Evaluation of Outcomes With Citalopram for Depression Using Measurement-Based Care in STAR*D: Implications for Clinical Practice
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Article
Evaluation of Outcomes With Citalopram for Depression
Using Measurement-Based Care in STAR*D:
Implications for Clinical Practice
Madhukar H. Trivedi, M.D. Objective: Selective serotonin reuptake Results: Nearly 80% of the 2,876 outpa-
inhibitors (SSRIs) are widely used to treat tients in the analyzed sample had chronic
depression, but the rates, timing, and base- or recurrent major depression; most also
A. John Rush, M.D. line predictors of remission in “real world” had a number of comorbid general medi-
patients are not established. The authors’ cal and psychiatric conditions. The mean
Stephen R. Wisniewski, Ph.D. primary objectives in this study were to exit citalopram dose was 41.8 mg/day. Re-
evaluate the effectiveness of citalopram, mission rates were 28% (HAM-D) and 33%
Andrew A. Nierenberg, M.D. an SSRI, using measurement-based care in
(QIDS-SR). The response rate was 47%
actual practice, and to identify predictors
(QIDS-SR). Patients in primary and psychi-
of symptom remission in outpatients with
Diane Warden, Ph.D., M.B.A. atric care settings did not differ in remis-
major depressive disorder.
sion or response rates. A substantial por-
Louise Ritz, M.B.A. Method: This clinical study included out- tion of participants who achieved either
patients with major depressive disorder
response or remission at study exit did so
who were treated in 23 psychiatric and 18
Grayson Norquist, M.D. primary care “real world” settings. The pa-
at or after 8 weeks of treatment. Partici-
pants who were Caucasian, female, em-
tients received flexible doses of citalopram
Robert H. Howland, M.D. ployed, or had higher levels of education
prescribed by clinicians for up to 14 weeks.
or income had higher HAM-D remission
The clinicians were assisted by a clinical re-
rates; longer index episodes, more concur-
Barry Lebowitz, Ph.D. search coordinator in the application of
measurement-based care, which included rent psychiatric disorders (especially anxi-
the routine measurement of symptoms ety disorders or drug abuse), more general
Patrick J. McGrath, M.D. medical disorders, and lower baseline
and side effects at each treatment visit and
the use of a treatment manual that de- function and quality of life were associated
Kathy Shores-Wilson, Ph.D. scribed when and how to modify medica- with lower HAM-D remission rates.
tion doses based on these measures. Re-
Conclusions: The response and remis-
Melanie M. Biggs, Ph.D. mission was defined as an exit score of ≤7
on the 17-item Hamilton Depression Rat- sion rates in this highly generalizable sam-
ing Scale (HAM-D) (primary outcome) or a ple with substantial axis I and axis III co-
G.K. Balasubramani, Ph.D. morbidity closely resemble those seen in
score of ≤5 on the 16-item Quick Inventory
of Depressive Symptomatology, Self-Re- 8-week efficacy trials. The systematic use
Maurizio Fava, M.D. port (QIDS-SR) (secondary outcome). Re- of easily implemented measurement-
sponse was defined as a reduction of ≥50% based care procedures may have assisted
STAR*D Study Team in baseline QIDS-SR score. in achieving these results.
(Am J Psychiatry 2006; 163:28–40)
R emission, the virtual absence of symptoms, is the
aim of depression treatment because it is associated with
remission, lower rates of relapse, lower risk of suicide and
alcohol/drug abuse, and lack of disabling symptoms (1–3).
better function and a better prognosis than is response Few efficacy studies, even in research settings, have em-
without remission. Response is typically defined as a clin- ployed remission as an outcome (4–7). Remission rates
ically meaningful reduction in symptoms (e.g., a reduction from research-based, 8-week, randomized, placebo-con-
of at least 50% in baseline symptom levels). However, re- trolled efficacy trials with depressed, symptomatic volun-
sponse that falls short of remission is suboptimal because teers range from 25% to 40% (4), and 12-week efficacy tri-
it is associated with continued disabling symptoms, nega- als with subjects suffering from chronic depression reveal
tive effects on other axis I and axis III disorders, higher even more modest remission rates of 22%–30% (8, 9).
rates of relapse and recurrence, poorer work productivity, Results from these efficacy trials lack ecological validity
more impaired psychosocial functioning, higher levels of and generalizability to clinical practice (10, 11). Typically,
health care use, and potentially higher risk for suicide. Re- they enroll symptomatic volunteers (often recruited through
mission, on the other hand, is associated with return of advertising) with uncomplicated (minimal comorbid gen-
normal psychosocial function, higher rates of sustained eral medical or psychiatric conditions), nonchronic, non-
28 http://ajp.psychiatryonline.org Am J Psychiatry 163:1, January 2006TRIVEDI, RUSH, WISNIEWSKI, ET AL.
substance-abusing, nonsuicidal depression and treat in disorder, length of the current major depressive episode,
research clinics as opposed to enrolling patients already number of major depressive episodes, length of illness,
seeking health care in typical clinical treatment settings. course of illness [single or recurrent], major depressive
Unfortunately, no large-scale antidepressant medication disorder subtype [anxious, melancholic, and atypical fea-
trials have evaluated safety, efficacy, and tolerability in tures], family history of depression, concurrent general
“real world” primary or psychiatric care settings with re- medical and axis I psychiatric disorders, symptom sever-
mission as the predefined primary endpoint. ity, and functional status at baseline).
Evidence from practice settings (12) also demonstrates This report addresses the following questions about
that antidepressant medication treatment is often inade- treatment with citalopram, a representative of the SSRI
quate in dose and/or duration and that there are unac- class of medications:
ceptably high dropout rates—all of which likely contribute
1. What are the remission and response rates in represen-
to lower remission rates. In the available effectiveness tri-
tative outpatients with nonpsychotic major depressive
als conducted in real clinical practice settings, even the
disorder in primary and psychiatric care settings?
addition of depression care specialists leads to modest re-
2. Which citalopram doses, treatment durations, and
mission rates (15% to 35%) (10, 13, 14).
adverse events characterize patients who do or do
The Sequenced Treatment Alternatives to Relieve De-
not achieve remission?
pression (STAR*D) study was designed to assess effective-
3. What pretreatment features in demographic, social,
ness of treatments in generalizable samples and ensure
and clinical domains are associated with remission?
the delivery of adequate treatments. The study aimed to
define the symptomatic outcomes for outpatients with
nonpsychotic major depressive disorder treated initially Method
with citalopram, a prototype of selective serotonin re- Study Overview and Organization
uptake inhibitors (SSRIs). The primary outcome was re-
The rationale, methods, and design of the STAR*D study have
mission. Adequate doses of citalopram had to be given for been detailed elsewhere (7, 36). Investigators at each of 14 re-
a sufficient time period to ensure that an adequate treat- gional centers across the United States oversaw protocol imple-
ment trial was conducted to assess efficacy in representa- mentation at two to four clinical sites providing primary (N=18)
tive practice settings and to ensure that those patients or psychiatric (N=23) care to patients in both the public and pri-
who progressed to the next treatment step in STAR*D were vate sectors. Clinical research coordinators at each clinical site as-
sisted participants and clinicians in protocol implementation
truly treatment resistant. To that end, a systematic but and collection of clinical measures. A central pool of research out-
easily implemented approach to treatment, measure- come assessors conducted telephone interviews to obtain pri-
ment-based care, was developed. Measurement-based mary outcomes.
care includes the routine measurement of symptoms and
Participants
side effects at each treatment visit and the use of a treat-
All risks, benefits, and adverse events associated with STAR*D
ment manual describing when and how to modify medi-
participation were explained to subjects, who provided written in-
cation doses based on these measures. The manual allows formed consent before entering the study. The University of Texas
for flexible dosing and was designed to maximize ade- Southwestern Medical Center at Dallas and the institutional re-
quate dosing and duration of treatment. view boards at each clinical site and regional center and the Data
Finally, since most depressed patients do not achieve re- Coordinating Center and the Data Safety and Monitoring Board of
the National Institute of Mental Health (NIMH) approved and
mission with any initial treatment, baseline features (mod-
monitored the protocol.
erators) that identify who will achieve remission (15, 16) To maximize generalizability of findings, only patients seeking
are clinically important. With a rare exception (17), no ade- medical care in routine medical or psychiatric outpatient treat-
quately powered previous studies have searched for base- ment (as opposed to those recruited through advertisements)
line features predicting which patients will achieve remis- were eligible for the study. Minimal exclusion criteria and broad
inclusion criteria that allowed a majority of axis I and axis II disor-
sion as opposed to those who will respond to treatment.
ders were used. Outpatients who were 18–75 years of age and had
Response moderator studies with small samples have a nonpsychotic major depressive disorder determined by a base-
yielded inconsistent correlates of response (18), except for line 17-item Hamilton Depression Rating Scale (HAM-D) (37, 38)
pretreatment depressive symptom severity, which has score ≥14 were eligible if their clinicians determined that outpa-
been associated consistently with lower response rates tient treatment with an antidepressant medication was both safe
and indicated. The initial HAM-D at study entry was administered
(19–35). Therefore, STAR*D also aimed to evaluate moder-
and scored by the clinical research coordinators. Patients who
ators of symptom remission. were pregnant or breast-feeding and those with a primary diagno-
This study defined remission as the a priori primary sis of bipolar, psychotic, obsessive-compulsive, or eating disorders
endpoint and divided baseline moderators into three do- were excluded from the study, as were those with general medical
mains: 1) demographic features (e.g., age, race, ethnicity, conditions contraindicating the use of protocol medications in the
first two treatment steps, substance dependence (only if it re-
and gender), 2) social features (e.g., education, employ- quired inpatient detoxification), or a clear history of nonresponse
ment status, income, insurance, and marital status), and or intolerance (in the current major depressive episode) to any
3) clinical features (e.g., age at onset of major depressive protocol antidepressant in the first two treatment steps (7).
Am J Psychiatry 163:1, January 2006 http://ajp.psychiatryonline.org 29MEASUREMENT-BASED CARE IN STAR*D
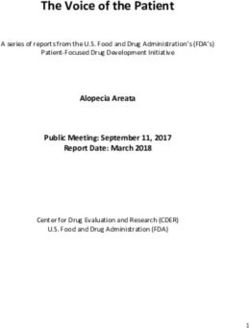
FIGURE 1. Participant Flow (CONSORT Chart) for the comes were based on the QIDS-SR collected at baseline and at
Sequenced Treatment Alternatives to Relieve Depression each treatment visit.
(STAR*D) Study An automated, telephonic, interactive voice response system
(7, 50–52) was used to collect ratings on the 12-item Short-Form
Health Survey (53) (perceived physical functioning and mental
Screened Not offered consent health functioning), the 16-item Quality of Life Enjoyment and
or refused to consent Satisfaction Questionnaire (54), the Work and Social Adjustment
(N=4,790)
(N=613) Scale (55), and the 5-item Work Productivity and Activity Im-
pairment (56).
Consented Ineligible Intervention and Measurement-Based Care
(N=4,177) (N=136) Citalopram was selected as a representative SSRI given the ab-
sence of discontinuation symptoms, demonstrated safety in el-
derly and medically fragile patients, once-a-day dosing, few dose
Eligible HAM-D scoreTRIVEDI, RUSH, WISNIEWSKI, ET AL.
TABLE 1. Baseline Characteristics of 2,876 Outpatients With TABLE 1. Baseline Characteristics of 2,876 Outpatients With
Nonpsychotic Major Depressive Disordera Nonpsychotic Major Depressive Disordera (continued)
Characteristic N % Mean SD Characteristic N % Mean SD
Demographic domain Clinical domain
Race
Caucasian 2,180 75.8 Age at onsetMEASUREMENT-BASED CARE IN STAR*D
TABLE 2. Treatment Characteristics and End-of-Study Remission Status of 2,876 Outpatients With Nonpsychotic Major
Depressive Disordera
Characteristic No Remission (N=2,086) Remission (N=790) Total (N=2,876)
N % N % N %
Maximum dose of citalopram (mg/day)TRIVEDI, RUSH, WISNIEWSKI, ET AL.
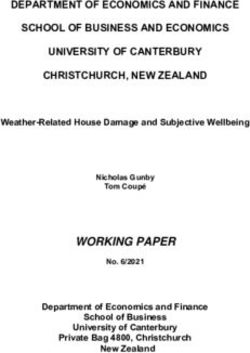
FIGURE 2. Total Exit Scores on the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), of 2,876
Outpatients With Nonpsychotic Major Depressive Disorder
No depression Mild symptoms Moderate symptoms Severe symptoms Very severe symptoms
8
7
6
Percent
5
4
3
2
1
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Last QIDS-SR Score
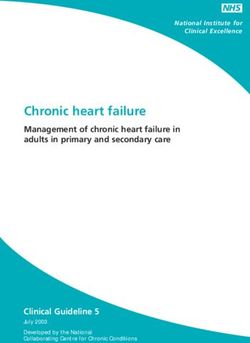
Symptomatic Outcomes FIGURE 3. Percent of 2,876 Outpatients With Nonpsychotic
Major Depressive Disorder Who Achieved Response or Re-
The overall remission rate was 27.5% (N=790) with the mission Defined by 16-Item Quick Inventory of Depressive
HAM-D definition (primary outcome) and 32.9% (N=943) Symptomatology, Self-Report (QIDS-SR), Scores by Week of
Treatmenta
with the QIDS-SR definition. Remission rates were com-
parable in primary and psychiatric care for the HAM-D 25
(26.6% versus 28.0%) and the QIDS-SR (32.5% versus Remission (N=943)
33.1%). The overall QIDS-SR response rate was 47% (N= Response (N=1,343)
1,343) (46% primary care, 48% psychiatric care). Figure 2 20
shows the distribution of the exit QIDS-SR scores. A QIDS-
SR score of 10 approximates an HAM-D score of 13 (45).
15
Figure 3 shows the distribution of the time to first
Percent
remission and response for those who ultimately did
achieve remission and response in this study based on 10
QIDS-SR scores. For those who achieved QIDS-SR re-
mission, the mean time to remission was 6.7 weeks (SD=
3.8) and was comparable in primary care (approximately 6 5
weeks) and psychiatric care (approximately 7 weeks). For
those who achieved a QIDS-SR response, the mean time to
response was approximately 5.7 weeks (SD=3.5) and was 0
2 4 6 8 10 12 ≥13
comparable in primary care (mean=5.7 weeks, SD=3.7)
Week of Treatment
and psychiatric specialty care (mean=5.6 weeks, SD=3.5).
a Response was defined as improvement of ≥50% in QIDS-SR score
For those who achieved remission according to QIDS- from baseline. Remission was defined as a QIDS-SR score of ≤5 at
SR scores, the mean time in treatment was approximately endpoint.
12 weeks (SD=3).
Intolerance and Adverse Events Pretreatment Correlates of Remission
Only 2% of the patients who achieved HAM-D remis- Several pretreatment demographic, social, and clinical
sion were considered to have discontinued citalopram features were associated with remission based on either
because of intolerance, compared with 11% of those who the HAM-D or QIDS-SR following adjustments for base-
did not achieve HAM-D remission (Table 3). Those who line symptom severity and regional center (Table 4). Find-
achieved HAM-D remission had lower rates of side effect ings were almost identical for the HAM-D and the QIDS-
frequency, intensity, and burden at exit and lower rates of SR except that anxious depression and concurrent gener-
serious adverse effects than those who did not achieve alized anxiety disorder were also associated with lower
HAM-D remission. Overall, 116 participants experienced QIDS-SR remission rates.
at least one serious adverse effect; most of these patients Table 5 presents pretreatment features that were non-
(88.8% [N=103]) did not achieve HAM-D remission. There overlapping and independently associated with remission
were no suicides in the 2,876 participants in this acute- after baseline depressive symptom severity and regional
phase citalopram study. center for each domain separately and across all domains
Am J Psychiatry 163:1, January 2006 http://ajp.psychiatryonline.org 33MEASUREMENT-BASED CARE IN STAR*D
TABLE 3. Adverse Events, Side Effects, Attrition, and End-of-Study Remission Status of 2,876 Outpatients With Non-
psychotic Major Depressive Disordera
No Remission (N=2,086) Remission (N=790) Total (N=2,876)
Adverse Events, Side Effects, and Attrition N % N % N %
Maximum side effect frequencyb
None 320 15.4 128 16.2 448 15.7
10%–25% of the time 535 25.8 273 34.6 808 28.2
50%–75% of the time 681 32.9 233 29.6 914 31.9
90%–100% of the time 537 25.9 154 19.5 691 24.2
Maximum side effect intensityb
None 315 15.2 127 16.1 442 15.5
Trivial–mild 510 24.6 283 35.9 793 27.7
Moderate–marked 871 42.0 302 38.3 1,173 41.0
Severe–intolerable 377 18.2 76 9.6 453 15.8
Maximum side effect burdenb
No impairment 402 19.4 181 23.0 583 20.4
Minimal–mild impairment 771 37.2 403 51.1 1,174 41.0
Moderate–marked impairment 695 33.5 169 21.5 864 30.2
Severe impairment, unable to function 205 9.9 35 4.4 240 8.4
Serious adverse events
Total 103 4.9 13 1.6 116 4.0
Death, nonsuicide 3 — 0 — 3 —
Hospitalization for general medical conditions 47 — 11 — 58 —
General medical conditions without hospitalization 4 — 0 — 4 —
Psychiatric hospitalization 50 — 2 — 52 —
Suicidal ideation (without hospitalization)c 6 — 0 — 6 —
Any psychiatric serious adverse eventd 55 2.6 2 0.3 57 2.0
Intolerance 234 11.2 13 1.6 247 8.6
a Remission was defined as an exit score of ≤7 on the 17-item Hamilton Depression Rating Scale (HAM-D). Subjects with missing exit HAM-D
scores were considered not in remission. Numbers do not always add up to total N because of missing data; percents are based on number
of subjects for whom data were available.
b Maximum ratings of intensity, frequency, and burden of side effects are the highest ratings during citalopram treatment.
c Includes psychiatric hospitalization and suicidal ideation without hospitalization.
d Includes hospitalizations for worsening depression, substance abuse, suicidal ideation, and other.
were controlled for. Lower remission rates were associated pression (22%) (9), possibly because of a number of factors
with being unemployed; having a lower income; being discussed below, including the use of measurement-based
non-Caucasian, male, and less educated; and having care and the clinical research coordinators.
poorer function and lower quality of life at baseline. Re- Higher remission rates were found with the QIDS-SR
markably consistent findings were obtained with the HAM- than with the HAM-D because our primary analyses classi-
D and the QIDS-SR. fied patients with missing exit HAM-D as nonremitters a
priori. Of the 690 patients with missing exit HAM-D scores,
Discussion 152 (22.1%) achieved QIDS-SR remission at the last treat-
ment visit.
Results of this study should be generalizable to routine As described earlier, a sensitivity analysis was con-
clinical practice because this is the largest ecologically ducted to evaluate the methods used to address the miss-
valid “real world” study of outpatients with nonpsychotic ing HAM-D data. Both the multiple imputation approach
major depressive disorder treated in psychiatric and pri- and the use of values imputed from the observed exit QIDS-
mary care settings with diligently followed guidelines. C score based on item response theory revealed remark-
Participants in the study were patients seeking treatment ably similar findings, indicating that the analyses were not
in “real world” clinical practices who had high rates of affected by the missing data methodology.
chronic or recurrent major depressive disorder and con- Of participants who responded, 56.0% did so only at or
current axis I and axis III (general medical conditions) dis- after 8 weeks of treatment. Not surprisingly, remission fol-
orders. Since there were very broad inclusion criteria and lowed response in most cases. Of those who achieved
few exclusion criteria, this study included patients who QIDS-SR remission, 40.3% did so only at or after 8 weeks of
would have been excluded from most efficacy trials (58– citalopram.
61). Results also highlight the feasibility, safety, tolerability,
The remission rates (28% for HAM-D; 33% for QIDS-SR) and effectiveness of delivering high-quality care with
were robust and similar to rates found in uncomplicated, easy-to-use clinical methods employed at each treatment
nonchronic symptomatic volunteers enrolled in placebo- visit to ensure adequate treatment delivery (measure-
controlled, 8-week, randomized, controlled trials with ment-based care approach). The approach may have con-
SSRIs (4). These remission rates were better than those tributed to the better-than-expected remission rates in
found in efficacy studies among patients with chronic de- this group of patients as well, although a firm conclusion
34 http://ajp.psychiatryonline.org Am J Psychiatry 163:1, January 2006TRIVEDI, RUSH, WISNIEWSKI, ET AL.
TABLE 4. Factors Associated With Remission Defined According to the 17-Item Hamilton Depression Rating Scale (HAM-D)
or the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), in Outpatients With Nonpsychotic
Major Depressive Disordera
Remission Defined by HAM-D (N=790) Remission Defined by QIDS-SR (N=943)
Patients With Patients With
Baseline Characteristic Characteristic Analysisb Characteristic Analysisc
Odds Odds
N % Ratio p N % Ratio p
RacedMEASUREMENT-BASED CARE IN STAR*D
TABLE 4. Factors Associated With Remission Defined According to the 17-Item Hamilton Depression Rating Scale (HAM-D)
or the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), in Outpatients With Nonpsychotic
Major Depressive Disordera (continued)
Remission Defined by HAM-D (N=790) Remission Defined by QIDS-SR (N=943)
Patients With Patients With
Baseline Characteristic Characteristic Analysisb Characteristic Analysisc
Recurrent depression 0.82TRIVEDI, RUSH, WISNIEWSKI, ET AL.
TABLE 4. Factors Associated With Remission Defined According to the 17-Item Hamilton Depression Rating Scale (HAM-D)
or the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), in Outpatients With Nonpsychotic
Major Depressive Disordera (continued)
Remission Defined by HAM-D (N=790) Remission Defined by QIDS-SR (N=943)
Patients With Patients With
Baseline Characteristic Characteristic Analysisb Characteristic Analysisc
Odds Odds
Mean SD Ratio p Mean SD Ratio p
Age (years) (units=10) 39.9 12.8 0.99 0.86 40.1 12.9 0.96 0.26
Education (years) (units=3) 14.1 3.2 1.20MEASUREMENT-BASED CARE IN STAR*D
TABLE 5. Factors Independently Associated With Remission Defined According to the 17-Item Hamilton Depression Rating
Scale (HAM-D) or the 16-Item Quick Inventory of Depressive Symptomatology, Self-Report (QIDS-SR), in Outpatients With
Nonpsychotic Major Depressive Disordera
Remission Defined Remission Defined
by HAM-D by QIDS-SR
(N=790) (N=943)
Factor Odds Ratiob p Odds Ratioc p
Social domain
Employment status (reference group=employed) 0.01TRIVEDI, RUSH, WISNIEWSKI, ET AL.
vices, Public Health Service, Agency for Health Care Policy and 20. Croughan JL, Secunda SK, Katz MM, Robins E, Mendels J, Swann
Research, 1993 A, Harris-Larkin B: Sociodemographic and prior clinical course
5. Koran LM, Gelenberg AJ, Kornstein SG, Howland RH, Friedman characteristics associated with treatment response in de-
RA, DeBattista C, Klein D, Kocsis JH, Schatzberg AF, Thase ME, pressed patients. J Psychiatr Res 1988; 22:227–237
Rush AJ, Hirschfeld RM, LaVange LM, Keller MB: Sertraline ver- 21. Greenhouse JB, Kupfer DJ, Frank E, Jarrett DB, Rejman KA:
sus imipramine to prevent relapse in chronic depression. J Af- Analysis of time to stabilization in the treatment of depression:
fect Disord 2001; 65:27–36 biological and clinical correlates. J Affect Disord 1987; 13:259–
6. Paykel ES, Scott J, Teasdale JD, Johnson AL, Garland A, Moore R, 266
Jenaway A, Cornwall PL, Hayhurst H, Abbott R, Pope M: Preven- 22. Hooley JM, Teasdale JD: Predictors of relapse in unipolar de-
tion of relapse in residual depression by cognitive therapy: a pressives: expressed emotion, marital distress, and perceived
controlled trial. Arch Gen Psychiatry 1999; 56:829–835 criticism. J Abnorm Psychol 1989; 98:229–235
7. Rush AJ, Fava M, Wisniewski SR, Lavori PW, Trivedi MH, Sackeim 23. Joyce PR, Paykel ES: Predictors of drug response in depression.
HA, Thase ME, Nierenberg AA, Quitkin FM, Kashner TM, Kupfer Arch Gen Psychiatry 1989; 46:89–99
DJ, Rosenbaum JF, Alpert J, Stewart JW, McGrath PJ, Biggs MM, 24. Katz MM, Koslow SH, Maas JW, Frazer A, Bowden CL, Casper R,
Shores-Wilson K, Lebowitz BD, Ritz L, Niederehe G: Sequenced Croughan J, Kocsis J, Redmond EJ: The timing, specificity and
Treatment Alternatives to Relieve Depression (STAR*D): ratio- clinical prediction of tricyclic drug effects in depression. Psy-
nale and design. Control Clin Trials 2004; 25:119–142 chol Med 1987; 17:297–309
8. Keller MB, Gelenberg AJ, Hirschfeld RM, Rush AJ, Thase ME, Koc- 25. Keller MB, Lavori PW, Mueller TI, Endicott J, Coryell W, Hirsch-
sis JH, Markowitz JC, Fawcett JA, Koran LM, Klein DN, Russell JM, feld RM, Shea T: Time to recovery, chronicity, and levels of psy-
Kornstein SG, McCullough JP, Davis SM, Harrison WM: The treat- chopathology in major depression: a 5-year prospective fol-
ment of chronic depression, part 2: a double-blind, random- low-up of 431 subjects. Arch Gen Psychiatry 1992; 49:809–816
ized trial of sertraline and imipramine. J Clin Psychiatry 1998; 26. Kocsis JH, Mason BJ, Frances AJ, Sweeney J, Mann JJ, Marin D:
59:598–607 Prediction of response of chronic depression to imipramine. J
9. Keller MB, McCullough JP, Klein DN, Arnow B, Dunner DL, Affect Disord 1989; 17:255–260
Gelenberg AJ, Markowitz JC, Nemeroff CB, Russell JM, Thase ME, 27. Vallejo J, Gasto C, Catalan R, Bulbena A, Menchon JM: Predic-
Trivedi MH, Zajecka J: A comparison of nefazodone, the cogni- tors of antidepressant treatment outcome in melancholia: psy-
tive behavioral-analysis system of psychotherapy, and their chosocial, clinical and biological indicators. J Affect Disord
combination for the treatment of chronic depression. N Engl J 1991; 21:151–162
Med 2000; 342:1462–1470 28. Kocsis JH: New issues in the prediction of antidepressant re-
10. Unützer J, Katon W, Callahan CM, Williams JW Jr, Hunkeler E, sponse. Psychopharmacol Bull 1990; 26:49–53
Harpole L, Hoffing M, Della Penna RD, Noel PH, Lin EH, Arean 29. Brugha TS, Bebbington PE, MacCarthy B, Sturt E, Wykes T, Potter
PA, Hegel MT, Tang L, Belin TR, Oishi S, Langston C: Collabora- J: Gender, social support and recovery from depressive disorders:
tive care management of late-life depression in the primary a prospective clinical study. Psychol Med 1990; 20:147–156
care setting: a randomized controlled trial. JAMA 2002; 288: 30. Goodwin FK: Predictors of antidepressant response. Bull Men-
2836–2845 ninger Clin 1993; 57:146–160
11. Rush AJ, Prien RF: From scientific knowledge to the clinical 31. Hoencamp E, Haffmans PM, Duivenvoorden H, Knegtering H,
practice of psychopharmacology: can the gap be bridged? Psy- Dijken WA: Predictors of (non-) response in depressed outpa-
chopharmacol Bull 1995; 31:7–20 tients treated with a three-phase sequential medication strat-
12. Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas egy. J Affect Disord 1994; 31:235–246
KR, Rush AJ, Walters EE, Wang PS: The epidemiology of major 32. Friedman RA, Parides M, Baff R, Moran M, Kocsis JH: Predictors
depressive disorder: results from the National Comorbidity of response to desipramine in dysthymia. J Clin Psychopharma-
Survey Replication (NCS-R). JAMA 2003; 289:3095–3105 col 1995; 15:280–283
13. Katon WJ, Von Korff M, Lin EH, Simon G, Ludman E, Russo J, 33. Cohn CK, Robinson DS, Roberts DL, Schwiderski UE, O’Brien K,
Ciechanowski P, Walker E, Bush T: The Pathways Study: a ran- Ieni JR: Responders to antidepressant drug treatment: a study
domized trial of collaborative care in patients with diabetes comparing nefazodone, imipramine, and placebo in patients
and depression. Arch Gen Psychiatry 2004; 61:1042–1049 with major depression. J Clin Psychiatry 1996; 57(suppl 2):15–18
14. Trivedi MH, Rush AJ, Crismon ML, Kashner TM, Toprac MG, Car- 34. Esposito K, Goodnick P: Predictors of response in depression.
mody TJ, Key T, Biggs MM, Shores-Wilson K, Witte B, Suppes T, Psychiatr Clin North Am 2003; 26:353–365
Miller AL, Altshuler KZ, Shon SP: Clinical results for patients 35. Aliapoulous J, Zisook S: Tricyclic antidepressant medications, in
with major depressive disorder in the Texas Medication Algo- Predictors of Treatment Response in Mood Disorders. Edited
rithm Project. Arch Gen Psychiatry 2004; 61:669–680 by Goodnick PJ. Washington, DC, American Psychiatric Press,
15. Baron RM, Kenny DA: The moderator-mediator variable dis- 1996, pp 1–36
tinction in social psychological research: conceptual, strategic, 36. Fava M, Rush AJ, Trivedi MH, Nierenberg AA, Thase ME, Sack-
and statistical considerations. J Pers Soc Psychol 1986; 51: eim HA, Quitkin FM, Wisniewski S, Lavori PW, Rosenbaum JF,
1173–1182 Kupfer DJ: Background and rationale for the Sequenced Treat-
16. Kraemer HC, Wilson T, Fairburn CG, Agras WS: Mediators and ment Alternatives to Relieve Depression (STAR*D) study. Psychi-
moderators of treatment effects in randomized controlled tri- atr Clin North Am 2003; 26:457–494
als. Arch Gen Psychiatry 2002; 59:877–883 37. Hamilton M: A rating scale for depression. J Neurol Neurosurg
17. Bosworth HB, McQuoid DR, George LK, Steffens DC: Time-to-re- Psychiatry 1960; 23:56–62
mission from geriatric depression: psychosocial and clinical 38. Hamilton M: Development of a rating scale for primary depres-
factors. Am J Geriatr Psychiatry 2002; 10:551–559 sive illness. Br J Soc Clin Psychol 1967; 6:278–296
18. Nierenberg AA: Predictors of response to antidepressants gen- 39. Zimmerman M, Mattia JI: A self-report scale to help make psy-
eral principles and clinical implications. Psychiatr Clin North chiatric diagnoses: the Psychiatric Diagnostic Screening Ques-
Am 2003; 26:345–352, viii tionnaire. Arch Gen Psychiatry 2001; 58:787–794
19. Bielski RJ, Friedel RO: Prediction of tricyclic antidepressant re- 40. Zimmerman M, Mattia JI: The Psychiatric Diagnostic Screening
sponse: a critical review. Arch Gen Psychiatry 1976; 33:1479– Questionnaire: development, reliability and validity. Compr
1489 Psychiatry 2001; 42:175–189
Am J Psychiatry 163:1, January 2006 http://ajp.psychiatryonline.org 39MEASUREMENT-BASED CARE IN STAR*D
41. Rush AJ, Zimmerman M, Wisniewski SR, Fava M, Hollon SD, 55. Mundt JC, Marks IM, Shear MK, Greist JH: The Work and Social
Warden D, Biggs MM, Shores-Wilson K, Shelton RC, Luther JF, Adjustment Scale: a simple measure of impairment in func-
Thomas B, Trivedi MH: Comorbid psychiatric disorders in de- tioning. Br J Psychiatry 2002; 180:461–464
pressed outpatients: demographic and clinical features. J Af- 56. Reilly MC, Zbrozek AS, Dukes EM: The validity and reproducibil-
fect Disord 2005; 87:43–55 ity of a work productivity and activity impairment instrument.
42. Novick JS, Stewart JW, Wisniewski SR, Cook IA, Manev R, Nieren- Pharmacoeconomics 1993; 4:353–365
berg AA, Rosenbaum JF, Shores-Wilson K, Balasubramani GK, 57. Nierenberg AA, Trivedi MH, Ritz L, Burroughs D, Greist J, Sack-
Biggs MM, Zisook S, Rush AJ (STAR*D investigators): Clinical and eim H, Kornstein S, Schwartz T, Stegman D, Fava M, Wisniewski
demographic features of atypical depression in outpatients SR: Suicide risk management for the Sequenced Treatment Al-
with major depression: preliminary findings from STAR*D. J ternatives to Relieve Depression study: applied NIMH guide-
Clin Psychiatry 2005; 66:1002–1011 lines. J Psychiatr Res 2004; 38:583–589
43. Fava M, Alpert JE, Carmin CN, Wisniewski SR, Trivedi MH, Biggs 58. Posternak MA, Zimmerman M, Keitner GI, Miller IW: A reevalu-
MM, Shores-Wilson K, Morgan D, Schwartz T, Balasubramani ation of the exclusion criteria used in antidepressant efficacy
GK, Rush AJ: Clinical correlates and symptom patterns of anx- trials. Am J Psychiatry 2002; 159:191–200
ious depression among patients with major depressive disor-
59. Rapaport MH, Pollack M, Wolkow R, Mardekian J, Clary C: Is pla-
der in STAR*D. Psychol Med 2004; 34:1299–1308
cebo response the same as drug response in panic disorder?
44. Khan AY, Carrithers J, Preskorn SH, Wisniewski SR, Lear R, Rush Am J Psychiatry 2000; 157:1014–1016
AJ, Stegman D, Kelley C, Kreiner K, Nierenberg AA, Fava M: Clin-
60. Zimmerman M, Chelminski I, Posternak MA: Exclusion criteria
ical and demographic factors associated with DSM-IV melan-
used in antidepressant efficacy trials: consistency across stud-
cholic depression. Ann Clin Psychiatry (in press)
ies and representativeness of samples included. J Nerv Ment
45. Rush AJ, Trivedi MH, Ibrahim HM, Carmody TJ, Arnow B, Klein Dis 2004; 192:87–94
DN, Markowitz JC, Ninan PT, Kornstein S, Manber R, Thase ME,
61. Zimmerman M, Chelminski I, Posternak MA: Generalizability of
Kocsis JH, Keller MB: The 16-item Quick Inventory of Depres-
antidepressant efficacy trials: differences between depressed
sive Symptomatology (QIDS), Clinician Rating (QIDS-C), and Self-
psychiatric outpatients who would or would not qualify for an
Report (QIDS-SR): a psychometric evaluation in patients with
efficacy trial. Am J Psychiatry 2005; 162:1370–1372
chronic major depression. Biol Psychiatry 2003; 54:573–583
62. Hunkeler EM, Meresman JF, Hargreaves WA, Fireman B, Ber-
46. Trivedi MH, Rush AJ, Ibrahim HM, Carmody TJ, Biggs MM,
man WH, Kirsch AJ, Groebe J, Hurt SW, Braden P, Getzell M,
Suppes T, Crismon ML, Shores-Wilson K, Toprac MG, Dennehy
Feigenbaum PA, Peng T, Salzer M: Efficacy of nurse telehealth
EB, Witte B, Kashner TM: The Inventory of Depressive Symp-
care and peer support in augmenting treatment of depression
tomatology, Clinician Rating (IDS-C) and Self-Report (IDS-SR),
in primary care. Arch Fam Med 2000; 9:700–708
and the Quick Inventory of Depressive Symptomatology, Clini-
cian Rating (QIDS-C) and Self-Report (QIDS-SR) in public sector 63. Hirschfeld RM, Montgomery SA, Aguglia E, Amore M, Delgado
patients with mood disorders: a psychometric evaluation. Psy- PL, Gastpar M, Hawley C, Kasper S, Linden M, Massana J, Men-
chol Med 2004; 34:73–82 dlewicz J, Moller HJ, Nemeroff CB, Saiz J, Such P, Torta R, Versi-
ani M: Partial response and nonresponse to antidepressant
47. Rush AJ, Bernstein IH, Trivedi MH, Carmody TJ, Wisniewski S,
therapy: current approaches and treatment options. J Clin Psy-
Mundt JC, Shores-Wilson K, Biggs MM, Woo A, Nierenberg AA,
chiatry 2002; 63:826–837
Fava M: An evaluation of the Quick Inventory of Depressive
Symptomatology and the Hamilton Rating Scale for Depres- 64. Keller MB, Klerman GL, Lavori PW, Coryell W, Endicott J, Taylor
sion: a Sequenced Treatment Alternatives to Relieve Depres- J: Long-term outcome of episodes of major depression. clinical
sion (STAR*D) trial report. Biol Psychiatry (in press) and public health significance. JAMA 1984; 252:788–792
48. Linn BS, Linn MW, Gurel L: Cumulative Illness Rating Scale. J Am 65. Rush AJ, Roffwarg HP, Giles DE, Schlesser MA, Fairchild C, Tarell
Geriatr Soc 1968; 16:622–626 J: Psychobiological predictors of antidepressant drug response.
49. Miller MD, Paradis CF, Houck PR, Mazumdar S, Stack JA, Rifai AH, Pharmacopsychiatria 1983; 16:192–194
Mulsant B, Reynolds CF III: Rating chronic medical illness burden 66. Fava M, Uebelacker LA, Alpert JE, Nierenberg AA, Pava JA,
in geropsychiatric practice and research: application of the Cu- Rosenbaum JF: Major depressive subtypes and treatment re-
mulative Illness Rating Scale. Psychiatry Res 1992; 41:237–248 sponse. Biol Psychiatry 1997; 42:568–576
50. Kobak KA, Greist JH, Jefferson JW, Mundt JC, Katzelnick DJ: Com- 67. Iosifescu DV, Nierenberg AA, Alpert JE, Smith M, Bitran S, Dord-
puterized assessment of depression and anxiety over the tele- ing C, Fava M: The impact of medical comorbidity on acute
phone using interactive voice response. MD Comput 1999; 16: treatment in major depressive disorder. Am J Psychiatry 2003;
63–68 160:2122–2127
51. Mundt JC: Interactive voice response systems in clinical re- 68. Hagerty BM, Williams RA: The effects of sense of belonging, so-
search and treatment. Psychiatr Serv 1997; 48:611–612 cial support, conflict, and loneliness on depression. Nurs Res
52. Trivedi MH, Rush AJ, Wisniewski SR, Warden D, McKinney W, 1999; 48:215–219
Downing M, Berman SR, Farabaugh A, Luther J, Nierenberg AA, 69. George LK, Blazer DG, Hughes DC, Fowler N: Social support and
Lis J, Sackeim H: Factors associated with health-related quality the outcome of major depression. Br J Psychiatry 1989; 154:
of life among outpatients with major depressive disorder: a 478–485
STAR*D report. J Clin Psychiatry (in press) 70. Hirschfeld RM, Klerman GL, Andreasen NC, Clayton PJ, Keller
53. Ware J Jr, Kosinski M, Keller SD: A 12-item short-form health MB: Psycho-social predictors of chronicity in depressed pa-
survey: construction of scales and preliminary tests of reliabil- tients. Br J Psychiatry 1986; 148:648–654
ity and validity. Med Care 1996; 34:220–233 71. Khan A, Leventhal RM, Khan SR, Brown WA: Severity of depres-
54. Endicott J, Nee J, Harrison W, Blumenthal R: Quality of Life En- sion and response to antidepressants and placebo: an analysis
joyment and Satisfaction Questionnaire: a new measure. Psy- of the Food and Drug Administration database. J Clin Psycho-
chopharmacol Bull 1993; 29:321–326 pharmacol 2002; 22:40–45
40 http://ajp.psychiatryonline.org Am J Psychiatry 163:1, January 2006You can also read