterranean Diet, Parc Cientific
other forms of cereals, beans, nuts, and seeds);
de Barcelona, Universitat de Barcelona, Baldiri
● Minimally processed, seasonally fresh, and locally
Reixac, 4 Torre D 08028 Barcelona, Spain; Phone:
34-934-034-541; Fax: 34-934-034-543; E-mail: grown foods;
dietmed@pcb.ub.es ● Fresh fruits as the typical daily dessert with sweets
Nutrition Reviews姞, Vol. 64, No. 2 S27based on nuts, olive oil, and concentrated sugars or experimental studies analyzing the Mediterranean diet in
honey consumed during feast days; disease prevention.
● Olive oil as the principal source of dietary lipids;
● Dairy products (mainly cheese and yogurt) con-
METHODS
sumed in low to moderate amounts;
● Fewer than four eggs consumed per week; We searched MEDLINE (National Library of Med-
● Red meat consumed in low frequency and amounts; icine, Bethesda, MD) for relevant articles about the
and Mediterranean diet and prevention of certain pathologies
● Wine consumed in low to moderate amounts, gen- published from October 2004 to January 2005. We used
erally with meals. the keywords “Mediterranean diet,” “health,” “cancer,”
This characteristic definition of the Mediterranean “cardiovascular disease,” “bone disease,” “prevention,”
diet and its typical composition is not without ambigu- and combinations such as “Mediterranean diet and
ities, which require certain consideration.8-10 health,” “Mediterranean diet and cancer prevention,”
Evidence-based nutrition is the application of the “Mediterranean diet and cardiovascular disease,” and
principles of evidence-based medicine to the area of food “Mediterranean diet and bone health.” We narrowed the
and nutrition, in both clinical practice and in the public search to clinical trials published in English and limited
health. to those conducted in humans. We focused the search on
Usually, in the field of public health nutrition/dietary articles referring to the Mediterranean diet as a whole
guidelines/policy development, the application of evi- and excluded studies regarding specific foods of this diet.
dence-based nutrition has several weaknesses, since We also excluded those articles evaluating the effects of
there are some limitations when analyzing the effect that an isolated intake of a Mediterranean menu instead of the
diet modification has on health: prolonged effect of such a diet. Additional publications
● The modification of a diet not only requires much
were identified from references provided in original
papers.
collaboration from the patient but also of the envi-
We found 46 articles that met the inclusion criteria.
ronment, with convenient access to products and
Regarding the sample size, 22 of the studies had less than
willingness to buy and cook the food according to
50 subjects, 9 studies included 50 to 100 subjects, 9
the dietary plan. Moreover, measuring dietary ad-
studies had a sample of 101 to 500 subjects, 4 studies
herence entails greater effort from both the partici-
included a sample having between 500 and 1000 indi-
pant and the investigator.
viduals, and 1 study included more than 1000 subjects.
● The complexity of dietary modifications makes it
difficult to develop a double-blind intervention to
analyze its effects on health. RESULTS
● The enormous diversity of food habits, basal meta-
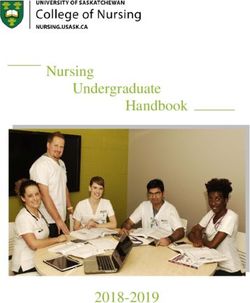
bolic status, and nutritional objectives and dietary A total of 489 articles studies were selected with the
guidelines worldwide are limitations for making term “Mediterranean diet” and analyzed. The year dis-
tribution is shown in Figure 1. After excluding animal
comparisons between studies developed in different
research, 416 studies remained, with only 324 having
contexts.
abstracts and, of these, 128 were reviews.
There is very small number of systematic reviews
Among the original research articles, 55 were clin-
analyzing the effect of the Mediterranean diet on health-
ical trials and 41 of them were randomized clinical trails.
related issues, and also the number of randomized, con-
From the total of 55 clinical trial citations obtained,
trolled clinical trials is scarce (less than 50). In contrast,
43 were selected (12 excluded due to: language, inter-
the worldwide popularity of the Mediterranean diet as a vention limited to one food and methodological weak-
healthy and recommended diet is evident in the prolifer- nesses, among others), corresponding to 35 different
ation of media attention (more than 740,000 citations in studies. Studies were conducted in Italy, Spain, France,
Google® as of January 2005). Great Britain, Chile, Sweden, Canada, Australia, United
Most of the scientific articles published are obser- States, Denmark, Finland, and India, and the number of
vational epidemiological studies (primarily ecological or subjects ranged from 11 to 13,000.
case control studies and a few cohorts). Almost all the Studies were classified into six groups according to
reviews published are non-systematic and reflect an their objectives and outcome measures: lipoproteins/
opinion or a collection of self-selected articles rather endothelial resistance/ diabetes, cardiovascular disease,
than an objective analysis of sound evidence. arthritis, cancer, body composition, and psychological
The objective of this study is to analyze the literature function.
published on the Mediterranean diet and to review all A first group consisted of different intermediate
S28 Nutrition Reviews姞, Vol. 64, No. 2Figure 1. Number and type of articles published about the Mediterranean diet. 䉬, Publications; ‚, reviews; E, clinical trials.
outcomes such as lipoproteins, glycemic control, endo- showed a risk reduction of 60% in the Mediterranean diet
thelial resistance, inflammation markers, and antioxidant group. The studies on body weight also showed favor-
capacity. It included 30 articles published from 1982 to able results with the Mediterranean diet, particularly the
2004, with more than half (18) published from 2001, and study by McManus et al.51 which in addition to higher
only 5 before 1995.11-40 weight losses, showed greater compliances to diet ther-
A second group measured cardiovascular disease apies. Finally, the Mediterranean diet did not show any
incidence or morbidity with five articles.41-45 A third alterations in mood in the last group.
group included two articles on arthritis.46,47 A fourth
group focused on cancer with only one article.48 Three DISCUSSION
articles on body weight and obesity comprised the fifth
group,49-51 and the last group included two articles on The aim of this article was not to cast doubts on the
psychological function.52,53 level of evidence for Mediterranean diet interventions
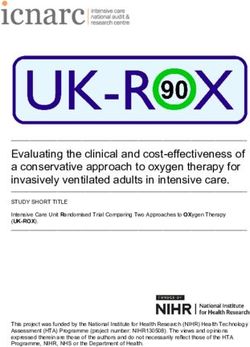
All results are summarized in Table 1. Most of the but to emphasize the weaknesses of research on the
clinical trails in the first group analyzing the effect of Mediterranean diet and to stress the need for further
Mediterranean diet on lipids found reductions in total research and systematic reviews. One of the most imme-
cholesterol, low-density lipoprotein (LDL) cholesterol diate conclusions obtained from this review is that the
(decrease in small LDL particles number in some), scientific evidence for the Mediterranean diet is mostly
tryglicerides, apoprotein B, and very-low-density li- sustained by observational studies and personal reviews.
poprotein (VLDL) cholesterol, and an increase in high- For some of the years during the period analyzed,
density lipoprotein (HDL) cholesterol. An increase of the the number of original articles related to the Mediterra-
total plasma antioxidant capacity was also observed in nean diet was similar to the number of reviews. Addi-
two studies, but not in another. Endothelium function tionally, it is remarkable that most of the reviews are
improved with the Mediterranean diet, and endothelial- non-systematic and at times are very subjective and
dependent vasodilatation was increased by adding nuts to biased.
the Mediterranean diet. Insulin resistance and metabolic An example can be found in an interesting review
syndrome were reduced after changing to a Mediterra- article of the Mediterranean diet in Greece by Simopou-
nean diet, but some studies showed no effects on insulin los.54 The author cited 114 references, but none included
or glucose levels. All of the articles addressing cardio- Trichopoulou (author of 53 of the 284 references in the
vascular disease and secondary prevention showed an search “diet and Greece”) or Kafatos (author of 28 of the
odds ratio for fatal myocardial infarction between 0.25 284 references). Another very similar article from the
and 0.7. The single study on arthritis functionality and previously mentioned author55 reviewed the relationship
pain demonstrated benefits, and the sole study on cancer between the Mediterranean diet and cancer in Greece,
Nutrition Reviews姞, Vol. 64, No. 2 S29Table 1. Clinical Trials on the Mediterranean Diet
S30
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
DIABETES/LIPOPROTEINS/ENDOTHELIAL RESISTANCE
Vincent et al., Marseille, RCT Primary 212 subjects, M/F MD or a traditional BMI, fasting lipids and 3 months BMI: ⫺5.2% (vs. ⫺4.2%);
200411 France prevention with at least 1 low-fat/cholesterol lipoproteins, (still on TC: ⫺7.4% (vs. ⫺4.4%);
CV risk factor diet apolipoproteins, glucose, going) LDLC: ⫺9.9% (vs.
insulin and homocysteine ⫺5.4%); plasma TG:
⫺13.0% (vs. ⫺7.9%);
plasma glucose: ⫺3.0%
(vs. ⫺3.5%); plasma
insulin: ⫺21.3% (vs.
⫺17.5%) (p ⬍ 0.05 for all)
Esposito et al., Naples, RCT, single- Primary 180 subjects with Control group Nutrient intake, Endothelial 24 months 2 serum concentrations of
200412 Italy blind prevention metabolic following a function score (BP and high sensitivity-C-reactive
syndrome (99 prudent diet and platelet aggregation protein (p ⫽ 0.01),
M, 81 F) intervention group response to L-arginine), interleukin 6 (p ⫽ 0.04),
following a MD lipid and glucose interleukin 7 (p ⫽ 0.4) and
parameters, insulin interleukin 18 (p ⫽ 0.3),
sensitivity and 2 insulin resistance (p ⬍
circulating levels of high 0.001). Improved
sensitivity C-reactive endothelial function score
protein and interleukins (mean ⫹ SD) change,
6, 7 and 18 ⫹1.9 (0.6) p ⬍ 0.001). At
2 years follow up 40
subjects in intervention
group still had features of
the metabolic syndrome vs.
78 of the control group
Ros et al., Barcelona, R-crossover- Primary 21 hyper- 4 weeks of a Brachial artery vasomotor 4 weeks The walnut diet improved
200413 Spain CT prevention cholesterolemic cholesterol function, vascular cell endothelium dependent
subjects (8 M, lowering MD/4 adhesion molecul-1, vasodilation and 2 levels
12 F) weeks of a diet endothelium independent of vascular cell adhesion
similar of energy vasodilation levels of molecul-1 (p ⬍ 0.005 for
and fat content intercellular adhesion both), 2 TC and LDLC (p
where walnuts molecul-1, C-reactive ⬍ 0.05) respect to the MD.
replaced aprox protein, homocysteine, Endothelium independent
32% energy from oxidation biomarkers vasodilation and levels of
MUFA TC, LDLC intercellular adhesion
molecul-1, C-reactive
protein, homocysteine, and
oxidation biomarkers were
similar after each diet
Nutrition Reviews姞, Vol. 64, No. 2Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
Ambring et al., Goteborg, R-crossover- Primary 22 healthy 4 weeks of a Fasting blood lipids, 4 weeks 2 TC, LDLC, TG and apoB
200414 Sweden CT prevention subjects (12 Swedish diet, 4 insulin and glucose levels by 17%, 22%, 17%
M, 10 F) weeks of a MD levels, apo B and LDL and 16% (p ⬍ 0.05). No
particle size. Endothelial effect on insulin, glucose
dependent and level, LDL particle size,
independent vasodilation endothelial function,
evaluation and arterial arterial distensibility,
distensibility evaluated fibrinolitic capacity or
Nutrition Reviews姞, Vol. 64, No. 2
by ecocardiography. oxidative stress
Fibrinolitic capacity,
oxidative stress through
urinary F2-isoprostane
Goulel et al., 200415 Quebec, Clinical trial Primary 77 healthy F 12 weeks nutritional LDL-PPD, cholesterol 12 weeks No change on the LDL-PPD,
Canada prevention intervention with levels in small (LDLC LDL integrated size, and in
two group ⬍ 255 Å) and large the LDL distribution
sessions, three (LDLC ⬎ 260 Å) LDL among subclasses. No
individual sessions fractions, plasma lipid change on LDLC, HDLC,
and four 24-h and lipoprotein profile and TG. 1 LDL-PPD in F
recall in the first tertile of the
LDL-PPD distribution at
baseline (p ⫽ 0.03). 2 of
the proportion of LDL% ⬍
255 Å (p ⫽ 0.12) and 1
of the proportion of LDL%
⬎ 260 Å (p ⬍ 0.05) in F
with a reduced LDL-PPD
at baseline. 2LDL-PPD
and LDL integrated size in
F with large LDL particles
at baseline (LDL PPD ⬎
260 Å) (p ⫽ 0.007)
Flynn and Australia Clinical trial Primary 155 individuals 3 months on a MD TC, TG, HDLC, LDLC. 3 months 2TG (31.6%), 1HDLC
Colquhoun, prevention (31 M, 124 F) and control group? (9.6%), no significant
200416 (non specify) changes on TC, LDLC
Urquiaga et al., Santiago Clinical trial Primary 21 M 3 months on a MD Plasma fatty acids profile 3 months MD group ⬎ levels of MUFA,
200417 de Chile, prevention or western diet. (SFA, MUFA, PUFA, omega-3 fatty acids, ⬍
Chile The second month omega-3 fatty acids levels of PUFA and omega-
red wine was and omega-6/omega-3 6 fatty acids and ⬍ omega-
added to both fatty ratio) 6/omega-3 ratio. Wine
diets 2MUFA and 1PUFA in
both dietary groups
S31Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
S32
Publication Country Type of Study Population Methodology Outcome Follow Up Results
Bravo-Herrera Córdoba, R-crossover- Primary 41 subjects Three dietary TC, TG, LDLC, HDLC, 3 months The MD and CHO diet
et al., 200418 Spain CT prevention periods; saturated expression of a tissue showed ⬍TC, LDLC,
fat enriched diet, factor in circulating HDLC, and tissue factor
low fat and high monocytes. expression than the SFA
CHO diet, MD diet
Toobert et al., Oregon, RCT Secondary 279 2 groups: usual care HbA1, lipid profile, 6 months 2 HbAc ⫽ 0.4% (p ⫽
200319 USA prevention postmenopausal (control) and plasma fatty acids, BMI, 0.001), no statistical
DM2 F intervention group: BP, flexibility, quality changes on TC, TG,
an initial 3-days of life (measured by the LDLC, HDLC, 2 BMI ⫽
retreat and 6 months Medical Outcomes 0.37 (p ⫽ 0.015),
of weekly meetings Study (MOS) Short improvement of the PAID
with diet, physical Form General Health regimes related distress
activity and stress Survey and The dimension
management Problem Areas in
modification Diabetes (PAID) scale)
Rodriguez Villar Barcelona, R-crossover- Secondary 22 subjects (12 M, 6 weeks of a high LDL resistance to 6 weeks
No changes on body weight,
et al., 200420 Spain CT prevention 10 F) with DM2 CHO diet and 6 oxidation, body glycaemic control, serum
weeks on a high weight, glycaemic concentration of fasting
MUFA diet or control, serum lipids, LDLC and HDLC,
vice versa lipoproteins apolipoproteins Al and B,
and lipoprotein (a). The MD
2 VLDLC by 35%, VLDL-
TG by 16%, and the quotient
VLDL-TG to VLDL
apolipoprotein B (p ⫽
0.0029) indicating a lesser
particle enrichment with TG.
No differences were seen on
LDL oxidative resistance
Goulet et al., Quebec, Clinical trial Primary 77 F 12 weeks nutritional Plasma lipid lipoprotein 12 weeks 2 TC 2.5% (p ⬍ 0.05) at
200321 Canada prevention intervention with profiles; body weight week 6 and apoB levels
two group sessions, 5.1% (p ⬍ 0.05) at week
three individual 12, no effect on plasma
sessions and four LDLC, HDLC, TG, 2BMI
24-h recall (p ⬍ 0.01) at week 12
Sondergaard Svendborg, RCT Secondary 115 patients (92 12 months of statin Serum lipids, endothelial 12 months 2 TC and LDLC in both
et al., 200322 Denmark prevention M, 39 F) with treatment and MD function measured with groups, 2 TG levels only in
recent or remote intervention group non invasive the intervention group (p ⬍
MI or unstable or control group ultrasound scanning 0.05) and no changes in
or stable angina vessel-wall tracking of HDLC on either group. The
pectoris brachial artery FMD intervention group showed
an improvement in FMD (p
Nutrition Reviews姞, Vol. 64, No. 2
⬍ 0.01)Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
Mezzano et al., Santiago de Clinical trial Primary 42 healthy M 21 subjects on a MD Primary hemostasis 90 days The mean BT for the MD
200323 Chile, prevention and 21 subjects on variables (BT, plasma group was longer (p ⫽
Chile a high-fat diet for concentrations of 0.017). The MD produces
30 days, vWR: Ag and platelet no changes on vWF:Ag or
supplementation aggregation and platelet aggregation. The
with red wine in secretion ex vivo) addition of red wine
both groups from produced 1 platelet
day 31 to 60 serotonin secretion after
stimulation with collagen
Nutrition Reviews姞, Vol. 64, No. 2
and 1 platelet
aggregation at the higher
collagen concentration.
No changes on BT,
plasma vWF:Ag
concentration or platelet
count
Singh et al., 200224 London, RCT, Primary 56 healthy subjects 6 weeks on a MD or Forearm blood flow 6 weeks The MD 1 Bradykinin-
U.K. double- prevention (26 M, 30 F) vitamin C (measured by dependent vasodilatation (p
blind supplements or pletismography), ⫽ 0.011) versus placebo,
placebo endothelium- 1Glyceryl trinitrate-
dependent dependent relaxation (p ⫽
vasodilatation 0.003) versus placebo and
(measured by 1 plasma vitamin C levels
bradykinin similar to supplements (p
acetylcholine) and ⬍ 0.05)
independent
vasodilatation
(measured with the
nitric oxid donor
glyceryl trinitrate)
Perez Jimenez Cordoba, R-crossover- Primary 59 young subjects 28 days of a SFA Serum lipid levels, free 28 days 2 TC (p ⬍ 0.001), HDLC
et al., 200125 Spain CT prevention (30 M, 29 F) enriched diet, fatty acids, fasting (p ⬍ 0.001), LDLC (p ⬍
followed by 28 insulin and glucose, 0.001), fasting insulin
days of a low fat, glucose suppression and free fatty acids (p ⬍
high CHO diet or test, in vitro basal 0.001), 2 mean glucose
a MD and vice glucose-uptake, in vitro in steady state plasma
versa insulin-stimulated glucose in glucose
glucose uptake suppression test (p ⬍
000.1), 2 in vitro basal
glucose uptake and
insulin stimulated glucose
uptake
S33S34
Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
Mezzano et al., Santiago de Clinical trial Primary 42 healthy M 21 subjects on a MD Hemostatic 90 days The MD had lower plasma
200126 Chile, prevention and 21 subjects on cardiovascular risk fibrinogen (p ⫽ 0.03),
Chile a high-fat diet for factors: Fibrinogen, factor VIIc (p ⫽ 0.034)
30 days, Factor VIIc, Factor and factor VIIIc (p ⫽
supplementation VIIIc, tissue 0.0057) and higher levels
with red wine in plasminogen activator of protein S (p ⫽ 0.013).
both groups from antigen, plasminogen Wine produced 2 plasma
day 31 to 60 activator inhibitor fibrinogen (p ⫽ 0.001)
antigen, antithrombin and FVIIc (p ⫽ 0.05)
III, Protein C and and 1 tissue plasminogen
protein S, C-reactive activator antigen (p ⫽
protein 0.01), plasminogen
activator inhibitor antigen
(p ⫽ 0.0003)
Fuentes et al., Cordoba, R-crossover- Primary 22 hyper- 28 days of a SFA Serum lipid levels, 28 days The NCEP-1 and MD
200127 Spain CT prevention cholesterolemic enriched diet, endothelial function, produced 2 plasma TC
M followed by 28 plasma P-selectin (p ⫽ 0.001), LDLC (p ⬍
days of a low fat, levels 0.001), and
high CHO diet apolipoprotein B level (p
(NCEP-1) or a ⫽ 0.002). Measurement
MD and vice of the endothelial function
versa. showed no differences in
the basal diameters of the
brachial artery, or in the
glyceryl trinitrate-induced
vasodilation. Flow
associated vasodilatation
of the brachial artery was
higher (p ⫽ 0.027) and
P-selectin levels were
lower (p ⫽ 0.003) after
the MD and the resistance
index after flow-
associated vasodilatation
and after glyceril
trinitrate-induced
vasodilatation were lower
during the MD
Nutrition Reviews姞, Vol. 64, No. 2Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
28
Muñoz et al., 2001 Barcelona, R-crossover- Primary 10 hyper- 6 weeks of a Serum lipid levels (TC, 6 weeks The walnut diet 2 TC (4.2%,
Spain CT prevention cholesterolemic cholesterol LDLC, HDLC, p ⫽ 0.176) and LDLC
M lowering MD, 6 VLDLC, TG level), (6.0%, p ⫽ 0.087). The
weeks on a diet apolipoprotein A-I, and apolipoprotein B level
with walnut B, and LDL declined in parallel with
replacing 35% of association to human LDLC (6.0%). The LDL
the energy from hepatoma cells from the walnut diet 1
MUFA or vice 50% the association rates to
Nutrition Reviews姞, Vol. 64, No. 2
versa the LDL receptor in human
hepatoma HepG2 cells (p ⬍
0.05). The LDL uptake by
HepG2 cells was correlated
with alfa-linoleic acid
content of the trygliceride
plus cholesteryl ester
fractions of LDL particles
(r2 ⫽ 0.42, p ⬍ 0.05)
Zambon et al., Barcelona, R-crossover- Primary 49 hyper- 6 weeks of a LDL fatty acids, serum 6 weeks The walnut diet caused a
200029 Spain CT prevention cholesterolemic cholesterol lipid levels (TC, bigger 2 TC, LDLC, and
subjects (28 M, lowering MD, 6 LDLC, HDLC, TG lipoprotein (a) (9%, 11.2%,
27 F) weeks of a diet level), lipoprotein (a) and 9.1% (p ⬍ 0.001)) vs.
with walnut levels, and LDL the MD diet which 2 TC
replacing 35% of resistance to in vitro and LDLC by 5% and
the energy from oxidative stress 5.6%; and lipoprotein (a)
MUFA by 3.4%. No effects on
HDLC, VLDLC, TG,
apolipoprot A-I. LDL
susceptibility to oxidation
was similar in both diets
Madigan et al., Dublin, R-crossover- Secondary 11 M DM2 2 weeks on a MUFA Fasting glucose and 2 weeks Fasting glucose and insulin
200030 Ireland CT prevention rich diet (30 ml insulin levels, plasma were higher on the PUFA
olive oil per day) cholesterol and LDLC, diet (p ⬍ 0.01 and
and 2 weeks on a fasting chylomicron ⬍0.002, respectively). TC
PUFA rich diet and VLDLC, and LDLC were higher on
(30 ml sunflower postprandial the PUFA diet (p ⬍
oil) and vice versa chylomicron and 0.001). Plasma TG and
VLDLC levels HDLC were similar.
Fasting chylomicron
components apoB48 (p ⬍
0.05) and apoB100 (p ⬍
0.02) and VLDL
S35Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
S36
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
phospholipid levels (p ⬍
0.02) were higher on the
PUFA diet. Postprandial
Chylomicron apoB48 and
apoB100 (p ⬍ 0.05),
VLDL apo B48 and B100
(p ⬍ 0.05), and VLDL
phospholipids (p ⬍ 0.01)
were higher on the PUFA
diet. The PUFA diet
produced an increased in
the phospholipids (p ⬍
0.01) and total fatty acids
(p ⬍ 0.05) LDL fasting
composition
Ryan et al., 200031 Dublin, clinical trial secondary 11 M DM2 2 months on a Insulin mediated glucose 2 months ⬍Fasting plasma insulin and
Ireland prevention PUFA rich diet transport, fatty acid ⬍ fasting insulin/glucose
and 2 months on a composition of the ratio (p ⬍ 0.02 and p ⬍
MUFA rich diet adipocyte membranes 0.002) with the MD diet.
(MD) and endothelium- The MD produced a ⬎
dependent and quantity of oleic acid (p ⬍
independent FMD. 0.0001) and ⬍ quantity of
linoleic acid (p ⬍ 0.0001)
and stearic acid (p ⬍ 0.01)
in the adipocyte membrane.
1 mean insulin-mediated
glucose transport with the
MD (0.29 ⫾ 0.14 and 0.56
⫾ 0.17 nmol/105 cells/3
min, at 1 ng/ml and 5 ng/ml
insulin with the linoleic
acid, and 0.53 ⫾ 0.18 and
0.79 ⫾ 0.28 mmol/103 cells/
3 min, at 1 ng/ml and 5 ng/
ml insulin with the oleic
acid) (p ⬍ 0.0001). 1
endothelium-dependent
FMD in the reactive
hyperaemia phase (p ⬍
0.0001) and 1 in the
glyceryl trinitrate-induced
Nutrition Reviews姞, Vol. 64, No. 2Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
FMD (p ⬍ 0.05) in the
MD. Correlation between
the ratio of adipocyte
membrane oleic/linoleic
acid and insulin-mediated
glucose transport at 1 g/
ml insulin (p ⬍ 0.001) and
at 5 ng/ml insulin (p ⬍
Nutrition Reviews姞, Vol. 64, No. 2
0.05) and this ratio with
the endothelium-dependent
FMD (p ⬍ 0.001)
Barbagallo C et al., Palermo, Clinical trial Secondary 78 renal transplant 24 weeks of usual Plasma lipid levels and 10–12 26.5% TG (p ⬍ 0.02), 2
199932 Italy prevention recipients (51 diet and 10–12 changes in lipid-related weeks 10.4% LDLC (p ⬍ 0.0001),
M, 27 F) weeks of MD cardiovascular risk 2 10.0 LDLC/HDLC (p ⬍
classes 0.001), 2TC and LDLC in
patients in “desirable
LDLC” (6.7% and 4.0%, p
⬍ 0.05), in “borderline
high-risk LDLC” (9.4% and
8.7%, p ⬍ 0.001) and in
“high-risk LDLC” (16.4%
and 19.7%, p ⬍ 0.0001).
2LDLC/HDLC in patients
in “borderline high-risk
LDLC” (6.8%, p ⬍ 0.05)
and in “high-risk LDLC”
(21.1%, p ⬍ 0.0001). 2TG
in patients in “desirable
LDLC” (12.3%, p ⬍ 0.01)
Leighton et al., Chile Clinical trial Primary 21 M 3 months on a MD Plasma vitamin C and E, 3 months The high fat diet 2 vitamin
199933 prevention or western diet. total plasma C levels, and 1 oxidative
The second month antioxidant capacity, DNA damage. The MD 1
red wine was oxidative DNA total plasma antioxidant
added to both damage in blood capacity (28%). Wine
diets leukocyte DNA, supplementation produced
endothelial function 1 plasma vit C (13.5%)
(flow mediated and total antioxidant
vascular reactivity) reactivity and a 2 vitamin
E (26%) and oxidative
DNA damage in the MD
group and a 2 vitamin E
S37S38
Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
(15%) and oxidative DNA
damage, 1 total
antioxidant reactivity. The
endothelial function was
suppressed by the high fat
diet and was normal after
wine supplementation
Pérez-Jiménez Córdoba, Clinical Primary 25 M 28 days on a low fat Serum lipid levels (TC, 28 days The MD diet 2 von
et al., 199934 Spain Trial Prevention NCEP-I-diet, or a LDLC, HDLC, TG Willebrand Factor, PAI-1,
MUFA-diet (MD) level), apolipoprotein TFPI plasma levels and
or a SFA-rich diet A-I, and B and 1lag time of conjugated
conjugated diene diene formation
formation after
incubation of LDL
particles with Cu.
Endothelial products
(von Willebrand
Factor, E-selectin,
Thrombomodulin and
Tissue Factor Pathway
inhibitor (TFPI)) levels
and plasminogen
activator inhibitor type
I (PAI-1) activity
Baroni et al., Italy Clinical trial Secondary Hyper- MUFA enriched diet LDL fatty acid The olive oil diet 1MUFA
199935 prevention cholesterolemic vs. a PUFA composition, LDL (11%) and 2PUFA (10%)
patients enriched diet susceptibility to concentrations on LDL
oxidation composition (p ⬍ 0.05).
The MUFA-enriched diet
2PUFA/MUFA ratio and
the unsaturation index. The
oleate-enriched LDL was
more resistant to oxidative
modifications.
Simoni et al., Italy Clinical trial Secondary 15 hyper- 2 months on a TC, Lipoprotein (a) 2 months 2Lipoprotein(a) 36.5 to 8.4
199536 prevention cholesterolemic Gemfibrozil (600 values mg/dl (p ⬍ 0.0002) and
with 1Lp(a) mg) treatment TC 254.5 to 208.0 mg/dl
patients combined with (p ⬍ 0.0001)
MD
Nutrition Reviews姞, Vol. 64, No. 2Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
37
Salen et al., 1994 France Clinical trial Secondary 41 hyper- 18 months of MD Platelet-aggregation, 18 months 2 platelet aggregation in
prevention cholesterolemic fasting plasma lipids response to trombine (p ⫽
heart transplant 0.02). Inverse correlation
M between linoleic acid intake
and platelet aggregation (r
⫽ ⫺0.44, p ⫽ 0.03). 2TC
and LDLC (p ⫽ 0.005 and
p ⫽ 0.04 respectively)
Nutrition Reviews姞, Vol. 64, No. 2
Moreno Vazquez Badajoz, Clinical trial Primary 90 pilots A. Uncontrolled diet TC, TG, HDLC, ⬍TC and TG in MD groups
et al., 199438 Spain prevention and exercise TC/HDLC ratio, and
programme, B. anxiety levels
MD and
uncontrolled
exercise, C. MD
and controlled
exercise
programme
Ferro-Luzzi et al., Italy Clinical trial Primary 48 M/F Shift from a MD to TC, LDLC, HDLC, 42 days In M 1TC 214 ⫾ 30 to 245
198439 prevention a MD high in apoprotein B ⫾ 33 mg/dl and 1LDLC
saturated fats and 19%, in F 1HDL (19%)
cholesterol and TC (16%).
1Apoprotein B in both
sexes
Ehnholm et al., North Clinical trial Primary 54 individuals MD TC, LDLC, apoprotein B, 6 weeks 2TC 263 ⫾ 8 to 201 ⫾ 5
198240 Karelia, prevention HDLC, apoprotein A-I mg/dl in M and 239 ⫾ 8
Finland and A-II to 188 ⫾ 8 mg/dl in F (p
⬍ 0.0001). 2LDLC and
apoprotein B. 2HDLC 54
⫾ 2 to 44 ⫾ 2 mg/dl in M
and 56 ⫾ 3 to 47 ⫾ 2 mg/
dl in F (p ⬍ 0.0001), 2
Apoprotein A-I
CARDIOVASCULAR
Barzi et al., 200341 Italy Clinical trial Secondary 11323 M/F Subjects received Association of food 6.5 years Compared with people in the
prevention surviving a MI advice to increase intakes (fish, fruit, raw worst dietary score quarter,
their consumption and cooked vegetables odds ratio for people in best
of fish, fruit, raw and olive oil), a score was 0.51 (95% CI
and cooked combined dietary score 0.44–0.59). 1 consumption
vegetables and and risk of death of each food was associated
olive oil with 2 risk of death.
S39Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
S40
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
42
Singh et al., 2002 Moradabad, RCT, single Secondary 1000 subjects with 499 individuals on a Non-fatal MI, fatal MI, 2 years adjusted rate ratios: non fatal
India blind prevention major risk indo-MD and 501 sudden cardiac death; MI: 0.47 (0.28–0.79), fatal
factors or controls on a total cardiac endpoints MI: 0.67 (0.31–1.42),
previous heart NCEP diet for 2 sudden cardiac death: 0.33
attack years (0.13–0.86) total cardiac end
points: 0.48 (0.33–0.71)
de Lorgeril et al., Lyon, RCT, single Secondary 423 subjects Randomisation to a CO1, cardiac death, non- 46 months The MD showed a 2CO1 (p
199943 France blind prevention surviving a MD group or fatal heart attack, CO2, ⫽ 0.0001) 2 CO2 (p ⫽
myocardial control group. 1 ⫹ unstable angina, 0.0001) and 2 CO3 (p ⫽
infarction stroke, heart failure, 0.0002)
pulmonary or peripheral
embolism, CO3 1 ⫹ 2
⫹ events requiring
hospitalisation
de Lorgeril et al., Lyon, RCT, single Secondary 605 subjects Randomisation to a Major primary end points 27 months Primary ⫹ major secondary
199644 France blind prevention surviving a MI MD group or (CV death, non fatal end points: risk ratio 0.24
control group. MI, Non-CV deaths), (95% CI 0.13 to 0.44, p ⬍
major secondary end 0.0001), major primary and
points (per procedural secondary end points ⫹
infarction, unstable minor end points: risk ratio
angina, nonfatal heart 0.63 (95% CI 0.46 to 0.87,
failure, stroke, p ⬍ 0.005)
pulmonary and
peripheral embolism),
minor secondary end
points (stable angina,
elective vascular
revascularization, post
angioplasty restenosis)
de Lorgeril et al., Lyon, RCT, single Secondary 605 subjects Randomisation to a Primary end points (deaths 27 months Risk ratio for: Cardiovascular
199445 France blind prevention surviving a MI MD group or from CV causes and deaths 0.24 (95% CI 0.07–
control group. non-fatal acute MI) and 0.85, p ⬍ 0.02), total
subsidiary end points major primary end points:
(non cardiac deaths and 0.27 (95% CI 0.12–0.59, p
unstable angina, post ⬍ 0.001), overall
infarct recurrent angina, mortality: 0.30 (95% CI
heart failure, stroke, 0.11–0.82 p ⬍ 0.02)
pulmonary and
peripheral embolism
and venous
trombophlebitis)
Nutrition Reviews姞, Vol. 64, No. 2Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
ARTHRITIS
Sköldstam et al., Sweden clinical trial Secondary 51 rheumathoid 12 weeks on either Disease Activity Index 12 weeks 2DAS28 ⫽ 0.56 (p ⬍
200346 prevention arthritis patients MD or control (DAS28), physical 0.001), 2HAQ ⫽ 0.15 (p
(10 M, 41 F) diet function index (HAQ), ⬍ 0.02), swollen joint
health survey of count (p ⫽ 0.001),
quality of life (SF36), improvement in pain VAS
daily consumption of (p ⫽ 0.006) and in two
NSAID dimensions of SF-36
Nutrition Reviews姞, Vol. 64, No. 2
Health Survey (p ⬍ 0.02).
NSAID use unaffected.
Hagfors et al., Sweden RCT Secondary 51 rheumatoid 3 months on either Antioxidant intake, 3 months The MD showed ⬎ intake of
200347 prevention arthritis patients MD or control plasma levels of vitamin E (p ⫽ 0.007) and
(10 M, 41 F) diet retinol, antioxidants (␣ selenium (p ⫽ 0.004) and
and ␥ tocopherol, - a ⬍ intake of retinol (p ⫽
carotene, lycopene, 0.049) excluding under and
vitamin C and uric over reporters. No changes
acid), and urinary in urine Malondialdehyde
Malondialdehyde or plasma levels of
antioxidants.
CANCER
de Lorgeril et al., Lyon, RCT Secondary 605 subjects MD group or control Occurrence of malignant 4 years 2risk in MD compared with
199848 France prevention surviving a MI group or non-malignant control subjects: 61% (p ⫽
tumor 0.05) for cancers and 56%
(p ⫽ 0.01) for the
combination of deaths and
cancer. The MD group
showed ⬎ levels of
vitamin C and E (p ⬍
0.05) and omega-3 fatty
acids (p ⬍ 0.001), and ⬍
levels of omega-6 fatty
acids measured 2 months
after randomisation
BODY COMPOSITION
Flynn et al., 200449 Australia Clinical trial Primary 41 individuals 41 individuals Change in body weight 3 months 24 individuals maintained the
prevention followed for 15 weight loss (8.18% of
months after weight lost) and 17
completing a 3 individuals regained the
S41
months MD weight lost.Table 1. (Cont’d) Clinical Trials on the Mediterranean Diet
S42
Author/Year
Publication Country Type of Study Population Methodology Outcome Follow Up Results
Fernandez de la Córdoba, Clinical trial Secondary 34 hyper- Every 17 subjects Body composition, 28 days Decreased in % fat when
Puebla et al., Spain prevention cholesterolemic underwent two plasma lipoproteins, changing from saturated fat
200350 M who dietary periods of fatty acids in to Mediterranean Diet (p ⬍
consumed a diet 28 days: cholesterol esters 0.05) or CHO rich diet (p ⬍
rich in saturated MD/carbohydrate 0.05). Lean mass increased
fat rich diet when changing from sat diet
to CHO diet (p ⬍ 0.05).
McManus et al., Boston, RCT Primary 101 overweight (10 MD versus low fat Change in body weight 18 months 24.1 Kg body weight, 21.6
200151 USA prevention M, 91 F) diet Kg/m2 BMI, 2 6.9 cm
waist circumference (p ⬍
0.001). 54% participants in
the MD group continued
after 18 months for 20% in
the control group.
PSYCHOLOGICAL FUNCTION
Hyyppä et al., 200352 Turku, R-crossover- Secondary 120 untreated MD versus Mood changes measured 12 weeks The MD produced no mood
Finland CT prevention hyper- simvastatin through a psychological changes nor changes in
cholesterolemic treatment distress scale (Brief steroid hormones. The MD
M Symptom Inventory), an 2TC by 7.7%
anger scale (State-Trait
Anger Inventory), and
two questionnaires to
measure aggression
based on the Strauss
Scale of Aggression,
Steroid Hormone levels
Wardle et al., 200053 London, RCT Secondary 176 hyper- 12 weeks of a low TC, LDLC, HDLC, TG, 12 weeks 2TC 10% (p ⬍ 0.001),
United prevention cholesterolemic fat diet, or MD or social functioning, 2LDLC 8.3% (p ⬍ 0.05),
Kingdom subjects control group mood and cognitive no changes in mood and
function aggression. Worse response
to one of the four cognitive
function tests (sustained-
attention task in the
intervention groups (p ⬍
0.001))
RCT ⫽ randomised clinical trial, CV ⫽ cardiovascular, MD ⫽ Mediterranean Diet, BMI ⫽ Body Mass Index, TC ⫽ Total Cholesterol, LDLC ⫽ LDL Cholesterol, TG ⫽ Tryglicerides, BP ⫽
Blood Pressure, MUFA ⫽ Monounsaturated Fat, LDL-PPD ⫽ LDL peak particle diameter, HDLC ⫽ HDL Cholesterol, SFA ⫽ Saturated fatty Acids, PUFA ⫽ Polyunsaturated Fat, CHO ⫽
carbohydrate, DM ⫽ Diabetes Mellitus, MI ⫽ myocardial infarction, FMD ⫽ flow mediated vasodilatation, BT ⫽ cutaneous bleeding time, vWF: Ag ⫽ von Willebrand factor antigen, vWF ⫽
Nutrition Reviews姞, Vol. 64, No. 2
von Willebrand Factor, CI ⫽ confidence interval, NSAID ⫽ non-steroidal anti-inflammatory drugs, VAS ⫽ visual analog scale.with more than 150 references, and more than 20% of tion, modified Mediterranean diets were associated with
them from the author himself, yet not one reference from remarkable reductions in CHD event rates and cardio-
Trichopoulou (author of 27 of the 70 articles related to vascular mortality in two secondary prevention trials
“diet and Cancer and Greece”). carried out in France (Lyon Diet Heart Study)43 and
Other examples in the area of obesity and the Med- India (Indo-Mediterranean diet Heart study).42 However,
iterranean diet56-58 put into evidence the lack of consen- no randomized, controlled trial has been conducted to
sus and objectivity that leads to reduced credibility of the assess to what extent a Mediterranean diet is superior to
research done in Mediterranean countries. the usually recommended low-fat diet in the primary
Mediterranean countries have been considered a prevention of cardiovascular disease and other chronic
difficult place to conduct reliable research (experimental diseases. Only two small clinical trials are currently
studies and large-scale cohort studies), not only due to being undertaken: the Mediet Project60 in Italy and the
the traditional subjectivism and lack of cooperation Medi-RIVAGE Study11 in France. The only large-scale
among researchers, but also because of the lack of ongoing clinical trial is running in Spain, the PRE-
commitment from the government and other institutions. DIMED Study, which is the most comprehensive and
Additionally, in the past, low priority was given to ambitious.
research careers, particularly in the area of nutrition.59 The Mediet Project60 is a randomized clinical trial
Fortunately, there has been rapid progress in recent being undertaken to investigate the potential impact of
years, and the number of original articles addressing the the traditional Mediterranean diet on the risk of devel-
Mediterranean diet have been increasing exponentially oping breast cancer in a sample of 115 women. The study
since 1999 (Figure 1). The rise of institutions and initi- is currently ongoing to verify the association of changes
atives dedicated to the Mediterranean diet, such as the in serum and urine hormone levels and breast cancer risk
Foundation for Advancement of Mediterranean diet, in the intervention group, who attended a weekly cook-
which was founded in 1996, may have contributed to ing course for one year.
this. The Medi RIVAGE study11 (Mediterranean diet,
Most of the trials analyzed had a limited number of Cardiovascular Risks and Gene Polymorphisms) is a
participants (24 of 43 articles included less than 60 randomized clinical trial developed in France conducted
participants in the sample), but the most important lim- in a sample of 212 males and females with at least one
itation is the different methodology used to define the cardiovascular risk factor. The study has two main goals.
intervention. Some authors characterized the Mediterra- The first one is the prevention of cardiovascular diseases
nean diet just as a monounsaturated fatty acid-rich or by evaluating the effect of two diets (a Mediterranean-
-enriched diet; others by additional supplementation with type diet and a low-fat, low-cholesterol diet) on arterio-
walnuts or wine, but only a few defined a score or pattern sclerosis risk factors. The second goal is to implement
of the Mediterranean diet. This is probably one of the extensive biological investigation in relation to the di-
major weaknesses of these experimental studies. Chang- etary intervention, with a special interest on fasting and
ing a group of persons to a particular dietary profile is postprandial examinations of lipid parameters and li-
hard to achieve and particularly difficult to maintain and poproteins, as well as some genetic polymorphisms that
guarantee compliance. influence lipoprotein metabolism and homeostasis. The
This review shows that the results of the following study is still ongoing. The data at 3 months of follow-up
studies are of special importance: the Lyon Diet Heart show that in subjects at risk, changing to a Mediterra-
Study,43 the Indo Mediterranean Heart Study,42 the nean-type diet improves blood biochemical parameters.
GISSI Prevention Trial for Secondary Prevention,41 the The PREDIMED Study (PREDIMED meaning
study by Esposito et al.12 on metabolic syndrome, and PREvención con DIeta MEDiterránea) was initiated in
also three ongoing trials on primary prevention: the October 2003 with the recruitment of participants for this
Mediet Project60 in Italy, the Medi-RIVAGE Study11 in primary prevention trial. This parallel group, multi-cen-
France, and the PREDIMED study in Spain. ter, randomized study was designed in 2002 and funded
However, most of the small clinical studies analyzed by a grant from the official biomedical research agency
in this review contributed greatly to explaining the mech- of the Spanish government, the Spanish Ministry of
anisms of how the Mediterranean diet itself or some of its Health. The PREDIMED Study is the first large-scale,
components improve certain biological variables and long-term clinical trial that enrolls high-risk patients to
affect disease outcomes. follow a Mediterranean diet supplemented with extra
Recent findings from two large European cohort virgin olive oil or nuts for primary cardiovascular disease
studies61,62 have suggested that a high degree of adher- prevention. The US Food and Drug Administration
ence to the Mediterranean diet is associated with a (FDA) has very recently approved a health claim for
reduction in both total and coronary mortality. In addi- olive oil as a putative cardio-protective food.63 However,
Nutrition Reviews姞, Vol. 64, No. 2 S43in this era of evidence-based medicine, definite medical baseline visit includes: 1) a general questionnaire; 2) a
advice and treatment should be supported by the results food-frequency questionnaire with 137 foods plus infor-
of randomized clinical trials with clinical events as pri- mation on vitamin supplements and alcohol consumption
mary outcomes. The results of the PREDIMED Study (adapted from the Nurses’ Health Study questionnaire
could provide the firm evidence required to issue dietary and validated in Spain); 3) the Minnesota physical ac-
guidelines for sound clinical practice. tivity questionnaire (validated Spanish version); 4) mea-
The primary outcome to be evaluated in this trial is surement of weight, height, waist circumference, blood
a composite end point of cardiovascular death, non-fatal pressure, and ankle-brachial blood pressure index; 5)
myocardial infarction, and non-fatal stroke. As second- collection of fasting blood samples and preparation of
ary outcomes, death by any cause and incidence of serum, plasma, and buffy-coat aliquots; 6) collection of
angina leading to a revascularization procedure, heart urine samples and toenail specimens; and 7) a 47-item
failure, diabetes mellitus, dementia, and cancer were general questionnaire with information about risk factors
included. Finally, other outcomes such as changes in and medication use. The same assessment is performed
blood pressure, body weight, adiposity measures, blood in the yearly visits, except that the initial questionnaire is
sugar, lipid profile, markers of inflammation, and other substituted by a follow-up questionnaire, which includes
intermediate markers of cardiovascular risk will also be new medical diagnoses and medication. Since the infor-
measured. mation from the food-frequency questionnaire provides
A sample size of 9000 with randomization to three only a subjective assessment of compliance, biological
equally sized groups (two intervention groups and one markers (plasma fatty acids and urinary tyrosol and
control group, with 3000 patients each) will provide hydroxytyrosol)64,65 are measured in a random subset
sufficient statistical power to evaluate the effect of the (10%) of participants from the three arms of the trial to
Mediterranean diet on the primary outcome. Participants objectively evaluate intervention compliance.
are free-living high-risk persons age 55 to 80 years for Participants initially recruited will be followed for
men and 60 to 80 years for women with no history of up to 5 years, and those entering later will be followed
cardiovascular disease, who fulfill at least one of the two for at least 4 years. Consequently, we expect a median
following criteria: 1) type 2 diabetes, 2) three or more of follow-up above 4 years. Primary and secondary out-
these risk factors: current smoker, hypertension, LDL comes will be detected by the primary care physicians
cholesterol ⱖ160 mg/dL, HDL cholesterol ⱕ 40 mg/dL, of each participant and confirmed by a clinical events
subcommittee. It is our hope that the results of the
BMI ⱖ 25 kg/m2, or a family history of premature CHD.
PREDIMED trial will provide strong evidence to estab-
The participants included as controls receive recom-
lish dietary guidelines to enforce sound clinical practice
mendations to follow a low-fat diet according to the
and public health policy within the Mediterranean Basin.
American Heart Association guidelines. The two inter-
Mediterranean diet recommendations need to be
vention group assignments are designated by allotment
evidence based, which requires the development of clin-
of either olive oil (15 liters⫽1 liter/week for 15 weeks)
ical and observational epidemiology in Mediterranean
or packets of walnuts, hazelnuts, and almonds (1350 g
countries. Also, objective systematic (non-personalized)
walnuts ⫽ 15 g/d, 675 g hazelnuts ⫽ 7.5 g/d, and 675 g
reviews need to address different areas of the relation-
almonds ⫽ 7.5 g/d for 90 days), together with instruc-
ship between Mediterranean diet and health.66 Other-
tions about their use and conservation. In the intervention
wise, the promotion of the Mediterranean diet will al-
groups, personalized advice regarding dietary changes
ways have shortcomings and thus continue to be viewed
with the aim of achieving an ideal Mediterranean diet is
with certain misgivings.
given. A leaflet with written information about the main
food components and cooking habits of the Mediterra-
ACKNOWLEDGMENTS
nean diet is provided, together with recommendations on
the desired frequency of intake of specific foods. A group
The authors would like to thank Lourdes Ribas and
session with up to 20 participants, with separate sessions
Joy Ngo for their assistance with the preparation and
for each of the two Mediterranean diet groups, is sched-
editing of the document.
uled every 3 months and consists of informative talks
and the provision of written material with elaborate
REFERENCES
descriptions of typical Mediterranean foods and shop-
ping lists, meal plans, and recipes adapted to the season 1. Keys A, Menotti A, Karoven MI. The diet and the
of the year. Each session includes three steps: assess- 15-year death rate in the Seven Countries Study.
Am J Epidemiol. 1986;124:903–915.
ment, intervention, and future directions. 2. Tunstall-Pedoe H, Kuulasmaa K, Mahonen M, et al.
Major measurements and data collection activities Contribution of trends in survival and coronary-
also take place at baseline and each subsequent year. The event rates to changes in coronary heart disease
S44 Nutrition Reviews姞, Vol. 64, No. 2mortality: 10 years results from 37 WHO MONICA obtained from blood during Mediterranean or high
project populations. Monitoring trends and determi- carbohydrate diets. Nutr Metab Cardiovasc Dis.
nants in cardiovascular disease. Lancet. 1999;353: 2004;14:128 –132.
1547–1557. 19. Toobert DJ, Glasgow RE, Strycker LA, et al. Bio-
3. Masiá R, Pena J, Marrugat J, et al. High prevalence logic and quality-of-life outcomes from the Mediter-
of cardiovascular risk factors in Gerona, Spain, a ranean Lifestyle Program: a randomized clinical
province with low myocardial infarction incidence. trial. Diabetes Care. 2003;26:2288 –2293.
REGICOR investigators. J Epidemiol Comm Health. 20. Rodrı́guez-Villar C, Pérez-Heras A, Mercadé I, et al.
1998;52:707–715. Comparison of a high-carbohydrate and a high
4. Helsing E, Trichopoulou A. The Mediterranean diet monounsaturated fat, olive oil-rich diet on the sus-
and food culture: a symposium. Eur J Clin Nutr. ceptibility of LDL to oxidative modification in sub-
1989;43(suppl 1):1–92. jects with type 2 diabetes mellitus. Diabet Med.
5. Serra Majem L, Helsing E. Changing patterns of fat 2004;21:142–149.
intake in Mediterranean countries. Eur J Clin Nutr. 21. Goulet J, Lamarche B, Nadeau G, Lemieux S. Effect
1993;47(suppl 1):1–100. of a nutritional intervention promoting the Mediter-
6. Nestle E. Mediterranean diets: science and policy ranean food pattern on plasma lipids, lipoproteins
implications. Am J Clin Nutr. 1995;61(suppl 6):1313– and body weight in healthy French-Canadian
1427. women. Atherosclerosis. 2003;170:115–124.
7. Willett WC, Sacks F, Trichopoulou A, et al. Mediter- 22. Sondergaard E, Moller JE, Egstrup K. Effect of
ranean diet pyramid: a cultural model for healthy dietary intervention and lipid-lowering treatment on
eating. Am J Clin Nutr. 1995;61(suppl 6):1402–1406. brachial vasoreactivity in patients with ischemic
8. Trichopoulou A, Lagiou P. Healthy traditional Med- heart disease and hypercholesterolemia. Am
iterranean diet: an expression of culture, history, Heart J. 2003;145:19.
and lifestyle. Nutr Rev. 1997;55:383–389. 23. Mezzano D, Leighton F, Strobel P, et al. Mediterra-
9. Serra Majem L, Ngo de la Cruz J (eds). ¿Qué es la nean diet, but not red wine, is associated with
dieta Mediterránea?. Barcelona: Nexus Ediciones. beneficial changes in primary haemostasis. Eur
2002:1–221. J Clin Nutr. 2003;57:439 – 446.
10. Serra Majem L, Trichopoulou A, Ngo de la Cruz J, et 24. Singh N, Graves J, Taylor PD, et al. Effects of a
al. Foreword: does the definition of the Mediterra-
‘healthy’ diet and of acute and long-term vitamin C
nean diet need to be updated? Public Health Nutr.
on vascular function in healthy older subjects. Car-
2004;7:927–929.
diovasc Res. 2002;56:118 –125.
11. Vincent S, Gerber M, Bernard MC, et al. The Medi-
25. Perez-Jimenez F, Lopez-Miranda J, Pinillos MD, et
RIVAGE study (Mediterranean diet, cardiovascular
al. A Mediterranean and a high-carbohydrate diet
risks and gene polymorphisms): rationale, recruit-
improve glucose metabolism in healthy young per-
ment, design, dietary intervention and baseline
sons. Diabetologia. 2001;44:2038 –2043.
characteristics of participants. Public Health Nutr.
26. Mezzano D, Leighton F, Martinez C, et al. Comple-
2004;7:531–542.
mentary effects of Mediterranean diet and moderate
12. Esposito K, Marfella R, Ciotola M, et al. Effect of a
Mediterranean-style diet on endothelial dysfunction red wine intake on haemostatic cardiovascular risk
and markers of vascular inflammation in the meta- factors. Eur J Clin Nutr. 2001;55:444 – 451.
bolic syndrome: a randomized trial. JAMA. 2004; 27. Fuentes F, Lopez-Miranda J, Sanchez E, et al. Med-
292:1440 –1446. iterranean and low-fat diets improve endothelial
13. Ros E, Nunez I, Perez-Heras A, et al. A walnut diet function in hypercholesterolemic men. Ann Intern
improves endothelial function in hypercholester- Med. 2001;134:1115–1159.
olemic subjects: a randomized crossover trial. Cir- 28. Muñoz S, Merlos M, Zambon D, et al. Walnut-
culation. 2004;109:1609 –1614. enriched diet increases the association of LDL from
14. Ambring A, Friberg P, Axelsen M, et al. Effects of a hypercholesterolemic men with human HepG2
Mediterranean-inspired diet on blood lipids, vascu- cells. J Lipid Res. 2001;42:2069 –2076.
lar function and oxidative stress in healthy subjects. 29. Zambon D, Sabate J, Munoz S, et al. Substituting
Clin Sci. 2004;106:519 –525. walnuts for monounsaturated fat improves the se-
15. Goulet J, Lamarche B, Charest A, et al. Effect of a rum lipid profile of hypercholesterolemic men and
nutritional intervention promoting the Mediterra- women. A randomized crossover trial. Ann Intern
nean food pattern on electrophoretic characteristics Med. 2000;132:538 –546.
of low-density lipoprotein particles in healthy 30. Madigan C, Ryan M, Owens D, et al. Dietary unsat-
women from the Quebec City metropolitan area. urated fatty acids in type 2 diabetes: higher levels of
Br J Nutr. 2004;92:285–293. postprandial lipoprotein on a linoleic acid-rich sun-
16. Flynn G, Colquhoun D. Mediterranean diet improves flower oil diet compared with an oleic acid-rich olive
lipid profiles over three months. Asia Pac J Clin oil diet. Diabetes Care. 2000;23:1472–1477.
Nutr. 2004;13(suppl):S138. 31. Ryan M, McInerney D, Owens D, et al. Diabetes and
17. Urquiaga I, Guasch V, Marshall G, et al. Effect of the Mediterranean diet: a beneficial effect of oleic
Mediterranean and occidental diets, and red wine, acid on insulin sensitivity, adipocyte glucose trans-
on plasma fatty acids in humans. An intervention port and endothelium-dependent vasoreactivity.
study. Biol Res. 2004;37:253–261. QJM. 2000;93:85–91.
18. Bravo-Herrera MD, Lopez-Miranda J, Marin C, et al. 32. Barbagallo CM, Cefalu AB, Gallo S, et al. Effects of
Tissue factor expression is decreased in monocytes Mediterranean diet on lipid levels and cardiovascu-
Nutrition Reviews姞, Vol. 64, No. 2 S45You can also read